

Abstract
Context:
Cerbera odollam is a tree native to South Asia. It belongs to the poisonous Apocynaceae family. Deliberate self-harm with fruit of this plant is a major clinical problem in the developing world. Ingestion of C. odollam kernels is the cause of deaths in more than half of Kerala's plant poisoning deaths. The data on clinical features and complications of C. odollam poisoning are sparse, apart from a few case reports and limited studies.
Aims:
The present study was done to find the mode of presentation, complications, need for cardiac pacing, inhospital mortality, and the predictors of mortality in patients with C. odollam poisoning.
Settings and Design:
This was a retrospective study conducted in the department of general medicine in a tertiary care center in Alappuzha district, Kerala. The study period was for 1 year from January 1, 2016, to December 31, 2016.
Subjects and Methods:
All the patients admitted with a history of ingestion of odollam during the study period were included in the study. Data were collected from case records. The study was approved by the institutional ethics committee and research committee (IEC/TDMCA/EC3.dated29/11/201).
Statistical Analysis Used:
The data were analyzed using SPSS 16 for Windows (SPSS Inc., Chicago, IL, USA).
Results:
In this study, 102 patients were identified with C. odollam poisoning, and the mortality rate was 16.7%. Electrocardiogram (ECG) changes were common in our patients, and we observed different types of heart block in the same ECG itself. Ingestion of more than two kernels of odollam, late presentation to hospital, vomiting, bradycardia, hypotension, hyperkalemia, and more severe ECG changes were associated with significantly higher mortality in this study.
Conclusions:
C. odollam poisoning is a common method of deliberate self-harm in Kerala. It carries a high mortality rate, and the predictors of mortality include vomiting, bradycardia, hypotension, hyperkalemia, and the presence of severe ECG changes.
Keywords: Cerbera odollam, mortality predictors, poisoning
INTRODUCTION
Cerbera odollam (Pong-pong/Yellow-eyed Cerbera/Suicide tree/Buta buta) is a tree native to South Asia. Mainly seen in India and Sri Lanka, it belongs to the poisonous Apocynaceae family.[1] Deliberate self-harm with fruit of this plant is a major clinical problem in the developing world; however, it is relatively unknown to the western physicians.[2] Ease of availability makes C. odollam kernels, the cause of deaths in more than half of Kerala's ingested plant poisonings.[3] The fruits of this tree are smooth and round and contain a single large seed. They are seen along the sides of watercourses, ponds, coastal areas, and mangrove forests.[4] The principal cardiac glycosides in the seeds of C. odollam are cerberin, neriifolin, and diacetyl tanghinin.[1] The data on clinical features and complications of odollam poisoning are sparse apart from a few case reports and limited studies. The present study was done to find the mode of presentation, complications, need for cardiac pacing, inhospital mortality, and the predictors of mortality in patients with C. odollam poisoning.
SUBJECTS AND METHODS
This was a retrospective study conducted in the department of general medicine in a tertiary care center in Alappuzha district, Kerala. The study period was for 1 year from January 1, 2016, to December 31, 2016. All the patients admitted with a history of ingestion of odollam during the study period were included in the study. Patients with concurrent ingestion of another poisonous substance, patients younger than 12 years, patients with previous reports of electrocardiogram (ECG) changes, patients with chronic kidney disease or acute kidney injury, and patients whose case records were incomplete were excluded from the study. Data were collected from case records. The collected data included quantity of kernel consumed, time interval between ingestion of odollam and presentation to hospital, symptoms, co-ingestion with alcohol, clinical examination findings, investigation results, ECG, need for Intensive Care Unit (ICU) care, use of inotropes, temporary cardiac pacing, and mortality. The study was approved by the institutional ethics committee and research committee (IEC/TDMCA/EC34.dated29/11/2016).
Statistical analysis
The data were analyzed using SPSS 16 for Windows (SPSS Inc., Chicago, IL, USA). Quantitative data were expressed as mean and standard deviation. Descriptive data were expressed using percentages and frequencies. Chi-square test was done to assess the association of gender, quantity of ingestion, time interval between ingestion and presentation to hospital, co-ingestion with alcohol, vomiting, abdominal pain, type of pulse, heart rate, blood pressure, serum potassium levels, ECG changes, and type of block with mortality.
RESULTS
A total of 102 patients were studied of which 59 (57.8%) were males and 43 (42.2%) were females. The mean age of the patients was 29.9 ± 13.71 years with an age range of 13–79 years. Majority of the patients 56 (54.9%) were in the age group of 16–30 years closely followed by those in 31–45 years as shown in Figure 1.
Figure 1.
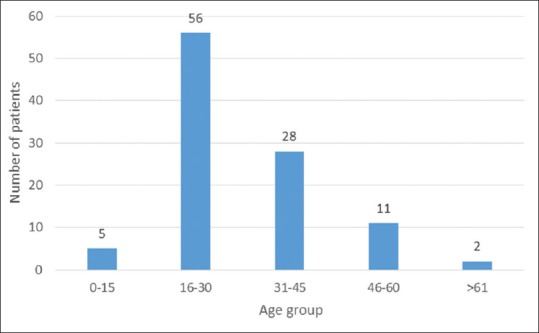
Age group of patients presenting with Cerbera odollam poisoning
About 54 (52.9%) patients sought treatment after a time lapse of more than 6 h after ingestion and 24 each after a time interval of <3 h and 3–6 h. The mean hospital stay was 4.62 ± 2.83 days with a duration range of 3 h to 15 days. Around 66 (64.7%) required ICU stay as depicted in Figure 2. The quantity consumed ranged from 0.5 to 5 kernels with a mean quantity of 1.77 ± 1.1 kernels. About 30 (29.4%) patients had co-ingested the odollam kernels along with alcohol.
Figure 2.
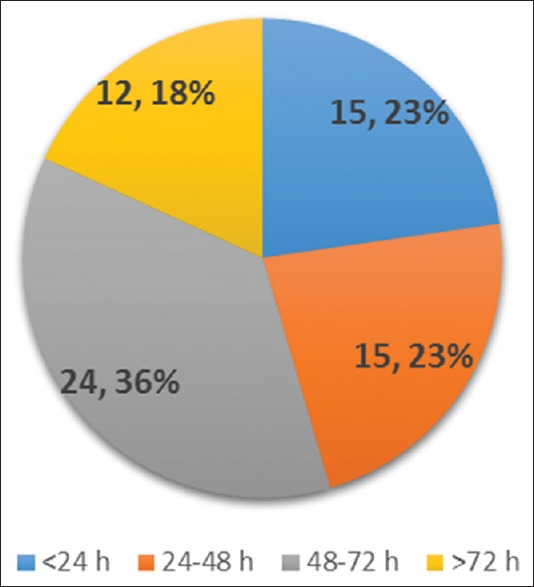
Intensive Care Unit stay in patients with Cerbera odollam poisoning
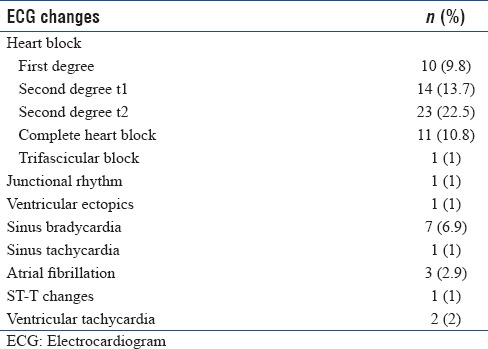
As summarized in Table 1, patients presented with vomiting, drowsiness, abdominal pain, and diarrhea. Irregular pulse, bradycardia, and hypotension were noted. ECG changes as listed in Table 2 were present in 75 (73.5%) patients. About 24 (23.5%) patients had hyperkalemia with serum k + more than 5.5 mEq/L.
Table 1.
Clinical profile of patients with Cerbera odollam poisoning (n=102)
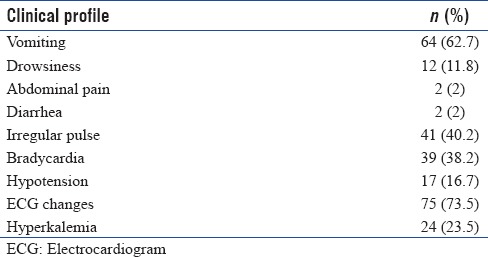
Table 2.
Electrocardiogram changes in patients with Cerbera odollam poisoning (n=102)
Patients were initially managed with stomach wash and activated charcoal. Hyperkalemia was corrected. Atropine was given for bradycardia as well as heart blocks. Of the 17 patients with hypotension, 16 received inotropic support. Temporary cardiac pacing was done for 18 patients with severe bradycardia not responding to atropine and higher degrees of heart block. One patient received temporary pacing for 33 h, and the rest received it for 48–72 h.
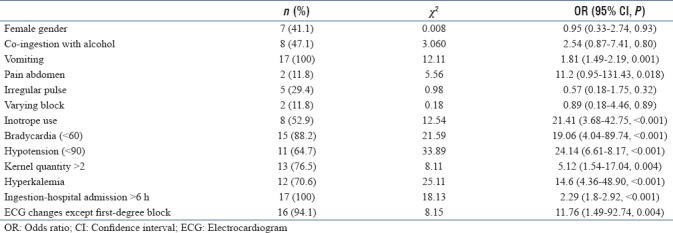
Of the 102 patients, 17 patients died and the mortality rate was 16.7%. Ingestion of more than two kernels, late presentation to hospital, presence of vomiting, bradycardia, hypotension, hyperkalemia, and more severe ECG changes were associated with statistically significant higher mortality as shown in Table 3.
Table 3.
Factors predicting mortality (n=17)
DISCUSSION
In this retrospective analysis, 102 patients were identified with C. odollam poisoning and the mortality rate was 16.7%. 57.8%of the victims of this suicide tree in our study were men. In an older study done in Kerala among the 537 suicidal deaths studied in 1989–1999, about 70%–75% were females.[5] The mean age of the patients in this study was 29.9 ± 13.71 years. Deliberate self-harm with Cerbera manghas, a closely related species, has been studied in Batticaloa district, Sri Lanka.[6,7] In line with this study, analysis on epidemic self-poisoning as with seeds of C. manghas showed that it is common among young unmarried males.[6]
Delayed admission to the hospital can affect the outcome of the patient as early medical intervention is necessary as in any case of poisoning. In this study, most of the patients were brought for medical treatment after a gap of 6 h after ingestion. Menon et al. stated that C. odollam poisoning merits monitoring and treatment in the ICU.[5] About 66 (64.7%) patients in this study were admitted to the ICU of which 12 required care for more than 3 days. Most of the deaths occurred within the first 24 h of poisoning.
The number of kernels of this plant has been deemed to be a useful measure of dosage in some studies.[5] There has been no established positive correlation between the amount of fruit kernel consumed and the number of deaths. However, in this study, the quantity consumed ranged from 0.5 to 5 kernels with a mean quantity of 1.77 ± 1.1 kernels, and consumption of more than two kernels was positively associated with mortality with an odds ratio (OR) of 5.12, confidence interval (CI) 1.54–17.04, and P = 0.004. The minimum lethal dose in this study was half a kernel of odollam in line with study by Menon et al. and in contrast to another study by Iyer and Narendranath in which it was one full kernel.[5,8]
In this study, all the patients were brought with a history of ingestion of odollam and all the cases were suicidal. Cardiac glycosides (cardenolides) such as cerberin reversibly inhibit the sodium-potassium adenosine triphosphatase (Na+-K+-ATPase) exchanger in myocardial cells.[2,9] This leads to increased levels of calcium in cardiac myocytes which causes increase in automaticity, increased vagal tone, and hyperkalemia.[10] All these produce cardiac arrhythmias and heart blocks. The common symptoms of odollam poisoning are vomiting, dizziness, abdominal pain, loose stools, chest pain, palpitation, and drowsiness.[5,6] Patients may have abnormalities in pulse such as bradycardia, irregular pulse, hypotension, ECG abnormalities, and hyperkalemia. In this study, vomiting was seen in more than 60% of the patients. Studies by Menon et al. and Selladurai et al. also described vomiting as the most common symptom.[5,6] Dizziness (11.8%), abdominal pain (2%), and diarrhea (2%) were seen in lesser number of patients. ECG changes were common in our patients, and we observed different types of heart block in the same ECG itself. Cardiac glycoside poisonings following suicidal ingestion of Cerbera species have shown ECG changes varying from sinus bradycardia to various degrees of atrioventricular block with ST-T changes on a 12-lead cardiogram.[11,12] Hyperkalemia with potassium concentration above 5.5 mEq/L was seen in 24 patients. A study by Bismuth et al.[13] on intentional overdose of acute digoxin poisoning showed that hyperkalemia was positively associated with mortality which is comparable to this study with OR = 14.6, CI = 4.36–48.90, P < 0.001. However, Menon et al. opinioned that hyperkalemia was not associated with higher mortality.[5]
Supportive treatment was provided to the patients. Temporary pacing was given to selected patients in this study. Timely use of pacemaker therapy has brought down the mortality of patients.[5] Although there are reports of use of digoxin-specific antibody fragments in managing the patients with odollam poisoning,[2,12] none of the patients in the study population received that. We observed a mortality rate of 16.7%, which was comparable to other similar studies.[5,6] Ingestion of more than two kernels of odollam, late presentation to hospital, vomiting, bradycardia, hypotension, hyperkalemia, and more severe ECG changes were associated with significantly higher mortality in this study. In a study by Selladurai et al. on C. manghas, persistent vomiting, severe abdominal pain, neurological signs, and persistent hyperkalemia were associated with higher mortality.[6]
The detection of Cerbera in body fluids is difficult. Thin-layer chromatography and high-pressure liquid chromatography can detect this poison.[14,15] Majority of cases are suicidal, but there are concerns about its use as a homicidal agent as the bitter taste of seeds can be masked with spices and may be added to food.[3,16] This plant is largely unknown to the western world, but there are reports of its use in the western countries after ingestion of seeds purchased online.[2,12]
CONCLUSIONS
C. odollam poisoning is a common method of deliberate self-harm in Kerala. It carries a high mortality rate, and the predictors of mortality include vomiting, bradycardia, hypotension, hyperkalemia, and the presence of severe ECG changes. Cases of C. odollam poisoning may be undiagnosed in areas of the world where this plant is not seen as the doctors may be unaware of the clinical features. With the global travel and availability of the seeds online, cases of odollam poisoning may be seen in other parts of world also. The clinicians need to be aware of this poison and the clinical and ECG manifestations and treatment options to save these patients. Although all the cases in this study were suicidal, there is a chance of odollam being used as a homicidal agent and analytical techniques such as HPLC will help in identifying this poison.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Chan EW, Wong SK, Chan HT. Apocynaceae species with antiproliferative and/or antiplasmodial properties: A review of ten genera. J Integr Med. 2016;14:269–84. doi: 10.1016/S2095-4964(16)60261-3. [DOI] [PubMed] [Google Scholar]
- 2.Kassop D, Donovan MS, Cohee BM, Mabe DL, Wedam EF, Atwood JE, et al. An unusual case of cardiac glycoside toxicity. Int J Cardiol. 2014;170:434–7. doi: 10.1016/j.ijcard.2013.11.019. [DOI] [PubMed] [Google Scholar]
- 3.Gaillard Y, Krishnamoorthy A, Bevalot F. Cerbera odollam: A 'suicide tree' and cause of death in the state of Kerala, India. J Ethnopharmacol. 2004;95:123–6. doi: 10.1016/j.jep.2004.08.004. [DOI] [PubMed] [Google Scholar]
- 4.Cerbera odollam Gaertn. [Last accessed on 2017 Oct 27]. Available from: http://www.indiabiodiversity.org/biodiv/species/show/229134 .
- 5.Menon MS, Kumar P, Jayachandran CI. Clinical profile and management of poisoning with suicide tree: An observational study. Heart Views. 2016;17:136–9. doi: 10.4103/1995-705X.201783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Selladurai P, Thadsanamoorthy S, Ariaranee G. Epidemic self-poisoning with seeds of Cerbera manghas in Eastern Sri Lanka: An analysis of admissions and outcome. J Clin Toxicol. 2016;6:287. [Google Scholar]
- 7.Eddleston M, Haggalla S. Fatal injury in Eastern Sri Lanka, with special reference to cardenolide self-poisoning with Cerbera manghas fruits. Clin Toxicol (Phila) 2008;46:745–8. doi: 10.1080/15563650701668617. [DOI] [PubMed] [Google Scholar]
- 8.Iyer GV, Narendranath M. A preliminary report on the neurological manifestations of Cerbera odollam poisoning. Indian J Med Res. 1975;63:312–4. [PubMed] [Google Scholar]
- 9.Chan EW, Wong SK, Chan HT, Baba S, Kezuka M. Cerbera are coastal trees with promising anticancer properties but lethal toxicity: A short review. J Chin Pharm Sci. 2016;25:161–9. [Google Scholar]
- 10.Auerbach PS. Wilderness Medicine. 6th ed. United States: Mosby; 2011. [Google Scholar]
- 11.Tsai YC, Chen CY, Yang NI, Yang CC. Cardiac glycoside poisoning following suicidal ingestion of Cerbera manghas. Clin Toxicol (Phila) 2008;46:340–1. doi: 10.1080/15563650701291766. [DOI] [PubMed] [Google Scholar]
- 12.Fok H, Victor P, Bradberry S, Eddleston M. Novel methods of self-poisoning: Repeated cardenolide poisoning after accessing Cerbera odollam seeds via the internet. Clin Toxicol (Phila) 2018;56:304–6. doi: 10.1080/15563650.2017.1369543. [DOI] [PubMed] [Google Scholar]
- 13.Bismuth C, Gaultier M, Conso F, Efthymiou ML. Hyperkalemia in acute digitalis poisoning: Prognostic significance and therapeutic implications. Clin Toxicol. 1973;6:153–62. doi: 10.3109/15563657308990513. [DOI] [PubMed] [Google Scholar]
- 14.Malathy K, Krishnamoorthy A. Detection of Cerbera odollam by thin-layer chromatography. J Chromatogr. 1978;152:592–4. doi: 10.1016/s0021-9673(00)85107-9. [DOI] [PubMed] [Google Scholar]
- 15.Ramakrishnan UK, Pillay VV, Arathy SL. Forensic implications of viscera analysis in death due to Cerbera odollam poisoning. J Indian Soc Toxicol. 2014;10:23–7. [Google Scholar]
- 16.Shetty CK. Forensic relevance of the suicide tree “Cerebra odollam”. Int J Clin Pharmacol Toxicol. 2016;5:240–1. [Google Scholar]