

Abstract
Aim
Functional high intensity training (F-HIT) is a novel fitness paradigm that integrates simultaneous aerobic and resistance training in sets of constantly varied movements, based on real-world situational exercises, performed at high intensity in workouts that range from ~8-20 min/session. We hypothesized that F-HIT would be an effective exercise mode for reducing insulin resistance in type 2 diabetes (T2D).
Methods
We recruited 13 overweight/obese adults (5 males, 8 females; 53±7 years; BMI 34.5±3.6 kg•m−2, Mean±SD) with T2D to participate in a 6 week (3d/wk) supervised F-HIT program. An oral glucose tolerance test was used to derive measures of insulin sensitivity.
Results
F-HIT significantly reduced fat mass (43.8±83.8 vs 41.6±7.9 kg; P<0.01), diastolic blood pressure (80.2±7.1 vs 74.5±5.8; P<0.01), blood lipids (triglyceride and VLDL, both P<0.05) and metabolic syndrome z-score (6.4±4.5 vs −0.2±5.2 AU; P<0.001), and increased basal fat oxidation (FOX: 0.08±0.03 vs 0.10±0.04 g•min−1; P=0.05), and HMW adiponectin (214.4±88.9 vs 288.8±127.4 ng•mL−1; P<0.01). Importantly, F-HIT also increased insulin sensitivity (0.037±0.010 vs 0.042±0.010 AU; P<0.05). Increases in HMW adiponectin and FOX correlated with the change in insulin sensitivity (rho: 0.75; P<0.05, rho: 0.81; P<0.01, respectively). Compliance with the training program was >95% and no injuries or adverse events were reported.
Conclusion
These data suggest that F-HIT may be an effective exercise mode for managing T2D. The increase in insulin sensitivity addresses a key defect in T2D and is consistent with improvements observed after more traditional aerobic exercise programs in overweight/obese adults with T2D.
Keywords: Crossfit™, diabetes, insulin resistance, insulin sensitivity, obesity
INTRODUCTION
Physical activity remains central to the treatment and prevention of type 2 diabetes (T2D) and cardiovascular disease, yet empirical evidence for durable exercise training-induced improvements in insulin sensitivity and cardiovascular health in diabetes is scarce. Current physical activity recommendations for T2D include at least moderate intensity (40-60% VO2max), aerobic exercise, 3-5 times per week. In addition to aerobic exercise, resistance training 2-3 times per week is also recommended, recognising greater benefits from this combined training than either aerobic or resistance training alone (Colberg et al., 2016). Such programs typically take more than 5 hours per week to complete. Despite these recommendations, compliance and adherence to exercise advice continues to remain disappointingly low. Although patients with prediabetes and T2D report awareness that diet and physical activity can improve their condition, these patients have not applied this advice to their own health (Green et al., 2007). In fact, only 42% of US patients with T2D are reported to have met the guidelines for physical activity (Zhao et al., 2008). One of the most cited barriers to regular physical activity is lack of time (Korkiakangas et al., 2009).
In order to mitigate this perceived barrier to physical activity, high-intensity exercise has been proposed as a time-efficient method for achieving cardio-metabolic health outcomes equivalent to traditional aerobic training programs (Gibala, 2007; Gibala et al., 2012). Such has been the increased popularity of high-intensity training amongst exercise specialists and the general public that programs like “boot camp’ – a military-styled fitness approach (Thompson, 2014) - and high-intensity interval training (HIIT) have become mainstays in the top 20 worldwide fitness trends since 2010, with HIIT featured in the top 5 in each year since its initial appearance in 2014 (Thompson, 2014). Moreover, Crossfit™, which provides a form of Functional High Intensity Training (F-HIT), has established remarkable participation rates worldwide (Butcher et al., 2015).
HIIT typically involves repeated, short intervals of running or cycling performed at 85-95% of peak heart rate interspersed with periods of rest or low intensity exercise, while sprint interval training (SIT) refers to similar modes of exercise performed at ≥100% peak heart rate (Weston et al., 2013). While these modes of high intensity training may be adequate, or perhaps superior, alternatives to moderate intensity aerobic exercise for metabolic health (Boule et al., 2001; Snowling & Hopkins, 2006; Weston et al., 2014; Jelleyman et al., 2015), they typically lack a resistance exercise component (Weston et al., 2013). Crossfit™, on the other hand, involves functional high intensity training (F-HIT) that incorporate 2-3 different exercises per workout including weightlifting, gymnastics, body weight, and endurance type exercises. The workouts are performed either in the shortest amount of time, for as many rounds as possible in a given time, or for maximal loads. Despite its growing popularity, few studies have examined the efficacy of such interventions in the general population (McRae et al., 2012; Heinrich et al., 2014; Butcher et al., 2015; Murawska-Cialowicz et al., 2015), and none to our knowledge in individuals with T2D. We therefore examined the effectiveness of a 6 week CrossFit™ F-HIT intervention in individuals with T2D. We hypothesized that, given the combined aerobic and resistance components, F-HIT would reduce body fat while maintaining lean tissue mass, and ameliorate insulin resistance and cardio-metabolic risk in individuals with T2D.
METHODS
Ethical Approval
The study was approved by the Cleveland Clinic Institutional Review Board (IRB#: 12-436) and all subjects provided signed informed consent in accordance with guidelines for the protection of human subjects and the Declaration of Helsinki, except for registration in a database (clause 35).
Subject Population
We recruited 13 overweight/obese, sedentary adults (5 males, 8 females; age 53±7 years; BMI 34.5±3.6 kg•m−2; mean±SD) with clinically diagnosed non-insulin dependent T2D from the local community. This dataset includes 12 participants that were described in a previous publication examining the effect of F-HIT on pancreatic β-cell function in individuals with T2D (Nieuwoudt et al., 2017). All participants were screened with a medical history and physical examination, blood and urine chemistry analyses, and a resting and exercise stress test with 12-lead electrocardiogram. Individuals were excluded from participation if they, 1) were smokers in the past 5 years, 2) had greater than 5 kg weight change in the previous 6 months, 3) undertook regular exercise (>30 min/day, >3 days/week), 4) had contraindications to elevated levels of physical activity as indicated by an electrocardiogram, 5) demonstrated any evidence of current or previous hematological, renal, hepatic, cardiovascular, or pulmonary disease, or 6) patients taking insulin, or thyroid medications. Female subjects were either, postmenopausal and not using any hormone replacement therapy, or premenopausal and in the follicular phase of the menstrual cycle during the testing period. Thus, premenopausal women had baseline testing ~2 weeks prior to the commencement of the exercise intervention.
Medications & Supplements
All but one participant was taking one (n=5) or more (2 drugs, n=4; >2 drugs, n=3) oral hypoglycemic agents. These included metformin (n=12), sulfonylureas (n=5), and GLP-1 agonists (n=3). In addition, 5 participants were taking one blood pressure medication and 4 were taking two blood pressure medications. These included thiazide diuretics (n=6), ACE inhibitors (n=4), ANGII inhibitors (n=3). In addition, seven participants were taking statins. All participants were instructed under medical supervision to withhold medications for 48 hours prior to metabolic testing.
Four participants reported taking a daily multivitamin and four also reported taking vitamin D daily. In addition, aspirin and ibuprofen was taken daily by four participants and tramadol by one. One participant also reported taking L-Lysine, zinc, cinnamon, and Naftifine HCl. Additionally two participants were taking fish oil supplements. Medications and supplement dosages were maintained constant throughout the duration of the study.
Exercise Intervention
Subjects participated in a 6-week F-HIT training program at an established CrossFit™ gym. An experienced CrossFit™ coach led groups of 2-6 subjects in three exercise training sessions per week. Training sessions included a warm-up, skill practice, and one high-intensity workout, performed at >85% HR maximum, ranging in duration from ~8-20 minutes. Over the course of 6-weeks, subjects were exposed to an array of functional weightlifting, gymnastics, and endurance movements in various combinations such as deadlifts, clean and snatch, overhead press, gymnastic style ring exercises, box jumps, and body weight exercises. All subjects completed the same workouts, however, no individual sessions were replicated - with the exception of session 2 and 18 which was used as a measure of functional improvement (Nieuwoudt et al., 2017). Examples of specific workouts are described in table 1. In addition, sample relative heart rate responses from 5 individuals during a session are presented in Figure 1. Three-day diet records were obtained prior to, and in the last week of, the exercise intervention to monitor any changes in dietary intake. Furthermore, subjects were instructed to avoid caffeine consumption for 12- and alcohol for 48-hours prior to testing and to consume the same diet containing 250 g carbohydrate on the day prior to the pre- and post-study testing days. Post-intervention testing commenced ~24-36 hours following the last exercise bout.
Table 1.
Example workouts performed by participants during the 6-week F-HIT intervention
| Day 2 | Day 11 | Day 16 | |
|---|---|---|---|
| Warm Up: |
|
3 sets; 15 reps
|
Warmup 3 sets; 10 reps
|
| WOD: |
5 sets; 1 min per exercise:
|
|
|
| Cool down: | 3 sets:
|
|
30 reps each:
Mountain Climbers |
Figure 1.
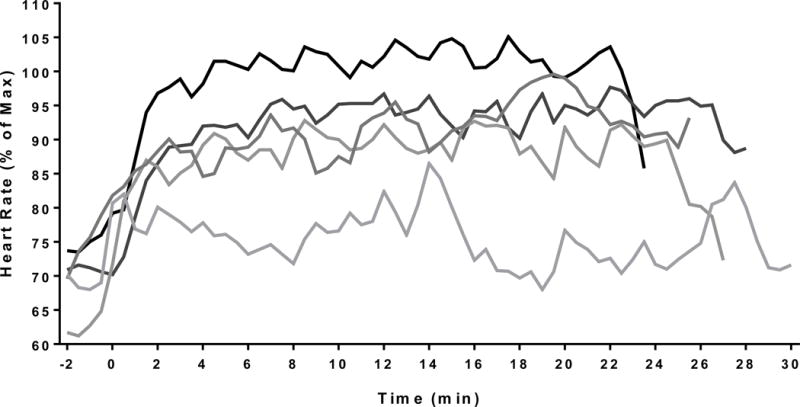
Relative heart rates for 5 individuals during the “deck of cards” workout (Session 12). During this workout participants performed a set of exercises determined by deck of cards. In this example, ♣ = Kettlebell Swings; ♠ = Squats; ♥ = Push Ups; ◆ = Sit Ups; Joker = 10 Burpees, and the number of reps performed was determined by the value of the card, ie. 8◆ = 8 Sit Ups. Participants alternated between flipping a card and performing the exercise with a partner until the deck was finished.
Body Composition
Height and weight were obtained with participants wearing a standard hospital gown and by use of a wall-mounted stadiometer and a calibrated scale. BMI was calculated as body mass (kilograms) divided by the square of height (meters). Body fat distribution, and fat-free mass were assessed using dual-energy x-ray absorptiometry (iDXA, Lunar Prodigy; GE Healthcare). Waist circumference was measured up to 3 times with the use of a plastic tape measure ∼2 cm above the umbilicus. Measurements within 0.5 cm were averaged and used for analysis.
Blood Pressure
Blood pressure was measured using an automated platform (DINAMAPProcare 400; GE Medical Systems) to obtain morning brachial SBP and DBP measurements. Measurements were performed on the left arm in a lowly lighted room while participants lay semisupine after 10 min of awake rest. Reported data were based on the mean of 3 measurements. Mean arterial pressure was calculated as 2/3(DBP) + 1/3(SBP). Pulse pressure was estimated by subtracting DBP from SBP.
Insulin Sensitivity and Substrate Metabolism
Subjects arrived at the Clinical Research Unit following an overnight fast, and lay supine in bed for 30 minutes followed by assessment of non-protein corrected, whole body fat oxidation (FOX) by indirect calorimetry using the following equation; (FOX = 1.695(VO2) – 1.701(VCO2) (Peronnet & Massicotte, 1991). Subsequently, a 75 gram OGTT was administered. Baseline blood draws were obtained from an antecubital vein prior to ingestion of the glucose drink. Blood samples were drawn in EDTA tubes at 30, 60, 90, 120 and 180 minutes after ingestion. Total and incremental metabolite responses (area under the curve, tAUC and iAUC, respectively) during the OGTT were calculated using the trapezoidal rule. Insulin sensitivity during the OGTT was calculated using the modified Stumvoll equation (Solomon et al., 2014).
Biochemical Analysis and Cardiometabolic Risk Score
Plasma analyses were performed on samples that had been stored at −80°C immediately following post-draw processing. Glucose was determined using the YSI 2300 STAT Plus analyser (Yellow Springs, OH), and insulin was determined via radioimmunoassay (Millipore, Billerica, MA). Triglycerides and cholesterol were analysed using enzymatic methods with an automated platform (Roche Modular Diagnostics, Indianapolis, IN). Fasting plasma high molecular weight (HMW) adiponectin and resistin were measured at baseline and following the exercise intervention by ELISA (Millipore, Billerica, MA). Plasma creatine kinase (CK) was measured using an enzymatic activity assay (Sigma-Aldrich, St. Louis, MO). Sex-specific z-scores were calculated to determine the efficacy of the intervention on decreasing the severity of the metabolic syndrome (Malin et al., 2014)
Statistical Analyses
Statistical analysis was performed using GraphPad Prism 6.0 (Graphpad Software Inc., San Diego CA). Values were tested for normality using the D’Agostino & Pearson omnibus normality test. Pre- to post-intervention changes were assessed using a repeated measures analysis of variance for normally distributed samples. Pre- to post-changes that were not normally distributed were assessed using the non-parametric Wilcoxon signed rank test. Pearson’s correlation was used to examine associations between normally distributed data. In addition, Spearman’s rank correlation analyses were used to identify relationships between variables that failed the normality test. Statistical significance was accepted when P<0.05 and all data are expressed as mean±SD.
RESULTS
Body Composition and Blood Pressure
Anthropometric data for the group are summarised in Table 2. Six-weeks of F-HIT training did not produce significant changes in body weight or BMI (P=0.11). Regional changes to body composition are reported in Table 3. Notably, android fat (P<0.05), gynoid fat (P<0.01), trunk fat (P<0.05), and leg fat (P<0.0001) were all decreased, while lean tissue remained unchanged. Aerobic fitness (VO2max) was increased after the F-HIT training program (Nieuwoudt et al., 2017). The 6-week exercise intervention also resulted in a decrease in diastolic blood pressure (DBP; P<0.01), mean arterial pressure (MAP; P<0.05).
Table 2.
Participant demographic and anthropometric characteristics, and blood pressure responses before and after six weeks of F-HIT training. Data are Mean±SD.
| Variable | PRE | POST | P–value |
|---|---|---|---|
| Sex (M/F) | 5/8 | – | – |
| Age (years) | 53±7 | – | – |
| Height (cm) | 168.7±10.1 | – | – |
| Weight (kg) | 98.2±11.8 | 96.5±9.2 | 0.09 |
| BMI (kg•m−2) | 34.5±3.6 | 34.0±3.1 | 0.11 |
| Waist circumference (cm) | 110.7±12.3 | 108.7±11.7 | 0.11 |
| SBP (mmHg) | 133.8±7.7 | 132.8±12.3 | 0.73 |
| DBP (mmHg) | 81.0±5.1 | 75.4±7.1 | <0.01 |
| MAP (mmHg) | 98.6±5.1 | 94.6±7.8 | <0.05 |
| Pulse Pressure (mmHg) | 52.8±6.9 | 57.4±10.3 | 0.06 |
Table 3.
Total and regional fat and lean mass distribution before and after 6-weeks of F-HIT training. Data are Mean±SD.
| Variable | PRE | POST | P-value |
|---|---|---|---|
| Total Fat Mass (kg) | 43.0±8.8 | 40.7±7.9 | <0.001 |
| Android Fat (kg) | 4.8±1.1 | 4.4±0.9 | <0.05 |
| Gynoid Fat (kg) | 6.8±2.1 | 6.4±2.0 | <0.01 |
| Arms Fat (kg) | 4.6±1.2 | 4.4±1.3 | 0.09 |
| Legs Fat (kg) | 11.7±1.9 | 11.0±1.7 | <0.0001 |
| Trunk Fat (kg) | 24.4±5.0 | 23.1±4.5 | <0.05 |
| Total Fat-Free Mass (kg) | 55.2±7.8 | 55.5±6.8 | 0.63 |
| Android Lean (kg) | 3.8±0.7 | 3.7±0.9 | 0.68 |
| Gynoid Lean (kg) | 7.6±1.5 | 7.7±1.3 | 0.68 |
| Arms Lean (kg) | 6.4±1.3 | 6.4±1.3 | 1.00 |
| Legs Lean (kg) | 18.3±1.4 | 18.6±1.7 | 0.41 |
| Trunk Lean (kg) | 25.4±3.6 | 25.6±3.2 | 0.58 |
Insulin Sensitivity and Metabolic Syndrome Severity
ISIOGTT was increased in all but one individual following training (Figure 2A). Even though there was a downward shift in the overall glucose response during the post-intervention OGTT, total (tAUC; P=0.20) and incremental (iAUC; P=0.85) glucose area under the curve (Table 4) were not significantly altered. Insulin areas under the curve (tAUC P=0.16 and iAUC; P=0.88) were unchanged after the intervention (Table 4). Metabolic syndrome severity was also reduced following the intervention (P<0.001; Figure 2B).
Figure 2.
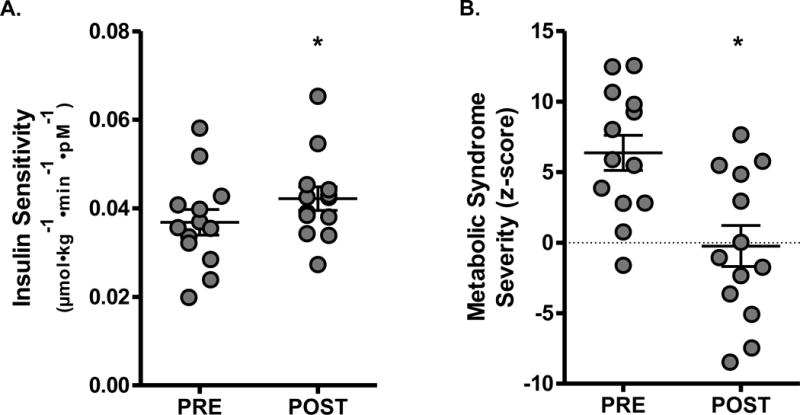
A) ISIOGTT was significantly increased and B) metabolic syndrome severity was reduced following the 6-week intervention. Data are Mean±SD. *P<0.05
Table 4.
Blood biochemistry changes before and after a 6-week F-HIT intervention. AUC values were determined from a 3-hour OGTT. All other measures were taken in the morning following an overnight fast. Data are Mean±SD.
| Variable | PRE | POST | P-value |
|---|---|---|---|
| tAUC Glucoseᵜ (mmol•L−1•3h) | 2783.7±706.6 | 2578.4±619.8 | 0.20 |
| iAUC Glucose (mmol•L−1•3h) | 1049.8±216.9 | 1038±210.4 | 0.85 |
| tAUC Insulinᵜ (μU•mL−1•3h) | 10859±8031 | 12355±10850 | 0.16 |
| iAUC Insulinᵜ (μU•mL−1•3h) | 8464±7403 | 8555±8763 | 0.88 |
| Triglycerides (mg•dL−1)ᵜ | 146.7±88.3 | 110.8±64.9 | <0.05 |
| Cholesterol (mg•dL−1) | 176.9±30.3 | 160.4±32.7 | 0.11 |
| VLDL cholesterol (mg•dL−1)ᵜ | 29.3±17.6 | 22.2±13.0 | <0.05 |
| LDL cholesterol (mg•dL−1)ᵜ | 96.7±26.1 | 87.1±29.9 | 0.15 |
| Resistin (ng•mL−1) | 6.4±4.9 | 5.6±4.4 | <0.05 |
| Creatine Kinase (U•L−1) | 83.4±17.3 | 116.2±67.9 | <0.05 |
denotes that data was analyzed using the non-parametric Wilcoxon signed rank test.
Substrate Metabolism and Blood Biochemistry
F-HIT resulted in significant increases in fat oxidation (P<0.05; Figure 3A) and HMW adiponectin (P<0.01; Figure 3B) along with reductions in plasma triglycerides (P<0.05) and VLDL cholesterol (P<0.05) (Table 3). There were also reductions in total cholesterol (P=0.11) and LDL cholesterol (P=0.15); however, these changes did not reach statistical significance. Plasma resistin was reduced (P<0.05) after the exercise program (Table 3). Plasma CK was increased (P<0.05), following 6-weeks of training (Table 3).
Figure 3.
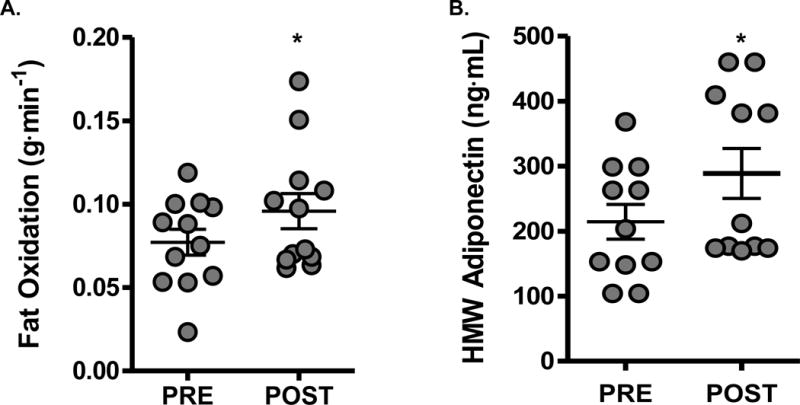
A) Fat oxidation and B) HMW adiponectin are significantly increased following the intervention. Data are Mean±SD. *P<0.05
Correlation Analysis
The increase in HMW adiponectin and FOX both correlated with the change in ISIOGTT (P<0.01, Figure 4A and B). Moreover, ISIOGTT changes were correlated with decreases in both fasting glucose (Nieuwoudt et al., 2017) (rho −0.26; P<0.05) and tAUC glucose (rho −0.27; P<0.05). Changes in HMW adiponectin were also associated with alterations in total fat mass (rho −0.67; P<0.05), while differences in glucose iAUC were correlated with increases in CK (r=0.61; P<0.05).
Figure 4.
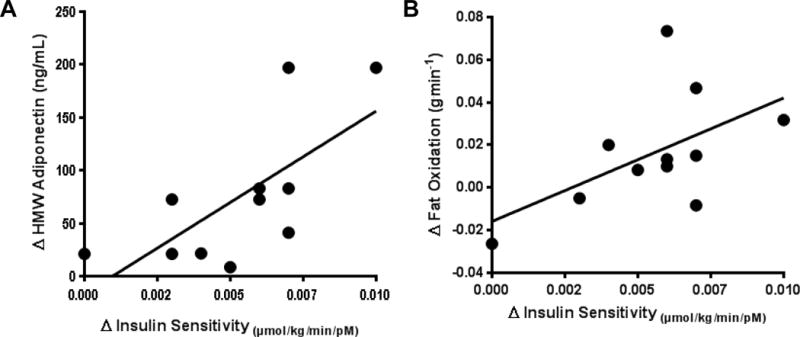
Correlation between pre- to post-intervention changes in ISIOGTT and A. plasma HMW adiponectin (rho = 0.70; P<0.05) and, B. whole body fat oxidation (rho = 0.86; P<0.05). Data were analysed using a Spearman’s rank correlation.
DISCUSSION
Exercise training has long been recognised as a key component in the clinical management of patients with T2D (American Diabetes Association, 2014). Despite this, adherence to traditional exercise programs is low (Ary et al., 1986; Clark, 1997), with one of the main barriers to adherence cited as a lack of time (Korkiakangas et al., 2009). Here, we demonstrate for the first time in patients with T2D, the effectiveness of a novel high intensity training modality for increasing insulin sensitivity, FOX, and HMW-adiponectin, while reducing fat mass, plasma triglycerides and cholesterol, metabolic syndrome severity, diastolic blood pressure, and plasma concentration of the pro-inflammatory adipokine resistin over the course of a 6-week intervention using short 8-20 minute workouts, 3-days per week. It is important to note that this was achieved with no injuries reported, and greater than 95% compliance with the exercise program. This is significant due to the widespread, and legitimate, concerns expressed within the fitness and scientific community regarding the safety and efficacy of Crossfit-style F-HIT training programs for individuals with pre-existing chronic illness (Karstoft et al., 2013; Mitranun et al., 2014; Thompson, 2014). The data presented herein, however, indicate that F-HIT, performed in a controlled setting, and under appropriate supervision, is effective for individuals with T2D. Our data also adds to the growing body of literature which suggests that high intensity exercise interventions may offer a time efficient approach to achieve outcomes comparable to traditional aerobic exercise programs.
Glucose lowering is the major focus in the management of patients with T2D (Inzucchi et al., 2012). Traditional, long duration, moderate intensity aerobic exercise programs have proven extremely effective at improving insulin sensitivity (Mourier et al., 1997), reducing HbA1c (Umpierre et al., 2011), and regulating plasma glucose levels (Holloszy et al., 1986). Indeed, we have observed improvements of ~25% in clamp and OGTT derived measures of insulin sensitivity with as little as 7-days of moderate intensity aerobic exercise (Kirwan et al., 2009). However, these interventions lack a resistance training component, and this is particularly important where weight loss is accompanied by a loss of lean tissue (Baba et al., 1999; Saris et al., 2000; Brehm et al., 2005; Solomon et al., 2010). Increasing recognition of the role of lean mass in the regulation of blood glucose in T2D (Srikanthan & Karlamangla, 2011; Kirwan et al., 2017) has prompted the ADA to add 2-3 days of resistance training per week to their physical activity recommendations (Colberg et al., 2016). Nonetheless, while the addition of resistance exercise training to physical activity recommendations is a welcome step, the added exercise burden is unlikely to increase adherence to exercise recommendations. We were therefore interested to understand whether the combination of aerobic and resistance training performed at high intensity would result in similar improvements in insulin sensitivity to those we have previously observed in individuals with T2D (Fenicchia et al., 2004; Kirwan et al., 2009; Ryan, 2010) while preserving the lean mass sparing benefits of resistance training. The 15% improvement in insulin sensitivity observed in this study reflects a consistent and positive outcome. This was achieved while maintaining total and regional lean mass coincident with reductions in total and regional fat mass.
Despite the improvements insulin sensitivity, we did not observe significant reductions in glucose area under the curve following the exercise intervention. Several recent interventional studies have suggested that high intensity exercise programs may result in improvements in HbA1c (Dunstan et al., 2002; Hansen et al., 2009), and improvements in glucose homeostasis measured by continuous glucose monitoring (Karstoft et al., 2014) without apparent differences in glucose AUC during an OGTT. Previous research indicates that muscle damage from eccentric exercise transiently reduces insulin sensitivity (Kirwan et al., 1992) and there have been isolated reports of rhabdomyolysis associated with CrossFit-style exercise (Larsen & Jensen, 2014). However, while eccentric exercise induced muscle damage is an expected, acute response, training adaptations rapidly result in a resistance to exercise induced muscle damage (Howatson et al., 2007). Nonetheless, we considered whether transient impairments in glucose uptake induced by muscle damage might have contributed to this anomaly and we did observe a modest increase in circulating CK after the 6-week training intervention. In the absence of a control group it is unclear whether this change was related to the intervention or just a normal fluctuation associated with T2D, and although the increases in CK are well below the levels reported in rhabdomyolysis, we did observe a positive correlation between changes in plasma CK and glucose iAUC which suggests that a longer intervention may be required to allow the skeletal musculature to fully adapt to the demands of F-HIT. Moreover, the ISIOGTT response observed in the current study may, as a result, underestimate the magnitude of change in glucose homeostasis achievable with F-HIT exercise.
Individuals with T2D are at significantly higher risk for cardiovascular disease, which can manifest as increased metabolic syndrome severity. This elevated risk persists when compared to non-diabetic individuals similar in age and body fat distribution (Malin et al., 2014). Wijndaele et al. (Wijndaele et al., 2006) developed a metabolic syndrome risk score (z-score) that provides a continuous metric of metabolic syndrome severity. Here we observed a ~110% decrease in the metabolic syndrome z-score following the exercise intervention. There are currently few interventional studies that we are aware of that have examined metabolic syndrome z-score responses to exercise interventions in individuals with T2D. Nonetheless, the decreased risk observed in the current study appears superior to a recent study examining z-score risk in individuals with T2D undergoing 16 weeks of either moderate intensity continuous training 5 days per week (41% reduction), or HIIT 3 days per week (51% or 1% protocol dependent reduction) (Ramos et al., 2017). This may be due to the fact that the participants started with higher average baseline z-score values. However, it should also be noted that the post-intervention average z-score in the current study was lower compared to the Ramos et al. study, despite a markedly reduced duration of intervention.
Components of the metabolic syndrome z-score include fasting plasma glucose, triglycerides, waist circumference, mean arterial pressure, and high density lipoprotein content. We observed significant improvements in triglycerides and mean arterial pressure, while fasting glucose and waist circumference tended towards a significant reduction. The improvement in MAP was provoked by a significant reduction in diastolic blood pressure of ~5.5 mmHg following the intervention. Notably, this was achieved in a cohort where significant hypertension was not present. We did not observe changes in systolic blood pressure or heart rate, however, the duration of the intervention may have been too short to achieve significant improvements in these outcomes. Nonetheless, the reduction in diastolic blood pressure represents a significant reduction in mortality risk, especially stroke risk (Lindenstrom et al., 1995). The reduction in diastolic blood pressure may represent a novel early adaptation to F-HIT style exercise, compared to HIIT/SIT, in T2D or metabolic syndrome as several recent reports utilizing 12- and 15 week HIIT or SIT interventions showed no change in diastolic blood pressure (Stensvold et al., 2010; Mitranun et al., 2014; Mohr et al., 2014), though notably systolic pressure was reduced in a 12 week intervention (Mohr et al., 2014). In a 6-week aerobic conditioning and HIIT intervention, diastolic blood pressure was reduced in older, healthy sedentary men, however, the reduction was observed in the conditioning component and no further reduction was observed following HIIT (Grace et al., 2017).
Similar to previous HIIT interventions in participants with T2D or metabolic syndrome reductions in fat mass (Stensvold et al., 2010; Terada et al., 2013; Mitranun et al., 2014; Mohr et al., 2014) and plasma triglycerides (Freese et al., 2015) also contributed to the lowering of cardio-metabolic risk and this was associated with reductions in VLDL cholesterol. The mechanism for decreased plasma lipids is unclear, though improved adipose tissue health is likely to be a factor. Our observation of altered adipokines - increased HMW adiponectin and reduced plasma resistin - support the possible contribution of improved adipose tissue function leading to improved lipid profiles and overall metabolic health. Enhanced whole body fat oxidation may also have contributed to reductions in cardiometabolic risk. Increased fat oxidation is a common adaptation to endurance exercise (Holloszy & Booth, 1976; Henriksson, 1977; Calles-Escandon et al., 1996; Lund et al., 2017) and our data suggests that this adaptation is preserved after F-HIT. This increase in fat oxidation may be attributable, at least in part, to the increases in HMW adiponectin. HMW adiponectin is a known insulin sensitizer and increases oxidative capacity by signaling through Sirt1 and AMPK, key cell mediators of mitochondrial biogenesis in muscle that contribute to increased mitochondrial mass (Iwabu et al., 2010). Indeed the consistent relationship between HMW-adiponectin, fat oxidation, and insulin resistance, both in cross-sectional studies (Cnop et al., 2003) and following exercise training programs (Kelly et al., 2012; Navaneethan et al., 2015), a relationship that is replicated in the current study, support the hypothesis that mitochondrial adaptations are central to the reductions in insulin resistance and cardio-metabolic risk in individuals with and without T2D, though the exact mechanism remains elusive (Holloszy, 2009; Dela & Helge, 2013).
In summary, this proof of principle study suggests that F-HIT, performed under controlled supervised conditions, is an effective means of improving insulin sensitivity and reducing cardiometabolic risk in individuals with T2D. Moreover, F-HIT may provide a time efficient method for reducing the metabolic burden of T2D.
NEW FINDINGS.
What is the central question of this study?
The goal of this study was to examine whether short-duration, high-intensity exercise training that it combines functional aerobic and resistance exercises into training sessions lasting 8-20 minute could benefit individuals with type 2 diabetes.
What is the main finding and its importance?
Here we show that Functional High Intensity Training improves insulin sensitivity and reduces cardiometabolic risk in individuals with type 2 diabetes. These data suggest that this type of exercise training may be an effective exercise mode for managing T2D. The increase in insulin sensitivity addresses a key defect in T2D.
Acknowledgments
We thank the research volunteers for outstanding dedication and effort, the staff of the Clinical Research Unit, and the technical staff and students who helped with the implementation of the study and assisted with data collection. The staff and coaches at Great Lakes CrossFit in Bedford Heights, Ohio, particularly Patrick Flannery, for the outstanding work in coaching the research participants through the exercise program.
GRANTS
This research was supported by an investigator-initiated grant from CrossFit, Inc.™ (JPK), Cleveland Clinic research support award RPC 2013-1010, and National Institutes of Health, National Center for Research Resources Grant UL1RR024989.
Footnotes
Competing Interests
Julie Foucher is an elite CrossFit athlete and has received consulting fees from CrossFit. S Nieuwoudt, CE Fealy, AR Scelsi, SK Malin, M Pagadala, L Cruz, M Li, M Rocco, B Burguera, and JP Kirwan have no conflicts of interest relative to this work. CrossFit, Inc™ provided no input to the study design, data analysis, interpretation, or writing of this article.
AUTHOR CONTRIBUTIONS
Author contributions: C.E.F., J.A.F., A.R.S., S.K.M., and J.P.K. conception and design of research; C.E.F., S.N., A.R.S, M.P., L.C., and M.L. performed experiments; C.E.F., M.R., B.B., and J.P.K. analyzed data; C.E.F. and J.P.K. interpreted results of experiments; C.E.F. prepared figures; C.E.F. drafted manuscript; All authors edited and revised manuscript; All authors approved final version of manuscript.
References
- American Diabetes Association. Standards of medical care in diabetes–2014. Diabetes Care. 2014;37(Suppl 1):S14–80. doi: 10.2337/dc14-S014. [DOI] [PubMed] [Google Scholar]
- Ary DV, Toobert D, Wilson W, Glasgow RE. Patient perspective on factors contributing to nonadherence to diabetes regimen. Diabetes Care. 1986;9:168–172. doi: 10.2337/diacare.9.2.168. [DOI] [PubMed] [Google Scholar]
- Baba NH, Sawaya S, Torbay N, Habbal Z, Azar S, Hashim SA. High protein vs high carbohydrate hypoenergetic diet for the treatment of obese hyperinsulinemic subjects. Int J Obes Relat Metab Disord. 1999;23:1202–1206. doi: 10.1038/sj.ijo.0801064. [DOI] [PubMed] [Google Scholar]
- Boule NG, Haddad E, Kenny GP, Wells GA, Sigal RJ. Effects of exercise on glycemic control and body mass in type 2 diabetes mellitus: a meta-analysis of controlled clinical trials. JAMA. 2001;286:1218–1227. doi: 10.1001/jama.286.10.1218. [DOI] [PubMed] [Google Scholar]
- Brehm BJ, Spang SE, Lattin BL, Seeley RJ, Daniels SR, D’Alessio DA. The role of energy expenditure in the differential weight loss in obese women on low-fat and low-carbohydrate diets. J Clin Endocrinol Metab. 2005;90:1475–1482. doi: 10.1210/jc.2004-1540. [DOI] [PubMed] [Google Scholar]
- Butcher SJ, Neyedly TJ, Horvey KJ, Benko CR. Do physiological measures predict selected CrossFit((R)) benchmark performance? Open Access J Sports Med. 2015;6:241–247. doi: 10.2147/OAJSM.S88265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Calles-Escandon J, Gordan MI, O’Connell M, Sreekumaran Nair K, Danforth E., Jr Exercise increases fat oxidation at rest unrelated to changes in energy balance or lipolysis. Am J Physiology. 1996;270:E1009–E1014. doi: 10.1152/ajpendo.1996.270.6.E1009. [DOI] [PubMed] [Google Scholar]
- Clark DO. Physical activity efficacy and effectiveness among older adults and minorities. Diabetes Care. 1997;20:1176–1182. doi: 10.2337/diacare.20.7.1176. [DOI] [PubMed] [Google Scholar]
- Cnop M, Havel PJ, Utzschneider KM, Carr DB, Sinha MK, Boyko EJ, Retzlaff BM, Knopp RH, Brunzell JD, Kahn SE. Relationship of adiponectin to body fat distribution, insulin sensitivity and plasma lipoproteins: evidence for independent roles of age and sex. Diabetologia. 2003;46:459–469. doi: 10.1007/s00125-003-1074-z. [DOI] [PubMed] [Google Scholar]
- Colberg SR, Sigal RJ, Yardley JE, Riddell MC, Dunstan DW, Dempsey PC, Horton ES, Castorino K, Tate DF. Physical Activity/Exercise and Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care. 2016;39:2065–2079. doi: 10.2337/dc16-1728. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dela F, Helge JW. Insulin resistance and mitochondrial function in skeletal muscle. Int J Biochem Cell Biol. 2013;45:11–15. doi: 10.1016/j.biocel.2012.09.019. [DOI] [PubMed] [Google Scholar]
- Dunstan DW, Daly RM, Owen N, Jolley D, De Courten M, Shaw J, Zimmet P. High-intensity resistance training improves glycemic control in older patients with type 2 diabetes. Diabetes Care. 2002;25:1729–1736. doi: 10.2337/diacare.25.10.1729. [DOI] [PubMed] [Google Scholar]
- Fenicchia LM, Kanaley JA, Azevedo JL, Jr, Miller CS, Weinstock RS, Carhart RL, Ploutz-Snyder LL. Influence of resistance exercise training on glucose control in women with type 2 diabetes. Metabolism. 2004;53:284–289. doi: 10.1016/j.metabol.2003.10.007. [DOI] [PubMed] [Google Scholar]
- Freese EC, Gist NH, Acitelli RM, McConnell WJ, Beck CD, Hausman DB, Murrow JR, Cureton KJ, Evans EM. Acute and chronic effects of sprint interval exercise on postprandial lipemia in women at-risk for the metabolic syndrome. J Appl Physiol (1985) 2015;118:872–879. doi: 10.1152/japplphysiol.00380.2014. [DOI] [PubMed] [Google Scholar]
- Gibala MJ. High-intensity interval training: a time-efficient strategy for health promotion? Curr Sports Med Rep. 2007;6:211–213. [PubMed] [Google Scholar]
- Gibala MJ, Little JP, Macdonald MJ, Hawley JA. Physiological adaptations to low-volume, high-intensity interval training in health and disease. J Physiol. 2012;590:1077–1084. doi: 10.1113/jphysiol.2011.224725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grace F, Herbert P, Elliott AD, Richards J, Beaumont A, Sculthorpe NF. High intensity interval training (HIIT) improves resting blood pressure, metabolic (MET) capacity and heart rate reserve without compromising cardiac function in sedentary aging men. Exp Gerontol. 2017 doi: 10.1016/j.exger.2017.05.010. [DOI] [PubMed] [Google Scholar]
- Green AJ, Bazata DD, Fox KM, Grandy S. Health-related behaviours of people with diabetes and those with cardiometabolic risk factors: results from SHIELD. Int J Clin Pract. 2007;61:1791–1797. doi: 10.1111/j.1742-1241.2007.01588.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hansen D, Dendale P, Jonkers RA, Beelen M, Manders RJ, Corluy L, Mullens A, Berger J, Meeusen R, van Loon LJ. Continuous low- to moderate-intensity exercise training is as effective as moderate- to high-intensity exercise training at lowering blood HbA(1c) in obese type 2 diabetes patients. Diabetologia. 2009;52:1789–1797. doi: 10.1007/s00125-009-1354-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heinrich KM, Patel PM, O’Neal JL, Heinrich BS. High-intensity compared to moderate-intensity training for exercise initiation, enjoyment, adherence, and intentions: an intervention study. BMC Public Health. 2014;14:789. doi: 10.1186/1471-2458-14-789. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Henriksson J. Training induced adaptation of skeletal muscle and metabolism during submaximal exercise. J Physiol. 1977;270:661–675. doi: 10.1113/jphysiol.1977.sp011974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holloszy JO. Skeletal muscle “mitochondrial deficiency” does not mediate insulin resistance. Am J Clin Nutr. 2009;89:463S–466S. doi: 10.3945/ajcn.2008.26717C. [DOI] [PubMed] [Google Scholar]
- Holloszy JO, Booth FW. Biochemical adaptations to endurance exercise in muscle. Ann Rev Physiol. 1976;38:273–291. doi: 10.1146/annurev.ph.38.030176.001421. [DOI] [PubMed] [Google Scholar]
- Holloszy JO, Schultz J, Kusnierkiewicz J, Hagberg JM, Ehsani AA. Effects of exercise on glucose tolerance and insulin resistance. Acta Med Scand (Suppl) 1986;711:55–65. doi: 10.1111/j.0954-6820.1986.tb08932.x. [DOI] [PubMed] [Google Scholar]
- Howatson G, Van Someren K, Hortobagyi T. Repeated bout effect after maximal eccentric exercise. Int J Sports Med. 2007;28:557–563. doi: 10.1055/s-2007-964866. [DOI] [PubMed] [Google Scholar]
- Inzucchi SE, Bergenstal RM, Buse JB, Diamant M, Ferrannini E, Nauck M, Peters AL, Tsapas A, Wender R, Matthews DR. Management of hyperglycaemia in type 2 diabetes: a patient-centered approach. Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) Diabetologia. 2012;55:1577–1596. doi: 10.1007/s00125-012-2534-0. [DOI] [PubMed] [Google Scholar]
- Iwabu M, Yamauchi T, Okada-Iwabu M, Sato K, Nakagawa T, Funata M, Yamaguchi M, Namiki S, Nakayama R, Tabata M, Ogata H, Kubota N, Takamoto I, Hayashi YK, Yamauchi N, Waki H, Fukayama M, Nishino I, Tokuyama K, Ueki K, Oike Y, Ishii S, Hirose K, Shimizu T, Touhara K, Kadowaki T. Adiponectin and AdipoR1 regulate PGC-1alpha and mitochondria by Ca(2+) and AMPK/SIRT1. Nature. 2010;464:1313–1319. doi: 10.1038/nature08991. [DOI] [PubMed] [Google Scholar]
- Jelleyman C, Yates T, O’Donovan G, Gray LJ, King JA, Khunti K, Davies MJ. The effects of high-intensity interval training on glucose regulation and insulin resistance: a meta-analysis. Obes Rev. 2015;16:942–961. doi: 10.1111/obr.12317. [DOI] [PubMed] [Google Scholar]
- Karstoft K, Christensen CS, Pedersen BK, Solomon TP. The acute effects of interval- Vs continuous-walking exercise on glycemic control in subjects with type 2 diabetes: a crossover, controlled study. J Clin Endocrinol Metab. 2014;99:3334–3342. doi: 10.1210/jc.2014-1837. [DOI] [PubMed] [Google Scholar]
- Karstoft K, Winding K, Knudsen SH, Nielsen JS, Thomsen C, Pedersen BK, Solomon TP. The effects of free-living interval-walking training on glycemic control, body composition, and physical fitness in type 2 diabetic patients: a randomized, controlled trial. Diabetes Care. 2013;36:228–236. doi: 10.2337/dc12-0658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kelly KR, Blaszczak A, Haus JM, Patrick-Melin A, Fealy CE, Solomon TP, Kalinski MI, Kirwan JP. A 7-d exercise program increases high-molecular weight adiponectin in obese adults. Med Sci Sports Exerc. 2012;44:69–74. doi: 10.1249/MSS.0b013e318228bf85. [DOI] [PubMed] [Google Scholar]
- Kirwan J, Sacks J, Nieuwoudt S. The essential role of Exercise in the management of type 2 diabetes. Cleveland Clinic Journal of Medicine. 2017;84 doi: 10.3949/ccjm.84.s1.03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kirwan JP, Hickner RC, Yarasheski KE, Kohrt WM, Wiethop BV, Holloszy JO. Eccentric exercise induces transient insulin resistance in healthy individuals. J Appl Physiol. 1992;72:2197–2202. doi: 10.1152/jappl.1992.72.6.2197. [DOI] [PubMed] [Google Scholar]
- Kirwan JP, Solomon TP, Wojta DM, Staten MA, Holloszy JO. Effects of 7 days of exercise training on insulin sensitivity and responsiveness in type 2 diabetes mellitus. Am J Physiol Endocrinol Metab. 2009;297:E151–156. doi: 10.1152/ajpendo.00210.2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Korkiakangas EE, Alahuhta MA, Laitinen JH. Barriers to regular exercise among adults at high risk or diagnosed with type 2 diabetes: a systematic review. Health Promot Int. 2009;24:416–427. doi: 10.1093/heapro/dap031. [DOI] [PubMed] [Google Scholar]
- Larsen C, Jensen MP. Rhabdomyolysis in a well-trained woman after unusually intense exercise. Ugeskr Laeger. 2014;176 [PubMed] [Google Scholar]
- Lindenstrom E, Boysen G, Nyboe J. Influence of systolic and diastolic blood pressure on stroke risk: a prospective observational study. Am J Epidemiol. 1995;142:1279–1290. doi: 10.1093/oxfordjournals.aje.a117595. [DOI] [PubMed] [Google Scholar]
- Lund J, Rustan AC, Lovsletten NG, Mudry JM, Langleite TM, Feng YZ, Stensrud C, Brubak MG, Drevon CA, Birkeland KI, Kolnes KJ, Johansen EI, Tangen DS, Stadheim HK, Gulseth HL, Krook A, Kase ET, Jensen J, Thoresen GH. Exercise in vivo marks human myotubes in vitro: Training-induced increase in lipid metabolism. PLoS One. 2017;12:e0175441. doi: 10.1371/journal.pone.0175441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Malin SK, Finnegan S, Fealy CE, Filion J, Rocco MB, Kirwan JP. beta-Cell dysfunction is associated with metabolic syndrome severity in adults. Metab Syndr Relat Disord. 2014;12:79–85. doi: 10.1089/met.2013.0083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McRae G, Payne A, Zelt JG, Scribbans TD, Jung ME, Little JP, Gurd BJ. Extremely low volume, whole-body aerobic-resistance training improves aerobic fitness and muscular endurance in females. Appl Physiol Nutr Metab. 2012;37:1124–1131. doi: 10.1139/h2012-093. [DOI] [PubMed] [Google Scholar]
- Mitranun W, Deerochanawong C, Tanaka H, Suksom D. Continuous vs interval training on glycemic control and macro- and microvascular reactivity in type 2 diabetic patients. Scand J Med Sci Sports. 2014;24:e69–76. doi: 10.1111/sms.12112. [DOI] [PubMed] [Google Scholar]
- Mohr M, Nordsborg NB, Lindenskov A, Steinholm H, Nielsen HP, Mortensen J, Weihe P, Krustrup P. High-intensity intermittent swimming improves cardiovascular health status for women with mild hypertension. Biomed Res Int. 2014;2014:728289. doi: 10.1155/2014/728289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mourier A, Gautier JF, De Kerviler E, Bigard AX, Villette JM, Garnier JP, Duvallet A, Guezennec CY, Cathelineau G. Mobilization of visceral adipose tissue related to the improvement in insulin sensitivity in response to physical training in NIDDM. Effects of branched-chain amino acid supplements. Diabetes Care. 1997;20:385–391. doi: 10.2337/diacare.20.3.385. [DOI] [PubMed] [Google Scholar]
- Murawska-Cialowicz E, Wojna J, Zuwala-Jagiello J. Crossfit training changes brain-derived neurotrophic factor and irisin levels at rest, after wingate and progressive tests, and improves aerobic capacity and body composition of young physically active men and women. J Physiol Pharmacol. 2015;66:811–821. [PubMed] [Google Scholar]
- Navaneethan SD, Fealy CE, Scelsi AC, Arrigain S, Malin SK, Kirwan JP. A Trial of Lifestyle Modification on Cardiopulmonary, Inflammatory, and Metabolic Effects among Obese with Chronic Kidney Disease. Am J Nephrol. 2015;42:274–281. doi: 10.1159/000441155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nieuwoudt S, Fealy CE, Foucher JA, Scelsi AR, Malin SK, Pagadala MR, Rocco M, Burguera B, Kirwan JP. Functional High Intensity Training Improves Pancreatic beta-cell Function in Adults with Type 2 Diabetes. Am J Physiol Endocrinol Metab. 2017 doi: 10.1152/ajpendo.00407.2016. ajpendo 00407 02016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peronnet F, Massicotte D. Table of nonprotein respiratory quotient: an update. Can J Sport Sci. 1991;16:23–29. [PubMed] [Google Scholar]
- Ramos JS, Dalleck LC, Borrani F, Beetham KS, Wallen MP, Mallard AR, Clark B, Gomersall S, Keating SE, Fassett RG, Coombes JS. Low-Volume High-Intensity Interval Training Is Sufficient to Ameliorate the Severity of Metabolic Syndrome. Metab Syndr Relat Disord. 2017;15:319–328. doi: 10.1089/met.2017.0042. [DOI] [PubMed] [Google Scholar]
- Ryan AS. Exercise in aging: its important role in mortality, obesity and insulin resistance. Aging health. 2010;6:551–563. doi: 10.2217/ahe.10.46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saris WH, Astrup A, Prentice AM, Zunft HJ, Formiguera X, Verboeket-van de Venne WP, Raben A, Poppitt SD, Seppelt B, Johnston S, Vasilaras TH, Keogh GF. Randomized controlled trial of changes in dietary carbohydrate/fat ratio and simple vs complex carbohydrates on body weight and blood lipids: the CARMEN study. The Carbohydrate Ratio Management in European National diets. Int J Obes Relat Metab Disord. 2000;24:1310–1318. doi: 10.1038/sj.ijo.0801451. [DOI] [PubMed] [Google Scholar]
- Snowling NJ, Hopkins WG. Effects of different modes of exercise training on glucose control and risk factors for complications in type 2 diabetic patients: a meta-analysis. Diabetes Care. 2006;29:2518–2527. doi: 10.2337/dc06-1317. [DOI] [PubMed] [Google Scholar]
- Solomon TP, Haus JM, Kelly KR, Cook MD, Filion J, Rocco M, Kashyap SR, Watanabe RM, Barkoukis H, Kirwan JP. A low-glycemic index diet combined with exercise reduces insulin resistance, postprandial hyperinsulinemia, and glucose-dependent insulinotropic polypeptide responses in obese, prediabetic humans. Am J Clin Nutr. 2010;92:1359–1368. doi: 10.3945/ajcn.2010.29771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Solomon TP, Malin SK, Karstoft K, Knudsen SH, Haus JM, Laye MJ, Pedersen M, Pedersen BK, Kirwan JP. Determining pancreatic beta-cell compensation for changing insulin sensitivity using an oral glucose tolerance test. Am J Physiol Endocrinol Metab. 2014;307:E822–829. doi: 10.1152/ajpendo.00269.2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Srikanthan P, Karlamangla AS. Relative muscle mass is inversely associated with insulin resistance and prediabetes. Findings from the third National Health and Nutrition Examination Survey. J Clin Endocrinol Metab. 2011;96:2898–2903. doi: 10.1210/jc.2011-0435. [DOI] [PubMed] [Google Scholar]
- Stensvold D, Tjonna AE, Skaug EA, Aspenes S, Stolen T, Wisloff U, Slordahl SA. Strength training versus aerobic interval training to modify risk factors of metabolic syndrome. J Appl Physiol (1985) 2010;108:804–810. doi: 10.1152/japplphysiol.00996.2009. [DOI] [PubMed] [Google Scholar]
- Terada T, Friesen A, Chahal BS, Bell GJ, McCargar LJ, Boule NG. Feasibility and preliminary efficacy of high intensity interval training in type 2 diabetes. Diabetes Res Clin Pract. 2013;99:120–129. doi: 10.1016/j.diabres.2012.10.019. [DOI] [PubMed] [Google Scholar]
- Thompson WR. Worldwide Survey of Fitness Trends for 2015 What’s Driving the Market. Acsms Health & Fitness Journal. 2014;18:8–17. [Google Scholar]
- Umpierre D, Ribeiro PA, Kramer CK, Leitao CB, Zucatti AT, Azevedo MJ, Gross JL, Ribeiro JP, Schaan BD. Physical activity advice only or structured exercise training and association with HbA1c levels in type 2 diabetes: a systematic review and meta-analysis. JAMA. 2011;305:1790–1799. doi: 10.1001/jama.2011.576. [DOI] [PubMed] [Google Scholar]
- Weston KS, Wisloff U, Coombes JS. High-intensity interval training in patients with lifestyle-induced cardiometabolic disease: a systematic review and meta-analysis. Br J Sports Med. 2014;48:1227–1234. doi: 10.1136/bjsports-2013-092576. [DOI] [PubMed] [Google Scholar]
- Wijndaele K, Beunen G, Duvigneaud N, Matton L, Duquet W, Thomis M, Lefevre J, Philippaerts RM. A continuous metabolic syndrome risk score: utility for epidemiological analyses. Diabetes Care. 2006;29:2329. doi: 10.2337/dc06-1341. [DOI] [PubMed] [Google Scholar]
- Zhao G, Ford ES, Li C, Mokdad AH. Compliance with physical activity recommendations in US adults with diabetes. Diabet Med. 2008;25:221–227. doi: 10.1111/j.1464-5491.2007.02332.x. [DOI] [PubMed] [Google Scholar]