

Abstract
BACKGROUND:
Apitherapy is the medical use of honey bee products, “honey, propolis, royal jelly, bee wax, and bee venom to relieve human ailments. Propolis is one of the most well-documented products derived from the honeybee and has always played an important role in traditional folk medicine.
AIM:
The aim was to justify the consideration of Aloe Vera as an effective remedy for the treatment of psoriasis.
METHODS:
The study follows (857) patients (354 females, 503 males) with a mean age range from (9 - 62) years, affected with moderate to severe psoriasis in palms and foot soles treated by a combination mixture of propolis and Aloe in the form of an ointment (Aloreed) and Beauty reed cream. The treatment duration was for 12 weeks. Results were evaluated by using clinical, histological and statistical parameters.
RESULTS:
After the 12 - week treatment, we observed an 86% overall response rate from which 62% showed excellent results and 24% showed good results, therefore proving the efficiency in the use of the mixture of propolis 50% and aloe vera 3% as topically applied ointment in the treatment of mild to moderate psoriasis
CONCLUSION:
Patients who have palmoplantar psoriasis, who were treated with a topically applied mixture of propolis (50%) and aloe vera (3%), have shown noteworthy improvement thus proving the efficiency of propolis and aloe vera in the treatment of mild to moderate psoriasis.
Keywords: Psoriasis, Apitherapy, Skin disease, Natural therapy, Propolis
Introduction
Psoriasis is a genetic inflammatory and proliferative skin disease characterised by chronic, sharply bordered, dull - red, scaly plaques appeared on the skin and particularly on the extensor prominences and in the scalp area [1]. On the palms and soles, psoriasis may present as scaly white patches; a fine silvery scale can be evoked by scratching, as less well – defined plaques resembling lichen simplex or hyperkeratotic eczema - or as a pustulosis (chronic palmoplantar pustular psoriasis). A strong association between body mass index and psoriasis was shown [2].
There is no satisfactory or effective cure for psoriasis. However a variety of therapeutic modalities have yielded limited efficacy with frequent side effects. Available treatments include both local and systemic ones. In vivo and in vitro data prove the effectiveness of cytokines taken in low - doses [3] and antioxidants [4]. Complementary therapy based on psychotherapeutic approaches has also shown some efficacy [5].
Apitherapy is a therapy that uses hive products (e.g. propolis) for medical and pharmacological purposes [6]. It was found that propolis has versatile activities including physiological, antibacterial, antiviral, fungicide, local anaesthetic, antiulcer, immunostimulant and recently discovered cytostatic activities. The principal components of propolis are flavonoids of group 5 (betulinol, quercetin, isovanillin), cafeic acids, unsaturated aromatic acid, and ferulic acids. Propolis is a very stable substance and has equal composition regardless of the geographic areas where it was produced. The composition of propolis indicates high antioxidant activity, and thus the substance can be investigated for the treatment of psoriasis.
Aloe vera is a plant that grows widely in the Egyptian desert. Its mucilaginous gel has been used in folk medicine for its effectiveness in itching, hair loss and burns. Aloe vera has also been proven to be effective in cutaneous wound healing [7]. Research has shown that active agents have considerable analgesic, antipruritic, wound healing and anti-inflammatory properties [8].
The aim was to justify the consideration of Aloe Vera as an effective remedy for the treatment of psoriasis.
Patients and Methods
The study follows (857) patients (354 females & 503 males) with a mean age range from (9 - 62) years, affected with a clinical diagnosis of mild to moderate psoriasis of palms and soles.
The subjects, afferent to the in the centre of dermatology in Heliopolis (Cairo - Egypt), were randomly allocated. Written consent was approved by all patients under this clinical trial, Patient information and progress was thoroughly documented during the study. Both treatment and follow - up was taken place in the centre of dermatology in Heliopolis from July 2006 to August 2008.
During the start and toward the end of the study skin biopsies were taken and stained with hematoxylin and eosin (H&E) for the evaluation of acanthosis, parakeratosis, thinning capillary dilatation, and inflammatory infiltration. A leading pharmaceutical company was responsible for preparation of the mixture (Propolis 50% with Aloe 3%) as an ointment [6].
Pre-treatment biopsy
A punch biopsy was taken before application of the treatment and stained by H&E for histological examination.
Figure 1.
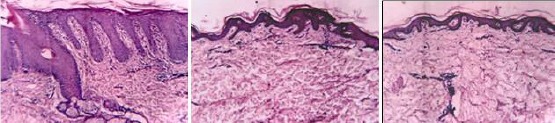
Pre and post Treatment Histology (Biopsy Rt.Sole)
Treatment application
Patients were advised to rub the ointment into psoriatic palms and soles twice daily for 4 - 12 weeks.
Follow up
On a weekly basis reexamination and evaluation of the treated areas were done to control any side effects and to analyse the degree of patient satisfaction or inconvenience, follow up lasted for 12 weeks.
Post-treatment biopsy
At the end of the study, a punch biopsy was taken from the treated area to evaluate the efficacy of the treatment.
Post-treatment assessment
Assessment of the trial therapy depended on clinical state, photography and histopathology and was classified as follows:
Excellent response: when all psoriatic lesions disappeared, and skin became nearly normal (No erythema, no infiltration or desquamation of skin).
Good response: when some of the lesions disappeared.
Weak response: when no marked improvement was noted.
No response: when no improvement was seen.
For a standard method of clinical assessment of patients, Psoriasis Area and Severity Index (PASI score) was used. This clinical rating system assesses the area of the body affected by the intensity of the main symptoms.
To measure the % reduction of PASI Score, we applied the following equation:
% reduction of PASI score = Baseline PASI x PASI at the end of the program X 100 Baseline PASI
Result
After the 12 - week treatment, we observed an 86% overall response rate from which 62% showed excellent results and 24% showed good results, therefore proving the efficiency in the use of the mixture of propolis 50% and aloe vera 3% as topically applied ointment in the treatment of mild to moderate psoriasis [6].
Figure 2.

Pre (left) and post (right) 3 months of treatment
Table 1.
Comparison of the mean effective and non-effective
| Variable | Effective Mean | Non-Effective Mean | t | P |
|---|---|---|---|---|
| ± SD | ± SD | |||
| N = 625 | N = 232 | ** | ||
| % -reduction | 0.73 | 0.28 | 5.57 | < 0.01 |
| ± 0.26 | ± 0.033 | |||
H. is significant.
Table 2.
Comparison of the mean excellent and good effect
| Variable | Excellent Effective Mean | Good Effective Mean | t | P |
|---|---|---|---|---|
| ± SD | ± SD | |||
| N = 531 | N = 205 | ** | ||
| % -reduction | 0.87 | 0.38 | 38.24 | < 0.01 |
H. is significant.
Punch biopsy was taken before application of the treatment and stained to be examined histologically.
Within the typical plaque, psoriatic epidermis shows marked epidermal acanthosis, hyperkeratosis, and elongation of capillaries, and presence of Munro’s microabscesses (to the left).
Table 3.
Results of treatment
| Result | Total | |||||
|---|---|---|---|---|---|---|
| Excellent | Good | No Response | Weak | |||
| Effect | Count % | 531 | 206 | - | - | 737 |
| 72.1% | 27.9% | 100% | ||||
| Non Effect | Count % | - | - | 68 | 52 | 120 |
| 4% | 42.9% | 100% | ||||
| Total | Count % | 531 | 206 | 68 | 52 | 857 |
| 62% | 24% | 4% | 6% | 100% | ||
Chi Square Test =857 **; **H sig.
Parakeratosis changed to orthokeratosis, acanthosis decreased, the rete ridges became shorter, and Munro’s microabscesses disappeared (to the right).
Table 4.
Results of treatment % reduction of the PASI score
| %- a reduction of PASI score | Cases | Per cent |
|---|---|---|
| Effective 33% ↓↓ | 737 | 86% |
| Non Effective 33% ↑↑ | 120 | 14% |
| Total | 857 | 100% |
In conclusion, patients who have palmoplantar psoriasis, who were treated with a topically applied mixture of propolis (50%) and aloe vera (3%), have shown noteworthy improvement thus proving the efficiency of propolis and aloe vera in the treatment of mild to moderate psoriasis.
Table 5.
Results of treatment - effectiveness
| Cases | Per cent | ||
|---|---|---|---|
| Effective | Excellent | 531 | 62% |
| Good | 206 | 24% | |
| Non-Effective | Weak | 52 | 6% |
| No Response | 68 | 8% | |
| Total | 857 | 100% |
Footnotes
Funding: This research did not receive any financial support
Competing Interests: The authors have declared that no competing interests exist
References
- 1.Lotti T, Hercogova J, Prignano F. The concept of psoriatic disease: can cutaneous psoriasis any longer be separated by the systemic comorbidities? Dermatol Ther. 2010;23(2):119–22. doi: 10.1111/j.1529-8019.2010.01305.x. https://doi.org/10.1111/j.1529-8019.2010.01305.x PMid:20415818. [DOI] [PubMed] [Google Scholar]
- 2.Hercogová J, Ricceri F, Tripo L, Lotti T, Prignano F. Psoriasis and body mass index. Dermatol Ther. 2010;23(2):152–4. doi: 10.1111/j.1529-8019.2010.01309.x. https://doi.org/10.1111/j.1529-8019.2010.01309.x PMid:20415822. [DOI] [PubMed] [Google Scholar]
- 3.Barygina V, Becatti M, Lotti T, Taddei N, Fiorillo C. J Low dose cytokines reduce oxidative stress in primary lesional fibroblasts obtained from psoriatic patients. Dermatol Sci. 2016;83(3):242–4. doi: 10.1016/j.jdermsci.2016.06.002. https://doi.org/10.1016/j.jdermsci.2016.06.002 PMid:27317477. [DOI] [PubMed] [Google Scholar]
- 4.Barygina V, Becatti M, Soldi G, Prignano F, Lotti T, Nassi P, Wright D, Taddei N, Fiorillo C. Altered redox status in the blood of psoriatic patients: involvement of NADPH oxidase and role of anti-TNF-αtherapy. Redox Rep. 2013;18(3):100–6. doi: 10.1179/1351000213Y.0000000045. https://doi.org/10.1179/1351000213Y.0000000045 PMid:23601139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Capella GL1, Finzi AF. Complementary therapy for psoriasis. Dermatol Ther. 2003;16(2):164–74. doi: 10.1046/j.1529-8019.2003.01625.x. https://doi.org/10.1046/j.1529-8019.2003.01625.x. [DOI] [PubMed] [Google Scholar]
- 6.El-Gammal A. In Medical environmental science: Apitherapy as a new approach in the treatment of psoriasis. African Journal of Dermatology. 2006:6–2. [Google Scholar]
- 7.Hashemi SA, Madani SA, Abediankenari S. The Review on Properties of Aloe Vera in Healing of Cutaneous Wounds. BioMed Research International. 2015:714216. doi: 10.1155/2015/714216. https://doi.org/10.1155/2015/714216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Duke EE. Treatment of skin conditions: Dermatology - an Illustrated Guide. Canadian Medical Association Journal. 1985;133(12):1254. [Google Scholar]