

Abstract
Background
The association between fine particulate matter (PM2.5) and lung cancer (LC) mortality in China is limited. The Beijing‐Tianjin‐Hebei region is infamous for serious air pollution. Seven of the top 10 cities with the worst air quality are located in Hebei Province. Thus, we explored the effect of 10 years of PM2.5 on the LC mortality rate in Hebei Province.
Methods
We quantified associations between LC mortality and PM2.5 and estimated the LC mortality burden attributed to PM2.5 with predicted county level LC deaths in 2014.
Results
The 10‐year PM2.5 LC mortality associations were non‐linear, with thresholds of 63 μg/m3 overall, 69 μg/m3 for men, 68 μg/m3 for women, 66 μg/m3 for those aged 30–64 years, and 62 μg/m3 for those aged ≥ 65 years. The relative risks for these groups were 1.09 (95% confidence interval [CI] 1.08–1.10), 1.06 (95% CI 1.03–1.10), 1.20 (95% CI 1.10–1.26), 1.07 (95% CI 1.05–1.11), and 1.10 (95% CI: 1.07–1.13), respectively. There were 2525 (95% CI 2265–2780) LC deaths attributed to 10‐year PM2.5 in 2014, at fractions of 8.3% (95% CI 7.4–9.1%) overall, 5.7% (95% CI 2.8–9.4%) for men, 16.7% (95% CI: 8.3–21.6%) for women, 6.5% (95% CI 4.7–10.3%) for those aged 30–64 years, and 9.1% (95% CI 6.4–11.5%) for those aged ≥ 65 years.
Conclusion
Our results suggest that a reduction in the PM2.5 exposure levels below thresholds would prevent a substantial number of LC deaths in Hebei Province.
Keywords: Air pollution, attributed fraction, fine particulate matter, generalized additive model, lung cancer mortality
Introduction
Lung cancer (LC) has the highest morbidity and mortality rate of all malignant tumors.1 Globocan 2012 reported an estimated 1.8 million new lung cancer cases in 2012 (12.9% of the total) and 1.59 million deaths, accounting for almost one in five cancer deaths (19.4% of the total) in the world.2 The latest National Central Cancer Registry (NCCR) data shows that LC is the leading cause of cancer incidence and death in China (733 000 new cases with an incidence of 53.86/100000; 591 000 new cases with a mortality rate of 43.41/100000).3 Hebei Province is located in the north of China, and accounts for approximately 6% of the national population. LC was also the leading cause of cancer death in Hebei province (27 000 new cases with a mortality rate of 37.14/100.000).4
Exposure to ambient air pollution increases mortality and morbidity and shortens life expectancy. The Global Burden of Diseases, Injuries, and Risk Factors Study 2015 (GBD 2015) identified air pollution as a leading cause of global disease burden, especially in low and middle‐income countries.5 Particle mass with an aerodynamic diameter < 2.5 μm (PM2.5) is the most consistent and robust predictor of mortality.6, 7 Long‐term exposure to PM2.5 has been associated with increased mortality, especially from cardiovascular and respiratory diseases.8 An increasing number of studies have reported positive associations of PM2.5 with LC risk.9, 10 Globally, it is estimated that 283 000 deaths from LC in 2015 could be attributed to exposure to fine particulate matter air pollution alone.11
Studies have examined the association between air pollution and LC mortality in China.12 With the rapid economic growth and increased urbanization of rural areas over the past decades, severe and widespread air pollution in China has become a major public health and social issue, attracting global attention.13 Notably, the North China Plain experiences poor air conditions and persistent fog and haze.13, 14 Increasing concern over the adverse influences of PM2.5 on human health has seen the promotion of health awareness among citizens. Previous studies have examined the association between PM2.5 and mortality in several Chinese cities, including Shanghai, Guangzhou, Xi'an, and Hong Kong;15, 16, 17, 18 however, reports on Hebei Province are limited. Thus, we examined the association between the accumulated 10‐year PM2.5 exposure with LC mortality in Hebei Province.
Methods
Data collection
Observed data of lung cancer deaths
To examine the associations between PM2.5 and LC mortality, county level annual data on LC deaths were collected from the Hebei Cancer Registration Center of China, which is responsible for the collection, evaluation, and publication of cancer statistics from population‐based cancer registries in Hebei Province each year. We selected 22 cancer registries from 2010 and 2014 for the study, based on the integrity and quality of LC mortality data. LC deaths were classified using the International Classification of Disease for Oncology, version 10 (ICD10). Detailed information on each case, including year and age at diagnosis, gender, and community type (rural or urban area), was collected. LC deaths were stratified into 12 age groups for each community: 30–34 years, 35–39, 40–44, 45–49, 50–54, 55–59, 60–64, 65–69, 70–74, 75–79, 80–84, and 85 + years. Population information was collected from the local statistical bureau or household registry department in the local public security bureau. We limited analyses to persons aged at least 30 years as few LC deaths occur below this age.
PM2.5 data
We obtained data for the annual mean PM2.5 during the years 2001 to 2014 from a previous publication.19 The annual mean exposure to PM2.5 was estimated at 0·1 × 0·1° (~11 km × 11 km at the equator) resolution using estimates from satellites combined with Aerosol Optical Depth retrievals from Moderate Resolution Imaging Spectroradiometer, Multi‐angle Imaging Spectroradiometer, and Sea‐viewing Wide Field‐of‐view Sensor instruments with the GEOS‐Chem chemical transport model (NASA, Washington, DC, USA), which were subsequently calibrated by geographically weighted regression (GWR). The annual mean ambient concentrations were then calculated for each grid. This method has previously been validated in other studies and shows significant agreement between satellite‐derived and ground‐based measurements outside North America and Europe (R2 = 0.81; slope = 0.68).20 Finally, we linked the LC death data and 10‐year concentrations of PM2.5 during 2010–2014.
Statistical analysis
Modeling PM2.5 lung cancer association
A generalized additive model (GAM) was used to estimate the association between mortality and air pollutant exposure. In this study, a Poisson age‐period‐cohort model allowing for overdispersion was used to assess the association between LC mortality and PM2.5 to control for the effects of age, calendar time (period), and birth cohort effects. To determine the linearity of the associations between county average PM2.5 and LC deaths we used a natural cubic spine for PM2.5. As men are at higher absolute risk of LC than women (because of the high prevalence of smoking in Chinese men), we adjusted for gender in the model. We also adjusted for the community type (urban vs. rural area). In addition, the log of the population size was used as the offset to control for the influence of population size. The model is described as follows:
where t and i are the year and site of LC deaths, respectively; Yt, i is the number of observed annual deaths in year t at site i; α is the intercept; age is a categorical variable of age group for LC death; and β is a vector of coefficients for age. S(.) is a natural cubic spline, and period (calendar time) is the year of LC death. Cohort is a categorical variable representing birth cohort, and λ is vector of coefficients. Sex represents the gender category, and η is the vector of corresponding coefficients. Urbanity is a binary variable that is 1 for urban and 0 for rural areas. PM2.5 is a period of 10 years PM2.5, with a natural cubic spline. The degrees of freedom for spline functions were chosen using Akaike information criterion for quasi‐Poisson models (Q‐AIC). The log of the population size was used as the offset. We examined the effects of PM2.5 on LC death separately for men, women, people aged 30–65 years, and those aged ≥ 65 years.
Linearity of the association
If a linear relationship was observed between PM2.5 and LC death, the linear term of PM2.5 was used to calculate relative risk (RR), interpretable as the risk of cancer death with a 10 μg/m3 increase of PM2.5. If the relationship was non‐linear, we detected the threshold of the association by iteratively estimating the AIC of the GAM model using 1 unit increment in PM2.5 within the identified range of threshold, based on the visual detection of the exposure‐response plots. The concentrations of PM2.5 with the lowest AIC were chosen as the threshold. The LC RR associated with PM2.5 below the threshold was set at 1. The effect of PM2.5 with 100 μg/m3 increment above the threshold was then estimated using linear threshold function.
Assessing lung cancer death attributed to PM2.5
There were 30 590 LC deaths in Hebei Province (67.3% men) in 2014, with approximately three out of 10 LC deaths occurring in the 30–64 age group (8638) and seven out of 10 in the ≥ 65 age group (21 952). County level LC deaths attributed to PM2.5 were calculated as follows:
where i is county i; ALCD is LC deaths attributed to PM2.5; RRi is the relative risk of LC deaths associated with PM2.5 at county i above the threshold; and LCDi is number of LC deaths at countyi. We assessed ALCD in the subgroups (men, women, people aged 30–64 years, and those aged ≥ 65 years), as the RRs were different in different groups.
Finally, we calculated the fraction of ALCD attributed to PM2.5 as follows:
where i is county i; NAFLCD is provincial level fraction of LC deaths attributed to PM2.5; SUM (ALCD1−i) is the total number of LC deaths attributed to PM2.5 in 22 counties in Hebei Province; and SUM (LCD1−i) is the total number of LC deaths in Hebei Province. We also assessed NAFLCD in the subgroups (men, women, people aged 30–64 years, and those aged ≥ 65 years).
Results
Figure 1 shows that Hebei Province is located between longitude 113 and 36 north latitude. Data on the geographical variation in LC deaths obtained from 22 cancer registries in Hebei Province are shown in Figure 2. Figure 3 illustrates the spatial distribution of the PM2.5 concentration in 2014 across Hebei Province. Specifically, concentrations are high in central and southern Hebei Province and low in Southwest Hebei Province.
Figure 1.

The location of Hebei Province in China.
Figure 2.
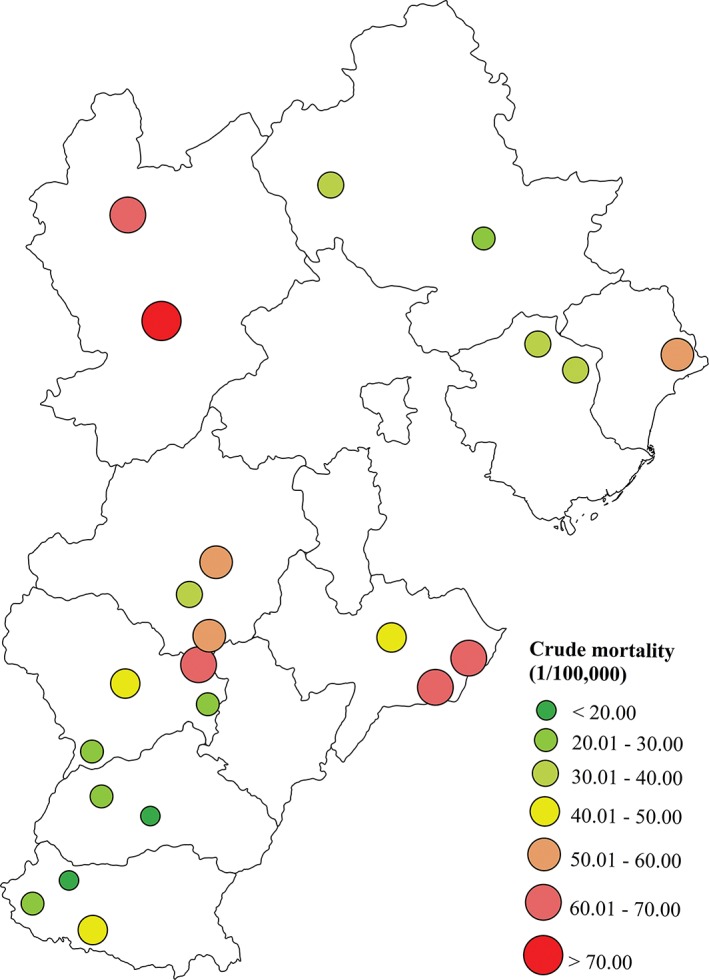
The location of the 22 registries and lung cancer mortality rate for people aged ≤ 30 years in Hebei Province from 2010 to 2014. <20.00, 20.01–30.00, 30.01–40.00, 40.01–50.00, 50.01–60.00, 60.01–70.00, and >70.00.
Figure 3.
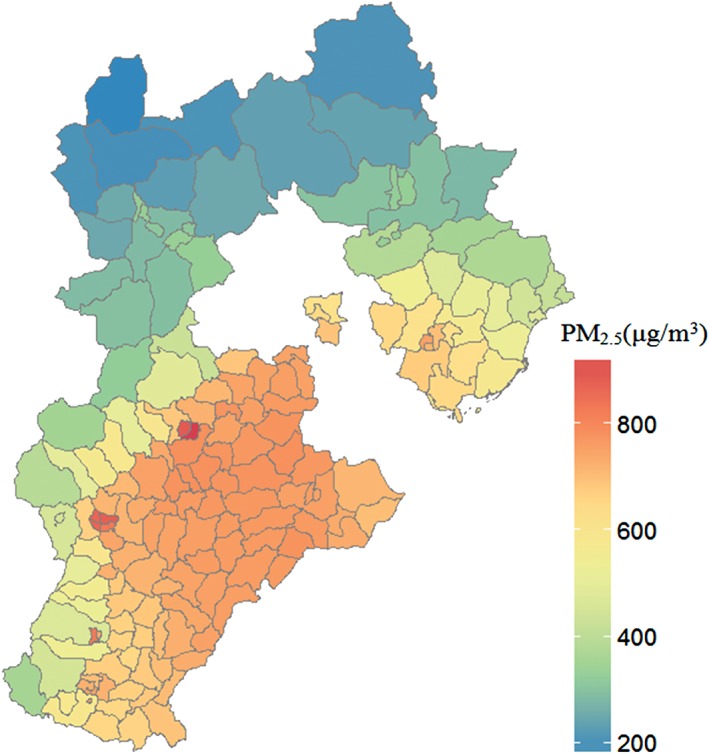
Spatial distribution of 10‐year PM2.5 concentration in 2014 in Hebei Province.
Figure 4 shows the associations between 10 year PM2.5 exposure and LC deaths in different groups. The associations were non‐linear with the thresholds; when under the threshold, 10 year‐PM2.5 had no impact on lung cancer death. The estimated thresholds were 630 μg/m3 for all LCs, 690 μg/m3 for men, 680 μg/m3 for women, 660 μg/m3 for those aged 30–64 years, and 620 μg/m3 for those aged ≥ 65 years (Table 1).
Figure 4.
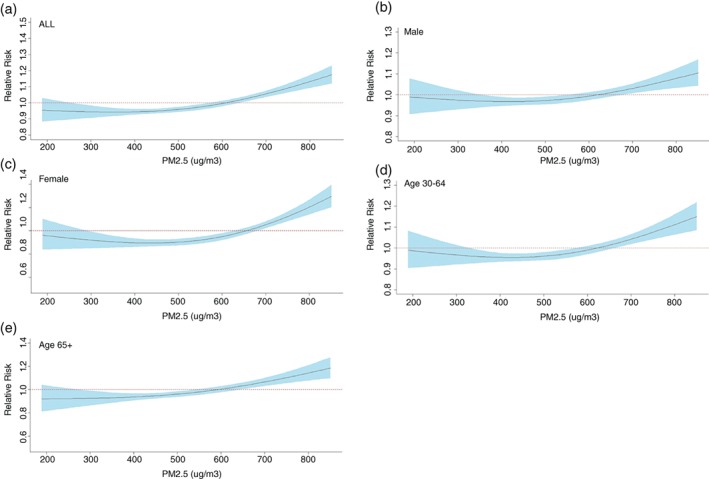
The associations between 10‐year PM2.5 and lung cancer mortality in Hebei Province during 2010–2014 using a spatial age‐period‐cohort design: (a) overall cohort, (b) men, (c) women, (d) those aged 30–64 years, and (e) those aged ≥ 65. A natural cubic spline with foue degrees of freedom was used for PM2.5.
Table 1.
Relative risk of lung cancer mortality associated with a 100 μg/m3 increase in 10‐year PM2.5 above the thresholds in different groups
| Groups | Thresholds (μg/m3) | Annual mean PM2.5 (μg/m3) | Relative risk (95% CI) |
|---|---|---|---|
| All | 630 | 63 | 1.09 (1.08–1.10) |
| Men | 690 | 69 | 1.06 (1.03–1.10) |
| Women | 680 | 68 | 1.20 (1.10–1.26) |
| Aged 30–64 | 660 | 66 | 1.07 (1.05–1.11) |
| Aged ≥ 65 | 620 | 62 | 1.10 (1.07–1.13) |
CI, confidence interval.
The RRs of LC death associated with one 100 μg/m3 increase of PM2.5 varied from 1.06 to 1.20 depending on gender and age (Table 1). The RRs were 1.09 (95% CI 1.08–1.10) for all LC, 1.06 (95% CI 1.03–1.10) for men, 1.20 (95% CI 1.10–1.26) for women, 1.07 (95% CI 1.05–1.11) for those aged 30–64 years, and 1.10 (95% CI 1.07– 1.13) for those aged ≥ 65 years, indicating that women and the elderly had a higher risk of LC mortality associated with PM2.5 than men and those aged 30–64 years.
Table 2 shows the absolute number of LC deaths in 2014 in Hebei Province and the fraction of LC mortality as a result of PM2.5. Overall, 8.3% of LC deaths (approximately 2525 deaths) could be attributed to PM2.5. Compared with 5.7% in men, roughly 16.7% of LC deaths in women in Hebei Province could be explained by PM2.5. Similarly, roughly 6.5% and 9.1% of LC deaths in those aged 30–65 and ≥ 65 years were attributed to PM2.5, respectively.
Table 2.
Lung cancer deaths and fraction attributed to PM2.5 in China in 2014
| Groups | Lung cancer deaths attributed (n) | Fraction attributed (%) |
|---|---|---|
| All | 2525 (2265–2780) | 8.3 (7.4–9.1) |
| Men | 1165 (582–1942) | 5.7 (2.8–9.4) |
| Women | 1667 (830–2167) | 16.7 (8.3–21.6) |
| Aged 30–65 | 564 (403–888) | 6.5 (4.7–10.3) |
| Aged ≥ 65 | 1995 (1396–2525) | 9.1 (6.4–11.5) |
Discussion
In the past several decades, China has achieved rapid economic growth, industrialization, and urbanization, with annual increases in gross domestic product of 9.7% from 1979 to 2015 according to the Chinese Statistical Yearbook 2016. As a result of the rapid development of industrialization, counties with high level PM2.5 are mainly located in the densely populated regions, such as the Beijing‐Tianjin‐Hebei region and the North China Plain.21 Particularly in Hebei Province, emissions caused by an increase in the number of coalmines, cement plants, motor vehicles, and boilers, coupled with the influence of meteorological factors, has contributed to the aggravated state of PM2.5 pollution. According to data from China's Ministry of Environmental Protection, seven cities in Hebei Province ranked in the top 10 most heavily polluted cities in China from 2013 to 2016.
Recently, the International Agency for Research on Cancer (IARC) concluded that outdoor air pollution causes LC.22 Guo et al. showed that the RR of LC mortality associated with one increase of 10 μg/m3 of ambient PM2.5 was 1.08 (95% CI 1.07–1.09) in China.12 A prospective cohort study showed that each 10 μg/m3 increase of PM2.5 in exposure was associated with LC mortality (RR 1.17, 95%CI 0.98–1.14).23 Other studies from the United States and Europe have reported that ambient air pollutants, including particulate matter, are related to LC death.10, 24 Our findings are comparable with a recent meta‐analysis of 17 studies that reported that one 10 μg/m3 increase in PM2.5 was associated with an RR of 1.11 (95% CI 1.05–1.18) for LC mortality.25
In earlier studies, the association between air pollutants and health outcomes has been linear. This assumption may have been made because PM2.5 concentrations in the United States and Europe are considerably lower than those in China, thus, non‐linearity of the relationship at high levels of PM2.5 concentrations was not observed. However, recent studies have shown that there are threshold effects for LC mortality and incidence. Consequently, any previous estimation of the burden of disease that has assumed linearity might overestimate the disease burden attributed to PM2.5.
We also evaluated the role of PM2.5 by gender and found a significantly greater RR for LC mortality among women than men. This might be a consequence of the much lower smoking prevalence in women (~4%) compared to men (~48%) in Hebei Province.26 Previous studies have shown that the impact of air pollution on LC exists mainly in never‐smokers, which would explain the stronger effect in women than in men.24, 27 Radon is a well‐established cause of LC in never smokers.28 In addition, Yin et al. showed that exposure to cooking oil fumes was associated with increased LC risk in Chinese non‐smoking women (odds ratio 1.59, 95% CI 1.13–2.23).29 Although the IARC evaluation was not specific to never‐smokers, one important feature of studies of air pollution from coal burning in China (and to a lesser extent other countries) is that they included a large number of never‐smoking women, especially in Hebei Province.30 The PM2.5 LC mortality association was also stronger in the elderly than in the young.31 This may be because the elderly are more sensitive to air pollution both in terms of physiology and behavior, but may also reflect a greater cumulative lifetime exposure to air pollution in those aged over 65.
Our previous studies have shown that LC incidence and mortality in Hebei Province has increased over the past 40 years. The LC mortality rate in 1973–1975 was 38.46/100 000, ranking first among all cancer deaths, but significantly increased to 189.15% in Hebei Province from 2010 to 2011.32 Environmental pollution, age, and gender are important contributors to LC mortality; however, rare studies have also reported that PM2.5 leads to LC mortality.
In China in 2013, approximately 251 250 LC deaths, on average 13 500 people in each province, were attributable to smoking.33 In Hebei Province in 2013, the number of LC deaths attributed to PM2.5 was less than a fifth of those attributed to smoking. By far, the greatest risk contributing to LC mortality is cigarette smoking; however, our results could enhance public awareness regarding the health risk caused by PM2.5. The public should not overestimate the effect of PM2.5 on LC, because the government has taken effective measures to curb air pollution.
To our knowledge, this study is the first to investigate the effect of long‐term PM2.5 exposure on LC mortality and the LC mortality burden attributed to PM2.5 in Hebei Province. We have taken into account 10 years of cumulative exposure to air pollution in order to more fully understand the mechanisms underpinning the association.
There are some limitations to our study. First, the 22 registry sites were selected by convenience and because of the data quality from these registries. These 22 sites are not fully representative of Hebei Province (although they cover 15.3% of the population); however, this is unlikely to have resulted in any appreciable underestimation or overestimation of the LC burden attributed to air pollution. Estimates of effect size are not dependent on representative populations; rather they require populations where there is heterogeneity in the exposure of interest. Secondly, although we have taken 10 years of PM2.5 into account, this period of observation was short. Thirdly, because of data availability we were not able to adjust for multiple pollutants, such as sulfur dioxide, nitrogen dioxide, and ozone.
Our findings suggest that ambient PM2.5 is significantly and positively associated with an increased risk of LC mortality in Hebei Province, with distinct threshold effects. Female never‐smokers are particularly at risk of atmospheric particulate pollution. Air pollution is currently the primary issue in the field of environmental health in Hebei Province. Thus, effective control measures to reduce particulate matter pollution in Hebei Province need to be taken to reduce the exposure risk of PM2.5.
Disclosure
No authors report any conflict of interest.
References
- 1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet‐Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin 2015; 65: 87–108. [DOI] [PubMed] [Google Scholar]
- 2.International Agency for Research on Cancer. GLOBOCAN 2012: Estimated cancer incidence, mortality and prevalence worldwide in 2012. 2015. [Cited 12 Apr 18.] Available from URL: http://globocan.iarc.fr/Default.aspx
- 3. Chen W, Zheng R, Zhang S et al Cancer incidence and mortality in China, 2013. Cancer Lett 2017; 401: 63–71. [DOI] [PubMed] [Google Scholar]
- 4. He Y, Liang D, Li D et al Cancer incidence and mortality in Hebei province, 2013. Medicine (Baltimore) 2017; 96: e7293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. GBD 2015 Risk Factors Collaborators . Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990‐2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016; 388: 1659–724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Hoek G, Krishnan RM, Beelen R et al Long‐term air pollution exposure and cardio‐respiratory mortality: A review. Environ Health 2013; 12 (1): 43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Villeneuve PJ, Weichenthal SA, Crouse D et al Long‐term exposure to fine particulate matter air pollution and mortality among Canadian women. Epidemiology 2015; 26: 536–45. [DOI] [PubMed] [Google Scholar]
- 8. Beelen R, Raaschou‐Nielsen O, Stafoggia M et al Effects of long‐term exposure to air pollution on natural‐cause mortality: An analysis of 22 European cohorts within the multicentre ESCAPE project. Lancet 2014; 383: 785–95. [DOI] [PubMed] [Google Scholar]
- 9. Yang WS, Zhao H, Wang X, Deng Q, Fan WY, Wang L. An evidence‐based assessment for the association between long‐term exposure to outdoor air pollution and the risk of lung cancer. Eur J Cancer Prev 2016; 25: 163–72. [DOI] [PubMed] [Google Scholar]
- 10. Turner MC, Jerrett M, Pope CA III et al Long‐term ozone exposure and mortality in a large prospective study. Am J Respir Crit Care Med 2016; 193: 1134–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Cohen AJ, Brauer M, Burnett R et al Estimates and 25‐year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017; 389: 1907–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Guo Y, Zeng H, Zheng R et al The burden of lung cancer mortality attributable to fine particles in China. Sci Total Environ 2017; 579: 1460–6. [DOI] [PubMed] [Google Scholar]
- 13. He Q, Geng F, Li C et al Long‐term characteristics of satellite‐based PM2.5 over East China. Sci Total Environ 2017; 612: 1417–23. [DOI] [PubMed] [Google Scholar]
- 14. Feng L, Ye B, Feng H et al Spatiotemporal changes in fine particulate matter pollution and the associated mortality burden in China between 2015 and 2016. Int J Environ Res Public Health 2017; 14: pii: E1321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Kan H, London SJ, Chen G et al Differentiating the effects of fine and coarse particles on daily mortality in Shanghai, China. Environ Int 2007; 33: 376–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Yang C, Peng X, Huang W et al A time‐stratified case‐crossover study of fine particulate matter air pollution and mortality in Guangzhou, China. Int Arch Occup Environ Health 2012; 85: 579–85. [DOI] [PubMed] [Google Scholar]
- 17. Cao J, Xu H, Xu Q, Chen B, Kan H. Fine particulate matter constituents and cardiopulmonary mortality in a heavily polluted Chinese city. Environ Health Perspect 2012; 120: 373–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Lin H, Ma W, Qiu H et al Using daily excessive concentration hours to explore the short‐term mortality effects of ambient PM2.5 in Hong Kong. Environ Pollut 2017; 229: 896–901. [DOI] [PubMed] [Google Scholar]
- 19. van Donkelaar A, Martin RV, Brauer M et al Global estimates of fine particulate matter using a combined geophysical‐statistical method with information from satellites, models, and monitors. Environ Sci Technol 2016; 50: 3762–72. [DOI] [PubMed] [Google Scholar]
- 20. van Donkelaar A, Martin RV, Brauer M, Boys BL. Use of satellite observations for long‐term exposure assessment of global concentrations of fine particulate matter. Environ Health Perspect 2015; 123: 135–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Zhang H, Wang Z, Zhang W. Exploring spatiotemporal patterns of PM2.5 in China based on ground‐level observations for 190 cities. Environ Pollut 2016; 216: 559–67. [DOI] [PubMed] [Google Scholar]
- 22. Straif K, Cohen A, Samet J (eds) . IARC Scientific Publication No. 161: Air Pollution and Cancer. IARC Publications, Lyon: 2013. [Google Scholar]
- 23. Pinault L, Tjepkema M, Crouse DL et al Risk estimates of mortality attributed to low concentrations of ambient fine particulate matter in the Canadian community health survey cohort. Environ Health 2016; 15: 18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Raaschou‐Nielsen O, Andersen ZJ, Beelen R et al Air pollution and lung cancer incidence in 17 European cohorts: Prospective analyses from the European Study of Cohorts for Air Pollution Effects (ESCAPE). Lancet Oncol 2013; 14: 813–22. [DOI] [PubMed] [Google Scholar]
- 25. Huang F, Pan B, Wu J, Chen E, Chen L. Relationship between exposure to PM2.5 and lung cancer incidence and mortality: A meta‐analysis. Oncotarget 2017; 8: 43322–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Lu A, Wang X, Gao G, Ma Z, Sun J, Xue Y. [Comparative study on cigarette smoking between urban and rural residents in Hebei province.] Chin J Public Health 2005; 21: 908–9. (In Chinese.) [Google Scholar]
- 27. Samet JM, Avila‐Tang E, Boffetta P et al Lung cancer in never smokers: Clinical epidemiology and environmental risk factors. Clin Cancer Res 2009; 15: 5626–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Hall EJ, Hei TK. Genomic instability and bystander effects induced by high‐LET radiation. Oncogene 2003; 22: 7034–42. [DOI] [PubMed] [Google Scholar]
- 29. Yin Z, Cui Z, Ren Y et al Genetic polymorphisms of TERT and CLPTM1L, cooking oil fume exposure, and risk of lung cancer: A case‐control study in a Chinese non‐smoking female population. Med Oncol 2014; 31: 114. [DOI] [PubMed] [Google Scholar]
- 30. Lu S, Tan Z, Liu P et al Single particle aerosol mass spectrometry of coal combustion particles associated with high lung cancer rates in Xuanwei and Fuyuan, China. Chemosphere 2017; 186: 278–86. [DOI] [PubMed] [Google Scholar]
- 31. Pope CA III, Dockery DW. Air pollution and life expectancy in China and beyond. Proc Natl Acad Sci U S A 2013; 110: 12861–2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. He Y, Li D, Song G et al Lung cancer burden has increased during the last 40 years in Hebei Province, China. Thorac Cancer 2016; 7: 323–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Islami F, Chen W, Yu XQ et al Cancer deaths and cases attributable to lifestyle factors and infections in China, 2013. Ann Oncol 2017; 28: 2567–74. [DOI] [PubMed] [Google Scholar]