

Abstract
Improving maternal health and decreasing morbidity and mortality due to induced abortion are key endeavors in developing countries. One of the most controversial subjects surrounding interventions to improve maternal health is the effect of abortion laws. Chile offers a natural laboratory to perform an investigation on the determinants influencing maternal health in a large parallel time-series of maternal deaths, analyzing health and socioeconomic indicators, and legislative policies including abortion banning in 1989. Interestingly, abortion restriction in Chile was not associated with an increase in overall maternal mortality or with abortion deaths and total number of abortions. Contrary to the notion proposing a negative impact of restrictive abortion laws on maternal health, the abortion mortality ratio did not increase after the abortion ban in Chile. Rather, it decreased over 96 percent, from 10.8 to 0.39 per 100,000 live births. Thus, the Chilean natural experiment provides for the first time, strong evidence supporting the hypothesis that legalization of abortion is unnecessary to improve maternal health in Latin America.
Keywords: Maternal mortality, Abortion, Maternal health, Women education, Fertility paradox
Introduction
Improving maternal health and decreasing morbidity and mortality due to induced abortion are key endeavors in developing countries (Sachs and McArthur 2005; Okonofua 2006). Clearly, providing rigorous epidemiological information is crucial before proposing evidence-based public health interventions or legal policies regarding women's health worldwide.
One of the most controversial subjects surrounding interventions to improve maternal health is the effect of abortion laws, particularly where abortion is prohibited for the purpose of simultaneously safeguarding women's health, motherhood, and the gestating human life during the whole childbearing period. In the last three decades, the paradigm sustained by numerous international agencies, public health actors, politicians, and several research groups, claims that legislation in countries with restrictive abortion laws is ineffective in controlling the problem of clandestine abortions. Therefore, this paradigm introduces the notion that prohibition of abortion promotes “unsafe” abortions, which in turn lead to a higher maternal mortality and morbidity in those countries (Singh and Ratnam 1998; Berer 2000; World Health Organization 2003; Grimes et al. 2006; Okonofua 2006; Sedgh et al. 2012). However, there is no direct scientific evidence to date of a deleterious cause–effect relationship between abortion restrictive laws and maternal health. Despite this lack of direct scientific evidence, developing countries that prohibit abortion by law are often pressed to implement more liberal abortion policies (Koch et al. 2012a, 2012b, 2012c). This is the case for most countries in Latin America.
The aim of this brief communication is to summarize findings from recent studies, recounting the experience on maternal health in Chile over the last fifty years, which was presented at the International Symposium on Maternal Health in Dublin on September 8, 2012. In particular, this lecture intended to provide new insights into the complex relationship between abortion legislation and maternal health, particularly the impact of abortion banning on maternal and abortion-related mortality in Chile. Although some unpublished complementary information is presented in this report, it is not intended to describe full methodological aspects of the Chilean study that are already available in the full original research article published in the open access journal PLoS ONE (Koch et al. 2012d).
The Chilean Natural Experiment
Presently, it is very difficult to find developing countries with sufficient and reliable maternal mortality data to explore the actual effects of abortion restriction on maternal health (Yazbeck 2007; World Health Organization 2012). Chile, however, offers a natural laboratory to perform an investigation of the determinants influencing maternal health for several reasons (Koch et al. 2012d):
-
1.
Chile exhibits reliable vital statistics since 1909. The Chilean registry of statistics is classified by the WHO as a List A country, with virtually complete data series regarding causes of maternal death. To illustrate the integrity of the Chilean registry, Figure 1 shows complete time series of live births, stillbirths, and maternal deaths between 1909 and 2009.
-
2.
Chile also has kept reliable yearbooks of social, economic, and health statistics in parallel over the last fifty years. Complete time series from 1957 to 2007 are available in the main publication of the Chilean study (Koch et al. 2012d).
-
3.
Chile has implemented major public policies during the 20th century, including maternal child health programs and educational reforms.
-
4.
Chile banned therapeutic abortion in 1989.
Figure 1.
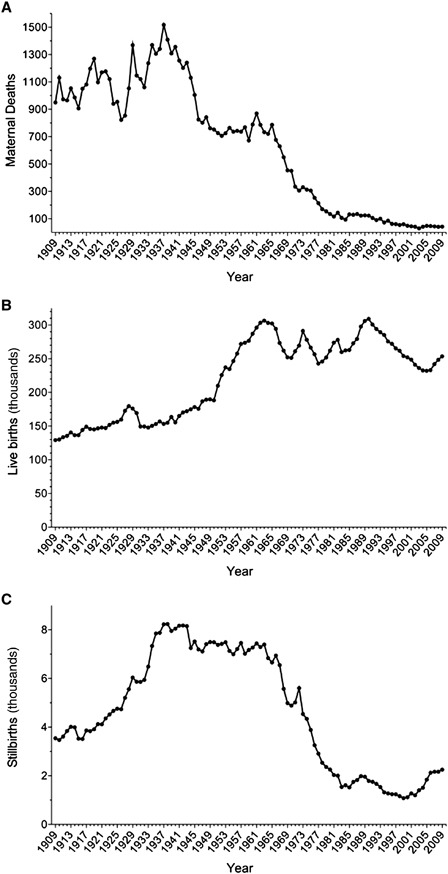
Trends in the absolute number of maternal deaths (A), live births in thousands (B), and stillbirths in thousands (C). Data based on official records from the National Institute of Statistics, Chile, 1909–2009.
It is important to note that this ban on therapeutic abortion does not affect medical interventions that are deemed necessary to save the life of the mother, such as those performed in ectopic pregnancy and other exceptional conditions (Valenzuela 2003). In Chile, these situations are considered a matter of medical ethics and are addressed using the principle of double effect. This principle applies when one medical act has two immediate effects: one that is good and wanted (save the life of the mother) and the other, unwanted and unavoidable (death of the unborn child).
Main Results and Discussion
Maternal mortality ratio (MMR) in Chile underwent different changes over the last century, with an overall reduction of 93.8 percent between 1909 and 2009 (Figure 2).
Figure 2.
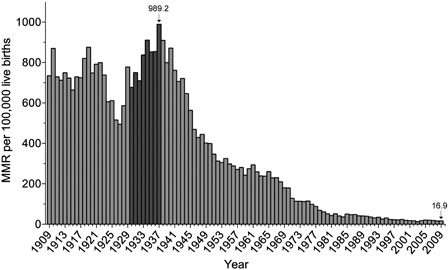
Historical trend of MMR year-by-year in Chile from 1909–2009. Dark gray bars identify the period of highest increase on maternal mortality between 1931 and 1937. (Koch et al., interim analyses: unpublished material from the Chilean Maternal Mortality Research Initiative CMMRI).
In 1931, induced abortion was allowed for the first time, requiring the permission of three physicians or one physician and two witnesses. Notably, there was no significant decrease in the MMR when the 1931 law was adopted liberalizing abortion in the country. Remarkably, the highest peak of the MMR during the last century in Chile occurred a few years after implementation of this law, in 1937 (989 deaths per 100,000 live births). In fact, there is 32 percent increase of the MMR between 1931 (749 deaths per 100,000 live births) and 1937 (Figure 2, dark gray bars).
In 1937, the first systematic program of prenatal care and complementary nutrition for pregnant women and their children (Monckeberg, Valiente, and Mardones 1987; Huneeus and Paz Lanas 2002) (the “mother–child” law) was implemented. Subsequent to the adoption of this program, a rapid fall in maternal mortality can be observed until approximately 1957 (from 989 to 288 per 100,000 live births). As shown in Figure 2, the MMR began to reach a plateau from this year until the mid-1960s.
Focusing on the period of time covered in the main article of the natural experiment in Chile (Koch et al. 2012d), several decreases in overall maternal deaths, abortion-related deaths, and stillbirths can be observed between 1957 and 2009, which are translated into decreases in MMR, abortion mortality ratio (AMR), and stillbirths ratio (SR), as depicted in Table 1 (Instituto Nacional de Estadística 2011).
Table 1.
Time series of official records on maternal mortality and abortion-related mortality, Chile 1957–2009 (Instituto Nacional de Estadística 2011)
| Year | Total maternal deaths | Abortion-related deaths‡ | Live births§ | Stillbirths | MMR* | AMR* | SR† |
|---|---|---|---|---|---|---|---|
| 1957 | 736 | 189 | 271,905 | 7461 | 270.7 | 69.5 | 27.4 |
| 1958 | 769 | 226 | 273,793 | 7018 | 280.9 | 82.5 | 25.6 |
| 1959 | 672 | 236 | 276,686 | 7171 | 242.9 | 85.3 | 25.9 |
| 1960 | 789 | 273 | 287,063 | 7269 | 274.9 | 95.1 | 25.3 |
| 1961 | 870 | 274 | 296,230 | 7442 | 293.7 | 92.5 | 25.1 |
| 1962 | 787 | 257 | 303,249 | 7294 | 259.5 | 84.8 | 24.1 |
| 1963 | 733 | 277 | 306,575 | 7395 | 239.1 | 90.4 | 24.1 |
| 1964 | 721 | 270 | 303,219 | 6839 | 237.8 | 89.0 | 22.6 |
| 1965 | 787 | 275 | 302,401 | 6657 | 260.3 | 90.9 | 22.0 |
| 1966 | 676 | 269 | 294,438 | 6940 | 229.6 | 91.4 | 23.6 |
| 1967 | 630 | 233 | 273,399 | 6550 | 230.4 | 85.2 | 24.0 |
| 1968 | 550 | 199 | 262,036 | 5572 | 209.9 | 75.9 | 21.3 |
| 1969 | 454 | 151 | 252,157 | 4987 | 180.0 | 59.9 | 19.8 |
| 1970 | 451 | 150 | 251,231 | 4884 | 179.5 | 59.7 | 19.4 |
| 1971 | 335 | 114 | 261,021 | 5015 | 128.3 | 43.7 | 19.2 |
| 1972 | 306 | 106 | 269,576 | 5603 | 113.5 | 39.3 | 20.8 |
| 1973 | 331 | 109 | 291,277 | 4538 | 113.6 | 37.4 | 15.6 |
| 1974 | 313 | 115 | 278,165 | 4340 | 112.5 | 41.3 | 15.6 |
| 1975 | 306 | 118 | 266,513 | 3886 | 114.8 | 44.3 | 14.6 |
| 1976 | 253 | 105 | 256,641 | 3257 | 98.6 | 40.9 | 12.7 |
| 1977 | 214 | 89 | 242,847 | 2909 | 88.1 | 36.7 | 12.0 |
| 1978 | 170 | 83 | 245,763 | 2534 | 69.2 | 33.8 | 10.3 |
| 1979 | 155 | 59 | 251,745 | 2361 | 61.6 | 23.4 | 9.4 |
| 1980 | 135 | 53 | 262,030 | 2257 | 51.5 | 20.2 | 8.6 |
| 1981 | 116 | 52 | 273,882 | 2032 | 42.4 | 19.0 | 7.4 |
| 1982 | 144 | 50 | 278,000 | 2003 | 51.8 | 14.8 | 7.2 |
| 1983 | 107 | 41 | 259,888 | 1542 | 41.2 | 14.2 | 5.9 |
| 1984 | 94 | 38 | 262,317 | 1612 | 35.8 | 13.3 | 6.1 |
| 1985 | 132 | 33 | 263,039 | 1522 | 50.2 | 11.0 | 5.8 |
| 1986 | 129 | 47 | 272,941 | 1746 | 47.3 | 15.8 | 6.4 |
| 1987 | 135 | 47 | 279,367 | 1823 | 48.3 | 15.0 | 6.5 |
| 1988 | 123 | 49 | 297,823 | 1985 | 41.3 | 13.8 | 6.7 |
| 1989 | 125 | 42 | 306,080 | 1960 | 40.8 | 10.8 | 6.4 |
| 1990 | 123 | 29 | 309,220 | 1789 | 39.8 | 7.4 | 5.8 |
| 1991 | 106 | 39 | 300,740 | 1754 | 35.2 | 11.0 | 5.8 |
| 1992 | 91 | 28 | 294,218 | 1667 | 30.9 | 7.8 | 5.7 |
| 1993 | 100 | 31 | 289,419 | 1535 | 34.6 | 9.7 | 5.3 |
| 1994 | 73 | 19 | 285,228 | 1321 | 25.6 | 4.6 | 4.6 |
| 1995 | 86 | 20 | 275,760 | 1277 | 31.2 | 5.8 | 4.6 |
| 1996 | 63 | 14 | 272,163 | 1244 | 23.1 | 4.0 | 4.6 |
| 1997 | 61 | 12 | 265,493 | 1240 | 23.0 | 3.8 | 4.7 |
| 1998 | 55 | 14 | 261,802 | 1161 | 21.0 | 3.1 | 4.4 |
| 1999 | 60 | 5 | 254,096 | 1080 | 23.6 | 0.8 | 4.3 |
| 2000 | 49 | 13 | 252,155 | 1116 | 19.4 | 4.8 | 4.4 |
| 2001 | 45 | 4 | 248,651 | 1278 | 18.1 | 1.2 | 5.1 |
| 2002 | 42 | 7 | 241,027 | 1197 | 17.4 | 2.1 | 5.0 |
| 2003 | 30 | 5 | 236,223 | 1404 | 12.7 | 1.3 | 5.9 |
| 2004 | 42 | 4 | 232,588 | 1510 | 18.1 | 1.3 | 6.5 |
| 2005 | 48 | 7 | 232,092 | 1841 | 20.7 | 0.9 | 7.9 |
| 2006 | 47 | 7 | 233,104 | 2124 | 20.2 | 1.3 | 9.1 |
| 2007 | 44 | 4 | 242,054 | 2165 | 18.2 | 0.8 | 8.9 |
| 2008 | 41 | 5 | 248,366 | 2167 | 16.5 | 0.8 | 8.7 |
| 2009 | 43 | 3 | 253,574 | 2252 | 16.9 | 0.4 | 8.9 |
Maternal mortality ratio (MMR) and abortion-related mortality ratio (AMR) per 100,000 live births. AMR numerator considered maternal deaths codes O03-O08 from the ICD-10.
Stillbirths ratio (SR) per 1000 live births.
Considering homologation of codes of the International Classification of Diseases (ICD) 7th version (codes 650–651, period 1957–1967), the 8th version (codes 640–645, period 1968–1979), the 9th version (codes 630–639, period 1980–1996), and 10th version (codes O00-O08, period 1997–2009).
Corrected live births.
Several interventions were implemented in the country in the 1960s. In 1964 through 1967, the program of complementary nutrition for mother and child was strengthened, including a comprehensive design to implement universal access to early prenatal care (with twelve weeks of gestation as upper limit) and introducing a family planning component especially for women after hospitalization due to complications of induced abortions (Viel 1969). In 1965, a law requiring eight years of mandatory primary schooling was passed. Subsequent to these three major interventions, MMR again fell rapidly over the following fifteen years (from 260 to 42 per 100,000 live births between 1965 and 1981) before reaching a slower downward trend in the early 1980s (Figures 1 and 2).
In 1989, induced abortion was completely banned. This provided for an excellent, rare, and unique natural experiment involving an entire population (Koch et al. 2012d). If the hypothesis that abortion legislation was necessary to keep maternal mortality low, then the banning of abortion should have resulted in a measurable increase in the maternal and AMR in years subsequent to the abortion ban. Interestingly, no such increases were observed (Figure 3). Instead, MMR and, particularly, AMR continued to fall for the next two decades (Figure 3A and B).
Figure 3.
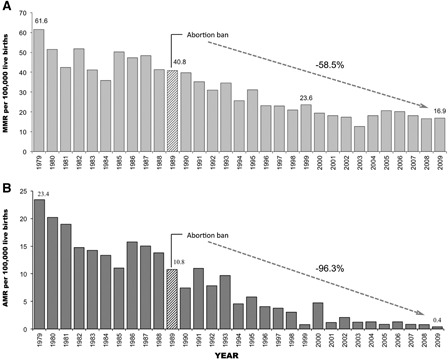
Trends for MMR and AMR after abortion ban in Chile. A continuous decreasing trend can be observed for MMR (A) and AMR (B) between 1979 and 2009. Since abortion prohibition, MMR decreased from 40.8 to 16.9 per 100,000 live births. The accumulated decrease between 1989 and 2009 was 58 percent. AMR decreased from 10.8 to 0.4 per 100,000 live births. The accumulated decrease for the period was 96 percent.
(adapted with permission from Koch et al. 2012d)
Interestingly, in 2009, the MMR in Chile (16.9 per 100,000 live births) was lower than the MMR in the United States (23.2 per 100,000 live births) for the same year (Koch et al. 2012d). Currently, Canada and Chile are the countries with the lowest maternal mortality rates in the American continent.
Another key issue of the Chilean study refers to the assessment of different factors influencing the downward maternal mortality trend over the last fifty years. Using a parallel time series design, we simultaneously evaluated the effect of the following variables on maternal mortality between 1957 and 2007:
-
1.
Average number of schooling years for women of reproductive age.
-
2.
Reproductive behavior, measured through total fertility rate (TFR) and other components, including percent of primiparous women and age at first delivery.
-
3.
Access to maternal health services measured through access to delivery by skilled birth attendants.
-
4.
Access to clean water and sanitary sewer facilities
-
5.
Per capita income.
A multiple autoregressive integrated moving average model (ARIMA) revealed that the educational level of women was the strongest influence on the decrease of MMR. In fact, Chile has seen a dramatic increase in schooling years of women at reproductive age, from 3.5 to 12 years between 1957 and 2007. Increasing the educational level empowers women, improving their access and navigation through the healthcare system, and enable control of their own fertility. Indeed, while skilled birth attendance and the other factors were also associated with a decrease in MMR, the educational level of women modulated all other variables, increasing the effect in a synergistic fashion. Furthermore, increasing education had a simultaneous effect on TFR and MMR (Koch et al. 2012d).
Fertility (measured as TFR, i.e., the average number of children a woman has during her reproductive lifetime) showed an interesting association with age of motherhood and complicated obstetric condition. According to an intuitive notion, a reduction in the number of children born from a woman should be associated with a decreased risk of maternal death. However, it is possible that increasing women's educational level may decrease fertility while also delaying initiation of pregnancy to advanced ages, which increases obstetric complications. This phenomenon is presented as a fertility paradox (Koch et al. 2012d). Figure 4 illustrates the synergistic effect of increasing women's educational level on MMR for different variables, including primiparous women over 29 years of age. Thus, the risk of maternal mortality also increase in societies with an advanced stage of epidemiological and demographic transition. The recent cases of Chile and Mexico are very good examples. Figure 5 compares profiles of death causes in these countries for 2009, possibly reflecting the epidemiologic impact of a delayed motherhood. In both countries, approximately 98 percent of maternal deaths are related to causes other than induced abortion, including hypertension and eclampsia, hemorrhage (in the case of Mexico), and especially indirect causes. (Koch et al. 2012b).
Figure 4.
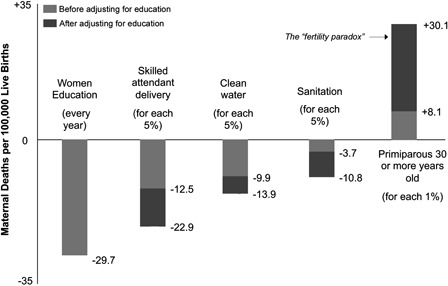
Impact of different factors on MMR based on pathway modeling using ARIMA. The dark area in the each bar illustrates the synergistic effect of the increasing women's educational level on the impact of any other variable.
Adapted with permission from the study by Koch et al. (2012d).
Figure 5.
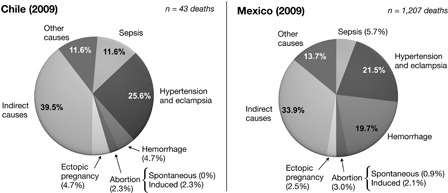
Main causes of maternal deaths in Chile and Mexico during 2009.
Adapted with permission from the study by Koch et al. (2012b).
When the effect of banning therapeutic abortions in Chile was examined, no increase in hospitalizations due to abortion was noted. If banning abortion actually resulted in increasing unsafe illegal abortions, as has been theorized, then a significant increase in hospitalizations due to complications of illegal abortion would be expected. On the contrary, hospitalization due to any kind of abortion (whether spontaneous or induced) continued to decrease. Furthermore, if banning abortion resulted in more deaths from illegal abortion, then an increase in the AMR should have been observed. Remarkably, rather than increasing, the AMR decreased over 96 percent after abortion banning in 1989, from 10.8 to 0.39 per 100,000 live births (Figure 3B).
The decrease in abortion mortality and particularly abortion hospitalizations after the abortion ban in Chile strongly suggest a parallel reduction of induced abortion rates. On the other end of the spectrum, one of the effects of the liberalization of abortion laws is the increase in the total number of abortions performed. This observation can be exemplified by the increase of abortion figures in several nations, including Spain, Belgium, Finland, France, Hungary, Slovakia, and the UK, at least during the first twenty years after abortion legalization. Moreover, detailed data from Spain, Finland, and England and Wales, also demonstrate that the number of repeat abortions increases as the time from legalization of abortion increases (Koch et al. 2012a; Leppalahti et al. 2012). In addition, legalization of abortion in Guyana in 1995 as an effort to reduce maternal mortality (Nunes and Delph 1997), has yielded no progress in decreasing MMR (Koch et al. 2012a; World Health Organization 2012). In fact, according the most recent global report on maternal mortality by WHO (2012), the MMR has substantially increased over the last fifteen years. Whether the legalization of abortion negatively influenced maternal mortality in Guyana remains to be investigated (Koch et al. 2012a).
Concluding Remarks
Taken together, the results of the Chilean natural experiment suggest that the factors positively associated with a decrease in maternal mortality in developing countries include (Koch et al. 2012d):
-
1.
Increased level of female education, which synergistically influences other factors such as access and efficient utilization of available maternal health services, and promotes changes in reproductive behavior, especially decreasing fertility and delaying motherhood.
-
2.
Complementary nutrition programs for mothers and their children.
-
3.
Universal access to prenatal, perinatal, and postnatal health services.
-
4.
Development of emergency obstetrical units and specialized care for complex high-risk cases, which is pivotal for reducing maternal mortality during the slow phase of reduction.
-
5.
Sanitary development, e.g., access to clean water and sewer facilities.
Abortion restrictions were neither associated with increased overall maternal mortality nor with increased total numbers of abortions. Legalization of abortion appears therefore unnecessary to improve maternal health. Restrictive laws are likely to reduce the incidence of abortion when combined with adequate health and social policies, as in the case of Chile. In contrast, liberal laws are accompanied by an increase in abortion figures and, in some low-income developing nations, may also be associated with overall increases in maternal mortality, a hypothesis that requires additional research.
Biography
Dr. Koch is a research fellow in molecular epidemiology, associate professor, and director of the Institute of Molecular Epidemiology (MELISA), Center of Embryonic Medicine and Maternal Health at the Faculty of Medicine of the Universidad Católica de la Santísima Concepción UCSC, 4070129, Concepción, Chile.
References
- Berer M. 2000. Making abortions safe: a matter of good public health policy and practice. Bulletin of the World Health Organization 78: 580–92. [PMC free article] [PubMed] [Google Scholar]
- Grimes D.A., Benson J., Singh S., Romero M., Ganatra B., Okonofua F.E., Shah I.H. 2006. Unsafe abortion: the preventable pandemic. Lancet 368: 1908–19 [DOI] [PubMed] [Google Scholar]
- Huneeus C., Paz Lanas M. 2002. Political science and history: Eduardo Cruz-Coke and the welfare state in Chile, 1937–38. Historia Santiago 35: 151–86. [PubMed] [Google Scholar]
- Instituto Nacional de Estadística (INE). 2011. Estadísticas Vitales, Informe Anual 2009. Instituto Nacional de Estadística. http://www.ine.cl/canales/chile_estadistico/demografia_y_vitales/estadisticas_vitales/2011/Vitales_2009_21102011.pdf.
- Koch E., Aracena P., Bravo M., Gatica S., Stecher J.F., Valenzuela S., Ahlers I. 2012. a. Methodological flaws on abortion estimates for Latin America: Authors’ reply to Singh and Bankole. Ginecologia y obstetricia de Mexico 80(11): 740–7. [PubMed] [Google Scholar]
- Koch E., Aracena P., Gatica S., Bravo M., Huerta-Zepeda A., Calhoun B.C. 2012. b. Fundamental discrepancies in abortion estimates and abortion-related mortality. A re-evaluation of recent studies in Mexico with special reference to the International Classification of Diseases. International Journal of Women's Health 4: 613–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koch E., Bravo M., Gatica S., Stecher J.F., Aracena P., Valenzuela S., Ahlers I. 2012. c. Overestimation of induced abortion in Colombia and other Latin American countries. Ginecologia y Obstetricia de Mexico 80(5): 360–72. [PubMed] [Google Scholar]
- Koch E., Thorp J., Bravo M., Gatica S., Romero C.X., Aguilera H., Ahlers I. 2012. d. Women's education level, maternal health facilities, abortion legislation and maternal deaths: a natural experiment in Chile from 1957 to 2007. PLoS ONE 7(5): e36613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leppalahti S., Gissler M., Mentula M., Heikinheimo O. 2012. Trends in teenage termination of pregnancy and its risk factors: a population-based study in Finland, 1987–2009. Human Reproduction 27(9): 2829–36. [DOI] [PubMed] [Google Scholar]
- Monckeberg F., Valiente S., Mardones F. 1987. Infant and pre-school nutrition: economical development, versus intervention strategies. The case of Chile. Nutrition Research 7: 327–42. [Google Scholar]
- Nunes F., Delph Y. 1997. Making abortion law reform work: steps and slips in Guyana. Reproductive Health Matters 9: 66–76. [Google Scholar]
- Okonofua F. 2006. Abortion and maternal mortality in the developing world. Journal of Obstetrics and Gynaecology Canada 28(11): 974–9. [DOI] [PubMed] [Google Scholar]
- Sachs J.D., McArthur J.W. 2005. The Millennium Project: a plan for meeting the Millennium Development Goals. Lancet 365(9456): 347–53. [DOI] [PubMed] [Google Scholar]
- Sedgh G., Singh S., Shah I.H., Ahman E., Henshaw S.K., Bankole A. 2012. Induced abortion: incidence and trends worldwide from 1995 to 2008. Lancet 379(9816): 625–32. [DOI] [PubMed] [Google Scholar]
- Singh K., Ratnam S.S. 1998. The influence of abortion legislation on maternal mortality. International Journal of Gynaecology and Obstetrics 63 (Suppl. 1): S123–9. [DOI] [PubMed] [Google Scholar]
- Valenzuela C.Y. 2003. Scientific ethics of therapeutic abortion. Revista Medica de Chile 131: 562–8. [PubMed] [Google Scholar]
- Viel B. 1969. Results of a family planning program in the western area of the city of Santiago. American Journal of Public Health 59: 1898–909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization. 2003. Safe abortion: technical and policy guidance for health systems. http://whqlibdoc.who.int/publications/2003/9241590343.pdf. [PubMed]
- World Health Organization. 2012. Trends in maternal mortality: 1990 to 2010. Geneva. http://www.unfpa.org/webdav/site/global/shared/documents/publications/2012/Trends_in_maternal_mortality_A4-1.pdf.
- Yazbeck A.S. 2007. Challenges in measuring maternal mortality. Lancet 370: 1291–2. [DOI] [PubMed] [Google Scholar]