

Abstract
Background
Alcohol and marijuana are the most commonly used substances among adolescents but little is known about patterns of co-use.
Objectives
This study examined patterns of concurrent (not overlapping) and simultaneous (overlapping) use of alcohol and marijuana among adolescents.
Methods
Data from US-national samples of 12th graders (N=84,805, 48.4% female) who participated in the Monitoring the Future study from 1976 to 2016 and who used alcohol and/or marijuana in the past 12 months were used to identify latent classes of alcohol use, marijuana use, and simultaneous alcohol and marijuana (SAM) use.
Results
A four-class solution indicated four patterns of use among adolescents: (1) Simultaneous alcohol and marijuana (SAM) use with binge drinking and recent marijuana use (SAM-Heavier Use; 11.2%); (2) SAM use without binge drinking and with recent marijuana use (SAM-Lighter Use; 21.6%); (3) Marijuana use and alcohol use but no SAM use (Concurrent Use; 10.7%); and (4) Alcohol use but no marijuana or SAM use (Alcohol-Only Use; 56.4%). Membership in either SAM use class was associated with a higher likelihood of truancy, evenings out, and use of illicit drugs other than marijuana. SAM-Heavier Use, compared to SAM-Lighter Use, classes were more likely to report these behaviors and be male, and less likely to have college plans.
Conclusions
Among 12th graders who use both alcohol and marijuana, the majority use simultaneously, although not all use heavily. Given the recognized increased public health risks associated with simultaneous use, adolescent prevention should include focus on particular risks of simultaneous use.
Keywords: Cannabis, marijuana, alcohol, concurrent use, simultaneous use, adolescents
Alcohol and marijuana are now the two most commonly used substances among U.S. high school students [1, 2]. Some adolescents use only one of these two substances, others use alcohol and marijuana concurrently (on separate occasions within a given period, such as within the past 30 days [3, 4]), and still others use alcohol and marijuana simultaneously (at the same time, such that their effects overlap [3, 5]). In comparison with adults, adolescents are more likely to engage in simultaneous, or sometimes called polydrug, use [6]. Nationally representative data indicated that 32% of U.S. 12th graders reported using only alcohol, less than 1% reported using only marijuana, 13% reported concurrent alcohol and marijuana use, and 21% reported simultaneous alcohol and marijuana (SAM) use during the past 12 months [7].
The negative consequences of either alcohol or marijuana use during adolescence are well-documented [8–11]. Risks associated with adolescent SAM use are less studied but include alcohol dependence and abuse [12], dangerous driving [7], and higher use frequency of both alcohol and marijuana [13, 14]. The research literature on adult SAM use is more extensive and links SAM use to more frequent binge drinking and marijuana consumption [15], and adverse social consequences, dangerous driving, and depression [16]. SAM use is of particular concern due to additive (and possibly synergistic) effects on a range of cognitive, perceptual, and motor functions [17–25].
While SAM use is clearly associated with higher substance use frequency, studies have found that some adolescents report SAM use at lower frequency levels of both marijuana and alcohol [13]. At present, there are no estimates of (a) the proportion of late adolescents who engage in SAM use characterized by lower versus higher alcohol and/or marijuana use, (b) the associations with key covariates that may differentiate patterns of use, or (c) the stability of these use patterns across historical time.
Covariates associated with patterns of adolescent alcohol, marijuana, and SAM use include sex, race/ethnicity, and home and school factors [26–28]. Boys have a higher likelihood than girls of binge drinking [27, 28], any marijuana use [1, 26, 28], and any SAM use [13]. Black adolescents consistently have a lower likelihood of recent and/or heavy alcohol use than White or Hispanic adolescents [1, 26, 28], but rates of marijuana use have recently shown greater similarity across racial/ethnic groups [1, 26, 28]. SAM use is higher among White (vs. Black or Hispanic) adolescents even after controlling for substance use frequency [13]. Higher average parental education (a proxy for socio-economic status) is associated with higher binge drinking among 12th grade students [1, 28] and higher odds of SAM use prior to controlling for substance use frequency [13]. Lower school grades are associated with a higher likelihood of SAM use [13] while college-bound students are less likely to report binge drinking or recent marijuana use [1, 28]. A greater number of weekly recreational evenings out, higher school truancy, and use of other illicit substances are associated with higher SAM use prevalence among adolescents [13]. Historically, adolescent alcohol use prevalence has decreased significantly since the end of the 1970s [1, 2] and the proportion who report using neither alcohol nor marijuana has increased [7]. Trends in both concurrent and SAM use have generally mirrored trends in alcohol-only use [7].
The current study aims to contribute to the literature on adolescent alcohol and marijuana use by utilizing data from 41 years of nationally representative samples of U.S. high school seniors to investigate three research questions: (1) Among students reporting either alcohol or marijuana use, what latent patterns of substance use define concurrent and simultaneous user classes? (2) To what extent do key demographic and academic covariates differentiate membership in the identified patterns of use? and (3) To what extent have membership probabilities in the observed latent patterns changed across historical time?
Method
Sample
Data are from the Monitoring the Future (MTF) study, which includes an ongoing cross-sectional survey of adolescents [1, 29]. Each year since 1976, nationally representative samples of approximately 15,000 12th graders are selected using a multistage sampling procedure (at the level of geographic areas, schools, and students). Students are randomly assigned to one (of five until 1988, and of six since 1989) survey forms and complete the self-administered survey during a normal class period. Student response rates have averaged 83%, with most of the non-response due to absenteeism on the day of the survey. Informed consent was obtained using school-specific protocols. The study is approved by the authors’ Institutional Review Board.
The analytic sample was limited to cases from 1976 to 2016 that (a) reported past 12-month alcohol or marijuana use, and (b) provided valid data on SAM use (asked on one of the survey forms). Of the 114,286 students who responded to the relevant survey form, 22,665 (19.8%) reported neither alcohol nor marijuana use in the past 12 months (and were thus not included in the analytic sample). An additional 2,898 (2.5%) did not provide data on either 12-month alcohol or marijuana use, and 3,918 (3.4%) who were eligible to respond to the SAM use item did not provide SAM use data. Thus, the final analytic sample included 84,805 students (74.2% of the original sample receiving the relevant survey form) who reported alcohol and/or marijuana use in the past 12 months.
Measures
Alcohol use
Alcohol use in the past 12 months was assessed with the question, “On how many occasions (if any) have you had any alcoholic beverage to drink—more than just a few sips … during the last 12 months?” with responses coded as 1=any alcohol use, 0=no alcohol use. Binge drinking was assessed with the question, “Think back over the last two weeks. How many times (if any) have you had five or more drinks in a row?” with responses dichotomized to 1=any binge drinking, 0=no binge drinking in the past two weeks. For analysis, an alcohol use trichotomy was created from the two alcohol measures. The mutually exclusive categories were: (1) no alcohol use in the past 12 months, (2) alcohol use in the past 12 months but no binge drinking in the past two weeks, and (3) alcohol use in the past 12 months and binge drinking in the past two weeks.
Marijuana use
Marijuana use in the past 12 months was assessed with the question, “On how many occasions (if any) have you used marijuana [or hashish] … during the last 12 months?” with responses coded as 1=any marijuana use, 0=no marijuana use. Marijuana use in the past 30 days was assessed with the same stem question referring to “… during the last 30 days?” with response options again dichotomized to as 1=any marijuana use, 0=no marijuana use in the past 30 days. For analysis, a marijuana use trichotomy was created from the two marijuana measures. The mutually exclusive categories were: (1) no marijuana use in the past 12 months, (2) marijuana use in the past 12 months but not in the past 30 days, and (3) marijuana use in the past 12 months and in the past 30 days.
Simultaneous alcohol and marijuana (SAM) use
To assess SAM use, students who reported use of marijuana in the past 12 months were asked, “How many of the times when you used marijuana or hashish during the last year did you use it along with alcohol—that is, so that their effects overlapped?” Responses were dichotomized to 1=any SAM use in the past 12 months, 0=no SAM use (including students reporting alcohol use but no marijuana use, or marijuana use but no alcohol use; users of neither alcohol nor marijuana were excluded from analysis).
Covariates
Covariates associated with alcohol and marijuana use were also examined. Self-reported measures included: gender (male, female); race/ethnicity (White, Black/African American, Hispanic, Other Races); parent education (a proxy for socioeconomic status, indicating that at least one parent had some college education vs. high school or less); high school grades (B- or better vs. C+ or lower); whether the student had definite plans to graduate from a four-year college (vs. not); evenings out with friends (three or more evenings out/week vs. fewer than three); truancy (skipping/cutting any class in the past four weeks vs. not); and past 12-month use of any illicit drugs other than marijuana, called illicit other than marijuana (IOTM) use (any use vs. none). High school 12th grade cohort was coded into four categories (1976–1985, 1986–1995, 1996–2005, and 2006–2016).
Plan of Analysis
Latent class analysis (LCA) was used to identify patterns of alcohol use (trichotomous), marijuana use (trichotomous), and SAM use in the past year (dichotomous). The selection of the number of latent classes that best represent the data was based on a combination of parsimony, interpretability, and fit (including the BIC and sample size-adjusted BIC [a-BIC], which have been shown in simulations to perform particularly well at selecting the “correct” latent class model [30]). LCA estimates two types of latent class probability: membership probability shows the estimated proportion of the sample represented by each class, based on patterns of alcohol, marijuana, and SAM use; and item-response probability shows the probability of reporting an indicator for members of each latent class. LCA models are able to account for measurement error (i.e., the mismatch between observed reports and class assignment) and missing data on the latent class indicator variables [31]. Missing data on the latent class indicator variables was assumed to be missing at random and handled by the full information maximum likelihood estimation procedure in Mplus [32]. Missing data on the categorical covariates in the analytic sample (ranging from 5.1% for race/ethnicity to 11.4% for truancy) were handled with the use of missing data indicators.
Analyses were conducted using Mplus v7.4 [32], using full information maximum likelihood estimation with robust standard errors. The complex sample design information was included in all models and weights were included to account for the unequal probability of selection. Identification of maximum likelihood solutions was confirmed for the models using 1000 initial stage random starts and 250 final stage optimizations.
To examine the association between the covariates and the latent classes, all covariates were entered simultaneously to baseline-category multinomial logistic regression models. The regression models utilized the R3STEP command in Mplus to examine covariate associations with the latent classes, in which covariates are not permitted to affect latent class formation [33, 34]. The R3STEP procedure accounts for the modal assignment of a respondent’s posterior probability of inclusion in a given class, along with a correction for classification error. This 3-step classification method [35] has been shown to be superior to the traditional modal assignment without correction and to the multiple psuedo-class draws also available in Mplus [34]. Due to the number of comparisons, discussion of observed associations will be limited to those significant at p<.01.
Results
Identification of Latent Patterns of Substance Use
Using the three indicator measures (SAM dichotomy, alcohol trichotomy, marijuana trichotomy), models estimating one to five latent classes were examined (see model fit indices in Table 1). All measures of fit (AIC, BIC, a-BIC, and loglikelihood) indicated the four-class solution. While all fit statistics indicated selection of the four-class solution, the three-, four-, and five-class solutions were evaluated for interpretability and parsimony. All three solutions included one class characterized by alcohol use only and one class characterized by concurrent use but no SAM use. The three-class solution had one class characterized by SAM use. The four-class solution had two classes differentiating SAM use into lighter SAM and heavier SAM use. The five-class solution included the same four classes, plus had an additional class characterized by SAM use without binge drinking or recent marijuana use. However, in the five-class solution, estimated membership probability for the additional class was very small, below 3% (which would be problematic for examining covariate associations). Thus, the four-class solution was selected as optimal (see Table 2 and Figure 1).
Table 1.
Model fit indices for 1 to 5 latent classes
| Classes | Parameters Estimated | AIC | BIC | a-BIC | VLMR | Entropy | Loglikelihood |
|---|---|---|---|---|---|---|---|
| 1 | 5 | 382609.0 | 382655.8 | 382639.9 | - | - | −191299.5 |
| 2 | 11 | 310841.0 | 310943.8 | 310908.8 | 0.333 | 0.949 | −155409.5 |
| 3 | 17 | 308159.1 | 308318.0 | 308263.9 | 0.000 | 0.873 | −154062.5 |
| 4 | 23 | 307566.2 | 307781.2 | 307708.1 | 0.000 | 0.838 | −153760.1 |
| 5 | 29 | 307578.1 | 307849.2 | 307757.0 | 0.502 | 0.856 | −153760.1 |
Notes: Bold font indicates class solution selected. Models were also run for 6 and 7 classes; however, there was no change in loglikelihood, and AIC, BIC and a-BIC were increasing, indicating the model fit was not improved by expanding the number of latent classes.
Table 2.
Class membership for the 4-class model
| Estimated Membership Probabilities | Latent Classes | ||||
|---|---|---|---|---|---|
| SAMa-Heavier Use | SAM-Lighter Use | Concurrent Use | Alcohol-Only Use | ||
|
| |||||
| 0.112 | 0.216 | 0.107 | 0.564 | ||
|
|
|||||
| Item response probabilities | |||||
| Overall | |||||
| SAM use | |||||
| No 12-month SAM use | .682 | 0.017 | 0.040 | 1.000 | 1.000 |
| Any past 12-month SAM use | .318 | 0.983 | 0.960 | 0.000 | 0.000 |
| Alcohol use | |||||
| No past 12-month alcohol or 2-week binge drinking | .011 | 0.001 | 0.000 | 0.096 | 0.000 |
| Any past 12-month alcohol use, no binge drinking | .637 | 0.098 | 0.527 | 0.656 | 0.789 |
| Any past 2-week binge drinking | .352 | 0.900 | 0.473 | 0.248 | 0.211 |
| Marijuana use | |||||
| No past 12-month or 30-day marijuana use | .538 | 0.000 | 0.000 | 0.000 | 0.951 |
| Any past 12-month marijuana use, no 30-day use | .163 | 0.000 | 0.402 | 0.497 | 0.042 |
| Any past 30-day marijuana use | .298 | 1.000 | 0.598 | 0.503 | 0.007 |
Notes: Unweighted N=84,805. Bold font indicates item response probabilities ≥ .50.
SAM = simultaneous alcohol and marijuana use.
Figure 1.
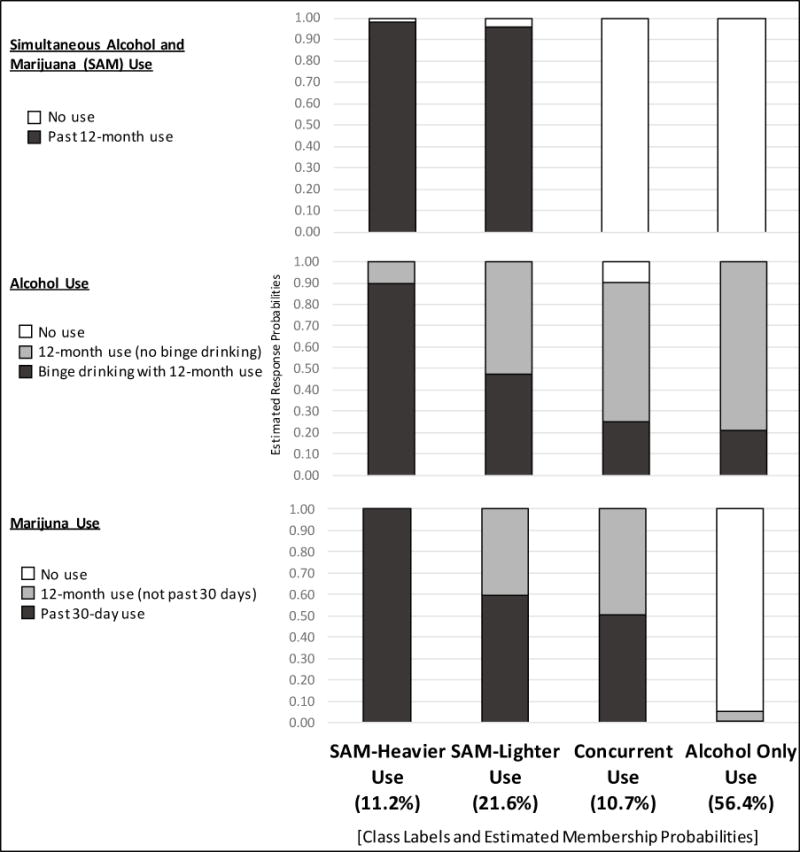
Four-class solution for latent class analysis of simultaneous and concurrent alcohol and marijuana use among U.S. 12th grade students, 1976-2016
The four classes were labeled and described as follows:
SAM-Heavier Use (11.2% estimated latent class membership): Very high probabilities for the following indicators: any SAM use (response probability = 0.98), heavy alcohol use with binge drinking (0.90), and recent (past 30-day) marijuana use (1.00).
SAM-Lighter Use (21.6%): Very high probabilities of any SAM use (0.96). Probabilities of recent marijuana use were high (0.60), but notably lower than for the SAM-heavier use class. High probability of past 12-month alcohol use without binge drinking (0.53).
Concurrent Use (10.7%): High probabilities of recent marijuana use (0.50; but clearly lower than for the SAM-heavier use class;) and past 12-month alcohol use without binge drinking (0.66). Very high probability of no SAM use (1.00).
Alcohol-Only Use (56.4%): Very high probabilities of past 12-month alcohol use without binge drinking (0.79), no past 12-month marijuana use (0.95), and no SAM use (1.00).
Demographic and Academic Covariate Associations with Latent Classes
Using the selected four-class solution described above, analysis turned to examining the extent to which selected covariates differentiated class membership. As shown in Table 3, among this sample of alcohol- and/or marijuana-using high school seniors overall, 46% male and 71% White. About three-fifths (59%) reported having at least one parent with some college education. High school grades of B- or better were reported by 70%, and 43% definitely planned to graduate from a four-year college. Just under half (45%) reported going out three or more evenings per week for fun/recreation. Past month truancy was reported by 31%, and 24% reported past 12-month IOTM use. A larger proportion of the analytic sample was from earlier cohorts (e.g., 33% of cases were from 1976-1985 cohorts), reflecting the fact that there has been an increase in the proportion of students who report using neither alcohol nor marijuana over time [36].
Table 3.
Covariate descriptives
| Covariate | % | (SE%) |
|---|---|---|
| Gender | ||
| Female | 48.4% | (0.3) |
| Male | 46.0% | (0.3) |
| Missing | 5.6% | |
| Race/Ethnicity | ||
| White | 70.9% | (0.6) |
| Black/African American | 9.2% | (0.4) |
| Hispanic | 7.7% | (0.3) |
| Other Races | 7.0% | (0.2) |
| Missing | 5.1% | |
| Parent Education | ||
| High school or less | 33.0% | (0.4) |
| Some college or more | 59.3% | (0.4) |
| Missing | 7.7% | |
| High school grades | ||
| Grades of B- or better | 70.0% | (0.3) |
| Grades of C+ or lower | 21.8% | (0.3) |
| Missing | 8.2% | |
| Four-year college graduation plans | ||
| No definite plans to graduate | 45.7% | (0.4) |
| Definitely plan to graduate | 43.4% | (0.4) |
| Missing | 10.9% | |
| Evenings out for fun/recreation | ||
| Less than 3 evenings out/week | 44.9% | (0.2) |
| Three or more evenings out/week | 45.0% | (0.2) |
| Missing | 10.1% | |
| Truancy | ||
| No classes cut in the past month | 57.6% | (0.3) |
| Any classes cut in the past month | 31.0% | (0.3) |
| Missing | 11.4% | |
| Illicit drug use other than marijuana (IOTM) | ||
| No past 12-month IOTM use | 67.0% | (0.3) |
| Any past 12-month IOTM use | 23.5% | (0.3) |
| Missing | 9.5% | |
| Cohorta | ||
| 1976–1985 | 33.0% | (1.1) |
| 1986–1995 | 26.5% | (1.0) |
| 1996–2005 | 20.6% | (0.8) |
| 2006–2016 | 19.9% | (0.8) |
Notes: Unweighted N = 84,805; estimates provided account for the complex sample design. (SE%) = standard error of the percentage (SE not reported for missing dummy terms).
No missing data for this covariate.
Table 4 presents the adjusted relative risk ratios (ARRs) from multivariable multinomial logistic regression models of latent class membership on covariates using SAM-Heavier Use as the base class (results indicate covariate-related differences in membership likelihood in SAM-Lighter Use, Concurrent Use, and Alcohol-Only Use classes compared with SAM-Heavier Use). The relative risk of membership in the SAM-Heavier Use class (vs. all other classes) was significantly higher for 12th grade students who were male (vs. female), reported three or more evenings out/week (vs. not), reported any truancy (vs. no truancy in the past four weeks), and reported IOTM use in the past 12 months (vs. not). Associations by race/ethnicity showed the risk of membership in the SAM-Heavier Use class versus Concurrent Use and Alcohol-Only Use classes was significantly higher for White students than students in all other race/ethnic groups. White students also reported higher risk than Black and Other Race students for membership in the SAM-Heavier Use class versus SAM-Lighter Use class, but no significant differences between White and Hispanic students was observed. The relative risk of membership in the SAM-Heavier Use class (vs. Alcohol-Only Use class) was significantly higher for 12th graders who reported that their parent(s) had at least some college education (vs. high school or less), and for those who reported grades of C+ or lower (vs. B- or better). Neither parent education nor high school grades differentiated the membership risk between SAM-Heavier versus SAM-Lighter or Concurrent Use classes. College plans did not differentiate the risk of membership in the SAM-Heavier versus Concurrent Use classes; however, membership in the SAM-Heavier Use class was significantly less likely than membership in either the SAM-Lighter or Alcohol-Only Use classes for students who definitely planned to graduate from a 4-year college when compared to those without such plans.
Table 4.
Adjusted relative risk ratios from multivariable multinomial logistic regressions of latent class membership on covariates: Comparisons with the SAMa-Heavier Use class
| SAM-Lighter Use | Concurrent Use | Alcohol-Only Use | ||||
|---|---|---|---|---|---|---|
| (vs. SAM-Heavier) | (vs. SAM-Heavier) | (vs. SAM-Heavier) | ||||
| ARRb | p | ARR | p | ARR | p | |
|
|
||||||
| Gender (ref = female) | ||||||
| Male | 0.28 | <.001 | 0.29 | <.001 | 0.27 | <.001 |
| Race/Ethnicity (ref = White) | ||||||
| Black/African American | 3.50 | <.001 | 6.11 | <.001 | 3.64 | <.001 |
| Hispanic | 1.29 | 0.067 | 1.79 | <.001 | 1.62 | <.001 |
| Other Races | 1.43 | 0.005 | 1.86 | <.001 | 1.73 | <.001 |
| Parent Education (ref = high school or less) | ||||||
| Some college | 0.96 | 0.523 | 0.87 | 0.028 | 0.81 | <.001 |
| High school grades (ref = B- or better) | ||||||
| C+ or worse | 0.87 | 0.030 | 0.94 | 0.331 | 0.62 | <.001 |
| Four-year college graduation plans (ref = no definite plans to graduate) | ||||||
| Definitely plan to graduate | 1.22 | 0.004 | 1.15 | 0.038 | 1.33 | <.001 |
| Evenings out (ref = fewer than 3) | ||||||
| Three or more evenings out/week | 0.37 | <.001 | 0.33 | <.001 | 0.25 | <.001 |
| Truancy (ref = no cutting class in past month) | ||||||
| Any classes cut in past month | 0.50 | <.001 | 0.43 | <.001 | 0.26 | <.001 |
| Illicit drug use other than marijuana (IOTM) (ref = no past 12-month use) | ||||||
| Any past 12-month IOTM use | 0.16 | <.001 | 0.09 | <.001 | 0.02 | <.001 |
| Cohort (ref = 2006-2016) | ||||||
| 1976-1985 | 0.39 | <.001 | 0.33 | <.001 | 0.43 | <.001 |
| 1986-1995 | 0.67 | <.001 | 0.46 | <.001 | 1.12 | 0.293 |
| 1996-2005 | 0.58 | <.001 | 0.52 | <.001 | 0.69 | 0.001 |
Notes: Unweighted N=84,805. All covariates entered simultaneously and included missing data indicators; estimates for missing indicators not shown. Bold entries represent associations significant at p < .01.
SAM = simultaneous alcohol and marijuana use.
ARR = Adjusted risk ratio.
Table 5 presents ARRs for multivariable multinomial logistic regression models where the Alcohol-Only Use class was used as the base class. The relative risk of membership in the Alcohol-Only Use class versus both SAM-Lighter and Concurrent Use classes was significantly lower for students who reported lower grades, three or more evenings out per week, truancy, and IOTM use. Conversely, the relative risk of membership in the Alcohol-Only Use class was significantly higher for those with definite plans to graduate from a four-year college. Regarding racial/ethnic differences, the relative risk of membership in the Alcohol-Only Use class versus SAM-Lighter Use class was significantly lower for White students compared with Hispanic and Other Race students (no significant differences were observed between White and Black students). White students were significantly more likely than Black students to be members of the Alcohol-Only Use class compared with the Concurrent Use class; this membership risk did not significantly differ between White versus Hispanic or Other Race students. Parent education did not differentiate membership risk between Alcohol-Only and Concurrent Use classes; however, membership in the Alcohol-Only Use class was significantly less likely for those reporting having at least one parent with some college education. Gender did not differentiate the relative risk of class membership in the Alcohol-Only Use class versus either SAM-Lighter or Concurrent Use classes.
Table 5.
Adjusted relative risk ratios from multivariable multinomial logistic regressions of latent class membership on covariates: Comparisons with the Alcohol-Only Use class
| SAMa-Lighter Use | Concurrent Use | |||
|---|---|---|---|---|
| (vs. Alcohol Only) | (vs. Alcohol Only) | |||
| ARRb | p | ARR | p | |
|
|
||||
| Gender (ref = female) | ||||
| Male | 1.06 | 0.045 | 1.06 | 0.081 |
| Race/Ethnicity (ref = White) | ||||
| Black/African American | 0.96 | 0.440 | 1.68 | <.001 |
| Hispanic | 0.80 | <.001 | 1.10 | 0.118 |
| Other Races | 0.83 | <.001 | 1.07 | 0.264 |
| Parent Education (ref = high school or less) | ||||
| Some college | 1.18 | <.001 | 1.08 | 0.041 |
| High school grades (ref = B- or better) | ||||
| C+ or worse | 1.39 | <.001 | 1.51 | <.001 |
| Four-year college graduation plans (ref = no definite plans to graduate) | ||||
| Definitely plan to graduate | 0.92 | 0.003 | 0.86 | <.001 |
| Evenings out (ref = fewer than 3) | ||||
| Three or more evenings out/week | 1.48 | <.001 | 1.33 | <.001 |
| Truancy (ref = no cutting class in past month) | ||||
| Any classes cut in past month | 1.88 | <.001 | 1.64 | <.001 |
| Illicit drug use other than marijuana (IOTM) (ref = no past 12-month use) | ||||
| Any past 12-month IOTM use | 6.97 | <.001 | 4.04 | <.001 |
| Cohort (ref = 2006-2016) | ||||
| 1976-1985 | 0.91 | 0.042 | 0.77 | <.001 |
| 1986-1995 | 0.60 | <.001 | 0.42 | <.001 |
| 1996-2005 | 0.84 | <.001 | 0.75 | <.001 |
Note: Unweighted N=84,805. All covariates entered simultaneously and included missing data indicators; estimates for missing indicators not shown. Bold entries represent associations significant at p < .01.
SAM = simultaneous alcohol and marijuana use.
ARR = Adjusted risk ratio.
In order to make full comparisons, SAM-Lighter Use versus Concurrent Use classes was also examined (results not tabled). In summary, risk of membership in the SAM-Lighter Use class (vs. Concurrent Use) was significantly higher for White students and students reporting frequent evenings out, truancy, and IOTM use (although the magnitude of associations were lower than those observed in comparisons with the SAM-Heavier Use class). Gender, parental education, high school grades, and four-year college plans were not associated with significant differences in membership risk between SAM-Lighter and Concurrent Use classes.
Change in Membership Probabilities across Historical Time
The final rows of Tables 4 and 5 report the relative risk of class membership by cohort group after controlling for other covariates. The risk of membership in the SAM-Heavier Use class (vs. all other classes) was generally lowest for students in the most recent cohorts (i.e., 2006–2016) (Table 4); the one exception to this pattern was no significant differences in membership risk in SAM-Heavier versus Alcohol-Only Use classes for students in 2006-2016 cohorts compared with 1986-1995 cohorts. The relative risk of being in the Alcohol-Only Use class (Table 5) versus the SAM-Lighter Use class was significantly lower for students in the most recent cohorts compared with the 1986–1995 and 1996–2005 cohorts. The relative risk of being in the Alcohol-Only Use class versus the Concurrent Use class was significantly lower for students in the most recent cohorts compared with all other cohorts. Finally, no significant differences in the relative risk of being in the SAM-Lighter Use versus Concurrent Use classes were observed between students in most recent cohorts (2006-2016) compared with the 1996–2005 cohorts; however, recent cohorts had a lower risk of membership in SAM-Lighter versus Concurrent Use classes than students in 1976-1985 and 1986-1995 (results not tabled).
Discussion
Previous studies examining alcohol and marijuana use among adolescents have typically, at most, described the percentage who used both substances. These studies do not show the heterogeneity in patterns of use or identify adolescents at risk of harm associated with SAM use [17–25]. Existing research shows that SAM use has serious consequences for youth [7, 13, 20, 37] and adults [7, 12, 15–20, 38], but to date the particular patterns of alcohol use, marijuana use, and SAM use have not been examined.
Among U.S. high school seniors reporting alcohol and/or marijuana use in the past 12 months, we found four distinct patterns of use. Two of the patterns were identified by SAM use: The SAM-Heavier use class had very high probabilities of recent binge drinking and marijuana use, and the SAM-Lighter use class had considerably lower probabilities of both. The SAM-Lighter use class was twice as prevalent as the SAM-Heavier use class. A Concurrent use class reported both alcohol and marijuana but no simultaneous use in the past year, and a fourth class showed alcohol use only. Consistent with previous research [15], SAM users had higher rates of binge drinking and past-month marijuana use than those in Concurrent and Alcohol-Only classes. We did not find a class of adolescents who report binge drinking but not marijuana use, nor a marijuana-only class in this population because it is rare for adolescents to use marijuana but not alcohol [7].
The two distinct groups of adolescent SAM users provide new information about variations in the intensity of substance use and related risks. Individuals in the SAM-Heavier Use class almost universally reported binge drinking and past-month marijuana use, while less than half of those in the SAM-Lighter Use class reported binge drinking and less than 60% reported past-month marijuana use. This is consistent with previous research documenting that SAM use is associated with high-intensity drinking (10+ drinks in a row; [39, 40]) and smoking marijuana near-daily [37]. Youth with high levels of alcohol and marijuana use are at particularly high risk of SAM use and associated negative outcomes, and may need intervention and treatment efforts that raise awareness of the risks of simultaneous use. Furthermore, adolescents with heavier versus lighter patterns of alcohol, marijuana, and SAM use differ in their sociodemographic, academic, and other behavioral characteristics. Risk factors for heavier versus lighter SAM use included being male and reporting more frequent evenings out with friends, truancy, IOTM use, and lower likelihood of college attendance. These are known risk factors for SAM use [e.g., 13, 15]; the current findings show that these characteristics also differentiate SAM users. Future longitudinal research should examine whether SAM use precedes and/or follows from these related factors. Prevention and intervention programs should acknowledge these co-occurring risks, as well as emerging findings that suggest that SAM use is perceived as different than alcohol or marijuana use alone, with distinct expectancies, motives, and consequences associated with SAM use [41–43].
Across historical time, we found that the proportion of 12th graders engaging in SAM-Heavier Use has decreased, which indicates decreasing public health risk. However, this may be offset by increases in patterns of Concurrent Use and SAM-Lighter Use, compared to Alcohol-Only Use. In sum, although fewer adolescents are drinking alcohol in more recent years [27], a greater proportion of adolescent drinkers are also using marijuana concurrently or simultaneously, suggesting that the intersections of alcohol and marijuana use need continued research attention.
The results from the present study have important implications for public health and clinical intervention. Many U.S. 12th graders engage in both alcohol and marijuana use, often simultaneously. It is therefore important to identify those at risk for SAM use, those engaging in lighter SAM use who may be at risk for escalating to heavier use, and those already engaging in heavier SAM use. Screening, brief intervention, and referral to treatment (SBIRT) strategies have proven successful in identifying individuals at risk in primary care, emergency departments, and general medicine settings for alcohol use and directing those in need to the appropriate level of care [44–47]. School-based health centers and primary care providers may need to routinely screen for alcohol, marijuana, and SAM use and provide those meeting risk criteria with brief intervention and/or referral to treatment. Successful brief motivational interventions have been developed and utilized with adolescent alcohol and marijuana users [48–50]. Future work should assess whether integrated interventions for SAM use are needed, or whether targeting alcohol or marijuana use also reduces SAM use.
Limitations of this study include that data are from a school-based sample of adolescents; high school dropouts are therefore not included. Data are cross-sectional and preclude using the findings to draw conclusions about the extent to which substance use is a cause or effect of risk factors such as poor school performance. Finally, the time frames for the alcohol use indicator (no use; past 12-month use without 2-week binge drinking; or past 2-week binge drinking) and the marijuana use indicator (no use; past 12-month use but not use in the past 30 days; past 30-day use) were not identical, due to the measures available.
The above limitations notwithstanding, the current study was able to utilize data from alcohol- and/or marijuana-using students in nationally representative samples of 12th grade students to identify meaningful and heterogeneous patterns of simultaneous and concurrent use. Among 12th graders who used alcohol and/or marijuana, the majority used simultaneously, although not all used heavily. Future research is needed to document how these patterns of use develop and change as individuals age and to explore how to intervene to reduce the particular risks associated with simultaneous use.
Acknowledgments
Data collection and development of this manuscript were supported by research grants from the National Institute on Alcohol Abuse and Alcoholism (R01 AA025037) and the National Institute on Drug Abuse (R01 DA037902, R01 DA001411). The study sponsors had no role in the study design, collection, analysis or interpretation of the data, writing of the manuscript, or the decision to submit the paper for publication. The content is solely the responsibility of the authors and does not necessarily represent the official views of the study sponsors.
Footnotes
Financial Disclosures: None to report.
References
- 1.Miech RA, Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future national survey results on drug use, 1975-2015: Volume I, secondary school students. Ann Arbor: Institute for Social Research, The University of Michigan; 2016. Available from: http://monitoringthefuture.org/pubs/monographs/mtf-vol1_2015.pdf. Accessed: January 15, 2017. [Google Scholar]
- 2.Johnston LD, O’Malley PM, Miech RA, Bachman JG, Schulenberg JE. Monitoring the Future national survey results on drug use, 1975-2016: Overview, key findings on adolescent drug use. Ann Arbor: Institute for Social Research, The University of Michigan; 2017. [Google Scholar]
- 3.Earleywine M, Newcomb MD. Concurrent versus simultaneous polydrug use: Prevalence, correlates, discriminant validity, and prospective effects on health outcomes. Exp Clin Psychopharmacol. 1997 Nov;5(4):353–64. doi: 10.1037//1064-1297.5.4.353. Epub 1997/12/05. eng. [DOI] [PubMed] [Google Scholar]
- 4.Martin CS, Clifford PR, Clapper RL. Patterns and predictors of simultaneous and concurrent use of alcohol, tobacco, marijuana, and hallucinogens in first-year college students. J Subst Abuse. 1992;4(3):319–26. doi: 10.1016/0899-3289(92)90039-z. Epub 1992/01/01. eng. [DOI] [PubMed] [Google Scholar]
- 5.Collins RL, Ellickson PL, Bell RM. Simultaneous polydrug use among teens: Prevalence and predictors. Journal of Substance Abuse. 1998;10(3):233–53. doi: 10.1016/S0899-3289(99)00007-3. Epub 2000/02/26. eng. [DOI] [PubMed] [Google Scholar]
- 6.Winters KC, Tanner-Smith EE, Bresani E, Meyers K. Current advances in the treatment of adolescent drug use. Adolescent Health, Medicine and Therapeutics. 2014 Nov 20;5:199–210. doi: 10.2147/AHMT.S48053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Terry-McElrath YM, O’Malley PM, Johnston LD. Alcohol and marijuana use patterns associated with unsafe driving among U.S. High school seniors: High use frequency, concurrent use, and simultaneous use. J Stud Alcohol Drugs. 2014 May;75(3):378–89. doi: 10.15288/jsad.2014.75.378. English. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.U.S. Department of Health and Human Services. The Surgeon General’s Call to Action to prevent and reduce underage drinking. Rockville, MD: 2007. Available from: https://www.ncbi.nlm.nih.gov/books/NBK44360/. Accessed: January 15, 2017. [PubMed] [Google Scholar]
- 9.Jacobus J, Tapert SF. Effects of cannabis on the adolescent brain. Curr Pharm Des. 2014;20(13):2186–93. doi: 10.2174/13816128113199990426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.National Academies of Sciences Engineering and Medicine. The health effects of cannabis and cannabinoids: The current state of evidence and recommendations for research. Washington, DC: National Academies Press; 2017. [PubMed] [Google Scholar]
- 11.Osuch EA, Manning K, Hegele RA, Theberge J, Neufeld R, Mitchell D, et al. Depression, marijuana use and early-onset marijuana use conferred unique effects on neural connectivity and cognition. Acta Psychiatr Scand. 2016 Nov;134(5):399–409. doi: 10.1111/acps.12629. Epub 2016/08/28. eng. [DOI] [PubMed] [Google Scholar]
- 12.Martin CS, Kaczynski NA, Maisto SA, Tarter RE. Polydrug use in adolescent drinkers with and without DSM-IV alcohol abuse and dependence. Alcohol Clin Exp Res. 1996 Sep;20(6):1099–108. doi: 10.1111/j.1530-0277.1996.tb01953.x. Epub 1996/09/01. eng. [DOI] [PubMed] [Google Scholar]
- 13.Terry-McElrath YM, O’Malley PM, Johnston LD. Simultaneous alcohol and marijuana use among US high school seniors from 1976 to 2011: Trends, reasons, and situations. Drug Alcohol Depend. 2013 Nov 1;133(1):71–9. doi: 10.1016/j.drugalcdep.2013.05.031. Epub 2013/06/29. Eng. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Patrick ME, Veliz PT, Terry-McElrath YM. High-intensity and simultaneous alcohol and marijuana use among high school seniors in the US. Subst Abus. doi: 10.1080/08897077.2017.1356421. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Subbaraman MS, Kerr WC. Simultaneous versus concurrent use of alcohol and cannabis in the national alcohol survey. Alcohol Clin Exp Res. 2015;39(5):872–9. doi: 10.1111/acer.12698.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Midanik LT, Tam TW, Weisner C. Concurrent and simultaneous drug and alcohol use: Results of the 2000 National Alcohol Survey. Drug Alcohol Depend. 2007 Sep 6;90(1):72–80. doi: 10.1016/j.drugalcdep.2007.02.024. Epub 2007/04/21. eng. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Belgrave BE, Bird KD, Chesher GB, Jackson DM, Lubbe KE, Starmer GA, et al. The effect of (-) trans-delta9-tetrahydrocannabinol, alone and in combination with ethanol, on human performance. Psychopharmacology (Berl) 1979 Mar 29;62(1):53–60. doi: 10.1007/BF00426035. Epub 1979/03/29. eng. [DOI] [PubMed] [Google Scholar]
- 18.Chesher GB, Franks HM, Hensley VR, Hensley WJ, Jackson DM, Starmer GA, et al. The interaction of ethanol and delta9-tetrahydrocannabinol in man: Effects on perceptual, cognitive and motor functions. The Medical Journal of Australia. 1976 Jul 31;2(5):159–63. Epub 1976/07/31. eng. [PubMed] [Google Scholar]
- 19.Chesher GB, Franks HM, Jackson DM, Starmer GA, Teo RK. Ethanol and delta9-tetrahydrocannabinol interactive effects on human perceptual, cognitive and motor functions II. The Medical Journal of Australia. 1977 Apr 02;1(14):478–81. Epub 1977/04/02. eng. [PubMed] [Google Scholar]
- 20.Kelly E, Darke S, Ross J. A review of drug use and driving: Epidemiology, impairment, risk factors and risk perceptions. Drug and Alcohol Review. 2004 Sep;23(3):319–44. doi: 10.1080/09595230412331289482. Epub 2004/09/17. eng. [DOI] [PubMed] [Google Scholar]
- 21.Lamers CT, Ramaekers JG. Visual search and urban driving under the influence of marijuana and alcohol. Human Psychopharmacology: Clinical and Experimental. 2001 Jul;16(5):393–401. doi: 10.1002/hup.307. Epub 2002/10/31. eng. [DOI] [PubMed] [Google Scholar]
- 22.Ramaekers JG, Robbe HW, O’Hanlon JF. Marijuana, alcohol and actual driving performance. Human Psychopharmacology: Clinical and Experimental. 2000 Oct;15(7):551–8. doi: 10.1002/1099-1077(200010)15:7<551::aid-hup236>3.0.co;2-p. Epub 2002/10/31. eng. [DOI] [PubMed] [Google Scholar]
- 23.Robbe HW. Marijuana’s impairing effects on driving are moderate when taken alone but severe when combined with alcohol. Human Psychopharmacology: Clinical and Experimental. 1998;13(S2):S70–S8. doi: 10.1002/(SICI)1099-1077(1998110)13:2+<S70::AID-HUP50>3.0.CO;2-R.. [DOI] [Google Scholar]
- 24.Hartman RL, Brown TL, Milavetz G, Spurgin A, Pierce RS, Gorelick DA, et al. Cannabis effects on driving lateral control with and without alcohol. Drug Alcohol Depend. 2015 Jun 23;154:25–37. doi: 10.1016/j.drugalcdep.2015.06.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hartman RL, Huestis MA. Cannabis effects on driving skills. Clin Chem. 2013 Mar;59(3):478–92. doi: 10.1373/clinchem.2012.194381. Epub 2012/12/12. eng. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kann L, McManus T, Harris WA, Shanklin SL, Flint KH, Hawkins J, et al. Youth risk behavior surveillance - United States, 2015. MMWR Surveill Summ. 2016;65(6):1–174. doi: 10.15585/mmwr.ss6506a1.. [DOI] [PubMed] [Google Scholar]
- 27.Miech RA, Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE, Patrick ME. Monitoring the Future national survey results on drug use, 1975-2016: Volume I, secondary school students. Ann Arbor: Institute for Social Research, University of Michigan; 2017. [Google Scholar]
- 28.Johnston LD, O’Malley PM, Miech RA, Bachman JG, Schulenberg JE. Demographic subgroup trends among adolescents in the use of various licit and illicit drugs, 1975-2016. Ann Arbor, MI: Institute for Social Research, University of Michigan; 2017. (Monitoring the Future occasional paper no. 88). [Google Scholar]
- 29.Bachman JG, Johnston LD, O’Malley PM, Schulenberg JE, Miech RA. The Monitoring the Future project after four decades: Design and procedures. Ann Arbor, MI: Institute for Social Research; 2015. (Monitoring the Future occasional paper no. 82). Available from: http://monitoringthefuture.org/pubs/occpapers/mtf-occ82.pdf. [Google Scholar]
- 30.Dziak JJ, Lanza ST, Tan X. Effect size, statistical power and sample size requirements for the bootstrap likelihood ratio test in latent class analysis. Structural Equation Modeling. 2014 Jan 1;21(4):534–52. doi: 10.1080/10705511.2014.919819. English. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Collins LM, Lanza ST. Latent class and latent transition analysis: With applications in the social, behavioral, and health sciences. New York, NY: Wiley; 2010. [Google Scholar]
- 32.Muthén LK, Muthén BO. Mplus user’s guide. Seventh. Los Angeles, CA: Muthén & Muthén;; 1998–2015. [Google Scholar]
- 33.Muthén B, Asparouhov T. Causal effects in mediation modeling: An introduction with applications to latent variables. Structural Equation Modeling: A Multidisciplinary Journal. 2015 Jan 2;22(1):12–23. doi: 10.1080/10705511.2014.935843. [DOI] [Google Scholar]
- 34.Asparouhov T, Muthén B. Auxiliary variables in mixture modeling: Three-step approaches using mplus. Structural Equation Modeling: A Multidisciplinary Journal. 2014;21(3):329–41. doi: 10.1080/10705511.2014.915181. 2014/07/03. [DOI] [Google Scholar]
- 35.Vermunt JK. Latent class modeling with covariates: Two improved three-step approaches. Polit Anal. 2010 Fal;18(4):450–69. doi: 10.1093/pan/mpq025. English. [DOI] [Google Scholar]
- 36.Stern SA, Terry-McElrath YM, Patrick ME. Beverage-specific binge drinking patterns in young adults aged 19/20; Poster presented at the annual meeting of the Research Society on Alcoholism; New Orleans, LA. 2016. Jun, [Google Scholar]
- 37.Patrick ME, Veliz PT, Terry-McElrath YM. High-intensity and simultaneous alcohol and marijuana use among high school seniors in the U.S. Substance Abuse. 2017 Jul;20:1–6. doi: 10.1080/08897077.2017.1356421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Chait LD, Perry JL. Acute and residual effects of alcohol and marijuana, alone and in combination, on mood and performance. Psychopharmacology (Berl) 1994 Jul;115(3):340–9. doi: 10.1007/BF02245075. Epub 1994/07/01. eng. [DOI] [PubMed] [Google Scholar]
- 39.Patrick ME, Schulenberg JE, Martz ME, Maggs JL, O’Malley PM, Johnston LD. Extreme binge drinking among 12th-grade students in the United States: Prevalence and predictors. JAMA Pediatr. 2013 Nov;167(11):1019–25. doi: 10.1001/jamapediatrics.2013.2392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Patrick ME, Terry-McElrath YM, Kloska DD, Schulenberg JE. High-intensity drinking among young adults in the United States: Prevalence, frequency, and developmental change. Alcohol Clin Exp Res. 2016;40(9):1905–12. doi: 10.1111/acer.13164. English. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Barnwell SS, Earleywine M, Wilcox R. Cannabis, motivation, and life satisfaction in an internet sample. Substance abuse treatment, prevention, and policy. 2006 Jan 12;1:2. doi: 10.1186/1747-597x-1-2. Epub 2006/05/26. eng. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Lee CM, Cadigan JM, Patrick ME. Differences in reporting of perceived acute effects of alcohol use, marijuana use, and simultaneous alcohol and marijuana use. Drug Alcohol Depend. doi: 10.1016/j.drugalcdep.2017.08.029. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Patrick ME, Fairlie AM, Lee CM. Motives for simultaneous alcohol and marijuana use among young adults. Addict Behav. 2017 Aug 31;76(363–369):363–9. doi: 10.1016/j.addbeh.2017.08.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Bernstein E, Bernstein J, Feldman J, Fernandez W, Hagan M, Mitchell P, et al. An evidence-based alcohol screening, brief intervention and referral to treatment (SBIRT) curriculum for emergency department (ED) providers improves skills and utilization. Subst Abus. 2007;28(4):79–92. doi: 10.1300/J465v28n04_01.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.D’Onofrio GD, Degutis LC. Preventive care in the emergency department: screening and brief intervention for alcohol problems in the emergency department: a systematic review. Acad Emerg Med. 2002;9:627–638. doi: 10.1111/j.1553-2712.2002.tb02304.x. [DOI] [PubMed] [Google Scholar]
- 46.Longabaugh R, Woolard RE, Nirenbereg TD. Evaluating the effects of a brief motivational intervention for injured drinkers in the emergency department. J Stud Alcohol. 2001;62:806–816. doi: 10.15288/jsa.2001.62.806. [DOI] [PubMed] [Google Scholar]
- 47.Mello MJ, Nirenberg TD, Longabaugh R, Woolard R, Minugh A, Becker B, et al. Emergency department brief motivational interventions for alcohol with motor vehicle crash patients. Ann Emerg Med. 2005;45:620–625. doi: 10.1016/j.annemergmed.2005.01.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.D’Amico EJ, Miles JN, Stern SA, Meredith LS. Brief motivational interviewing for teens at risk of substance use consequences: a randomized pilot study in a primary care clinic. J Subst Abuse Treat. 2008;35(1):53–61. doi: 10.1016/j.jsat.2007.08.008.. [DOI] [PubMed] [Google Scholar]
- 49.Spirito A, Monti PM, Barnett NP, Colby SM, Sindelar H, Rohsenow DJ, et al. A rondomized clinical trial of a brief motivational intervention for alcohol-positive adolescents treated in an emergency department. J Pediatr. 2004;145(3):396–402. doi: 10.1016/j.jpeds.2004.04.057.. [DOI] [PubMed] [Google Scholar]
- 50.Walker DD, Stephens R, Roffman R, DeMarce J, Lozano B, Towe S, et al. Randomized controlled trial of motivational enhancement therapy with nontreatment-seeking adolescent cannabis users: a further test of the teen marijuana check-up. Psychol Addict Behav. 2011;25(3):474–484. doi: 10.1037/a0024076. http://dx.doi.org/10.1037/a0024076. [DOI] [PMC free article] [PubMed] [Google Scholar]