

Abstract
Adipositas cordis is a rare cardiomyopathy characterized by diffuse fatty infiltration of the ventricular myocardium or interventricular septum. This occurs without myocardial cell destruction, unlike arrhythmogenic right ventricular cardiomyopathy. A 40-year-old obese woman was found to have a II/VI systolic murmur that worsened with standing. A transthoracic echocardiogram showed interventricular septal hypertrophy with a preserved left ventricular ejection fraction. Cardiac magnetic resonance imaging revealed a fatty mass in the interventricular septum. An endomyocardial biopsy revealed structurally normal myocytes with diffuse adipose cell infiltration and no evidence of malignant cells. Left and right cardiac catheterizations and stress echocardiography showed no abnormalities. This case shows the importance of considering a broad differential when approaching rare diseases. It also demonstrates the utility of noninvasive imaging and its impact on clinical decision making.
Keywords: adipositas cordis, cardiac MRI, hypertrophic cardiomyopathy, sudden cardiac death, left ventricular ejection fraction
INTRODUCTION
Adipositas cordis is characterized by structurally normal myocytes and diffuse adipose cell infiltration occurring in either ventricular myocardium or the interventricular septum. In some instances, it may provide a diagnostic challenge as it can closely mimic arrhythmogenic right ventricular cardiomyopathy (ARVC). The primary differentiating characteristics are myocyte degeneration and interstitial fibrosis that are present in ARVC and responsible for the higher risk of sudden cardiac death (SCD).3 We describe a case of adipositas cordis evidenced by prominent fatty infiltration of the interventricular septum.
CASE DESCRIPTION
A 40-year-old woman with a body mass index of 30.8 underwent a routine physical. Her medical history included syncope during childhood and palpitations with no family history of SCD. Physical exam revealed a grade II/VI systolic murmur that increased in intensity from squatting to standing. Initial electrocardiogram showed right axis deviation with T-wave inversions in the precordial leads (V1-V4). A transthoracic echocardiogram showed hypertrophy of the interventricular septum, left ventricular ejection fraction of between 60% and 65%, and moderate to severe left ventricular outflow tract obstruction (Figure 1). Cardiac magnetic resonance imaging (CMRI) revealed a 3-cm thick macroscopic fat-containing mass in the interventricular septum (Figure 2). An initial concern for cardiac sarcoma led to a full-body positron emission tomography scan that was negative for malignancy. An endomyocardial biopsy confirmed normal cardiac myocytes diffusely infiltrated with adipose tissue consistent with adipositas cordis (Figure 3). Left and right cardiac catheterizations revealed angiographically normal coronary arteries and stable hemodynamics. Exercise stress echocardiography elicited neither clinical symptoms nor any dynamic left ventricular outflow tract obstruction. The severity of adipose cell infiltration raised concerns about an increased risk of SCD, thus an implantable cardioverter defibrillator was placed for primary prevention.
Figure 1.

Transthoracic echocardiogram showing severely enlarged interventricular septum with a thickness of 3.5 cm (normal range 0.7–1.1 cm).
Figure 2.
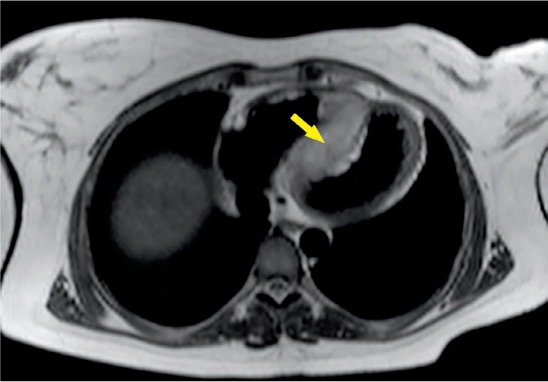
Cardiac magnetic resonance imaging demonstrates a mass centered in the interventricular septum (arrow).
Figure 3.
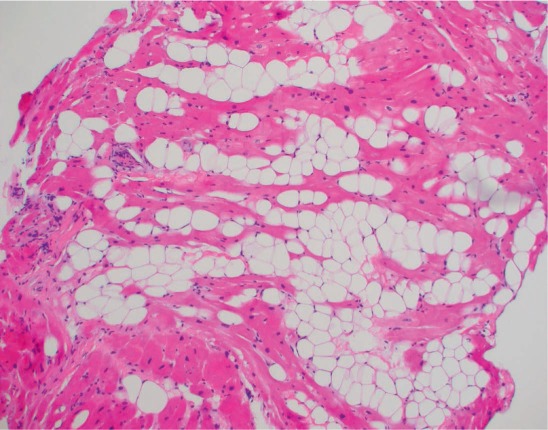
Endomyocardial biopsy (H&E stained sections at 100× magnification), which illustrates abundant benign adipocytes transecting myocytes. The myocytes themselves appear relatively normal without hypertrophy or significant histologic findings.
DISCUSSION
It is of diagnostic and prognostic importance to recognize conditions such as ARVC and adipositas cordis that can cause aggressive myocardial remodeling (through myocardial infiltration) or destruction. Cardiac imaging is crucial when screening for structural heart abnormalities. Echocardiography in our patient demonstrated hypertrophy of the interventricular septum with a thickness of 3.5 cm (Figure 1). These findings and symptoms (syncope with exertion) prompted concerns about possible hypertrophic cardiomyopathy or an infiltrative process. Cardiac MRI was performed and revealed a fat-containing septal mass with no evidence of myocardial hypertrophy. Figure 2 shows how fat signals were detected along the periphery of the septal mass. Further inquiry with a biopsy confirmed the presence of adipose tissue without evidence of malignancy, myocyte fibrosis, or destruction (Figure 3).
Although echocardiography is both noninvasive and cost and time efficient, its limited field of view and soft tissue resolution cannot provide the kind of comprehensive evaluation required when infiltrative processes are suspected. On the other hand, the high spatial and temporal resolution of CMRI allows better visualization and thus a more accurate measure of adipose tissue thickness.6 Therefore, our case demonstrated the importance of using CMRI to achieve better anatomic quality and tissue characterization.
CONCLUSION
This is a rare presentation of adipositas cordis that initially presented with clinical signs and symptoms concerning for hypertrophic obstructive cardiomyopathy. The patient did not meet criteria for arrhythmogenic right ventricular cardiomyopathy since she displayed neither right ventricular structural abnormalities nor cardiac myocyte fibrosis or destruction on biopsy. Additionally, this case demonstrates the importance of understanding the capabilities of available cardiac imaging modalities and the importance of utilizing CMRI for anatomic quality and tissue characterization.
Acknowledgments
We would like to thank Dr. Benjamin D. Mackie for advice regarding the content, edits, and teaching points of this case report. We would also like to thank Dr. Cristiano Caldeira for accepting the patient for initial evaluation. Lastly, those who contributed to the manuscript are greatly appreciated.
Footnotes
Conflict of Interest Disclosure:
The authors have completed and submitted the Methodist DeBakey Cardiovascular Journal Conflict of Interest Statement and none were reported.
REFERENCES
- 1. Liang YH, Zhu J, Zhong DR, . et al. Adipositas cordis sudden death: a series of 79 patients. Int J Clin Exp Pathol. 2015. September 1; 8 9: 10861– 7. [PMC free article] [PubMed] [Google Scholar]
- 2. Rowin EJ, Yucel KE, Salomon R, Maron MS.. Adipositas cordis: an uncommon cardiomyopathy identified by cardiovascular magnetic resonance. Circulation. 2010. November 23; 122 21: 2212– 4. [DOI] [PubMed] [Google Scholar]
- 3. Basso C, Thiene G. Adipositas cordis, fatty infiltration of the right ventricle, and arrhythmogenic right ventricular cardiomyopathy. Just a matter of fat? Cardiovasc Pathol. 2005. Jan-Feb; 14 1: 37– 41. [DOI] [PubMed] [Google Scholar]
- 4. De Scheerder I, Cuvelier C, Verhaaren R, De Buyzere M, De Backer G, Clement D.. Restrictive cardiomyopathy caused by adipositas cordis. Eur Heart J. 1987. June; 8 6: 661– 3. [DOI] [PubMed] [Google Scholar]
- 5. Roberts JD, Veinot JP, Rutberg J, Gollob MH.. Inherited cardiomyopathies mimicking ARVC. Cardiovasc Pathol. 2010. Sep-Oct; 19 5: 316– 20. [DOI] [PubMed] [Google Scholar]
- 6. Hoey ETD, Shahid M, Ganeshan A, Baijal S, Simpson H, Watkin RW.. MRI assessment of cardiac tumours: part 1, multiparametric imaging protocols and spectrum of appearances of histologically benign lesions. Quant Imaging Med Surg. 2014. December; 4 6: 478– 88. [DOI] [PMC free article] [PubMed] [Google Scholar]