

Abstract
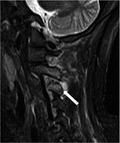
Sagittal T2‐weighted fat saturation magnetic resonance imaging reveals erosion and a high‐intensity area around the C3‐C4 facet joint.
Keywords: facet joint, septic arthritis
A 66‐year‐old Japanese female with no apparent medical history presented with a sudden onset of pain and stiffness on the right side of the neck. Physical examination revealed a body temperature of 38.5°C and an extremely reduced range of motion in her neck but without Kernig's or Brudzinski's signs. There were no wounds on her skin. Laboratory findings revealed a white blood cell (WBC) count of 13 300/μL and a C‐reactive protein (CRP) level of 0.8 mg/dL, which increased to 17 mg/dL after 1 week. The cerebrospinal fluid was clear, and culture results were negative. Computed tomography of the head and neck revealed slight enlargement of the right cervical lymph nodes. Arterial thrombosis and dissection were not observed. On day 2, the presence of methicillin‐susceptible Staphylococcus aureus was confirmed in two sets of blood cultures; therefore, intravenous cefazolin was thus administered (2 g every 8 hours). T2‐weighted fat saturation magnetic resonance imaging (MRI) of the cervical spine revealed erosion and a high‐intensity area around the C3‐C4 articular processes (Figure 1A, arrow), which spread to the paraspinal soft tissue around the right C2‐C3 facets (Figure 1B, arrow). No abnormalities were observed in the vertebral bodies or disks. The transthoracic and transesophageal echocardiography revealed no vegetations. Hence, the patient was diagnosed with septic arthritis of the cervical facets with abscess formation. The patient's symptoms gradually improved after antibiotic administration, and she was discharged without sequelae on day 35. She received intravenous cefazolin for 4 weeks, followed by oral therapy of trimethoprim (320 mg) or sulfamethoxazole (1600 mg) for 2 weeks.
Figure 1.
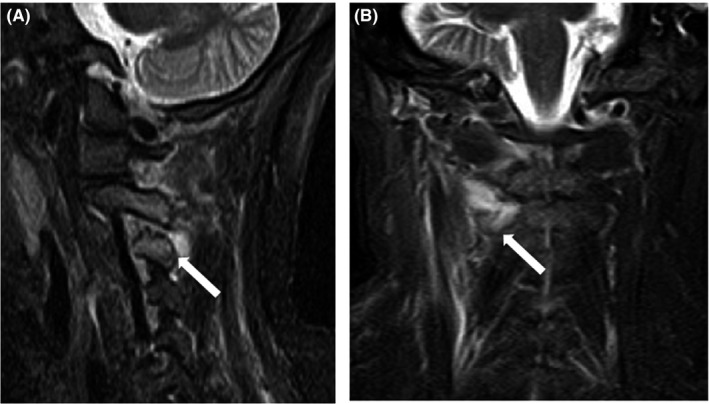
A, Sagittal T2‐weighted fat saturation magnetic resonance imaging reveals erosion and a high‐intensity area around the C3‐C4 articular processes (white arrow). B, The coronal image reveals a high‐intensity area around the right C2‐C3 facet joints (white arrow)
Septic arthritis of the facet joint is an unusual condition, accounting for only 4% of pyogenic spinal infections.1 The average age at onset is 60 years, with 55% of patients older than 60 years. Predisposing factors include immunosuppression, diabetes mellitus, liver cirrhosis, neoplastic disease, and other chronic diseases. Most cases are associated with hematogenous spread, including iatrogenic causes, such as corticosteroid injections and epidural catheterizations. In this case, no wounds and no any predisposing factors were found. A common site of septic arthritis of the facet joint is the lumbar spine, which is reported in approximately 90% cases.2 Only a few cases of cervical facet infection similar to this case have been reported.2, 3, 4, 5 In those cases, unilateral neck pain was the initial presentation, with rapid symptom progression. More than half of the cases were complicated with epidural abscess formation. The majority of cases were caused by S. aureus. Owing to its high sensitivity and specificity, MRI is the most useful method for identifying the infection site. The main treatment includes long‐term intravenous antibiotics. Percutaneous or surgical drainage of abscesses may be helpful; however, this is usually not required.4 In this case, it could be improved only by conservative treatment.
The differential diagnoses of acute nontraumatic neck pain are broad. However, physicians should consider septic arthritis of the cervical facet as a possible differential diagnosis, given that a delay in the diagnosis can easily result in complications such as epidural abscesses,3 joint destruction, and neurologic sequelae; these may ultimately become lethal. Therefore, precise investigation and immediate detection of the infectious source using MRI are essential for an early diagnosis and rapid treatment of the disease.
CONFLICT OF INTEREST
The authors have stated explicitly that there are no conflicts of interest in connection with this article.
Tomoda Y, Kihara Y, Kozuma R, Tanaka K. Septic arthritis of the cervical facets: Unusual cause of neck pain. J Gen Fam Med. 2018;19:143–144. https://doi.org/10.1002/jgf2.181
REFERENCES
- 1. Muffoletto AJ, Ketonen LM, Mader JT, Crow WN, Hadjipavlou AG. Hematogenous pyogenic facet joint infection. Spine. 2001;26:1570–6. [DOI] [PubMed] [Google Scholar]
- 2. Stecher JM, El‐Khoury GY, Hitchon PW. Cervical facet joint septic arthritis: a case report. Iowa Orthop J. 2010;30:182–7. [PMC free article] [PubMed] [Google Scholar]
- 3. Jones JL, Ernst AA. Unusual cause of neck pain: septic arthritis of a cervical facet. Am J Emerg Med. 2012;30:2094. e1‐4. [DOI] [PubMed] [Google Scholar]
- 4. Sethi S, Vithayathil MK. Cervical facet joint septic arthritis: a real pain in the neck. BMJ Case Rep. 2017;2017:1–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Kobayashi T, Miyakoshi N, Abe E, Abe T, Kikuchi K, Shimada Y. Acute neck pain caused by septic arthritis of the lateral atlantoaxial joint with subluxation: a case report. J Med Case Rep. 2015;9:171. [DOI] [PMC free article] [PubMed] [Google Scholar]