

Abstract
The objective of the present study was to investigate the role of blood glucose, lipid metabolism, body mass index (BMI), C-reactive protein (CRP) as well as an interleukin (IL)-17/IL-35 imbalance in the pathogenesis of concurrent gestational diabetes mellitus (GDM) and preeclampsia (PE) (DPE). The mRNA expression of forkhead box protein 3 (FoxP3), IL-35 [including Epstein-Barr virus-induced gene 3 (EBI3) and P35 subunits] and IL-17 in the peripheral blood mononuclear cells of patients with DPE (n=30), GDM (n=33), PE (n=33) and normal pregnancy (n=33) were determined by reverse transcription-quantitative polymerase chain reaction. The serum levels of IL-35, IL-17 and CRP were analyzed using ELISA. Serum total cholesterol (TC), triglyceride (TG), high-density lipoprotein (HDL) and fasting blood glucose (FBG) were also detected. The levels of low-density lipoprotein (LDL) were calculated using the Friedewald formula. Body weight and height were determined in order to calculate the BMI. It was observed that the levels of FBG were markedly elevated in patients with GDM, PE and DPE. In addition, significantly higher serum TG, TC, LDL and very LDL were detected in patients with GDM, PE and DPE compared with those in subjects with normal pregnancies. By contrast, the concentration of HDL was lower in the patient groups. In addition, higher BMI values were identified in patients with GDM, PE and DPE. A decreased expression of FoxP3, P35 and EBI3 mRNA, and an elevated expression of IL-17 in PBMCs was detected in patients with GDM, PE and DPE. In addition, higher serum levels of IL-17 and CRP, as well as lower levels of IL-35, were observed. Furthermore, in patients with DPE, positive correlations of diastolic blood pressure with IL-17 levels, BMI and TG, as well as IL-17 levels with BMI and proteinuria were identified. In conclusion, the present study indicated that abnormal maternal lipids, hyperglycemia, high BMI, high CRP and IL-17/IL-35 imbalance may have a role in the pathophysiology of DPE. Therefore, pregnant women and clinicians should be made aware that maternal hyperlipidaemia, hyperglycemia, high BMI, high CRP levels and IL-17/IL-35 imbalance may lead to DPE.
Keywords: pregnancy, maternal lipids, interleukin-35/interleukin-17, body mass index, gestational diabetes complicated by preeclampsia
Introduction
Pregnancy is a time of tremendous stress on the body of the mother, involving a substantial increase in the workload of various different organs (1). Therefore, organ systems that are well controlled in the non-pregnant state may become dysregulated during pregnancy, which may result in metabolic diseases, including diabetes mellitus (2). The dysregulation of organ systems during pregnancy may cause significant harm to the mother and/or the fetus (2). The late stages of pregnancy are catabolic and associated with the elevation of blood glucose. Gestational diabetes mellitus (GDM) is a common metabolic complication during pregnancy. Hyperglycemia has prominent effects on the mother, the course of the pregnancy and the fetus (3). Patients with gestational and pre-GDM have a greater risk for preeclampsia (PE), which is a hypertensive syndrome associated with proteinuria (4). Since a long-term consequence of diabetes mellitus is the damage to small blood vessels, it is hypothesized that PE results from endothelial cell injury as a consequence of ischemia (5). Abnormalities in the process of implantation appear to set in motion events that lead to the occurrence of PE from gestation week 20 (6). Clinical and experimental studies have suggested that GDM and PE share pathophysiological features, including systemic endothelial inflammation and dyslipidemia. These conditions are associated with augmented risks for cardiovascular morbidity and mortality later in life (7–9). However, few studies have assessed risk factors for concurrent GDM and PE (DPE).
In recent years, there has been an increased focus on the role of the maternal immune system in inflammation and endothelial dysfunction, which is associated with the development of DPE (10,11). The immune system has a major role in normal pregnancy (12). During pregnancy, the systemic maternal immune system is altered, and maternal T cells acquire a transient state of tolerance that is specific for paternal alloantigens (13). CD4+ T, type 17 T-helper (Th17) and regulatory T (Treg) cells have an important role in maintaining self-tolerance. The identification of Th17 and Treg cells has opened up a broad field of research into the potential roles of these cells in controlling disorders during pregnancy. An important characteristic of PE is an alteration in the prevalence of Th17 and Treg cells, which may contribute to the development of maternal systemic inflammation (14,15). The interleukin (IL)-17 cytokine is produced by Th17 cells, which are potent inflammatory factors for activating the adaptive immune response. Treg cells are a major component in establishing immune tolerance (16,17). IL-35 is a newly identified immunosuppressive cytokine secreted from Treg cells, and consists of p35 and Epstein-Barr virus-induced gene 3 (EBI3) subunits (18,19). C-reactive protein (CRP) is a systemic inflammatory marker primarily synthesized in the liver (20). In recent years, the role of immune activation and inflammation in the pathogenesis of DPE has gained increasing attention.
Recent studies have reported that an abnormal maternal lipid profile, including total cholesterol (TC), triglyceride (TG), low-density lipoprotein (LDL), very LDL (VLDL) and high-density lipoprotein (HDL), increase the health risks associated with pregnancy (21,22). The accumulation of cholesterol and TGs may cause damage to endothelial function. It has been reported that lipid profile abnormalities in maternal patients with GDM increase the risk of vascular injury, which may lead to endothelial dysfunction, a pathogenic factor of PE (23). Lipids constitute a large part of the arterial wall, as do plasma and intracellular membranes; therefore, lipid abnormalities may lead to vascular damage, which has a critically important role in the pathogenesis of GDM (24). Therefore, DPE may be associated with lipid profile abnormalities and vascular dysfunction.
Obesity and excessive gestational weight gain (GWG) are important preventable risk factors for adverse maternal and neonatal outcomes (25). Excessive maternal GWG and obesity are associated with an increased risk of metabolic and immunological dysfunction (26). Previous studies have indicated that excessive GWG and obesity during pregnancy are associated with increased secretion of adipokines and inflammatory cytokines (27,28). However, the pathophysiological mechanisms that underlie an increased body mass index (BMI) remain to be fully elucidated. Abnormal lipid levels and immunological dysfunction are likely to be important factors that contribute to disorders during pregnancy. At present, there is limited information on the effects of the immune mechanisms that link lipid metabolism and high BMI to the pathogenesis of DPE. The present study aimed to investigate the association between the levels of maternal lipids, blood glucose, IL-17/IL-35 and BMI in order to examine the risk factors for DPE.
Materials and methods
Study population
The present study comprised 30 patients with DPE, 33 patients with GDM, 33 patients with PE and 33 subjects with normal pregnancy were enrolled from regular checkups performed in the Department of Obstetrics of the Maternity and Child Health Hospital of Zhenjiang (Jiangsu, China) between January 2013 and August 2016. PE was considered when hypertension (≥140/90 mmHg) was detected on two separate occasions with an interval of >6 h. Proteinuria was considered to be present when the 24-h total urinary protein excretion was ≥300 mg/24 h. PE was categorized as severe when the systemic blood pressure was ≥160/110 mmHg, or if there was consistent proteinuria (>5 g/24 h). GDM was diagnosed using the criteria of the American Diabetes Association (ADA), where, following a 75-g oral glucose tolerance test during 24–28 weeks of gestation, one of the three following categories was fulfilled: Based on the one-step approach recommended by the ADA, the pregnant women were defined as having GDM if they had at least one abnormal high glucose value out of three 75 g OGTT, fasting blood glucose (FBG), ≥5.1 mmol/l, 1 h post 75-g oral glucose load, ≥10.0 mmol/l, and 2 h post 75-g oral glucose load, ≥8.5 mmol/l (27). Patients with cardiovascular, renal, metabolic disease and an abortion history were excluded from the study. None of the patients were undergoing treatment or received any medication within 2 months prior to sample collection. The ethics committee of the Maternity and Child Health Hospital (Zhenjiang, China) approved the study protocol, and all participants provided written informed consent. Their clinical characteristics are listed in Table I.
Table I.
Demographic data of the pregnant subjects.
| Parameter | NP (n=33) | GDM (n=33) | PE (n=33) | DPE (n=30) |
|---|---|---|---|---|
| Maternal age (years) | 28.70±1.16 | 29.20±1.03 | 28.20±6.97 | 29.90±1.37 |
| Gestational age (weeks) | 38.57±0.98 | 38.70±1.40 | 36.47±1.60 | 38.10±1.20 |
| Nulliparous | 23 (69.7) | 20 (60.6) | 19 (57.6) | 21 (70.0) |
| Smokers | 0 (0.0) | 1 (3.0) | 1 (3.0) | 1 (3.3) |
| Proteinuria | 0.080±0.01 | 0.92±0.61 | 4.27±1.04a,b | 2.91±0.64a |
P<0.05, vs. NP and GDM
P<0.05, vs. DPE. Values are expressed as n (%) or the mean ± standard deviation. NP, normal pregnancy; PE, preeclampsia; GDM, gestational diabetes mellitus; DPE, GDM with PE.
Blood sample preparation
Venous blood samples (10 ml) were obtained by venipuncture from patients with GDM, PE, DPE and normal pregnancy. Following centrifugation for 10 min at 3,000 × g at 20°C, the serum was stored at −80°C for later analysis of the cytokines. Peripheral blood mononuclear cells (PBMCs) were isolated using the standard Ficoll-Hypaque method (11).
Reverse transcription-quantitative polymerase chain reaction (RT-qPCR)
Total RNA was isolated from PBMCs using TRIzol reagent (Invitrogen; Thermo Fisher Scientific, Inc., Waltham, MA, USA). Complementary (c)DNA was synthesized using the High-Capacity cDNA Reverse Transcription kit (Applied Biosystems; Thermo Fisher Scientific, Inc.) according to the manufacturer's instructions. The mRNA levels of forkhead box P3 (FoxP3), P35, EBI3, IL-17 and β-actin were determined using the SYBR Green two-step RT-qPCR kit (Bio-Rad Laboratories, Inc., Hercules, CA, USA) according to the manufacturer's protocol and as previously described (11). β-actin was used as a housekeeping gene. The primer sequences for FoxP3, P35, EBI3, IL-17 and β-actin are listed in Table II. Quantification was performed using the 2−∆∆Cq method (29).
Table II.
Primers for polymerase chain reaction.
| Gene | Forward primer | Reverse primer |
|---|---|---|
| P35 | 5′-TCCTCCCTTGAAGAACCGGA-3′ | 5′-TGACAACGGTTTGGAGGGAC-3′ |
| EBI3 | 5′-TCCTTCATTGCCACGTACAG-3′ | 5′-GCTCTGTTATGAAAGGCACG-3′ |
| FoxP3 | 5′-TGAGAAGGACAGGGAGCCAA-3′ | 5′-GAGAAGCTGAGTGCCATGCA-3′ |
| IL-17 | 5′-CTCCAGAAGGCCCTCAGACTAC-3′ | 5′-GGGTCTTCATTGCGGTGG-3′ |
| β-actin | 5′-TGGCACCCAGCACAATGAA-3′ | 5′-CTAAGTCATAGTCCGCCTAGAAGCA-3′ |
FoxP3, forkhead box protein 3; EBI3, Epstein-Barr virus-induced gene 3; IL, interleukin.
Analysis of cytokines and CRP using ELISA
The concentrations of serum IL-35, IL-17 and CRP were analyzed using a commercial ELISA 3 plex sample kit according to the manufacturer's protocols (IL-17 cat. no. KAC1591; CRP cat. no. 88-7502-28; IL-35 cat. no. 439508 LEGEND MAX™ Human; Thermo Fisher Scientific, Inc, Waltham, MA, USA). All samples were analyzed in duplicate.
Biochemical analysis
The levels of serum TG, TC and HDL were measured using an automatic biochemistry analyzer (AU5800; Beckman Coulter, Inc., Brea, CA, USA). The levels of LDL and VLDL were calculated using the Friedewald equation (30). The glucose levels in maternal blood were determined using an enzymatic system (TMRUSGT15-0901; Beckman Coulter, Inc.).
BMI
The BMI was calculated using the Friedewald formula (kg/m2) and according to the Institute of Medicine classification and the published recommended guidelines for gestational weight gain (30), the patients were categorized as follows: Underweight, <18.5 kg/m2; normal weight, 18.5–24.9 kg/m2; overweight, 25.0–29.9 kg/m2 and obese, ≥30.0 kg/m2. Maternal patients with missing data regarding height, weight prior to pregnancy or time of delivery were excluded from the sample.
Statistical analysis
The statistical significance of differences among groups was assessed with GraphPad Prism (version 5.0; GraphPad Software, Inc., La Jolla, CA, USA). Values are expressed as the mean ± standard deviation. P<0.05 was considered to indicate a statistically significant difference. One-way analysis of variance with a post-hoc Turkey's test was performed to determine the differences in the means among multiple groups and was used for assessment of differences between two groups. Pearson's correlation coefficients were calculated for the assessment of correlations between variables.
Results
Elevated blood pressure in patients with DPE
In the present study, it was observed that the SBP and DBP in patients with PE and DPE were significantly higher compared with NP and patients with GDM. In addition, it was identified that the mean arterial pressure (MAP) were significantly higher in patients with GDM, PE and DPE compared with NP. These differences in MAP were significantly higher in patients with PE compared to patients with DPE. Of note, the MAP of patients with GDM was 97.50±10.34 mmHg, and an MAP of ≥85 mmHg is indicative of a tendency to develop PE (1) (Fig. 1).
Figure 1.

Blood pressure in patients with GDM, PE and DPE. (A) The SBP, (B) DBP and (C) MAP of the patients in each group. GDM, gestational diabetes mellitus; PE, preeclampsia; DPE, GDM with PE; SBP, systolic blood pressure; DBP, diastolic blood pressure; MAP, mean arterial pressure; NP, normal pregnant subjects.
Elevated levels of FBG in patients with DPE
The glucose levels in maternal blood were determined by ELISA. As indicated in Fig. 2, elevated levels of FBG were detected in patients with GDM, PE and DPE compared with NP. Furthermore, patients with DPE and GDM also exhibited elevated levels of FBG compared with PE. These results suggest that DPE and GDM have similar metabolic disorder characteristics by high level of blood glucose. It has been reported that elevated blood glucose levels of GDM have effects on other tissues (31). Therefore, the resultant hypertrophy and proliferation of vascular smooth muscle may contribute to hypertension.
Figure 2.
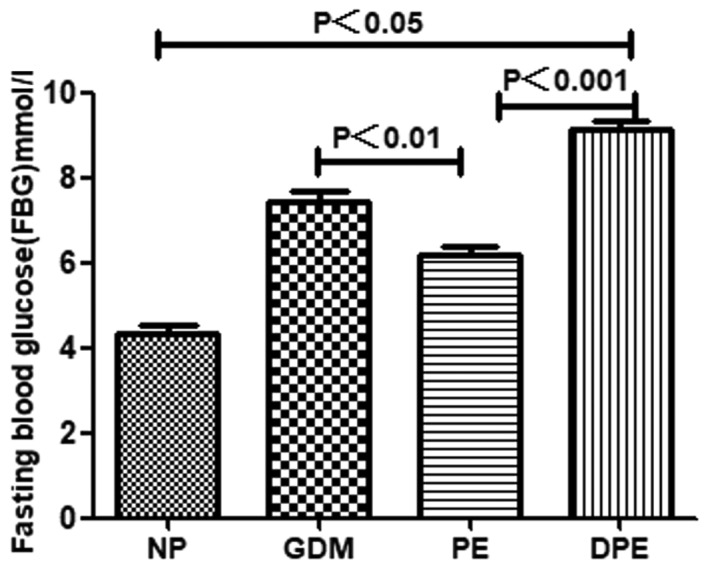
Levels of FBG in patients with GDM, PE and DPE. FBG, fasting blood glucose; GDM, gestational diabetes mellitus; PE, preeclampsia; DPE, GDM with PE; NP, normal pregnant subjects.
Hyperlipidaemia and high BMI in patients with DPE
As presented in Fig. 3, significantly higher levels of serum TG were identified in patients with GDM, PE and DPE compared with NP and the difference in TG were also significantly higher in GDM compared with PE and DPE. There were significantly higher levels of serum TC in patients with GDM, PE and DPE compared with NP and this difference of TC were also significantly higher in DPE compared with PE and GDM. In addition, there were significantly higher levels of serum LDL in patients with GDM, PE and DPE compared with NP and this difference LDL were also significantly higher in PE compared with DPE and GDM. Significantly higher levels of serum VLDL in patients with GDM, PE and DPE were observed when compared with NP and VLDL levels were also significantly higher in PE compared with GDM. In addition, higher BMI values were identified in patients with GDM, PE and DPE. Of note, lower concentrations of HDL were detected in patients with GDM, PE and DPE compared with those in subjects with normal pregnancy.
Figure 3.

Lipid profile and BMI of patients with GDM, PE and DPE. Levels of (A) TG, (B) TC, (C) LDL, (D) VLDL and (E) Serum HDL of patients in each group. (F) The BMI of patients in the GDM, PE and DPE group upon enrollment. BMI body mass index; DPE, GDM with PE; GDM, gestational diabetes mellitus; PE, preeclampsia; TG, triglyceride; TC, total cholesterol; LDL, low-density lipoprotein; VLDL, very LDL; HDL, high-density lipoprotein; NP, normal pregnant subjects.
mRNA expression of FoxP3, P35, EBI3 and IL-17 in patients with DPE
As previous studies have indicated a role for the IL-17/IL-35 imbalance in the pathogenesis of PE (11), possible alterations of the mRNA expression of FoxP3, P35, EBI3 and IL-17 were examined in the patients with GDM, PE and DPE. As indicated in Fig. 4, the mRNA expression of P35, EBI3 and FoxP3, which is characteristic of Treg cells, was decreased, while the expression of IL-17 was elevated in patients with GDM, PE and DPE compared with NP. These results suggested a potential involvement of the IL-17/IL-35 imbalance in GDM, PE and DPE.
Figure 4.

mRNA expression of FoxP3, P35, EBI3 and IL-17 in patients with GDM, PE and DPE. mRNA Levels of (A) IL-17, (B) P35, (C) EB13 and (D) FoxP3 in each group. FoxP3, forkhead box protein 3; EBI3, Epstein-Barr virus-induced gene 3; IL, interleukin; GDM, gestational diabetes mellitus; PE, preeclampsia; DPE, GDM with PE; NP, normal pregnant subjects.
Serum cytokine and CRP concentration
The production of the Th17-associated cytokines IL-17 and IL-35 by Tregs in patients with GDM, PE and DPE are indicated in Fig. 5. Significantly higher serum levels of IL-17 were observed in patients with GDM, PE and DPE compared with NP. This difference in IL-17 was also significantly higher in PE and DPE compared with GDM (Fig. 5A). By contrast, lower levels of IL-35 were observed in patients with GDM, PE and DPE compared with NP and levels of IL-35 were also significantly lower in PE and DPE compared with GDM (Fig. 5B). The levels of CRP, a systemic inflammatory marker, were significantly elevated in patients with GDM, PE and DPE. CRP was also significantly higher in PE and DPE compared with GDM (Fig. 5C). These results suggest an abnormal immune response in patients with GDM, PE and DPE, which is characteristic of a shift to Th17-type immunity and systemic inflammation.
Figure 5.

Serum levels of CRP and cytokines IL-17 and IL-35 in patients with GDM, PE and DPE. Serum levels of (A) IL-17, (B) IL-35 and. (C) CRP of patients in each group. CRP, C-reactive protein; IL, interleukin; GDM, gestational diabetes mellitus; PE, preeclampsia; DPE, GDM with PE; NP, normal pregnant subjects.
Correlation of DBP with IL-17, BMI and TG, as well as IL-17 with proteinuria and BMI in patients with DPE
As indicated in Fig. 6, positive correlations were identified between the DBP and the levels of IL-17 (r=0.8718 and P<0.001), the BMI (r=0.6575 and P<0.05) and TG (r=0.8058 and P<0.001). In addition, positive correlations between IL-17 levels and the BMI as well as between IL-17 levels and the presence of proteinuria were identified in patients with DPE (r=0.9020 and r=0.7666, respectively; P<0.01 for each). Based on these observations, it was hypothesized that elevated IL-17, BMI and TG are probably involved in the development of endothelial dysfunction with major effects, including elevated DBP and proteinuria.
Figure 6.

Correlations between various parameters in patients with DPE. (A) A significant positive correlation was detected between elevated IL-17 and DBP. (B) Positive correlation between increased BMI and DBP. (C) Positive correlation between elevated TG levels and DBP. (D) There was a significant positive correlation between serum IL-17 and proteinuria in patients with DPE. (E) A positive correlation was detected between serum IL-17 and the BMI. IL, interleukin; BMI, body mass index; TG, triglyceride; DBP, diastolic blood pressure; DPE, gestational diabetes mellitus with preeclampsia.
Discussion
GDM is a group of metabolic disorders characterized by hyperglycemia. GDM is 6–10 times more common than pre-gestational diabetes mellitus. GDM occurs in 4.3–17.5% of all pregnancies in China (32). Hyperglycemia has prominent effects on the mother, the course of the pregnancy and the fetus (33). In the present study, elevated levels of FBG were detected in patients with GDM, PE and DPE compared with those in subjects with normal pregnancy. Furthermore, the levels of FBG were also increased in patients with DPE and GDM compared with those in patients with PE. These results suggest that high blood glucose levels during pregnancy are common in patients with GDM. Of note, it was reported that elevated blood glucose levels in GDM patients affect other tissues, particularly small blood vessels (34). Therefore, the resultant hypertrophy and proliferation of vascular smooth muscle may contribute to the association between GDM and the subsequent development of PE (35). Although the mechanisms remain to be fully elucidated, several studies have suggested that hyperglycemia has a role in the etiology of these diseases (36,37). A hypothesis for this observation is that when blood glucose levels remain excessively high for extended periods of time, this induces damage to blood vessels, particularly small blood vessels (38). Furthermore, the present study identified that MAP values were significantly higher in patients with GDM, PE and DPE compared with those in normal pregnancy. In particular, the MAP of patients with GDM (97.50±10.34) was ≥85 mmHg, indicative of a tendency to develop PE (9). These results suggest that hyperglycemia in GDM may lead to vascular dysfunction and the subsequent complication of PE.
In the present study, significantly higher levels of serum TG, TC, LDL and VLDL were identified in patients with GDM, PE and DPE compared with those in subjects with normal pregnancies. By contrast, decreased HDL concentrations were identified in patients with GDM, PE and DPE. These results indicate that high TG, TC, LDL and VLDL, as well as low HDL levels, may be associated with DPE. The HDL concentration generally increases throughout pregnancy (39); HDL is a vasodilator, which may reverse cholesterol transport by carrying excess, potentially harmful cholesterol to the liver for excretion (40). A number of HDL constituents may interact with the vascular endothelium (41,42). Various of studies have reported that elevated TG, TC, LDL and VLDL levels and decreased HDL levels may serve a role in the development of endothelial damage and vascular dysfunction (43,44). Obesity, which is primarily caused by intake and storage of nutritional substrates, is an important public health issue (45). In the present study, the patients with DPE had an elevated BMI. In pregnant women who are obese, the plasma levels of TG and VLDL are higher, and the concentration of HDL is lower compared with those in non-obese pregnant women (46). It is possible that in pregnant women who are obese, the HDL concentration may be insufficient to fully protect the maternal vascular endothelium. Obese pregnant women are at a higher risk of endothelial dysfunction, thereby increasing the risk of developing DBP (47). Furthermore, positive correlations between DBP and BMI, and between DBP and TG were observed in patients with DPE. The present study indicated that abnormal lipid metabolism and elevated BMI are also risk factors for DBP.
Normal pregnancy is a state of immune tolerance (48). Maternal T lymphocytes acquire a transient state of tolerance for paternal alloantigens. T cells are a major component of the immune response and have an important role at the maternal-fetal interface (49). The impaired recruitment of T cells in the peripheral blood has been associated with disorders during pregnancy and the overactivation of the immune system (50). Treg cells may have an important role in avoiding maternal immune self-reactivity and establishing immune tolerance during pregnancy (51). The expression of FoxP3 is regarded as a characteristic of Treg cells, which distinguishes Treg cells from activated CD4+ T cells (51). IL-35 is only produced by Treg cells; the biological functions of IL-35 include the direct suppression of the proliferation and development of Th17 cells (52). A previous study has demonstrated that Treg cells and Th17 significantly increase and decrease, respectively, in a balanced state (Th17 and Treg cells form a complex and dynamic network to maintain homeostasis during normal pregnancy (53). On the other hand, Th17 plays a critical role in the induction of inflammation and Treg cells are essential for maintaining pregnancy and regulating inflammation. A previous study by our group demonstrated a decreased number of Treg cells in pregnancies with complications, including PE and miscarriage (54). In the present study, it was observed that the expression of FoxP3 and IL-35 declined in patients with GDM and DPE, suggesting that a reduced production of Treg cells may lead to inflammation. IL-17 and CRP are involved in low-grade inflammation (55). IL-17 is a characteristic inflammatory cytokine expressed by Th17 cells. IL-17 is hypothesized to serve as a link between somatic tissues and the immune response (56). The present study revealed that the levels of IL-17 and CRP are elevated in patients with DPE, whereas these factors are downregulated in a normal pregnancy. However, the levels of IL-17 and CRP are also significantly lower in normal pregnancy compared with non-pregnant individuals. Similar to other gestation-associated diseases (including PE and GDM), DPE was associated with a decreased expression of FoxP3 and IL-35, and an increased expression of IL-17. Therefore, maternal immune tolerance that is present in normal pregnancies may be less effective with concurrent DPE. The results of the present study suggest that an imbalance between pro-inflammatory factors (e.g., IL-17 and CRP) and anti-inflammatory factors (e.g., IL-35) is implicated in the pathogenesis of GDM, PE and DPE. Th17 cells may serve important roles in the pathogenesis of numerous inflammatory conditions, which are associated with complications during pregnancy. IL-35 is a newly identified immunosuppressive cytokine exclusively produced by Treg cells. It has been demonstrated that lymphocytes are endogenously polarized to IL-17 to induce a decrease in IL-35 (57), in patients with DPE. These data indicate that the blood environment characterized by increased Th17 and decreased Treg may contribute to the imbalance of circulating Th17/Treg in patients with DPE. CRP is a systemic inflammatory marker and a component of the innate immune system. Elevated levels of CRP may reflect an inflammatory state in women with DPE (58). Previous studies observed that the cytokine balance between Th1 cytokines (e.g., IL-2 and interferon-γ) and Th2 cytokines (e.g., IL-4) was broken in pregnant women with diabetes. Several studies have reported on this Th1/Th2 (IL-4) imbalance, also known as the pro-inflammatory/anti-inflammatory cytokine imbalance, in diabetes (59). Therefore, the role of immune activation and inflammation in the pathogenesis of DPE is worthy of further investigation. Furthermore, the present study indicated that enhanced levels of IL-17 in patients with DPE were positively correlated with increased proteinuria, DBP and BMI. These results suggested that a systemic inflammatory state may lead to damage to blood vessels and endothelial dysfunction. It appears that an abnormal maternal lipid profile, high BMI and an IL-17/IL-35 imbalance are involved in the development of endothelial dysfunction. These factors have major effects that lead to elevated blood pressure and proteinuria, as those parameters reflect endothelial function (60).
Of note, the present study has certain limitations. First, all of the study participants were recruited at one hospital. Furthermore, the number of recruited patients was relatively small. Therefore, further studies with a large sample size should be performed in the future.
In summary, the present study demonstrated that the DPE group was similar to the PE group with regard to systemic inflammation, as indicated by the increased levels of IL-17 and CRP, as well as the decreased levels of FoxP3 and IL-35. It was indicated that an abnormal maternal lipid profile, high BMI, hyperglycemia and low HDL may be involved in the endothelial injury that is associated with the pathogenesis of DPE. In addition, positive correlations of the DBP with the BMI, TG and IL-17 levels were observed. There were also positive correlations between IL-17 levels and BMI, as well as between IL-17 levels and proteinuria. These results suggest that systemic inflammation and endothelial dysfunction may be involved in the pathogenesis of DPE. Further studies are required to link systemic inflammation and endothelial dysfunction with the mechanisms of DPE.
Acknowledgements
Not applicable.
Glossary
Abbreviations
- PE
preeclampsia
- GDM
gestational diabetes mellitus
- DPE
GDM with PE
- PBMCs
peripheral blood mononuclear cells
- Th
T helper
- IL-17
interleukin-17
- EBI3
Epstein-Barr virus-induced gene 3
- Treg cells
regulatory T cells
- FoxP3
forkhead box protein 3
- BP
blood pressure
- MAP
mean arterial pressure
- BMI
body mass index
- CRP
C-reactive protein
Funding
The present study was supported by the Science and Technology Bureau of Zhenjiang Mandatory Research Projects (grant no. SH2016054) and the Maternal and Child Health Research Projects of Jiangsu Province (grant nos. F201502, F201604 and F201435).
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Authors' contributions
WC and XW conceived the study, designed the experiments, analyzed the data and prepared the manuscript. WC was a major contributor in writing the manuscript. TC, BX and YH selected the subject and obtained samples for the present study. WX and FF performed the experiments. SZ and ZW collected the clinical data. All authors have read and approved the manuscript.
Ethics approval and consent to participate
The ethics committee of the Maternity and Child Health Hospital (Zhenjiang, China) approved the study protocol, and all participants provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
References
- 1.Kopelman PG. Obesity as a medical problem. Nature. 2000;404:635–643. doi: 10.1038/35007508. [DOI] [PubMed] [Google Scholar]
- 2.Catalano PM. Trying to understand gestational diabetes. Diabet Med. 2014;31:273–281. doi: 10.1111/dme.12381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Cundy T, Ackermann E, Ryan EA. Gestational diabetes new criteria may tripli the prevalence but effect on outcomes is unclear. BMJ. 2014;348:g1567. doi: 10.1136/bmj.g1567. [DOI] [PubMed] [Google Scholar]
- 4.Steegers EA, von Dadelszen P, Duvekot JJ, Pijnenborg R. Preeclampsia. Lancet. 2010;376:631–644. doi: 10.1016/S0140-6736(10)60279-6. [DOI] [PubMed] [Google Scholar]
- 5.Committee Opinion No. 638: First-trimester risk assessment for early-onset preeclampsia. Obstet Gynecol. 2015;126:e25–e27. doi: 10.1097/AOG.0000000000001049. [DOI] [PubMed] [Google Scholar]
- 6.Lo JO, Mission JF, Caughey AB. Hypertensive disease of pregnancy and maternal mortality. Curr Opin Obstet Gynecol. 2013;25:124–132. doi: 10.1097/GCO.0b013e32835e0ef5. [DOI] [PubMed] [Google Scholar]
- 7.Chen CW, Jaffe IZ, Karumanchi SA. Preeclampsia and cardiovascular disease. Cardiovasc Res. 2014;101:579–586. doi: 10.1093/cvr/cvu018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Engeland A, Bjørge T, Daltveit AK, Skurtveit S, Vangen S, Vollset SE, Furu K. Risk of diabetes after gestational diabetes and preeclampsia. A registry-based study of 230,000 women in Norway. Eur J Epidemiol. 2011;26:157–163. doi: 10.1007/s10654-010-9527-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Jiwani A, Marseille E, Lohse N, Damm P, Hod M, Kahn JG. Gestational diabetes mellitus: Results from a survey of country prevalence and practices. J Matern Fetal Neonatal Med. 2012;25:600–610. doi: 10.3109/14767058.2011.587921. [DOI] [PubMed] [Google Scholar]
- 10.Pantham P, Aye IL, Powell TL. Inflammation in maternal obesity and gestational mellitus. Placenta. 2015;36:709–715. doi: 10.1016/j.placenta.2015.04.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Cao W, Wang X, Chen T, Zhu H, Xu W, Zhao S, Cheng X, Xia L. The expression of Notch/Notch Ligand, IL-35, IL-17, and Th17/Treg in preeclampsia. Dis Markers. 2015;2015:316182. doi: 10.1155/2015/316182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gaffen SL, Jain R, Garg AV, Cua DJ. The IL-23-IL-17 immune axis: From mechanisms to therapeutic testing. Nat Rev Immunol. 2014;14:585–600. doi: 10.1038/nri3707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Saito S. Th17 cells and regulatory T cells: New light on pathophysiology of preeclampsia. Immunol Cell Biol. 2010;88:615–617. doi: 10.1038/icb.2010.68. [DOI] [PubMed] [Google Scholar]
- 14.Laresgoiti-Servitje E. A leading role for the immune system in the pathophysiology of preeclampsia. J Leukoc Biol. 2013;94:247–257. doi: 10.1189/jlb.1112603. [DOI] [PubMed] [Google Scholar]
- 15.Gratz IK, Rosenblum MD, Maurano MM, Paw JS, Truong HA, Marshak-Rothstein A, Abbas AK. Self antigen controls the balance between effector and regulatory T cells in peripheral tissues. J Immunol. 2014;192:1351–1355. doi: 10.4049/jimmunol.1301777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hanidaizar D, Koulmanda M. Inflammation and the balance of Treg and Th17 cells in transplant rejection and tolerance. Curr Opin Organ Transplant. 2010;15:411–415. doi: 10.1097/MOT.0b013e32833b7929. [DOI] [PubMed] [Google Scholar]
- 17.Erlebacher A. Mechanisms of T cell tolerance towards the allogeneic fetus. Nat Rey Immunol. 2013;13:23–33. doi: 10.1038/nri3361. [DOI] [PubMed] [Google Scholar]
- 18.Collison LW, Workman CJ, Kuo TT, Boyd K, Wang Y, Vignali KM, Cross R, Sehy D, Blumberg RS, Vignali DA. The inhibitory cytokine IL-35 contributes to regulatory T-cell function. Nature. 2007;450:566–569. doi: 10.1038/nature06306. [DOI] [PubMed] [Google Scholar]
- 19.Collison LW, Chaturvedi V, Henderson AL, Glacomin PR, Guy C, Bankorti J, Finkelstein D, Forbes K, Workman CJ, Brown SA, et al. IL-35-mediated induction of a potent regulatory T cell population. Nat Immunol. 2010;11:1093–1101. doi: 10.1038/ni.1952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kashanian M, Aghbali F, Mahahi N. Evaluation of the diagnostic value of the first trimester maternal serum high-sensitivity C-reactive protein level for prediction of pre-eclampsia. J Obstet Gynaecol Res. 2013;39:1549–1554. doi: 10.1111/jog.12105. [DOI] [PubMed] [Google Scholar]
- 21.Zeb A. Triglyceride composition, oxidation and oxidation compounds in camellia oil using liquid chromatography-mass spectrometry. Chem Phys Lipids. 2012;165:608–614. doi: 10.1016/j.chemphyslip.2012.03.004. [DOI] [PubMed] [Google Scholar]
- 22.Gohil JT, Patel PK, Gupta P. Estimation of lipid profile in subjects of pre-eclampsia. J Obstet Gynaecol India. 2011;61:399–403. doi: 10.1007/s13224-011-0057-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Gaillard R, Durmuş B, Hofman A, Mackenbach JP, Steegers EA, Jaddoe VW. Risk factors and outcomes of maternal obesity and excessive weight gain during pregnancy. Obesity (Silver Spring) 2013;21:1046–1055. doi: 10.1002/oby.20088. [DOI] [PubMed] [Google Scholar]
- 24.Guariguata L, Whiting DR, Hambleton I, Beagley J, Linnenkamp U, Shaw JE. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res Clin Pract. 2014;103:137–149. doi: 10.1016/j.diabres.2013.11.002. [DOI] [PubMed] [Google Scholar]
- 25.Flegal K, Graubard B, Williamson D, Gail M. Excess deaths associated with underweight, overweight, and obesity. JAMA. 2005;293:1861–1867. doi: 10.1001/jama.293.15.1861. [DOI] [PubMed] [Google Scholar]
- 26.Kotsis V, Stabouli S, Papakatsika S, Rizos Z, Parati G. Mechanisms of obesity-induced hypertension. Hypertens Res. 2010;33:386–393. doi: 10.1038/hr.2010.9. [DOI] [PubMed] [Google Scholar]
- 27.American Diabetes Association: Standards of medical care in diabetes-2009. Diabetes Care. 2009;32(Suppl 1):S13–S61. doi: 10.2337/dc09-S013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Far Arjmandi M, Ziaei S, Kazemnejad A. The impact of maternal age, pre-pregnancy body mass index, weight gain and parity on glucose challenge test (GCT) Int J Fertil Steril. 2012;5:207–2010. [PMC free article] [PubMed] [Google Scholar]
- 29.Livak KJ, Schmittgen TD. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) method. Methods. 2001;25:402–408. doi: 10.1006/meth.2001.1262. [DOI] [PubMed] [Google Scholar]
- 30.Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;18:499–502. [PubMed] [Google Scholar]
- 31.Implementation Protocol Guidelines for Healthcare Professionals. International Diabetes Federation; Brussels: 2015. International Diabetes Federation: Recommended protocol for screening, management and follow up of women with GDM. [Google Scholar]
- 32.Zhu WW, Fan L, Yang HX, Kong LY, Su SP, Wang ZL, Hu YL, Zhang MH, Sun LZ, Mi Y, et al. Fasting plasma glucose at 24–28 weeks to screen for gestational diabetes mellitus: New environment from China. Diabetes Care. 2013;36:2038–2040. doi: 10.2337/dc12-2465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Lindsay KL, Brennan L, Kennelly MA, Curran S, Coffey M, Smith TP, Foley ME, Hatunic M, McAuliffe FM. Maternal metabolic response to dietary treatment for impairedglucose tolerance and gestational diabetes mellitus. Ir J Med Sci. 2018 doi: 10.1007/s11845-018-1744-y. Doi: 10.1007/s11845-018-1744-y. [DOI] [PubMed] [Google Scholar]
- 34.Smith GN, Pudwell J, Walker M, Wen SW. Risk estimation of metabolic syndrome at one and three years after a pregnancy complicated by preeclampsia. J Obstet Gynaecol Can. 2012;34:836–841. doi: 10.1016/S1701-2163(16)35382-8. [DOI] [PubMed] [Google Scholar]
- 35.Teodoro JS, Gomes AP, Varela AT, Duarte FV, Rolo AP, Palmeira CM. Uncovering the beginning of diabetes: The cellular redox status and oxidative stress as starting players in hyperglycemic damage. Mol Cell Biochem. 2013;376:103–110. doi: 10.1007/s11010-012-1555-9. [DOI] [PubMed] [Google Scholar]
- 36.Warrington JP, Gceorge EM, Palei AC, Spradley FT, Granger JP. Recent advances in the understanding if the pathophysiology of preeclampsia. Hypertension. 2013;62:666–673. doi: 10.1161/HYPERTENSIONAHA.113.00588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Coustan DR. Diagnosis of gestational diabetes. Scan J Clin Lab Invest Suppl. 2014;244:27–33. doi: 10.3109/00365513.2014.936677. [DOI] [PubMed] [Google Scholar]
- 38.Popova P, Tkachuk A, Dronova A, Gerasimov A, Kravchuk E, Bolshakova M, Rozdtestvenskaya O, Demidova K, Nikolaeva A, Grineva E. Fasting glycemia at the first prenatal visit and pregnancy outcomes in Russian women. Minerva Endocrinol. 2016;41:477–485. [PubMed] [Google Scholar]
- 39.Barrett HL, Nitert Dekker M, Mclntyre HD, Callaway LK. Normalizing metabolism in diabetic pregnancy: Is it time to target lipids? Diabetes Care. 2014;37:1484–1493. doi: 10.2337/dc13-1934. [DOI] [PubMed] [Google Scholar]
- 40.Kingwell BA, Chapman MJ. Future of high-density lipoprotein infusion therapies: Potential for clinical management of vascular disease. Circulation. 2013;128:1112–1121. doi: 10.1161/CIRCULATIONAHA.113.002683. [DOI] [PubMed] [Google Scholar]
- 41.Song GJ, Kim SM, Park KH, Kim J, Choi I, Cho KH. SR-BI mediates high density lipoprotein (HDL)-induced anti-inflammatory effect in macrophages. Biochem Biophys Res Commun. 2015;457:112–118. doi: 10.1016/j.bbrc.2014.12.028. [DOI] [PubMed] [Google Scholar]
- 42.Demirci O, Tuğrul AS, Dolgun N, Sözen H, Eren S. Serum lipids level assessed in early pregnancy and risk of pre-eclampsia. J Obstet Gynaecol Res. 2011;37:1427–1432. doi: 10.1111/j.1447-0756.2011.01562.x. [DOI] [PubMed] [Google Scholar]
- 43.Matsumoto S, Gotoh N, Hishinuma S, Abe Y, Shimizu Y, Katano Y, Ishihata A. The role of hypertriglyceridemia in the development of atherosclerosis and endothelial dysfunction. Nutrients. 2014;6:1236–1250. doi: 10.3390/nu6031236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Flood-Nichols SK, Stallings JD, Gotkin JL, Tinnemore D, Napolitano PG, Ippolito DL. Elevated ratio of maternal plasma ApoCIII to ApoCII in preeclampsia. Reprod Sci. 2011;18:493–502. doi: 10.1177/1933719110390390. [DOI] [PubMed] [Google Scholar]
- 45.Punthumapol C, Kittichotpanich B. Comparative study of serum lipid concentrations in preeclampsia and normal pregnancy. J Med Assoc Thai. 2008;91:957–961. [PubMed] [Google Scholar]
- 46.Kabiru W, Raynor B. Obstetric outcomes associated with increase in BMI category during pregnancy. Am J Obstet Gynecol. 2004;191:928–932. doi: 10.1016/j.ajog.2004.06.051. [DOI] [PubMed] [Google Scholar]
- 47.Gallos I, Sivakumar K, Kilby M, Coomarasamy A, Thangaratinam S, Vatish M. Pre-eclampsia is associated with, and preceded by, hypertriglyceridaemia: A meta-analysis. BJOG. 2013;20:1321–1332. doi: 10.1111/1471-0528.12375. [DOI] [PubMed] [Google Scholar]
- 48.Barrdel E, Larousserie F, Charlot-Rabiega P, Coulomb-L'Herminé A, Devergne O. Human CD4+ CD25+ FoxP3+ regulatory T cells do not constitutively express IL-35. J Immunol. 2008;181:6898–6905. doi: 10.4049/jimmunol.181.10.6898. [DOI] [PubMed] [Google Scholar]
- 49.Rasanen J, Girsen A, Lu X, Lapidus JA, Standley M, Reddy A, Dasari S, Thomas A, Jacob T, Pouta A, et al. Comprehensive maternal serum proteomic profiles of preclinical and clinical preeclampsia. J Proteome Res. 2010;9:4274–4281. doi: 10.1021/pr100198m. [DOI] [PubMed] [Google Scholar]
- 50.Ozkan ZS, Simsek M, Ilhan F, Deveci D, Godekmerdan A, Sapmaz E. Plasma IL-17, IL-35, Interferon-γ, Socs3 and TGF-β levels in pregnant women with preeclampsia, and their relation with severity of disease. J Matern Fetal Neonatal Med. 2014;27:1513–1517. doi: 10.3109/14767058.2013.861415. [DOI] [PubMed] [Google Scholar]
- 51.Kassan M, Wecker A, Kadowitz P, Trebak M, Matrogui K. CD4+CD25+FoxP3 regulatory T cells and vascular dysfunction in hypertension. J Hypertens. 2013;31:1939–1943. doi: 10.1097/HJH.0b013e328362feb7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Sasaki S, Darmochwal-Kolarz D, Suzuki D, Sakai M, Ito M, Shima T, Shiozaki A, Rolinski J, Saito S. Proportion of peripheral blood and decidual CD4(+) CD25(bright) regulatory T cells in pre-eclampsia. Clin Exp Immunol. 2007;149:139–145. doi: 10.1111/j.1365-2249.2007.03397.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Darmochwal-Kolarz D, Kludka-Sternik M, Tabarkiewicz J, Kolarz B, Rolinski J, Leszczynska-Gorzelak B, Oleszczuk J. The predominance of Th17 lymphocytes and decreased number and function of Treg cells in preeclampsia. J Reprod Immunol. 2012;93:75–81. doi: 10.1016/j.jri.2012.01.006. [DOI] [PubMed] [Google Scholar]
- 54.Cao W, Xu W, Chen T, Wang X, Wang X, Qiu J, Chen N, Mao Y. CD4+CD25+FoxP3+ regulatory T cells and cytokines interact with estradiol in case missed abortion. Exp Ther Med. 2014;7:417–422. doi: 10.3892/etm.2013.1422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Glebezdina NS, Olina AA, Nekrasova IV, Kuklina EM. Role of endogenous melatonin in the regulation of Th17/Treg balance during pregnancy. Bull Exp Biol Med. 2018;164:462–465. doi: 10.1007/s10517-018-4013-1. [DOI] [PubMed] [Google Scholar]
- 56.Figueiredo AS, Schummacher A. The T helper type 17/regulatory T cells paradigm in pregnancy. Immunology. 2016;148:13–21. doi: 10.1111/imm.12595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Onuegbu AJ, Olisekodiaka JM, Udo JU, Umeononihu O, Amah UK, Okwara JE, Atuegbu C. Evaluation of high-sensitivity C-reactive protwin and serum lipid profile in southeastern nigerlan women with pre-ealampsia. Med Princ Pract. 2015;24:276–279. doi: 10.1159/000381778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Khan NA. Role of T-cells in diabetic pregnancy and macrosomia. Indian J Biochem Biophys. 2007;44:344–349. [PubMed] [Google Scholar]
- 59.Di Mario U, Dotta F, Gargiulo P, Sutherland J, Andreani D, Guy K, Pachi A, Fallucca F. Immunology in diabetes pregnancy: Activated Tcells in diabetic mother and neonates. Diabetologia. 1987;30:66–71. doi: 10.1007/BF00274573. [DOI] [PubMed] [Google Scholar]
- 60.Lima VJ, Andrade CR, Ruschi GE, Sass N. Serum lipid levels in pregnancies complicated by preeclampsia. Sao Paulo Med J. 2011;129:73–76. doi: 10.1590/S1516-31802011000200004. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.