

Abstract
Purpose
The aims of the present study were to quantitatively assess graft height changes after sinus lift procedures and to analyze the factors that influenced graft height changes, including the residual bone height before surgery, surgical approach, and tooth type.
Methods
A total of 39 maxillary posterior implants placed during a simultaneous sinus lift procedure were evaluated. Panoramic radiographs of all patients were taken immediately after implant installation and at 3 months, 6 months, 1 year, 2 years, and 3 years. To analyze graft height changes over time, we measured the distance between the implant platform and the base of the grafted sinus floor at 3 locations. The radiographs were analyzed by a single examiner.
Results
Graft height tended to decrease over time, and a statistically significant difference was observed at 2 years compared to baseline (P<0.05). There was no statistically significant difference in graft height change according to the surgical approach or tooth type. For residual bone height, a statistically significant difference in graft height change was found between those with 4–7 mm of residual bone height and those with ≥7 mm (P<0.05).
Conclusions
Graft height after sinus lift procedures significantly decreased at 2 years compared to baseline after sinus augmentation. Further studies should be done with controlled variables, and prospective studies with 3-dimensional images are needed to clarify the factors that influence graft height changes.
Keywords: Alveolar bone grafting, Dental implants, Sinus floor augmentation
Graphical Abstract
INTRODUCTION
The structures beneath the maxillary sinus consist of the alveolar ridge and the maxillary posterior teeth [1]. Lack of sufficient alveolar bone height has long been a common deterrent to implant placement in the posterior maxilla. The lack of height may be the result of alveolar bone loss following tooth loss, periodontal disease, pneumatization of the maxillary sinus, or a combination of the above [1,2]. Grafting the floor of the maxillary sinus is a means of correcting this deficiency.
Currently, 2 main augmentation procedures are used: the transcrestal and lateral window approaches [2,3,4,5]. Indications for the transcrestal approach include a moderately resorbed ridge, a relatively flat sinus floor, and a single implant. In contrast, the lateral window approach is commonly reserved for severely resorbed ridges and multiple implants [6].
Stability of the graft material in the sinus and changes in the height of the graft material over time have been important issues. Wanschitz et al. [7] found a resorption rate of graft material of 10%–13.9% after bone grafting in the sinus. It was reported that progressive sinus pneumatization occurred after augmentation with a 2:1 autogenous bone/xenograft mixture, and the long-term stability of sinus graft height represents an important factor for implant success [8].
Anteriorly, the sinus generally extends to the canine and premolar region. Sharper angles and less width have often been observed in the premolar region, and septa have been more commonly found in the premolar region than in the molar region [9]. The Schneiderian membrane, which lines the maxillary sinus, is adherent to the underlying bone and is at risk of being perforated during sinus augmentation procedures [2,10]. If it is too small or too large, the mediolateral dimension of the maxillary sinus can present difficulties for sinus lifting procedures and can have negative effects on maintenance of the graft material in the maxillary sinus [11]. Therefore, it can be assumed that the position of implant installation might affect the difficulty of the sinus lift procedure, thereby influencing the stability of the graft materials [12].
Few studies have evaluated the maintenance of sinus graft height according to the surgical method and tooth type. The aims of the present study were to assess the amount of graft height change after sinus lift procedures and to analyze the factors influencing graft height changes, including the residual bone height before surgery, surgical approach, and tooth type.
MATERIALS AND METHODS
Patient selection
All the study participants provided informed consent, and this retrospective study was approved by the Institutional Review Board committee at Wonkwang University Daejeon Dental Hospital in 2016 (W1611/001-001). The study population comprised patients who had been treated with first-stage implant surgery with a simultaneous sinus elevation procedure on the maxillary posterior area of the edentulous region at the Department of Periodontology between 2009 and 2012.
The selected patients were examined to determine whether there were any signs or symptoms of oral disease before conducting sinus elevation. Patients who had absolute contraindications for implant surgery, such as uncontrolled diabetes, cardiovascular disease, and hematologic disorder were excluded.
The current study only included patients who had panoramic radiographs taken immediately after implant installation and at 3 months, 6 months, 1 year, 2 years, and 3 years after implant installation. Therefore, only 39 implants in 27 patients met the inclusion criteria. The patients ranged in age from 41 to 67 years (average, 54.5 years). All patients were non-smokers.
Surgical procedure
The sinus lift procedure was performed at the same time as implant placement. One periodontal surgeon performed all surgical procedures. The sinus was filled with deproteinized bovine bone mineral (OCS-B®, Nibec, Seoul, Korea).
The transcrestal approach (20 implants) was performed using the bone-added osteotome sinus floor elevation technique, which adds bone graft material to the site of the osteotome procedure, as described by Summers [5]. The lateral window approach (19 implants) was performed as described by Kent and Block [13]. In brief, the posterior part of the maxilla was exposed via a crestal incision and elevation of a mucoperiosteal flap. Implant sites were marked using surgical stain, and osteotomy was performed at the lateral aspect of the sinus wall. The sinus mucosa was carefully lifted and the bone graft materials were grafted into the sinus. The mucoperiosteal flap was repositioned and sutured.
Radiographic measurements of graft height changes
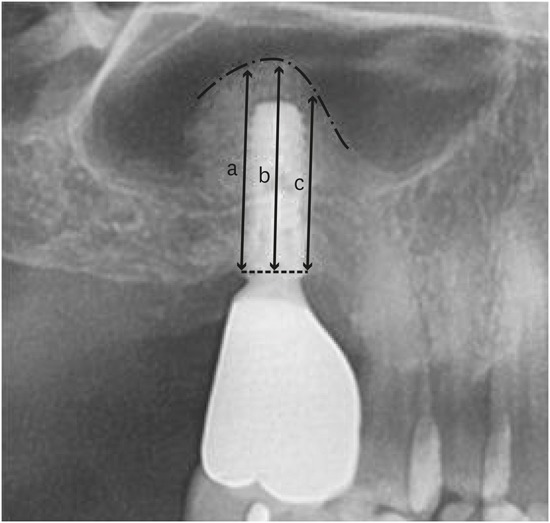
We measured the implant length, residual bone height, and the distance between the implant platform and the base of the grafted sinus floor at 3 sides (the mesial, middle, and distal sides of the implant platform) to evaluate changes in graft height using INFINITT® (Infinitt Healthcare, Seoul, Korea) software to the nearest 1/100 mm. These distances were abbreviated as MeGH, MiGH, and DiGH, respectively (Figure 1). All measurements were made by 1 examiner, and the intra-examiner agreement was calculated to be 0.92 by the kappa test.
Figure 1. Radiographic measurements of graft height change using a panoramic radiograph. Lower dotted line and upper dotted line mean implant platform and grafted sinus floor, respectively.

a: The distance from the implant platform to the base of grafted sinus floor at the mesial side of the implant, b: The distance from the implant platform to the base of the grafted sinus floor at the middle side of the implant, c: The distance from the implant platform to the base of the grafted sinus floor at the distal side of the implant.
To correct for distortion of the obtained panoramic radiographs, we measured the distance from the implant platform to the apex (implant length) on each image and revised the values using the actual length of the implant. The mean values of the graft height at the mesial, middle, and distal sides of the implants were calculated and compared according to several factors, including the residual bone height before surgery, surgical approach, and tooth type. The current study did not consider other variables, such as the type of prosthesis, implant surface modifications, and the diameter and length of the implants.
Statistical analysis
One-way analysis of variance (ANOVA) was used to assess the decrease in graft height over time compared to baseline in each group. Differences in graft height changes between the groups according to the influencing variables at each observation point (or period) were evaluated using ANOVA for repeated measures. The Bonferroni test for post hoc analysis was utilized. Statistically significant differences were considered to be present at P<0.05. All statistical measurements were performed using SPSS version 17 (SPSS Inc., Chicago, IL, USA).
RESULTS
Analysis of graft height changes over time
Graft height significantly decreased over time. A statistically significant difference compared to baseline was observed at 2 years after surgery for MeGH, at 6 months for MiGH, and at 1 year for DiGH. At 2 years after surgery, the graft height changes at all sides showed statistically significant differences compared to baseline (P<0.05, Table 1).
Table 1. Change in graft height over time.
| Period | MeGH (n=39) | MiGH (n=39) | DiGH (n=39) | Mean GH (n=39) |
|---|---|---|---|---|
| Baseline | 16.25±3.20 | 16.96±3.39 | 16.27±2.98 | 16.49±3.03 |
| 3 mon | 15.94±3.76 | 16.31±3.91 | 15.66±3.56 | 15.97±3.59 |
| 6 mon | 15.38±3.56 | 15.50±4.02a) | 15.20±3.89 | 15.36±3.69a) |
| 1 yr | 14.97±3.44 | 15.47±3.22a) | 14.96±3.53a) | 15.13±3.31a) |
| 2 yr | 14.31±3.16a) | 14.83±2.88a) | 14.41±3.34a) | 14.52±3.02a) |
| 3 yr | 13.99±3.23a) | 14.61±2.68a) | 14.17±3.32a) | 14.26±2.92a) |
| 3 yr to baseline | −2.26±3.29a) | −2.35±2.90a) | −2.10±2.24a) | −2.24±2.41a) |
Values are presented as mean±standard deviation (mm).
MeGH: distance from the implant platform to the base of the grafted sinus floor at the mesial side of the implant, MiGH: distance from the implant platform to the base of the grafted sinus floor at the middle side of the implant, DiGH: distance from the implant platform to the base of the grafted sinus floor at the distal side of the implant, ANOVA: analysis of variance.
a)Statistically significant decrease in height compared to baseline (P<0.05) by 1-way ANOVA.
A mean graft height change of −2.24±2.41 mm was measured at 3 years after sinus augmentation. The mean graft height change was larger between 3 and 6 months (−0.62±1.50 mm) than in other subsequent observation periods. However, that difference was not statistically significant (P>0.05, Table 2).
Table 2. Comparison of graft height changes between successive observation periods.
| Period | MeGH (n=39) | MiGH (n=39) | DiGH (n=39) | Mean GH (n=39) |
|---|---|---|---|---|
| Baseline to 3 mon | −0.31±1.62 | −0.65±2.17 | −0.61±2.24 | −0.52±1.71 |
| 3 mon to 6 mon | −0.57±1.85 | −0.81±2.10 | −0.46±1.76 | −0.62±1.50 |
| 6 mon to 1 yr | −0.41±1.35 | −0.03±1.73 | −0.24±1.24 | −0.23±1.18 |
| 1 yr to 2 yr | −0.66±1.79 | −0.64±1.46 | −0.55±1.33 | −0.61±1.40 |
| 2 yr to 3 yr | −0.32±1.27 | −0.22±1.09 | −0.25±0.94 | −0.21±1.06 |
Values are presented as mean±standard deviation (mm). No statistically significant difference in graft height change was detected between any successive observation periods (P>0.05).
MeGH: distance from the implant platform to the base of the grafted sinus floor at the mesial side of the implant, MiGH: distance from the implant platform to the base of the grafted sinus floor at the middle side of the implant, DiGH: distance from the implant platform to the base of the grafted sinus floor at the distal side of the implant.
Graft height changes according to residual bone height
The mean graft height change was −2.39±3.21 mm in the patients with residual bone height of <4 mm, −2.85±1.93 mm in the patients with residual bone height of ≥4 but <7 mm, and −0.67±0.46 mm in the patients with residual bone height of >7 mm. At 1 year after surgery, these changes were statistically significant compared to baseline (P<0.05). The ≥7 mm group showed significantly less graft height change than the group with residual bone height of ≥4 but <7 mm (P<0.05, Table 3).
Table 3. Comparison of mean graft height changes according to residual bone height.
| Group | 3 mon | 6 mon | 1 yr | 2 yr | 3 yr |
|---|---|---|---|---|---|
| <4 mm (n=14) | −0.36±4.64 | −0.83±4.49 | −1.29±4.26a) | −2.25±3.67a) | −2.39±3.21a) |
| ≥4 and <7 mm (n=17) | −0.76±3.00 | −1.54±3.21 | −1.71±2.83a) | −2.20±2.89a) | −2.85±1.93a,b) |
| ≥7 mm (n=8) | −0.31±2.03 | −0.82±2.76 | −0.74±2.03a) | −1.00±1.79a) | −0.67±0.40a,b) |
| P value | 0.300 | 0.220 | 0.150 | 0.070 | 0.015 |
Values are presented as mean±standard deviation (mm).
ANOVA: analysis of variance.
a)Statistically significant decrease in height compared to baseline (P<0.05) by 1-way ANOVA; b)Statistically significant difference between 2 groups (P<0.05) by ANOVA for repeated measures.
Graft height changes according to surgical approach
The mean graft height change after 3 years was −1.86±2.22 mm in the crestal approach group and −2.54±2.43 mm in the lateral window approach group. The lateral window approach group showed a greater graft height change than the crestal approach group, but no statistically significant difference was observed between the 2 surgical approaches. At 1 year after surgery, the graft height changes showed statistically significant differences compared to baseline (P<0.05, Table 4).
Table 4. Comparison of mean graft height changes according to surgical approach methods.
| Group | 3 mon | 6 mon | 1 yr | 2 yr | 3 yr |
|---|---|---|---|---|---|
| Crestal approach (n=20) | −0.54±2.23 | −1.51±2.48 | −1.54±2.23a) | −1.84±1.99a) | −1.86±2.22a) |
| Lateral window approach (n=19) | −0.50±4.49 | −0.74±4.32 | −1.24±3.96a) | −2.11±3.71a) | −2.54±2.43a) |
Values are presented as mean±standard deviation (mm).
ANOVA: analysis of variance.
a)Statistically significant decrease in height compared to baseline (P<0.05) by 1-way ANOVA; No statistically significant difference in graft height change was detected between the 2 surgical approach groups (P>0.05) by ANOVA for repeated measures.
Graft height changes according to tooth type
The mean graft height changes after 3 years were −3.64±3.18 mm in the first premolar, −1.72±1.20 mm in the second premolar, −2.37±2.93 mm in the first molar, and −1.93±1.78 mm in the second molar. The first premolar showed the greatest amount of graft height change, but no statistically significant differences in height change were found according to the tooth type (P>0.05, Table 5).
Table 5. Comparison of mean graft height change according to tooth type.
| Group | 3 mon | 6 mon | 1 yr | 2 yr | 3 yr |
|---|---|---|---|---|---|
| First premolar (n=3) | −1.52±2.84 | −3.45±2.30a) | −2.67±2.30a) | −3.27±1.03a) | −3.64±3.18a) |
| Second premolar (n=10) | 0.14±3.32 | −0.37±3.45a) | −0.56±2.87a) | −0.89±3.25a) | −1.72±1.20a) |
| First molar (n=20) | −0.47±3.93 | −1.12±3.97a) | −1.50±3.68a) | −2.37±2.93a) | −2.37±2.93a) |
| Second molar (n=6) | −1.27±3.09 | −1.29±2.18a) | −1.55±2.59a) | −2.06±2.11a) | −1.93±1.78a) |
Values are presented as mean±standard deviation (mm).
ANOVA: analysis of variance.
a)Statistically significant decrease in height compared to baseline (P<0.05) by 1-way ANOVA; No statistically significant difference in graft height change was detected among different tooth types (P>0.05) by ANOVA for repeated measures.
DISCUSSION
It is difficult to gain a sufficiently large amount of bone for implant placement when alveolar bone loss occurs after the extraction of maxillary posterior teeth and severe pneumatization. In situations where the alveolar bone has poor quality and short height, a sinus lift procedure should be the first option for treatment [14]. Although researchers have tried to compare different alloplastic and allograft materials, debate continues as to the best graft material and the proper criteria for ideal indications. Recently, it has been suggested that deproteinized bovine bone and tricalcium phosphate appear to be as effective as autogenous bone for augmentation of the maxillary sinus [15,16]. From a biological viewpoint, slow resorption and degradation of a biomaterial is attractive. We used deproteinized bovine bone mineral for sinus lift procedures on the basis of those recent studies and then analyzed graft height changes during 3 years after surgery. The mean graft height change was −2.24±2.41 mm at 3 years after surgery, and these changes became significant compared to baseline at 2 years after surgery.
Pneumatization may be caused by positive intrasinus air pressure due to respiration [17], and this pressure might promote resorption and pneumatization after sinus augmentation [18]. Pressure-induced degradation and resorption in the grafted sinus floor may lead to loss of vertical bone height. Listrom and Symington [19] reported that there were no changes in length and width from 3 months to 10 years after sinus floor grafting, but there was a significant decrease in height of approximately 10%–15% between 3 months and 2 years and 3 months and 10 years. In the present study, there was a significant decrease in height of approximately 13.52% during 3 years after surgery. Hatano et al. [8] reported that the overall height of the bone graft decreased during the first 2–3 years after augmentation and that only minor changes occurred thereafter, but the graft height remained higher than that observed before sinus augmentation for up to 96 months after augmentation. A long-term study investigating graft height changes after sinus augmentation seems to be necessary.
Although this trend was not statistically significant, a greater mean change was observed in the period before 6 months than between 6 and 12 months after surgery. We delivered the implant prosthesis at least 6 months after the simultaneous sinus augmentation and implant insertion procedure. We thus interpret these findings as supporting the proposal that implant loading may exert a stabilizing effect on the maintenance of bone graft height, consistent with the findings of Listrom and Symington [19].
It was reported that the amount of native bone did not have a significant effect on the change in mean graft height over 3 years, although the least amount of graft height loss was found in patients with the greatest amount of preoperative residual bone height [20]. In our study, there was a significant difference between the patients with residual bone height of ≥4 but <7 mm and the patients with residual bone height of ≥7 mm in terms of the graft height change after 3 years, but there was no proportional relationship of graft height change according to residual bone height. The least amount of height change at 3 years after augmentation was 0.67 mm in the patients with residual bone height of ≥7 mm. The stability of the graft height in those patients might have resulted from the technical simplicity of augmentation and the use of a relatively small amount of graft material.
Cho and Kim [21] reported that sinus graft height decreased significantly in the first 12 months after both the lateral window approach and crestal approach, consistent with our findings. Moreover, patients in whom the grafted sinus floor was above the implant apex showed a decrease over time, and this tendency was stronger in patients who underwent a procedure using the crestal approach than in those in whom the lateral window approach was used. However, there was no significant difference between the 2 surgical approaches in our study.
We analyzed graft height changes according to tooth type. We found that the first premolar sites showed the greatest changes of graft height, but the difference was not statistically significant. Sharper angles and less width have often been observed at premolar sites, so we assumed that the challenging sinus anatomy around the first premolar might have had a negative effect on the sinus lift procedures [11,12]. The limitations of this study in this regard include the considerably smaller sample size of the first premolar group (n=3). Obtaining fewer samples for the first premolar group was inevitable because molars are more commonly lost due to periodontitis and caries than premolars [22]. In addition, the preoperative residual bone height at the first premolar site is usually adequate to insert an implant fixture without the need for a sinus lift procedure.
It was difficult to assess the position of the maxillary sinus floor accurately on 2-dimensional panoramic radiographs due to poor visualization [23]. Therefore, we could not directly measure the length of the augmented sinus membrane, but instead indirectly measured graft height changes. To correct for the distortion of obtained panoramic radiographs, we revised the values using the actual length of the implants. This was done because we only included patients who had received first-stage implant surgery with a simultaneous sinus elevation procedure in this study. Computed tomography (CT) scans can be used to calculate the volume, not just the height, of graft materials in the sinus; however, multiple CT scans are not always justifiable and patient cooperation may be limited.
In conclusion, graft height after sinus lift procedures decreased over time, and the decrease was statistically significant starting at 2 years. There was no statistically significant difference in graft height change according to the surgical approach or tooth type. For residual bone height, significantly greater height change was detected in patients with residual bone height of ≥4 and <7 mm than in those with residual bone height of ≥7 mm (P<0.05).
Further studies are underway to determine whether the above trends are also found for other graft materials and other barrier membranes. Since the present study was conducted retrospectively without consideration of the type of graft material, implant surface modifications, diameter and length of the implants, or sinus anatomy, further studies with controlled variables should be done. More precisely designed prospective studies with 3-dimensional images will be also needed.
Footnotes
Funding: This study was supported by Wonkwang University in 2017.
Author Contributions: Conceptualization: Min-Jeong Ko, Seong-Nyum Jeong; Investigation: Do-Hyung Kim, Min-Jeong Ko, Seong-Nyum Jeong; Methodology: Do-Hyung Kim, Min-Jeong Ko, Jae-Hong Lee; Project administration: Seong-Nyum Jeong; Writing - original draft: Min-Jeong Ko, Seong-Nyum Jeong; Writing - review & editing: Do-Hyung Kim, Jae-Hong Lee, Seong-Nyum Jeong.
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
References
- 1.Davarpanah M, Martinez H, Tecucianu JF, Hage G, Lazzara R. The modified osteotome technique. Int J Periodontics Restorative Dent. 2001;21:599–607. [PubMed] [Google Scholar]
- 2.Tatum H., Jr Maxillary and sinus implant reconstructions. Dent Clin North Am. 1986;30:207–229. [PubMed] [Google Scholar]
- 3.Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marrow and bone. J Oral Surg. 1980;38:613–616. [PubMed] [Google Scholar]
- 4.Summers RB. A new concept in maxillary implant surgery: the osteotome technique. Compendium. 1994;15:152–156. [PubMed] [Google Scholar]
- 5.Summers RB. The osteotome technique: Part 3--Less invasive methods of elevating the sinus floor. Compendium. 1994;15:698–710. [PubMed] [Google Scholar]
- 6.Wang HL, Katranji A. ABC sinus augmentation classification. Int J Periodontics Restorative Dent. 2008;28:383–389. [PubMed] [Google Scholar]
- 7.Wanschitz F, Figl M, Wagner A, Rolf E. Measurement of volume changes after sinus floor augmentation with a phycogenic hydroxyapatite. Int J Oral Maxillofac Implants. 2006;21:433–438. [PubMed] [Google Scholar]
- 8.Hatano N, Shimizu Y, Ooya K. A clinical long-term radiographic evaluation of graft height changes after maxillary sinus floor augmentation with a 2:1 autogenous bone/xenograft mixture and simultaneous placement of dental implants. Clin Oral Implants Res. 2004;15:339–345. doi: 10.1111/j.1600-0501.2004.00996.x. [DOI] [PubMed] [Google Scholar]
- 9.van den Bergh JP, ten Bruggenkate CM, Disch FJ, Tuinzing DB. Anatomical aspects of sinus floor elevations. Clin Oral Implants Res. 2000;11:256–265. doi: 10.1034/j.1600-0501.2000.011003256.x. [DOI] [PubMed] [Google Scholar]
- 10.Velloso GR, Vidigal GM, Jr, de Freitas MM, Garcia de Brito OF, Manso MC, Groisman M. Tridimensional analysis of maxillary sinus anatomy related to sinus lift procedure. Implant Dent. 2006;15:192–196. doi: 10.1097/01.id.0000223233.29454.77. [DOI] [PubMed] [Google Scholar]
- 11.Chan HL, Suarez F, Monje A, Benavides E, Wang HL. Evaluation of maxillary sinus width on cone-beam computed tomography for sinus augmentation and new sinus classification based on sinus width. Clin Oral Implants Res. 2014;25:647–652. doi: 10.1111/clr.12055. [DOI] [PubMed] [Google Scholar]
- 12.Wen SC, Chan HL, Wang HL. Classification and management of antral septa for maxillary sinus augmentation. Int J Periodontics Restorative Dent. 2013;33:509–517. doi: 10.11607/prd.1609. [DOI] [PubMed] [Google Scholar]
- 13.Kent JN, Block MS. Simultaneous maxillary sinus floor bone grafting and placement of hydroxylapatite-coated implants. J Oral Maxillofac Surg. 1989;47:238–242. doi: 10.1016/0278-2391(89)90225-5. [DOI] [PubMed] [Google Scholar]
- 14.Hieu PD, Chung JH, Yim SB, Hong KS. A radiographical study on the changes in height of grafting materials after sinus lift: a comparison between two types of xenogenic materials. J Periodontal Implant Sci. 2010;40:25–32. doi: 10.5051/jpis.2010.40.1.25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Alayan J, Ivanovski S. A prospective controlled trial comparing xenograft/autogenous bone and collagen-stabilized xenograft for maxillary sinus augmentation-complications, patient-reported outcomes and volumetric analysis. Clin Oral Implants Res. 2018;29:248–262. doi: 10.1111/clr.13107. [DOI] [PubMed] [Google Scholar]
- 16.Pereira RS, Gorla LF, Boos FB, Okamoto R, Garcia Júnior IR, Hochuli-Vieira E. Use of autogenous bone and beta-tricalcium phosphate in maxillary sinus lifting: histomorphometric study and immunohistochemical assessment of RUNX2 and VEGF. Int J Oral Maxillofac Surg. 2017;46:503–510. doi: 10.1016/j.ijom.2017.01.002. [DOI] [PubMed] [Google Scholar]
- 17.Chanavaz M. Maxillary sinus: anatomy, physiology, surgery, and bone grafting related to implantology--eleven years of surgical experience (1979–1990) J Oral Implantol. 1990;16:199–209. [PubMed] [Google Scholar]
- 18.Hürzeler MB, Kirsch A, Ackermann KL, Quiñones CR. Reconstruction of the severely resorbed maxilla with dental implants in the augmented maxillary sinus: a 5-year clinical investigation. Int J Oral Maxillofac Implants. 1996;11:466–475. [PubMed] [Google Scholar]
- 19.Listrom RD, Symington JM. Osseointegrated dental implants in conjunction with bone grafts. Int J Oral Maxillofac Surg. 1988;17:116–118. doi: 10.1016/s0901-5027(88)80163-2. [DOI] [PubMed] [Google Scholar]
- 20.Geurs NC, Wang IC, Shulman LB, Jeffcoat MK. Retrospective radiographic analysis of sinus graft and implant placement procedures from the Academy of Osseointegration Consensus Conference on Sinus Grafts. Int J Periodontics Restorative Dent. 2001;21:517–523. [PubMed] [Google Scholar]
- 21.Cho SH, Kim OS. Radiographic change of grafted sinus floor after maxillary sinus floor elevation and placement of dental implant. J Korean Acad Periodontol. 2006;36:345–359. [Google Scholar]
- 22.McCaul LK, Jenkins WM, Kay EJ. The reasons for the extraction of various tooth types in Scotland: a 15-year follow up. J Dent. 2001;29:401–407. doi: 10.1016/s0300-5712(01)00036-7. [DOI] [PubMed] [Google Scholar]
- 23.Fredholm U, Bolin A, Andersson L. Preimplant radiographic assessment of available maxillary bone support. Comparison of tomographic and panoramic technique. Swed Dent J. 1993;17:103–109. [PubMed] [Google Scholar]