

Summary
In July 2005, four suicide bombers detonated explosive improvised high explosive devices (IEDs) in three separate underground carriages and a double decker bus in London, resulting in 56 deaths and 775 injured. This study aims to understand the mechanisms and patterns of burn injuries from high explosives, and the related factors that determine mortality. The types and patterns of burn injuries in survivors and fatalities in the confined underground train carriages and the bus were analysed, evaluating injury severity score and the victims’ relative position from the detonation point. The data were sourced from collated police witness statements, hospital records, forensic post mortem examinations and forensic examinations at the scene. The detonation of an explosive device in a confined space causes complex injuries to the human body, resulting in blast-related direct thermal and radiant burns. Injury patterns and mortality were related to crowd density, enclosure design, position of the victims and proximity to the device. Suicide bombings using IEDs will result in direct thermal burns and radiant burns currently categorised in the quaternary (miscellaneous) blast injury group. We propose a classification of these burns following an analysis of the London bombing data with respect to burns in both the fatalities and survivors. Distance from the device, crowd density and environment influences these burns.
Keywords: 7/7 bombings, London terrorist attack, London bombing, blast injuries, disaster management, suicide bomber
Abstract
En juillet 2005, 4 kamikazes faisaient exploser leur engin artisanal dans 3 rames de métro et 1 autobus à impériale de Londres, faisant 56 morts et 775 blessés. Cette étude a pour but d’étudier les mécanismes et la physiopathologie des brûlures liées à une explosion ainsi que d’évaluer les facteurs associés de mortalité. Nous avons analysé le type et la localisation des brûlures, l’ISS selon la position des victimes par rapport à l’épicentre. Les données provenaient des témoignages recueillis par les forces de police, des dossiers médicaux, des autopsies et des analyses de site. Une explosion en milieu clos entraînent des lésions complexes parmi lesquelles des brûlures thermiques directes et par radiation. La topographie des lésions et la mortalité étaient en relation avec la densité humaine, la topographie du volume clos, la position des victimes et leur situation par rapport à l’épicentre. Les brûlures directes et par radiation sont actuellement catégorisées dans les blasts quaternaires. A la suite des attentats londoniens, nous proposons une classification de ces brûlures, influencées par la distance à l’épicentre, la densité humaine et l’environnement.
Introduction
Suicide bombings significantly challenge emergency response and health care systems. The emergency services, rescue and recovery teams working alongside medical teams play a key role in the immediate aftermath of an explosive blast, and these teams require an understanding of the complexity of blast injuries, how they present and how they are managed from the scene to the trauma centre and beyond.1
On July 7th 2005, four suicide bombers detonated improvised high explosive devices in a coordinated attack on underground trains and a double decker bus in Central London.
There was a total of 56 fatalities, including the 4 suicide bombers, and 775 people injured, 24 of them critically.2 The victims were treated at multiple London hospitals and over half were treated at the Royal London Hospital Trauma Centre in East London. It was the largest mass casualty incident on the UK mainland since the Second World War.
The damage to the human body sustained from explosions is a unique pattern of injuries not seen in other forms of trauma, and is characterised as primary, secondary, tertiary and quaternary3 (Table I). Each explosion, however, is highly variable in terms of scene location, crowd density, explosive characteristics and the surrounding environment. As a result, there is a variation in the morbidity and mortality observed with each incident. 4 Burns occurring in explosions frequently co-exist with non-burn injuries resulting from other consequences of blast injury. All these injury patterns are heterogeneous in their presentation due to a combination of various factors; nature and type of explosive, mode of delivery, distance of the victims from the source, surrounding environment and structure, open or confined space and other hazards and barriers.
Table I. Classification of injuries from an explosion.

Recent major explosions resulting in severe burns have ranged from extreme mass casualty deaths of over 2000 people from conflagration, an extensive fire caused by the explosion following attacks on the world trade centres (9 November 2001), the Bali bombings in which 202 died (12 October 2002), and lesser scale incidents such as the London Soho pub bombings (30 April 1999).5-9
The aim of this work is to perform a detailed analysis of burn injuries in both the survivors and fatalities of the London 7/7 bombings. The findings of this investigation into blast-related burn injuries will be useful for future emergency planning and resource allocation in major explosive incidents, both accidental and terrorism related. Furthermore, this data set also has future application in the validation of computerised human injury prediction tools.6 It is hypothesised that blast-related burns can be classified beyond the quaternary (miscellaneous) type as described by Kluger.10,11
Methodology
A retrospective review of casualty data collected following the London July 7th bombing was performed. The data was initially collected during investigations performed by a multi-agency team including scientists from the UK Defence Science and Technology Laboratory (DSTL), Porton Down, and the Metropolitan Police. The evidence examined consisted of police witness statements, hospital records and forensic data, including scene and post mortem photography, laser scanning and digital imaging. The senior author (HP) was involved in this initial data collection and holds authority and permission to access and publish the data. Casualty demographic data collated including Injury Severity Score, standard blast injury system score classification, specific anatomical based injury profiles, position, orientation and proximity of the survivors to the devices, crowd density, surrounding structures and positioning of other people determined injuries and survivability.
Burn injuries in survivors treated at various London hospitals were analysed according to pattern of injury, and each was given an injury severity score. For the fatalities, data on the burn injury was determined from post mortem reports and also photographic evidence. The distance of the victims from the device was also determined from staged positional analysis.
Results
The extent and nature of burn injuries sustained by the survivors and the fatalities from the London suicide bombings were classified into two groups. Analysis was performed on all the burn data and classified into the two groups using the following parameters: type of burn, source of burn and energy transfer in the blast environment, injury severity score and distance from the blast.
Type of burn
Burn injuries in survivors: radiant burns (flash burns) were prevalent in 21 survivors from the four scenes. These burns mostly affected exposed parts of the body such as face, arms and lower limbs in those wearing shorts and skirts (Figs. 1 and 2). These burns healed within approximately 10 days with minimal surgical intervention. One of the survivors had inhalational injuries and required intubation. Radiant heat was secondary to high thermal energy dissipated by the improvised explosive device. The survivors sustained burns within 2 to 8 metres from the device, with injury severity scores of 1 to 35. The burns covered less than 20% total body surface area and were superficial dermal.
Fig. 1. A clinical photograph of an upper limb with radiant burns.

Fig. 2. A clinical photograph of radiant burns affecting the lower limbs.

Burn injuries in the fatalities: varying degrees of burn distribution including full thickness burns with significant charring, partial thickness burns and flash burns were observed in the fatalities. Signs of inhalation injury included singed nasal hair, eyelashes, anterior hairline and facial burns, as obtained from the post-mortem photographic analysis. The partial thickness burns were largely mid to deep dermal.
The total body surface area distribution of the burns ranged from 0% to 100%; at King’s Cross, 18 victims had over 80% burns, whilst there were only 2 and 0 victims with such distribution at Edgware Road and Aldgate respectively (Fig. 3). It was found that crowd density was an important factor in the pattern of burn injury. In those that had potentially survivable burns, other severe primary blast injuries precluded their survivability. Closer analysis of burn distribution in the fatalities shows that approximately half the victims had non-survivable burns aside from other fatal blast injuries (Table II).
Fig. 3. A bar chart demonstrating prevalence by total burn surface area (TBSA) at different explosion geographic locations.
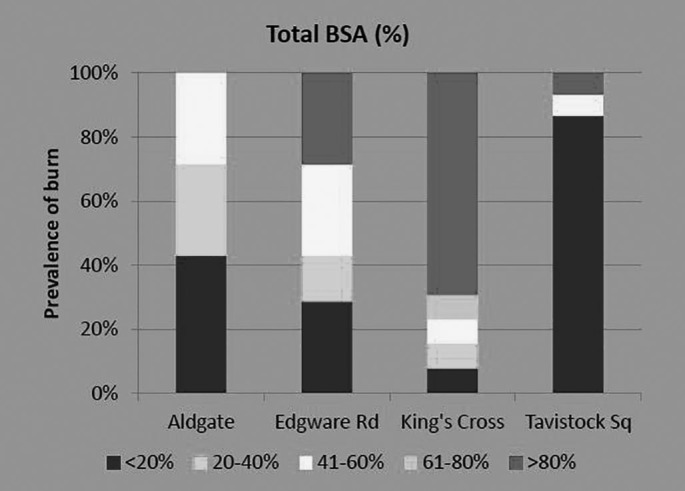
Table II. Survivable and non-survivable burns.

Evaluation of clothing worn by the fatalities
Evaluation of burn injuries in the fatalities and their clothing at all four scenes - Aldgate, Edgware, Kings Cross and Tavistock Square - showed that 50 to 100% of their lower body clothing was torn and dishevelled by the blast wave from the floor-based explosive device. Their upper body clothing was largely intact in 50 to 70% of the fatalities at each scene (Table III).
Table III. A summary of the evaluation of clothing in fatalities at the four scenes.

A closer evaluation of the state of their clothing revealed that in some of the victims with intact clothing, there were deep dermal burns affecting a large percentage of their total body surface area. These clothes showed no evidence of having caught fire. An important inference can therefore be made based on these observations: there was no evidence of conflagration at the blast scene, confirmed also by evidence that surrounding train structures such as seats were not burnt.
Distance from the IED
Burns at the Kings Cross scene occurred within a distance of 1 metre and were affected by crowd density, which was 5 people per square metre at this scene.
At the Aldgate and Edgware Road scenes, burns occurred within 3.6 metres and 3.8 metres (Fig. 4). Crowd density was similar at these scenes, being 2 people per square metre. On the double decker bus at Tavistock Square, the IED was detonated on the upper deck and the fatalities on the upper deck sustained burns at 1.8m. The people on the lower deck sustained crush injuries when the upper deck flooring collapsed onto the lower deck.
Fig. 4. A diagram of thermal injuries relative to blast source distance.

As for the fatalities in the underground, 41 were standing and only two were seated. On the double decker bus, all 13 victims were seated and did not sustain significant burn injuries (Fig. 5).
Fig. 5. A bar chart demonstrating the difference in the position of fatalities between the underground carriage and the bus.

Discussion
Terrorist bombings are a constant threat worldwide and the injuries they cause present unique triage, diagnostic and management challenges. These incidents occur indiscriminately and many factors contribute to the types of injuries seen. The environment of the bombing scene is an important determining factor for mortality and severity of injuries.12 The confined surroundings of the London Underground system and the double decker bus, and their structural components, contributed to the injury patterns. These environmental factors contributed further to the complexity of the blast wave that resulted in unique injury patterns and hence specific mechanisms for the types of injuries seen that had previously only been studied experimentally. 13 Injury mechanisms and their classification are important for understanding survivability and future mitigation against them.
Mass casualty events will by definition overwhelm the emergency medical response system, and the resultant accompanying chaos is not an optimum environment for non-preplanned recording of accurate data. Data capture in any terrorist incident is key to accurate prospective analysis of injuries, triage and injury mechanism. The explosions in the Tavern in the Town and the Mulberry Bush pubs in Birmingham on 21 November 1974 were studied with respect to the position of each person within the two bars at the time of the explosion and hence to the severity of injuries sustained.7 The positional analysis of the victims together with the severity of the injuries sustained were crucial to understanding survivability.8
The 7/7 London bombing retrospective forensic investigation allowed an accurate analysis of events. The positional analysis of victims and their ISS were key to determining triage, injury patterns and mechanisms.9
The blast wave overpressure calculated in the enclosed train carriages in the underground system following an explosion was a complex pressure wave due to the confinement of the blast wave and its multiple reflections off the ceiling, other people, glazing, windows and doors (Fig. 6).14 Its intensity is dependent on the volume of the underground space and the degree of venting through doors and windows, which will vary between a single bore tunnel design and a double cut and cover tunnel.
Fig. 6. A line graph of the resultant complex waveform of blast in an enclosed space due to reflection from solid structure.

Additionally, degradation of the overpressure is inversely related to the cube of distance from detonation, therefore proximity to the device determines the extent of injuries such as traumatic amputations and other blast injuries.15
The majority of severe burns occurred in the enclosed environment as opposed to the relatively semi confined environment of the bus.
Burns and penetrating injuries are features of an explosive event determined by proximity rather than environmental design. The crowd density on the train carriages also had a significant implication on the types of burn injuries sustained. Crowd density on the carriages at Aldgate and Edgware Road was similar (2 people per square metre) and the burns occurred at a greater distance as the blast was able to dissipate further. The crowd density on the carriage at Kings Cross was 5 people per square metre and the bomber had placed himself at a point of maximum concentration. These crowds absorbed the blast and this resulted in increased mortality and greater numbers of fatal burns and traumatic amputations from the floor-based device. These factors explain why four times as many people died at this scene compared to Aldgate and Edgware Road.
The burns seen in both the survivors and fatalities, thermal and radiant burns, can be classified as primary burns which were not a result of conflagration, or secondary burns (Fig. 7).
Fig. 7. The classification of burns from an explosion.

The burns in the survivors were radiant burns and occurred with the explosion. Those areas not covered with clothing, such as face, hands and lower leg, were affected. These burns healed within days. The direct thermal burns, resulting in full thick-ness burns, occurred in the fatalities together with significant inhalation burns and primary blast injuries. The most severe cases were seen at Kings Cross where the fatalities were closely packed around the bomber and the resultant injuries were not survivable.
The initial explosion resulted in momentary exothermic reaction, resulting in very high temperatures that quickly dissipated. The confined space made it difficult for the heat to dissipate, and it was absorbed by the victims within the enclosed space.
There was no conflagration; hence the number of victims that could have had severe burn injury was kept to a minimum.
On the double decker bus, again there was no conflagration despite the presence of an open space with lots of surrounding air. A different mechanism of energy dissipation may be responsible for this, as the blast resulted in the bus roof being separated from the main structure and large energy absorption. The blast however led to the structural collapse of the bus, resulting in other forms of injury to victims such as crush and severe head injuries in the fatalities. At this scene, minimal burn injuries were seen and those who were affected were very close to the device.
Conclusion
The studies carried out in the aftermath of the 7th July 2005 London suicide bombings have contributed towards understanding numerous individual facets of blast injury mechanics, in particular, the classification of burns (classified as quaternary blast injury) into primary or secondary burns. Primary burns can be further divided into thermal or radiant burns.
Thermal injuries are associated with severe burns, in the form of partial or full-thickness burns and a high mortality rate in the context of a blast injury, whilst radiant burns are more likely to be found in survivors as superficial burns. Application of this new understanding can allow emergency service responders and medical teams to more accurately assess survivability of victims with multiple injuries and thus influence prioritisation of immediate treatment, evacuation and hospital care. This study has also enabled the validation and development of the Human Injury Predictor model to assist in the target hardening of the structural design of populated spaces subject to terrorist attack. This in turn has contributed to the strategic and tactical planning for any possible future events.
References
- 1.Aylwin CJ, Konig TC, Brennan NW, Shirley PJ. Reduction in critical mortality in urban mass casualty incidents: analysis of triage, surge, and resource use after the London bombings on July 7, 2005. Lancet. 2006;368(9554):2219–2225. doi: 10.1016/S0140-6736(06)69896-6. [DOI] [PubMed] [Google Scholar]
- 2.Lockey D, MacKenzie R, Redhead J, Wise D. London bombings July 2005: the immediate pre-hospital medical response. Resuscitation. 2005;66(2):ix–xii. doi: 10.1016/j.resuscitation.2005.07.005. [DOI] [PubMed] [Google Scholar]
- 3.Zuckerman S. Discussion on the problem of blast injuries. Proceedings of the Royal Society of Medicine. 1941;34:171–188. doi: 10.1177/003591574103400305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Edwards DS, McMenemy L, Stapley SA, Patel HD. 40 years of terrorist bombings - a meta-analysis of the casualty and injury profile. Injury. 2016;47(3)X:646–652. doi: 10.1016/j.injury.2015.12.021. [DOI] [PubMed] [Google Scholar]
- 5.Ng RL, James SE, Philp B, Floyd D. The Soho nail bomb: the UCH experience. University College Hospital. Ann R Coll Surg Engl. 2001;83(5):297–301. [PMC free article] [PubMed] [Google Scholar]
- 6.Williams KN, Squires S. Experience of a major incident alert at two hospitals: ‘the Soho bomb’. Br J Anaesth. 2000;85(2):322–324. doi: 10.1093/bja/85.2.322. [DOI] [PubMed] [Google Scholar]
- 7.Patel HD, Dryden S. Clinical forensic investigation of the 2005 London suicide bombings. A Bull, J Clasper, P Mahoney (eds): “Blast Injury Science and Engineering. 2016:115–118. [Google Scholar]
- 8.Cooper GJ, Maynard RL, Cross NL, Hill JF. Casualties from terrorist bombings. The Journal of Trauma. 1983;23(11):955–967. doi: 10.1097/00005373-198311000-00001. [DOI] [PubMed] [Google Scholar]
- 9.Greenwood JE. Burn injury and explosions: an Australian perspective. Eplasty. 2009;9:e40. [PMC free article] [PubMed] [Google Scholar]
- 10.Kluger Y, Peleg K, Daniel-Aharonson L, Mayo A. The special injury pattern in terrorist bombings. Journal of the American College of Surgeons. 2004;199(6):875–879. doi: 10.1016/j.jamcollsurg.2004.09.003. [DOI] [PubMed] [Google Scholar]
- 11.Kluger Y, Nimrod A, Biderman P, Mayo A. The quinary pattern of blast injury. American Journal of Disaster Medicine. 2007;2(1):21–25. [PubMed] [Google Scholar]
- 12.Leibovici D, Gofrit ON, Stein M, Shapira SC. Blast injuries: bus versus open-air bombings - a comparative study of injuries in survivors of open-air versus confined-space explosions. J Trauma. 1996;41(6):1030–1035. doi: 10.1097/00005373-199612000-00015. [DOI] [PubMed] [Google Scholar]
- 13.Bowen IG, Fletcher ER, Richmond DR. Estimate of man’s tolerance to the direct effects of air blast. Washington D.C.: Lovelace Foundation for Medical Research and Education, Agency DAS. 1968 [Google Scholar]
- 14.Hepper AE, Pope DJ, Bishop M, Kirkman E. Modelling the blast environment and relating this to clinical injury: experience from the 7/7 inquest. J R Army Med Corps. 2014;160(2):171–174. doi: 10.1136/jramc-2014-000245. [DOI] [PubMed] [Google Scholar]
- 15.Edwards DS, Clasper J. Blast Injury Mechanism. A Bull, J Clasper, P Mahoney (eds): “Blast Injury Science and Engineering. (Springer) 2016:87–104. [Google Scholar]