

Summary
Although electrical burns have a rather low incidence, they are considered one of the most devastating injuries. The aim of this retrospective study was to analyse specific aspects of electrical injuries and to delineate a prevention strategy. A retrospective analysis of medical records of all the patients admitted to our Unit with electrical burns over a 10-year period (2006/01/01–2015/12/31) was undertaken. Demographic data, mechanism of injury and electric current voltage, total burn surface area (TBSA), location and depth of burns, acute complications, surgical interventions and length of hospital stay (LOS) were analysed. Out of 1695 burn patients admitted to our Unit, 99 subjects (5.84%) suffered electrical burns. 97% of these patients were male. The mean age was 38.3±13.7years and mean TBSA was 11.9%±13.2%. The mechanism of injury was occupational in 75 cases. Injuries were classified as low-voltage burns (24.2%), highvoltage burns (30.3%) and flash burns (45.5%). TBSA (p=0.014), mean LOS (p=0.002) and serum creatinine kinase levels (p<0.001) were significantly higher in patients with high-voltage injury in comparison to low-voltage injury, as well as the incidence of escharotomy/ fasciotomy (p=0.049) and flap surgeries (p=0.004). Although there was a higher incidence of amputations in this group (16.7% vs. 12.5%), the difference was not statistically significant (p=0.487). The high prevalence of electrical burns in males and workers emphasizes the need to review occupational safety regulations. Educational efforts regarding potential hazards of electricity and reinforcing compliance with safety measures are essential to avoid these injuri.
Keywords: burn, electrical burn, high-voltage, low-voltage, epidemiology
Abstract
Bien que plutôt rares, les brûlures électriques sont considérées comme les plus délabrants des accidents. Le but de cette étude était d’analyser les aspects spécifiques des brûlures électriques et de définir une stratégie de prévention. Elle a consister en l’analyse des dossiers de tous les patients admis pour brûlure électrique entre le 1er janvier 2006 et les 31 décembre 2015. Les données démographiques, le mécanisme exact de l’accident, le voltage, la surface brûlée (SB), la localisation, la profondeur, les complications initiales, les interventions chirurgicales et la durée moyenne de séjour (DMS) ont été analysées. Quatre vingt dix neuf (5,84%) des 1 695 patients hospitalisés pour brûlure avaient subi un accident électrique, 97% d’entre eux étaient des hommes. Leur âge moyen était de 38,3 +/- 13,7 ans, la surface brûlée de 11,9 +/- 13,2%. Soixante quinze accidents étaient survenus au travail. On recensait 24,2% de brûlures électrothermiques par bas voltage, 30,3% par haut voltage et 45,5% de flashes. La surface brûlés (p=0,014), la DMS (p=0,002), le niveau de CPK sanguine (p<0,001), l’incidence des incisions de décharge et aponévrotomies (p=0,049) et de lambeaux (p=0,004) était plus élevés en cas d’atteinte par haut voltage. Bien que plus élevée chez ces patients (16,7% VS 12,5%), l’incidence des amputation n’était pas statistiquement significative (p=0,487). L’incidence élevée des accidents électriques chez les hommes au travail est une indication à revoir la législation. Des efforts de formation et de contrôle de l’application de la législation sont nécessaires pour éviter ces accidents.
Introduction
Electrical burns are still a major problem in our society. Although their incidence is rather low, they are considered one of the most devastating injuries, due to their high morbidity and mortality.1 Moreover, high costs are usually implied, related to the long term hospitalization usually required, the need for multiple surgical procedures and eventually the functional sequels that might result from the original injury.2 The mechanism of injury is complex, being a result of the combination of diverse thermal and non-thermal processes. An electric current can reach deep tissues, causing deep and extensive injuries. Depending on voltage magnitude, injury may be sustained in nerve, bone and tendon tissue, as well as in skin.3 Electrical injuries are typically divided into high voltage (³1000V), low voltage (<1000V), “flash burn” (without passage of current through the patient) and burns caused by lightning.4,5
The burden of electrical burn injuries is different among developed and developing countries. According to multiple reports, it is more prevalent in developing countries.1,2 Statistics show that prevalence is higher among men, and it most commonly affects the young population and the working classes – the main human resources of countries.2,3,6 Preventive meas-ures, namely education on electric current danger and hazards, as well as safety measures in workplaces are probably the most effective methods to reduce the incidence of electrical injury.
In this retrospective study, we reviewed the medical records of patients admitted to the Burn Unit affiliated to Centro Hospitalar e Universitário de Coimbra (CHUC), the biggest burn centre in Portugal, over a 10-year period. The aim of this study was to analyse specific aspects of electrical injuries and, with the information gathered, obtain data to delineate an efficient prevention strategy.
Materials and methods
A retrospective analysis of medical records of all the patients admitted to our Unit with electrical burns, from 1st January 2006 to 31st December 2015, was undertaken. Incomplete records, records from patients who abandoned hospital against medical advice and from those admitted for later reconstructive surgery were excluded.
Demographic data, mechanism of injury and electric current voltage, total burn surface area (TBSA), location and depth of burns, acute complications, ventilation status, surgical interventions and length of hospital stay (LOS) were analysed. We reviewed the frequency of amputations and classified them as minor or major. Minor amputations were performed at the digit level, while major amputations were performed above the ankle or the wrist. We also analysed the variety and frequency of reconstructive flap surgery. The patients were assigned to one of three groups according to the mechanism of injury: high-voltage, low-voltage or flash burn.
All continuous variables were presented as mean±standard deviation (SD), and the frequencies of categorical variables as percentages. Statistical data were analysed with the Mann- Whitney U and Chi-square tests, as appropriate. A P value<0.05 was considered statistically significant.
Results
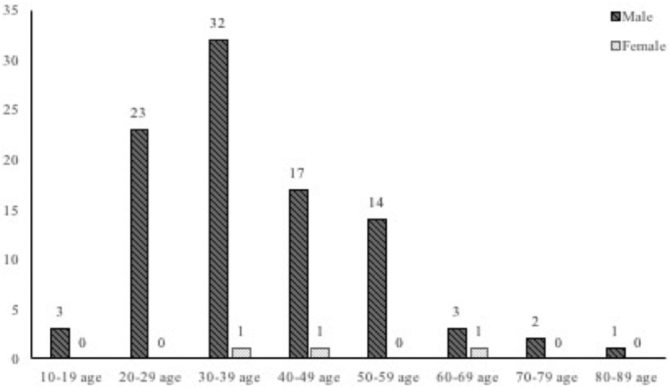
During the study period, 1695 burn patients were admitted to our Unit; 99 subjects (5.84%) suffered electrical burns. 97% (n=96) of these patients were male. The mean age was 38.3±13.7years. Age and gender data are shown in Fig. 1.
Fig. 1. Gender and age distribution of patients with electrical burns.
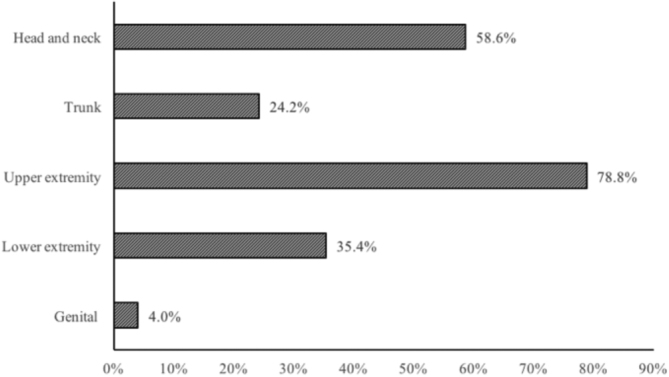
The mechanism of injury was occupational in 75 cases (75.8%), household related in 8 cases (8.1%), self-inflicted in 2 cases (2.0%) and involved individuals who were stealing copper in 10 cases (10.1%). Mean TBSA was 11.9%±13.2%. The mortality rate in this group of patients was null. Upper extremities were found to be more frequently injured than lower extremities, with hand involvement in 60.6% of the cases (Fig. 2).
Fig. 2. Distribution of burns according to body area.
Injuries were classified as low-voltage burns (n=24), highvoltage burns (n=30) and flash burns (n=45). There were no records of lightning burns during the study period. Flash burns accounted for 45.5% of the electrical burns that required hospital admissions. 97.8% (n=44) of these patients were male. Mean age was 40.6±13.0 years and mean TBSA was 7.8%±4.4%. Mean LOS was 8.2±6.5 days, which was the shortest hospital stay observed among the three groups. There were no reports of acute complications, such as arrhythmia, acute renal failure or compartmental syndrome. With regards to treatment in this group, 13.3% of these patients needed at least one surgical procedure but there was no need for amputations or reconstructive surgery with flaps.
Table I depicts the differences between high and low voltage groups of patients. TBSA, mean LOS and serum creatinine kinase (CK) levels were significantly higher in patients with high-voltage injury in comparison to low-voltage injury. The incidence of escharotomy/ fasciotomy and flap surgeries was also significantly higher in the high-voltage group. Although there was a higher incidence of amputations in this group (16.7% vs. 12.5%), the difference was not statistically significant. Regarding major amputations, there were no reports in the low-voltage group. On the other hand, in the high-voltage group there were 2 major amputations (Table II). Data regarding reconstructive flap surgery is shown in Table III.
Table I. Comparison between high-voltage and low-voltage groups.
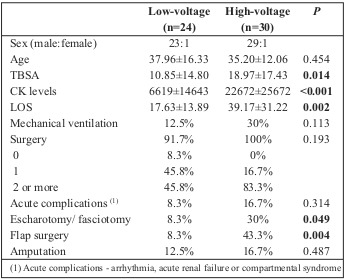
Table II. Summary of amputations required.
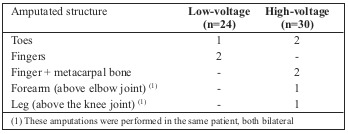
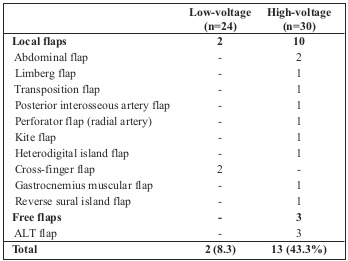
Table III. Summary of reconstructive procedures - flap surgeries.
We would like to point out a rather interesting finding regarding our epidemiological data which relates to electrical burns resulting from illicit activities, namely copper theft; this group comprises 10.1% of our study population. All of the individuals were male, 90% of whom had drug addiction problems, with a mean age of 35.80±9.33 years. Mean TBSA was 17.75%±13.27% and mean LOS was 38.30±28.69 days. Surgical treatment was given to all the patients: one procedure was sufficient in only 1 case (10%), while the others underwent 2 or more surgical procedures. Escharotomies/ fasciotomies were performed in 50% of these patients. A total of 4 flaps were performed in 4 of these patients (40%) and one minor extremity amputation was required.
Discussion
Electrical burns occur less frequently than scald or flame burns, but are still a cause of important morbidity, particularly in cases of high-voltage injury.3,7 Electrical trauma was responsible for 5.8% of the admissions to our Burn Unit. Reports from other studies show that the incidence of electrical burns varies from 4.5% in Brazil to 21% in Turkey.8,9 In this study, 97% of electrical burn injuries occurred in men and the mean age was 35 years, which is in accordance with data reported in the literature. 1,2,4,5,7,10 Most of our patients were young active males, with injuries occurring as occupational hazards. Consequently, electrical injury should be considered a potentially debilitating factor for the working-age population. Nevertheless, a relevant group in our study relates to electrical burns as a result of copper theft. This might be explained by our difficult socio-economic climate over the past few years, associated with an upward trend in copper prices.7 This incidence may be underestimated in our data since many patients do not report the truth about their accidents due to the fear of being arrested. As seen from our results, burn injury due to theft of copper comes with great cost to both the patient (usually young men) and to society.
Based on other reports, low-voltage injuries comprise 20% to 44.7% of all electrical injuries, and high-voltage injuries 38% to 50%.3-5 In our study, low-voltage burns accounted for 24.2% of injuries. On the other hand, high-voltage burns accounted for 30.3% of our study population, a slightly lower value compared to those encountered by other authors.3-5 Flash burns represented 45.5% of electrical injuries, being the major cause of electrical burns in our study. These results are in accordance with reports from Arnoldo et al.5 However, contradictory results were shown by other studies3-4 which reported flash burns as the third cause of electrical burns, after low- and high-voltage injuries. This high prevalence of flash burns may be explained by insufficient training in workplaces as well as poor adherence to safety measures since most of these occurred as work-related accidents.
This study, like others,4,5,11 identified the high-voltage injury group as potentially the most debilitating, since it is more often associated with deep muscle necrosis, hence requiring fasciotomy and, in the more severe cases, amputation. CK serum levels may provide a prognostic parameter for the clinical outcome of patients with electrical burns.12,13 Arenholz et al.12 have demonstrated that significantly elevated CK values are associated with longer LOS and a greater risk of skin grafting or amputation. Later, Kopp et al.13 added that, in the high-voltage group, patients with higher levels of CK were most likely to develop serious complications. In our study, CK serum levels were significantly higher in the high-voltage group. Our results also showed that these patients had longer hospitalization, a significantly higher incidence of escharotomy/ fasciotomy and a higher incidence of acute complications and amputation.
Tharim et al.14 studied the demographic characteristics, motif and outcomes of the amputations in patients who suffered burn injury. Their results showed a higher amputation rate in those with electrical burns. Amputation rate in our population was 8.1%. Although there was no statistical significance, the amputation rate in the high-voltage group was higher than in the low-voltage group, which confirms other studies’ findings. 10,15 Electrical flash burn damages skin but it usually does not involve deep tissues.10 Though some surgical procedures were performed in this group, there was no need for amputation.
Regarding reconstruction, simple surgical procedures, such as skin grafts or artificial dermis are useful on more superficial injuries. Regional or free flaps are useful if the injury is severe. Local flaps are primarily used to correct small defects, 15 such as those in the low-voltage group. In the high-voltage group, local and distant flaps were primarily used, but free flaps were also used for wide and complex defects with deep structure exposure.15 In our study, free flaps were only performed in the high-voltage group.
The overall mortality rate from electrical burns has been reported to be somewhere in between 0% and 21.7%.16,17 All 99 patients treated at our Burn Unit during this 10-year period survived. We consider that the overall in-hospital survival of 100% may be at least partially explained by the early transfer of patients to our Burn Unit, aggressive fluid resuscitation, continuous hemodynamic and metabolic support, and early aggressive surgical intervention. Another reason might be the exclusion of those patients who died before arriving at the hospital. One of the limitations of our work is that follow-up was not performed in order to obtain information about the delayed complications and adverse effects of electrical burn injury on quality of life.
Conclusion
Although their incidence is rather low, electrical burns may lead to an important socioeconomic burden due to their high morbidity. The high prevalence of electrical burns in young males and workers emphasizes the need to review occupational safety regulations. Educational efforts regarding potential hazards of electricity and reinforcing compliance with safety measures are essential for avoiding these injuries.
Acknowledgments
Conflict of interest.The authors declare that they have no conflict of interest.
References
- 1.Mohammadi AA, Amini M, Mehrabani D, Kiani Z. A survey on 30 months electrical burns in Shiraz University of Medical Sciences Burn Hospital. Burns. 2008;34(1):111–113. doi: 10.1016/j.burns.2006.12.007. [DOI] [PubMed] [Google Scholar]
- 2.Ghavami Y, Mobayen MR, Vaghardoost R. Electrical burn injury: a five-year survey of 682 patients. Trauma Mon. 2014;19(4):e18748. doi: 10.5812/traumamon.18748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kurt A, Yıldırım K, Yağmur Ç, Kelahmetoğlu O. Electrical burns: highlights from a 5-year retrospective analysis. Ulus Travma Acil Cerrahi Derg. 2016;22(3):278–282. doi: 10.5505/tjtes.2015.55491. [DOI] [PubMed] [Google Scholar]
- 4.Luz DP, Millan LS, Alessi MS, Uguetto WF. Electrical burns: a retrospective analysis across a 5-year period. Burns. 2009;35(7):1015–1019. doi: 10.1016/j.burns.2009.01.014. [DOI] [PubMed] [Google Scholar]
- 5.Arnoldo BD, Purdue GF, Kowalske K, Helm PA. Electrical injuries: a 20-year review. J Burn Care Rehabil. 2004;25(6):479–484. doi: 10.1097/01.bcr.0000144536.22284.5c. [DOI] [PubMed] [Google Scholar]
- 6.Maghsoudi H, Adyani Y, Ahmadian N. Electrical and lightning injuries. J Burn Care Res. 2007;28(2):255–261. doi: 10.1097/BCR.0B013E318031A11C. [DOI] [PubMed] [Google Scholar]
- 7.Aguilera-Saéz J, Binimelis MM, Collado JM, dos Santos BP. Electrical burns in times of economic crisis: a new epidemiologic profile. Burns. 2016;42(8):1861–1866. doi: 10.1016/j.burns.2016.06.016. [DOI] [PubMed] [Google Scholar]
- 8.Carvalho CM, Faria GEL, Milcheski DA, Gomez DS. Clinical epidemiological study of victims of electrical burns in the last 10 years. Rev Bras Queimaduras. 2012;11(4):230–232. [Google Scholar]
- 9.Nursal TZ, Yidirim S, Tarim A, Caliskan K. Burns in Southern Turkey: electrical burns remain a major problem. Burn Care Rehabil. 2003;24(5):309–314. doi: 10.1097/01.BCR.0000085876.28504.EE. [DOI] [PubMed] [Google Scholar]
- 10.Aghakhani K, Heidari M, Tabatabaee SM, Abdolkarimi L. Effect of current pathway on mortality and morbidity in electrical burn patients. Burns. 2015;41(1):172–176. doi: 10.1016/j.burns.2014.06.008. [DOI] [PubMed] [Google Scholar]
- 11.Duci SB, Arifi HM, Ahmeti HR, Selmani ME. Electrical burn injuries of 246 patients treated at the University Clinical Center of Kosovo during the period 2005-2010. Euro J Trauma Emerg Surg. 2014;40(6):679–685. doi: 10.1007/s00068-014-0379-6. [DOI] [PubMed] [Google Scholar]
- 12.Ahrenholz DH, Schubert W, Solem LD. Creatine kinase as a prognostic indicator in electrical injury. Surgery. 1998;104(4):741–747. [PubMed] [Google Scholar]
- 13.Kopp J, Loos B, Spilker G, Horch RE. Correlation between serum creatinine kinase levels and extent of muscle damage in electrical burns. Burns. 2004;30(7):680–683. doi: 10.1016/j.burns.2004.05.008. [DOI] [PubMed] [Google Scholar]
- 14.Tarim A, Ezer A. Electrical burn is still a major risk for amputations. Burns. 2013;39(2):354–357. doi: 10.1016/j.burns.2012.06.012. [DOI] [PubMed] [Google Scholar]
- 15.Kym D, Seo DK, Hur GY, Lee JW. Epidemiology of electrical injury: differences between low- and high-voltage electrical injuries during a 7-year study period in South Korea. Scand J Surg. 2015;104(2):108–114. doi: 10.1177/1457496914534209. [DOI] [PubMed] [Google Scholar]
- 16.Hanumadass ML, Voora SB, Kagan RJ, Matsuda T. Acute electrical burns: a 10-year clinical experience. Burns Incl Therm Inj. 1986;12(6):427–431. doi: 10.1016/0305-4179(86)90039-2. [DOI] [PubMed] [Google Scholar]
- 17.Acosta AS, Azarcon-Lim J, Ramirez AT. Survey of electrical burns in Philippine General Hospital. ANN N Y Acad Sci. 19999;888:12–18. doi: 10.1111/j.1749-6632.1999.tb07938.x. [DOI] [PubMed] [Google Scholar]