

Abstract
Background:
The optimal management of HBsAg-negative, anti-HBc-positive patients who receive immunosuppression remains unclarified. We systematically reviewed the available data on potential predictors of the risk of hepatitis B virus (HBV) reactivation in such patients.
Methods:
A literature search identified 55 studies with 3640 HBsAg-negative, anti-HBc-positive patients who received immunosuppressive regimens.
Results:
HBV reactivation was reported in 236 (6.5%) patients. The pooled HBV reactivation rates did not differ between patients with detectable or undetectable HBV DNA in studies with hematological diseases or regimens containing rituximab, but it was higher in patients with detectable than in those with undetectable HBV DNA who were taking rituximab-free regimens (14% vs. 2.6%; risk ratio [RR] 12.67, 95% CI: 95%CI 2.39-67.04, P=0.003) or had non-hematological diseases, although the latter was not confirmed by sensitivity analysis (RR 8.80, 95%CI 0.71-109.00, P=0.09). The pooled HBV reactivation rates were lower in patients with positive than in those with negative anti-HBs in studies with hematological (7.1% vs. 21.8%; RR 0.29, 95%CI 0.19-0.46, P<0.001) or non-hematological (2.5% vs. 10.7%; RR 0.28, 95%CI 0.11-0.76, P=0.012) diseases, and rituximab-containing (6.6% vs. 19.8%; RR 0.32, 95%CI 0.15-0.69, P=0.003) or rituximab-free (3.3% vs. 9.2%; RR 0.36, 95%CI 0.14-0.96, P=0.042) regimens.
Conclusions:
The risk of HBV reactivation is high; therefore, anti-HBV prophylaxis should be recommended in HBsAg-negative, anti-HBc-positive patients with hematological diseases and/or rituximab-containing regimens, regardless of HBV DNA and anti-HBs status. In contrast, patients with non-hematological diseases or rituximab-free regimens have a low risk of HBV reactivation and may not require anti-HBV prophylaxis if they have undetectable HBV DNA and positive anti-HBs.
Keywords: Chronic hepatitis B infection, antiviral therapy, lamivudine, entecavir, tenofovir
Introduction
Although HBsAg-negative, anti-HBc-positive patients have a lower risk of hepatitis B virus (HBV) reactivation compared to HBsAg-positive patients, the prevalence of anti-HBc is higher than that of HBsAg, ranging from 5% in Western to >50% in Far Eastern countries [1-3]. Thus, there are numerically many cases of HBV exacerbations in HBsAg-negative, anti-HBc-positive patients who receive immunosuppressive regimens. Recommendations based mostly on expert opinion state that HBsAg-negative, anti-HBc-positive patients with detectable HBV DNA should be managed similarly to HBsAg-positive patients, while those with undetectable HBV DNA should be followed carefully, with frequent aminotransferases and HBV DNA determinations, or should receive prophylaxis with lamivudine [3]. The type of immunosuppressive regimen seems to affect the probability of HBV reactivation in this setting. In particular, rituximab, an increasingly used anti-CD20 chimeric monoclonal antibody, has been associated with severe HBV reactivations in HBsAg-negative, anti-HBc-positive patients [1].
Recently, the American Gastroenterological Association [4] strongly recommended antiviral prophylaxis in HBsAg-negative, anti-HBc-positive patients treated with B-cell-depleting agents (e.g., rituximab, ofatumumab) because they were considered to be at high risk (>10%) of HBV reactivation. In the same position paper, all the other HBsAg-negative, anti-HBc-positive patients were considered to be at moderate (1-10%) or low (<1%) risk for HBV reactivation [4]. The latter recommendations were considered as weak and based on evidence of moderate quality. In addition, the usefulness of baseline HBV DNA evaluation is not reported, while the document counseled against using anti-HBs to stratify the risk of HBV reactivation [4]. Since literature data are scarce and no strong recommendation has been made, the optimal management of such cases remains controversial.
We systematically evaluated the available data in order to assess the risk of HBV reactivation in HBsAg-negative, anti-HBc-positive patients under immunosuppression in relation to their baseline HBV status (HBV DNA and anti-HBs), as well as the type of underlying primary disease (hematological vs. non-hematological) and immunosuppressive regimen (rituximab-containing vs. rituximab-free).
Materials and methods
Data sources and searches
PubMed and Scopus from January 2006 to February 2015 were searched to identify all medical literature included under the terms “hepatitis B” and “reactivation” or “immunosuppression” or “immunosuppressive therapy”. In addition, a manual search of all relevant review articles and of the retrieved original studies was performed.
Study selection
All studies published in English were included if they fulfilled all of the following criteria: 1) they were randomised trials or observational cohort studies; 2) they included adult patients with past HBV infection (i.e., HBsAg-negative, anti-HBc-positive patients) who received immunosuppressive regimens; and 3) there were patients without pre-emptive prophylaxis with nucleos(t)ide analogs (NAs) against HBV reactivation and with available data on the incidence of HBV reactivation. Studies evaluating solid organ transplant anti-HBc-positive recipients were excluded. In each selected study, only patients with a past HBV infection were evaluated, while HBsAg-positive patients were excluded. The only studies analyzed were those that included a comparative evaluation of differences in the risk for HBV reactivation between different groups of patients. The literature search was performed by one author (EC), who screened titles and abstracts and determined which studies could potentially be included. Each study in the list of the preselected papers was independently evaluated by two reviewers (EC, GP) to determine whether it fulfilled all the inclusion criteria.
Data extraction and quality assessment
Data extraction from the finally selected papers was carried out by two authors (EC, PC) according to a predefined form. Any queries regarding data extraction were arbitrated by discussion with another author (GP). Data extracted for selected studies included country and center(s), date of publication, type of study, sample size, age, sex, HBV status before initiation of immunosuppression regarding anti-HBs positivity and HBV DNA detectability, underlying primary disease (hematological or not), type of immunosuppressive regimen (rituximab or not), follow-up period, number of patients with HBV reactivation, administration of NAs after HBV reactivation, and final outcome. A pilot data extraction form was tested and revised. We categorized the included studies as randomized controlled trials (RCTs), prospective or retrospective cohort studies. The Cochrane Collaboration’s tool for assessing the risk of bias in RCTs [5] and the Newcastle Ottawa Scale [6] were used to assess the quality of the included randomized and nonrandomized studies, respectively.
Data synthesis and analysis
The outcome of interest involved HBV reactivation in two separate groups: patients with or without hematological disease and patients receiving rituximab-containing or rituximab-free regimens. The pooled rate of HBV reactivation (pi) was estimated by the inverse variance method, transforming to logits using the equation lpi=log(pi/[1-pi]) with the corresponding variance being 1/(Ni×pi×[1-pi]), where pi represents the estimated probability from the study and Ni represents the corresponding reference population at baseline. Pooled logit estimates and their 95% confidence intervals (CI) were back-transformed to probabilities by the inverse logit transformation pi=elpi/(elpi+1), where e is the base of the natural logarithm [7].
Meta-analysis aims to synthesize the outcomes of each included study into one weighted average to estimate the intervention effect, along with 95%CI to assess the statistical significance. Risk ratios (RR) were calculated for the predefined outcomes and studies were weighted against the natural logarithm of the variance of RR. Random-effects meta-analysis was chosen in advance as the analysis method, to incorporate the assumption that the true effect varies across studies. In cases of zero responders, zero was replaced by 0.5, and the number of participants was corrected accordingly. Funnel plots were produced to visually inspect for publication bias and were assessed using the modified Harbord’s test for outcomes when there were ≥10 studies available [8,9].
Heterogeneity was examined visually in the forest plots and its extent was estimated using the I2 measure, as proposed by Higgins et al [10], as low (I2=25-49%), moderate (I2=50-74%) and high (I2≥75%). All analyses were performed using STATA, version 12.0. We considered P<0.05 (two-sided) as significant.
Results
In total, 1120 articles were initially identified from the literature search, but only 58 studies [11-68] fulfilled the inclusion criteria. Six studies, two from a single center in China [32,66], two from a single center in Japan [22,67] and two from Turkey [51,68], had overlapping study periods; in these cases, only the more recent study from each center was included [22,32,51]. Thus, 55 studies with a total of 3640 HBsAg-negative, anti-HBc patients were included in our analysis [11-65]. Study and patient characteristics are presented in Table 1. There was only one RCT [34], 25 prospective [11,13,15,18-23,26,27,29,30,32,35,41,42,47,55-57,60,63-65], 2 prospective/retrospective [17,37], and 27 retrospective cohort studies [12,14,16,24,25,28,31,33,36,38-40,43-46,48-54,58,59,61,62]. The RCT and 26 (48%) of the 54 nonrandomized studies were of low quality.
Table 1.
Published studies regarding reactivation of hepatitis B virus (HBV) infection in HBsAg-negative, anti-HBc-positive patients receiving immunosuppressive therapy

HBV reactivation under immunosuppressive regimens
HBV reactivation was detected in 6.5% (236/3640) of HBsAg-negative, anti-HBc-positive patients who received immunosuppressive regimens during a median follow up of 24 months (range: 12-49). The definition of HBV reactivation was based on HBsAg reappearance and/or HBV DNA increase (with elevated levels of aminotransferases in 4 studies [27,42,47,54]). The rates of HBV reactivation ranged from 0-85.7% in 22 studies that defined reactivation as both HBsAg reappearance and HBV DNA increase [11-13,20,23,24,26,31-33,36,37,40,42,44,46-48,51,54,56,63], from 0-19.6% in 12 studies that defined reactivation as HBsAg reappearance alone [14,17,19,28,38,39,41,43,45,49,55,62], and from 0-17.9% in 16 studies that defined reactivation as an increase in HBV DNA alone [15,16,18,22,25,27,29,30,34,35,52,53,57,59,60,65]. No definition of HBV reactivation was provided in 5 studies that included 306 patients [21,50,58,61,64].
HBV reactivation occurred during immunosuppressive therapy in 58 patients (between 30 and 300 days after the initiation of immunosuppressive therapy) and after the cessation of immunosuppression in 48 patients (between 14 and 670 days after immunosuppression discontinuation) [12,15,16,28,32,37,40,44,45,48,53-56,59,64,65]. No data regarding the timing of HBV reactivation were provided for 130 patients.
HBV reactivation in patients with or without hematological diseases
The total pooled rate of HBV reactivation was significantly higher in patients with detectable than in those with undetectable serum baseline HBV DNA: 18.8% (95%CI 11.8-28.7) vs. 5.7% (95%CI 3.2-9.8); RR 4.27 (95%CI 1.45-12.56); P=0.008; I2=31.3%, P for heterogeneity=0.149 (Fig. 1). Evidence of bias was found in HBV DNA comparisons for HBV reactivation risk by visual inspection of funnel plots and by Harbord’s modified test (P=0.019).
Figure 1.
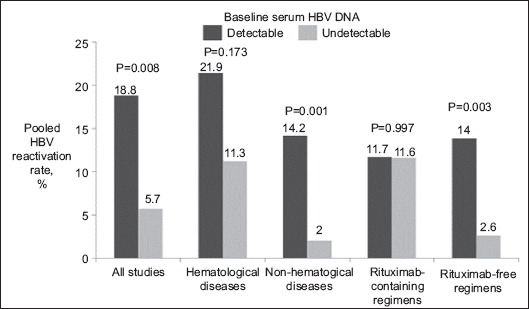
Pooled rates of hepatitis B virus (HBV) reactivation in different subgroups of HBsAg-negative, anti-HBc-positive patients in relation to their baseline serum HBV DNA detectability
The total pooled rate of HBV reactivation was also lower in patients with positive than in those with negative anti-HBs: 5.2% (95%CI 3.5-7.6) vs. 17.0% (95%CI 12.5-22.6); RR 0.29 (95%CI 0.19-0.44), P<0.001; I2=0%, P for heterogeneity=0.993 (Fig. 2). Visual inspection of funnel plots and Harbord’s modified test found no evidence of bias in anti-HBs comparisons for HBV reactivation risk (P=0.212).
Figure 2.
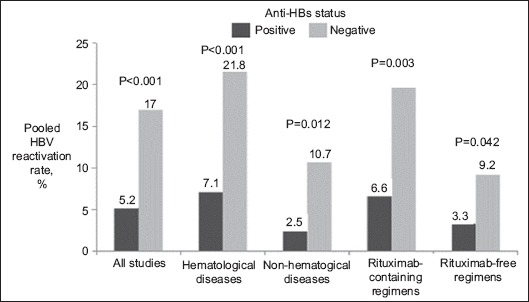
Pooled rates of hepatitis B virus (HBV) reactivation in different subgroups of HBsAg-negative, anti-HBc-positive patients in relation to their baseline anti-HBs status
The pooled rate of HBV reactivation was 10.9% (95%CI 7.8-14.9) in studies including patients with hematological and 3.6% (95%CI 2.2-5.7) in studies including patients with non-hematological diseases. Since no individual study included patients from both groups, no appropriate conclusion could be drawn regarding the RR for HBV reactivation in patients with hematological diseases compared to those with non-hematological diseases.
Comparing patients with detectable and undetectable serum baseline HBV DNA, the pooled rate of HBV reactivation was significantly higher in studies with non-hematological diseases: 14.2% (95%CI 6.9-26.9) vs. 2.0% (95%CI 1.1-3.6); RR 20.59 (95%CI 3.34-126.94), P=0.001; I2=0%, P for heterogeneity=0.788 [18,20,29,32]. However, it was only numerically higher in studies with hematological diseases: 21.9% (95%CI 12.9-34.7) vs. 11.3% (95%CI 6.3-19.5); RR 2.33 (95%CI 0.69-7.83), P=0.173; I2=30.5%, P for heterogeneity=0.195 [15,17,34,35,44,47,56] (Fig. 1, 3). In order to explore the wide 95%CIs, we conducted a sensitivity analysis excluding studies with uncertainty in estimates. Patients with detectable rather than undetectable baseline HBV DNA had a numerically higher risk for HBV exacerbation in studies with non-hematological diseases: RR 8.80 (95%CI 0.71-109.00), P=0.090 I2=0%, P for heterogeneity=0.965 [18,20]. However, there was no difference in studies with hematological patients: RR 0.96 (95%CI 0.32-2.89), P=0.938; I2=0%, P for heterogeneity=0.795 [15,34,35,44,56].
Figure 3.
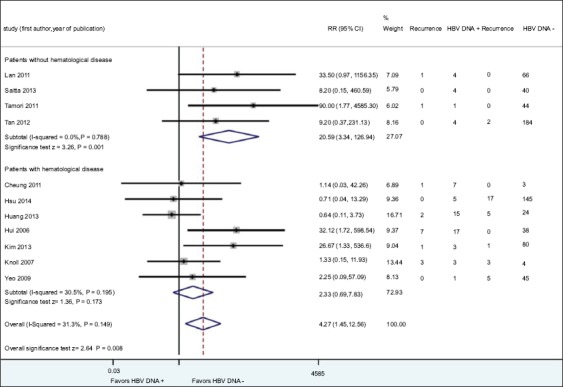
Forest plots of rates of hepatitis B virus (HBV) reactivation between HBsAg-negative, anti-HBc-positive patients with detectable and undetectable HBV DNA in studies with or without hematological diseases
RR, relative risk; 95%CI, 95% confidence interval.
Likewise, the pooled rate of HBV reactivation was lower in patients with positive than in those with negative anti-HBs in studies with hematological—7.1% (95%CI 4.4-11.2) vs. 21.8% (95%CI 15.3-30.1); RR 0.29 (95%CI 0.19-0.46), P<0.001, I2=0%, P for heterogeneity=0.862 [15-17,25,28,32,34-36,39,41,44,47,51,55,61]—or non-hematological—2.5% (95%CI 1.5-4.6) vs. 10.7% (95%CI 5.7-19.0); RR 0.28 (95%CI 0.11-0.76) P=0.012; I2=0%, P for heterogeneity=0.987 [13,18,19,22,23,26,30,33,42,50,52,58,59,62]—diseases (Fig. 2, 4).
Figure 4.
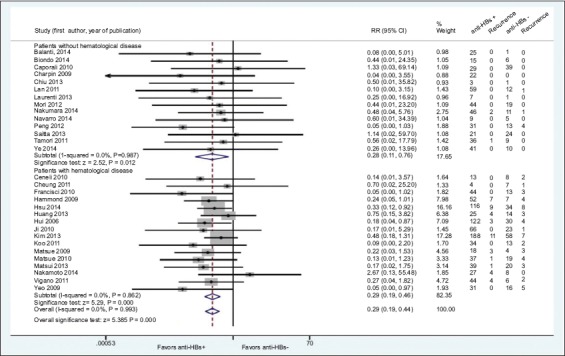
Forest plots of rates of hepatitis B virus (HBV) reactivation between HBsAg-negative, anti-HBc-positive patients with positive and negative anti-HBs in studies with or without hematological diseases
RR, relative risk; 95%CI, 95% confidence interval.
HBV reactivation with or without rituximab
The pooled rate of HBV reactivation was numerically higher in patients treated with rituximab-containing than in those with rituximab-free regimens: 9.7% (95%CI 6.3-14.6) vs. 4.1% (95%CI 2.8-6.1); RR 1.80 (95%CI 0.99-3.28), P=0.056; I2=0%, P for heterogeneity=0.849 (Fig. 5). Both groups had numerically close mean durations of follow up (20±12 vs. 22±10 months). The directions of the results were similar even when the rates of HBV reactivation were evaluated separately in prospective—RR 4.91 (95%CI 0.93-26.09), P=0.062 [35,47,63]—and retrospective—RR 1.49 (95%CI 0.74-2.98), P=0.265 [14,25,39,44,45,54]-studies.
Figure 5.

Forest plots of rates of hepatitis B virus (HBV) reactivation between HBsAg-negative, anti-HBc-positive patients treated with and without rituximab-containing regimens
RR, relative risk; 95%CI, 95% confidence interval.
HBV reactivation developed after the cessation of immunosuppression in 26 (42%) of 62 patients receiving rituximab-containing regimens (range: 14-409 days) and 6 (32%) of 19 patients receiving rituximab-free regimens (range: 90-300 days). No conclusions could be drawn because of the lack of available data concerning the incidence of HBV reactivation in patients: a) receiving rituximab-containing regimens for hematological vs. non-hematological diseases; or b) receiving rituximab alone vs. rituximab in combination with other regimens, particularly steroids.
The pooled rate of HBV reactivation was significantly higher in patients with detectable than in those with undetectable baseline serum HBV DNA treated with rituximab-free regimens: 14.0% (95%CI 7.5-24.7) vs. 2.6% (95%CI 1.2-5.3); RR 12.67 (95%CI 2.39-67.04), P=0.003; I2=0%, P for heterogeneity=0.599 [18,20,29,32,34]. However, no such difference was seen in patients treated with rituximab-containing regimens: 11.7% (95%CI 6.5-20.2) vs. 11.6% (95%CI 5.0-24.7); RR 1.00 (95%CI 0.25-3.97), P=0.997; I2=0%, P for heterogeneity=0.412 [15,34,65] (Fig. 1).
In contrast to baseline HBV DNA status, anti-HBs seropositivity affected the risk of HBV reactivation regardless of rituximab therapy. In particular, the pooled rate of HBV reactivation was lower in patients with than in those without anti-HBs treated with rituximab-containing—6.6% (95%CI 2.9-14.4) vs. 19.8% (95%CI 15.6-24.7); RR 0.32 (95%CI 0.15-0.69), P=0.003; I2=0%, P for heterogeneity=0.736 [15,25,28,32,34,35]—or rituximab-free regimens—3.3% (95%CI 2.0-5.5) vs. 9.2% (95%CI 5.3-15.4); RR 0.36 (95%CI 0.14-0.96), P=0.042; I2=0%, P for heterogeneity=0.988 [12,17,18,24,22,25,29,32,34,49,51,57,58,61] (Fig. 2).
Outcomes of patients with HBV reactivation
Data regarding outcomes were provided in 174 (73.8%) of 236 patients with HBV reactivation, while data regarding antiviral therapy after the onset of HBV reactivation were available for 148 (85%) of these 174 patients: 23 remained untreated and 125 were treated with NAs (entecavir: 56, lamivudine: 59, adefovir±lamivudine: 4, entecavir or lamivudine: 6) [12,15-17,21,23-25,27-41,44-48,51,54,65]. Twenty-two (14.9%) of the 148 patients died: 7/23 (30.4%) patients who remained untreated and 15/125 (12%) patients treated with NAs. Finally, 2 (3.5%) of 56 patients and 10 (17%) of 59 patients who received entecavir and lamivudine, respectively, for HBV reactivation died during the follow-up period [12,15-17,21,23-25,28-30,32-39,44,45,47,51,54].
Discussion
In this systematic review of more than 3600 HBsAg-negative, anti-HBc-positive patients who received immunosuppressive therapy we confirmed that patients treated with rituximab-containing regimens have a higher risk for HBV reactivation, compared to those receiving rituximab-free regimens: 9.7% vs. 4.1%; RR 1.80 (95%CI 0.99-3.28). No relevant studies were identified and therefore no conclusions could be drawn concerning the new generations of anti-CD20 monoclonal antibodies (e.g., ofatumumab, veltuzumab), developed recently. The pooled rates of HBV reactivation were 10.9% in patients with hematological diseases and 3.6% in patients with non-hematological diseases, but no direct statistical comparison could be drawn between these two groups because of limitations in the available data.
The detectability of baseline HBV DNA had no impact on the risk of HBV reactivation in patients at high risk due to the underlying disease or the immunosuppressive regimens. In particular, the pooled rates of HBV reactivation were similar in patients with detectable or undetectable HBV DNA treated with rituximab-containing regimens or having hematological diseases. In contrast, patients with detectable, compared to those with undetectable baseline HBV DNA had a higher risk for HBV reactivation if they were treated with rituximab-free regimens (14.0% vs. 2.6%; RR 12.67, P=0.003) or had non-hematological diseases (14.2% vs. 2%; RR 20.59, P=0.001), although the latter difference became insignificant in the sensitivity analysis (P=0.090). Practically, it could be suggested that in HBsAg-negative, anti-HBc-positive patients with non-hematological disease, or treated with rituximab-free regimens, HBV DNA evaluation is useful for stratification of the risk for HBV reactivation. However, in those who have hematological disease or are treated with rituximab-containing regimens, anti-HBV prophylaxis seems to be necessary in all cases, regardless of baseline HBV DNA status.
Although the current statement recommends against using anti-HBs status to guide antiviral prophylaxis [4], we found that positive compared to negative anti-HBs at baseline was associated with a significantly lower risk for HBV reactivation in all patient subgroups: those with hematological (7.1% vs. 21.8%, RR 0.29, 95%CI 0.19-0.46, P<0.001) or non-hematological diseases (2.5% vs. 10.7%, RR 0.28, 95%CI 0.11-0.76, P=0.012), and under rituximab-containing (6.6% vs. 19.8%, RR 0.32, 95%CI 0.15-0.69, P=0.003) or rituximab-free (3.3% vs. 9.2%, RR 0.36, 95%CI 0.14-0.96, P=0.042) regimens. This analysis was based on baseline anti-HBs status and not on baseline anti-HBs levels or their possible reduction during immunosuppression therapy, given the very limited literature data available. Based on these findings, and taking into account the impact of baseline HBV DNA, it could be suggested that anti-HBV prophylaxis seems to be necessary, irrespectively of baseline HBV DNA or anti-HBs status, in patients who have hematological disease or are under rituximab-containing regimens. On the other hand, in patients with non-hematological diseases under rituximab-free regimens, antiviral prophylaxis should be recommended in those with detectable baseline HBV DNA, regardless of anti-HBs status, but is not required in those with undetectable HBV DNA and positive anti-HBs. The decision for anti-HBV prophylaxis may be individualized in patients with non-hematological diseases under treatment with rituximab-free regimens and have undetectable HBV DNA and negative anti-HBs.
An interesting finding was that HBV reactivation developed in 26 (42%) of 62 patients receiving rituximab-containing regimens between 14 and 409 days after the cessation of immunosuppression and in 6 (32%) of 19 patients receiving rituximab-free regimens between 90 and 300 days after the end of immunosuppression. Thus, clinicians should continue to follow these patients closely for long after the completion of immunosuppression/chemotherapy, avoiding early discontinuation of possible anti-HBV prophylaxis.
The clinical presentation of HBV reactivation may vary from asymptomatic to acute liver failure and death [1]. Indeed, higher mortality has been reported in HBsAg-negative, anti-HBc-positive compared to HBsAg-positive patients, perhaps related to underestimation of the risk for HBV reactivation and the delay in diagnosis [1]. Thus, early diagnosis and prompt treatment initiation are crucial for the effective management of such cases not under anti-HBV prophylaxis. Of the 236 patients with HBV reactivation included in our review, 148 received NAs (mainly lamivudine or entecavir). The mortality rate was relatively high (15%), but the cause of death was not always clearly associated with the HBV reactivation, particularly in those who had hematological diseases or bone marrow transplantation. As might be expected, among the patients with HBV reactivation, mortality was 30% for those who remained untreated and 12% for those who received antiviral therapy. In addition, among the patients who received antiviral therapy for HBV reactivation, the mortality was 17% for those treated with lamivudine and 3.5% for those treated with entecavir. Although these data do not come from RCTs and direct comparison is not possible, it seems clinically more appropriate to use a high genetic barrier agent, like entecavir or tenofovir, whenever HBV reactivation is diagnosed. On the other hand, such data regarding antiviral therapy after HBV reactivation seem insufficient to justify a change in the current recommendation for the use of lamivudine as prophylaxis for HBsAg-negative, anti-HBc-positive patients who require immunosuppression, provided that serum HBV DNA is undetectable.
In conclusion, our findings favor the use of anti-HBV prophylaxis in HBsAg-negative, anti-HBc-positive patients with hematological diseases and/or under rituximab-containing regimens, regardless of their baseline anti-HBs and serum HBV DNA status. Antiviral prophylaxis should be given in HBsAg-negative, anti-HBc-positive patients with non-hematological diseases who are taking rituximab-free regimens and have detectable baseline HBV DNA, irrespectively of their anti-HBs status, but is not required in those with undetectable HBV DNA and positive anti-HBs. Since HBV reactivation often occurs after the completion of the immunosuppressive/chemotherapy courses, clinicians should continue anti-HBV prophylaxis and/or the follow up of such patients for at least 12 months after the discontinuation of immunosuppression. An agent with a high genetic barrier may be used in order to better optimize the management of HBV reactivations occurring in HBsAg-negative, anti-HBc-positive patients.
Summary Box.
What is already known:
HBsAg-negative, anti-HBc-positive patients have a lower risk of hepatitis B virus (HBV) reactivation compared to HBsAg-positive patients, but the prevalence of anti-HBc is higher than that of HBsAg
Antiviral prophylaxis is strongly recommended in HBsAg-negative, anti-HBc-positive patients treated with B-cell-depleting agents
The usefulness of baseline anti-HBs evaluation remains controversial
What the new findings are:
The use of anti-HBV prophylaxis is recommended in HBsAg-negative, anti-HBc-positive patients with hematological diseases and/or under rituximab-containing regimens, regardless of their baseline anti-HBs and serum HBV DNA status
Antiviral prophylaxis is not required in HBsAg-negative, anti-HBc-positive patients with non-hematological diseases who receive rituximab-free regimens and have undetectable HBV DNA and positive anti-HBs
The decision for anti-HBV prophylaxis may be individualized in patients with non-hematological diseases treated with rituximab-free regimens who have undetectable HBV DNA and negative anti-HBs
Since HBV reactivation often develops after the completion of the immunosuppressive/chemotherapy courses, clinicians should continue anti-HBV prophylaxis and/or the follow up of such patients for at least 12 months after discontinuation of immunosuppression
Biography
Medical School of National & Kapodistrian University, Athens; Medical School of Aristotle University of Thessaloniki; Medical School of Aristotle University, Hippokration General Hospital of Thessaloniki, Greece
Footnotes
Conflict of Interest: Evangelos Cholongitas has served as an advisor and/or lecturer for Bristol-Myers Squibb, Gilead and Novartis and has received research grants from Gilead. Anna-Bettina Haidich, Fani Apostolidou-Kiouti, Parthenis Chalevas: none. George Papatheodoridis has served as advisor/lecturer for Bristol-Myers Squibb, Gilead, Merck Sharp & Dohme, Novartis, Roche and has received research grants from Bristol-Myers Squibb, Gilead, Roche
References
- 1.Roche B, Samuel D. The difficulties of managing severe hepatitis B virus reactivation. Liver Int. 2011;31(Suppl 1):104–110. doi: 10.1111/j.1478-3231.2010.02396.x. [DOI] [PubMed] [Google Scholar]
- 2.Shouval D, Shibolet O. Immunosuppression and HBV reactivation. Semin Liver Dis. 2013;33:167–177. doi: 10.1055/s-0033-1345722. [DOI] [PubMed] [Google Scholar]
- 3.European Association for the Study of the Liver. EASL clinical practice guidelines: Management of chronic hepatitis B virus infection. J Hepatol. 2012;57:167–185. doi: 10.1016/j.jhep.2012.02.010. [DOI] [PubMed] [Google Scholar]
- 4.Reddy KR, Beavers KL, Hammond SP, Lim JK, Falck-Ytter YT, American Gastroenterological Association Institute American Gastroenterological Association Institute guideline on the prevention and treatment of hepatitis B virus reactivation during immunosuppressive drug therapy. Gastroenterology. 2015;148:215–219. doi: 10.1053/j.gastro.2014.10.039. [DOI] [PubMed] [Google Scholar]
- 5.Higgins JP, Altman DG, Gøtzsche PC, et al. Cochrane Statistical Methods Group The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi: 10.1136/bmj.d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wells G, Shea B, O'Connell D. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses (2004) Available from: http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm .
- 7.Greenland S, O'Rourke K. In: Meta-analysis Modern epidemiology. Rothman KJ, Greenland S, Lash TL, editors. Philadelphia, PA: Lippincott, Williams and Wilkins; 2008. pp. 652–682. [Google Scholar]
- 8.Harbord RM, Egger M, Sterne JA. A modified test for small-study effects in meta-analyses of controlled trials with binary endpoints. Stat Med. 2006;25:3443–3457. doi: 10.1002/sim.2380. [DOI] [PubMed] [Google Scholar]
- 9.Sterne JA, Sutton AJ, Ioannidis JP, et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ. 2011;343:d4002. doi: 10.1136/bmj.d4002. [DOI] [PubMed] [Google Scholar]
- 10.Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–560. doi: 10.1136/bmj.327.7414.557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Vassilopoulos D, Apostolopoulou A, Hadziyannis E, et al. Long-term safety of anti-TNF treatment in patients with rheumatic diseases and chronic or resolved hepatitis B virus infection. Ann Rheum Dis. 2010;69:1352–1355. doi: 10.1136/ard.2009.127233. [DOI] [PubMed] [Google Scholar]
- 12.Cassano N, Mastrandrea V, Principi M, et al. Anti-tumor necrosis factor treatment in occult hepatitis B virus infection: a retrospective analysis of 62 patients with psoriatic disease. J Biol Regul Homeost Agents. 2011;25:285–289. [PubMed] [Google Scholar]
- 13.Biondo MI, Germano V, Pietrosanti M, et al. Lack of hepatitis B virus reactivation after anti-tumour necrosis factor treatment in potential occult carriers with chronic inflammatory arthropathies. Eur J Intern Med. 2014;25:482–484. doi: 10.1016/j.ejim.2013.11.014. [DOI] [PubMed] [Google Scholar]
- 14.Mikulska M, Nicolini L, Signori A, et al. Hepatitis B reactivation in HBsAg-negative/HBcAb-positive allogeneic haematopoietic stem cell transplant recipients: risk factors and outcome. Clin Microbiol Infect. 2014;20:O694–O701. doi: 10.1111/1469-0691.12611. [DOI] [PubMed] [Google Scholar]
- 15.Hsu C, Tsou HH, Lin SJ, et al. Taiwan Cooperative Oncology Group Chemotherapy-induced hepatitis B reactivation in lymphoma patients with resolved HBV infection: a prospective study. Hepatology. 2014;59:2092–2100. doi: 10.1002/hep.26718. [DOI] [PubMed] [Google Scholar]
- 16.Matsui T, Kang JH, Nojima M, et al. Reactivation of hepatitis B virus in patients with undetectable HBsAg undergoing chemotherapy for malignant lymphoma or multiple myeloma. J Med Virol. 2013;85:1900–1906. doi: 10.1002/jmv.23694. [DOI] [PubMed] [Google Scholar]
- 17.Kim SJ, Hsu C, Song YQ, et al. Hepatitis B virus reactivation in B-cell lymphoma patients treated with rituximab: analysis from the Asia Lymphoma Study Group. Eur J Cancer. 2013;49:3486–3496. doi: 10.1016/j.ejca.2013.07.006. [DOI] [PubMed] [Google Scholar]
- 18.Chiu HY, Chen CH, Wu MS, Cheng YP, Tsai TF. The safety profile of ustekinumab in the treatment of patients with psoriasis and concurrent hepatitis B or C. Br J Dermatol. 2013;169:1295–1303. doi: 10.1111/bjd.12461. [DOI] [PubMed] [Google Scholar]
- 19.Saitta C, Musolino C, Marabello G, et al. Risk of occult hepatitis B virus infection reactivation in patients with solid tumours undergoing chemotherapy. Dig Liver Dis. 2013;45:683–686. doi: 10.1016/j.dld.2013.01.022. [DOI] [PubMed] [Google Scholar]
- 20.Papa A, Felice C, Marzo M, et al. Prevalence and natural history of hepatitis B and C infections in a large population of IBD patients treated with anti-tumor necrosis factor-αagents. J Crohns Colitis. 2013;7:113–119. doi: 10.1016/j.crohns.2012.03.001. [DOI] [PubMed] [Google Scholar]
- 21.Tan J, Zhou J, Zhao P, Wei J. Prospective study of HBV reactivation risk in rheumatoid arthritis patients who received conventional disease-modifying antirheumatic drugs. Clin Rheumatol. 2012;31:1169–1175. doi: 10.1007/s10067-012-1988-2. [DOI] [PubMed] [Google Scholar]
- 22.Mori S. Do low titers of antibody against hepatitis B surface antigen carry a risk of viral reactivation during immunosuppressive therapy for rheumatic diseases? J Rheumatol. 2012;39:1292–1293. doi: 10.3899/jrheum.120052. [DOI] [PubMed] [Google Scholar]
- 23.Peng JW, Lin GN, Xiao JJ, Jiang XM. Hepatitis B virus reactivation in hepatocellular carcinoma patients undergoing transcatheter arterial chemoembolization therapy. Asia Pac J Clin Oncol. 2012;8:356–361. doi: 10.1111/j.1743-7563.2012.01534.x. [DOI] [PubMed] [Google Scholar]
- 24.Morisco F, Castiglione F, Rispo A, et al. Hepatitis B virus infection and immunosuppressive therapy in patients with inflammatory bowel disease. Dig Liver Dis. 2011;43(Suppl 1):S40–S48. doi: 10.1016/S1590-8658(10)60691-3. [DOI] [PubMed] [Google Scholar]
- 25.Ji D, Cao J, Hong X, et al. Low incidence of hepatitis B virus reactivation during chemotherapy among diffuse large B-cell lymphoma patients who are HBsAg-negative/HBcAb-positive: a multicenter retrospective study. Eur J Haematol. 2010;85:243–250. doi: 10.1111/j.1600-0609.2010.01474.x. [DOI] [PubMed] [Google Scholar]
- 26.Caporali R, Bobbio-Pallavicini F, Atzeni F, et al. Safety of tumor necrosis factor alpha blockers in hepatitis B virus occult carriers (hepatitis B surface antigen negative/anti-hepatitis B core antigen positive) with rheumatic diseases. Arthritis Care Res (Hoboken) 2010;62:749–754. doi: 10.1002/acr.20130. [DOI] [PubMed] [Google Scholar]
- 27.Loras C, Gisbert JP, Mínguez M, et al. GETECCU (Grupo Español de Enfermedades de Crohn y Colitis Ulcerosa) Group Liver dysfunction related to hepatitis B and C in patients with inflammatory bowel disease treated with immunosuppressive therapy. Gut. 2010;59:1340–1346. doi: 10.1136/gut.2010.208413. [DOI] [PubMed] [Google Scholar]
- 28.Matsue K, Kimura S, Takanashi Y, et al. Reactivation of hepatitis B virus after rituximab-containing treatment in patients with CD20-positive B-cell lymphoma. Cancer. 2010;116:4769–4776. doi: 10.1002/cncr.25253. [DOI] [PubMed] [Google Scholar]
- 29.Urata Y, Uesato R, Tanaka D, et al. Prevalence of reactivation of hepatitis B virus replication in rheumatoid arthritis patients. Mod Rheumatol. 2011;21:16–23. doi: 10.1007/s10165-010-0337-z. [DOI] [PubMed] [Google Scholar]
- 30.Tamori A, Koike T, Goto H, et al. Prospective study of reactivation of hepatitis B virus in patients with rheumatoid arthritis who received immunosuppressive therapy: evaluation of both HBsAg-positive and HBsAg-negative cohorts. J Gastroenterol. 2011;46:556–564. doi: 10.1007/s00535-010-0367-5. [DOI] [PubMed] [Google Scholar]
- 31.Sugauchi F, Tanaka Y, Kusumoto S, et al. Virological and clinical characteristics on reactivation of occult hepatitis B in patients with hematological malignancy. J Med Virol. 2011;83:412–418. doi: 10.1002/jmv.21995. [DOI] [PubMed] [Google Scholar]
- 32.Koo YX, Tay M, Teh YE, et al. Risk of hepatitis B virus (HBV) reactivation in hepatitis B surface antigen negative/hepatitis B core antibody positive patients receiving rituximab-containing combination chemotherapy without routine antiviral prophylaxis. Ann Hematol. 2011;90:1219–1223. doi: 10.1007/s00277-011-1241-0. [DOI] [PubMed] [Google Scholar]
- 33.Lan JL, Chen YM, Hsieh TY, et al. Kinetics of viral loads and risk of hepatitis B virus reactivation in hepatitis B core antibody-positive rheumatoid arthritis patients undergoing anti-tumour necrosis factor alpha therapy. Ann Rheum Dis. 2011;70:1719–1725. doi: 10.1136/ard.2010.148783. [DOI] [PubMed] [Google Scholar]
- 34.Huang YH, Hsiao LT, Hong YC, et al. Randomized controlled trial of entecavir prophylaxis for rituximab-associated hepatitis B virus reactivation in patients with lymphoma and resolved hepatitis B. J Clin Oncol. 2013;31:2765–2772. doi: 10.1200/JCO.2012.48.5938. [DOI] [PubMed] [Google Scholar]
- 35.Cheung WI, Lin SY, Leung VK, et al. Prospective evaluation of seropositive occult hepatitis B viral infection in lymphoma patients receiving chemotherapy. Hong Kong Med J. 2011;17:376–380. [PubMed] [Google Scholar]
- 36.Matsue K, Aoki T, Odawara J, et al. High risk of hepatitis B-virus reactivation after hematopoietic cell transplantation in hepatitis B core antibody-positive patients. Eur J Haematol. 2009;83:357–364. doi: 10.1111/j.1600-0609.2009.01291.x. [DOI] [PubMed] [Google Scholar]
- 37.Fukushima N, Mizuta T, Tanaka M, et al. Retrospective and prospective studies of hepatitis B virus reactivation in malignant lymphoma with occult HBV carrier. Ann Oncol. 2009;20:2013–2017. doi: 10.1093/annonc/mdp230. [DOI] [PubMed] [Google Scholar]
- 38.Ferraro D, Pizzillo P, Di Marco V, et al. Evaluating the risk of hepatitis B reactivation in patients with haematological malignancies: is the serum hepatitis B virus profile reliable? Liver Int. 2009;29:1171–1177. doi: 10.1111/j.1478-3231.2009.02071.x. [DOI] [PubMed] [Google Scholar]
- 39.Hammond SP, Borchelt AM, Ukomadu C, Ho VT, Baden LR, Marty FM. Hepatitis B virus reactivation following allogeneic hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2009;15:1049–1059. doi: 10.1016/j.bbmt.2009.05.001. [DOI] [PubMed] [Google Scholar]
- 40.Pei SN, Chen CH, Lee CM, et al. Reactivation of hepatitis B virus following rituximab-based regimens: a serious complication in both HBsAg-positive and HBsAg-negative patients. Ann Hematol. 2010;89:255–262. doi: 10.1007/s00277-009-0806-7. [DOI] [PubMed] [Google Scholar]
- 41.Francisci D, Falcinelli F, Schiaroli E, et al. Management of hepatitis B virus reactivation in patients with hematological malignancies treated with chemotherapy. Infection. 2010;38:58–61. doi: 10.1007/s15010-009-9019-1. [DOI] [PubMed] [Google Scholar]
- 42.Charpin C, Guis S, Colson P, et al. Safety of TNF-blocking agents in rheumatic patients with serology suggesting past hepatitis B state: results from a cohort of 21 patients. Arthritis Res Ther. 2009;11:R179. doi: 10.1186/ar2868. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Giaccone L, Festuccia M, Marengo A, et al. Hepatitis B virus reactivation and efficacy of prophylaxis with lamivudine in patients undergoing allogeneic stem cell transplantation. Biol Blood Marrow Transplant. 2010;16:809–817. doi: 10.1016/j.bbmt.2009.12.533. [DOI] [PubMed] [Google Scholar]
- 44.Yeo W, Lam KC, Zee B, et al. Hepatitis B reactivation in patients with hepatocellular carcinoma undergoing systemic chemotherapy. Ann Oncol. 2004;15:1661–1666. doi: 10.1093/annonc/mdh430. [DOI] [PubMed] [Google Scholar]
- 45.Targhetta C, Cabras MG, Mamusa AM, Mascia G, Angelucci E. Hepatitis B virus-related liver disease in isolated anti-hepatitis B-core positive lymphoma patients receiving chemo- or chemo-immune therapy. Haematologica. 2008;93:951–952. doi: 10.3324/haematol.12557. [DOI] [PubMed] [Google Scholar]
- 46.Li JM, Wang L, Shen Y, et al. Rituximab in combination with CHOP chemotherapy for the treatment of diffuse large B cell lymphoma in Chinese patients. Ann Hematol. 2007;86:639–645. doi: 10.1007/s00277-007-0320-8. [DOI] [PubMed] [Google Scholar]
- 47.Hui CK, Cheung WW, Zhang HY, et al. Kinetics and risk of de novo hepatitis B infection in HBsAg-negative patients undergoing cytotoxic chemotherapy. Gastroenterology. 2006;131:59–68. doi: 10.1053/j.gastro.2006.04.015. [DOI] [PubMed] [Google Scholar]
- 48.Elkady A, Aboulfotuh S, Ali EM, et al. Incidence and characteristics of HBV reactivation in hematological malignant patients in south Egypt. World J Gastroenterol. 2013;19:6214–6220. doi: 10.3748/wjg.v19.i37.6214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Ramos CA, Saliba RM, de Pádua Silva L, et al. Resolved hepatitis B virus infection is not associated with worse outcome after allogeneic hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2010;16:686–694. doi: 10.1016/j.bbmt.2009.12.532. [DOI] [PubMed] [Google Scholar]
- 50.Laurenti R, Giovannangeli F, Gubinelli E, et al. Long-term safety of anti-TNF adalimumab in HBc antibody-positive psoriatic arthritis patients: a retrospective case series of 8 patients. Clin Dev Immunol. 2013;2013:410521. doi: 10.1155/2013/410521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Ceneli O, Ozkurt ZN, Acar K, et al. Hepatitis B-related events in autologous hematopoietic stem cell transplantation recipients. World J Gastroenterol. 2010;16:1765–1771. doi: 10.3748/wjg.v16.i14.1765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Ye H, Zhang XW, Mu R, et al. Anti-TNF therapy in patients with HBV infection—analysis of 87 patients with inflammatory arthritis. Clin Rheumatol. 2014;33:119–123. doi: 10.1007/s10067-013-2385-1. [DOI] [PubMed] [Google Scholar]
- 53.Hagiwara S, Sakurai T, Nishina S, et al. Characteristic pattern of reactivation of hepatitis B virus during chemotherapy for solid cancers. Dig Dis. 2012;30:541–546. doi: 10.1159/000343056. [DOI] [PubMed] [Google Scholar]
- 54.Masarone M, De Renzo A, La Mura V, et al. Management of the HBV reactivation in isolated HBcAb positive patients affected with Non Hodgkin Lymphoma. BMC Gastroenterol. 2014;14:31. doi: 10.1186/1471-230X-14-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.ViganòM Degasperi E, Aghemo A, Lampertico P, Colombo M. Anti-TNF drugs in patients with hepatitis B or C virus infection: safety and clinical management. Expert Opin Biol Ther. 2012;12:193–207. doi: 10.1517/14712598.2012.646986. [DOI] [PubMed] [Google Scholar]
- 56.Knöll A, Boehm S, Hahn J, Holler E, Jilg W. Long-term surveillance of haematopoietic stem cell recipients with resolved hepatitis B: high risk of viral reactivation even in a recipient with a vaccinated donor. J Viral Hepat. 2007;14:478–483. doi: 10.1111/j.1365-2893.2006.00830.x. [DOI] [PubMed] [Google Scholar]
- 57.Kato M, Atsumi T, Kurita T, et al. Hepatitis B virus reactivation by immunosuppressive therapy in patients with autoimmune diseases: risk analysis in Hepatitis B surface antigen-negative cases. J Rheumatol. 2011;38:2209–2214. doi: 10.3899/jrheum.110289. [DOI] [PubMed] [Google Scholar]
- 58.Navarro R, Concha-Garzón MJ, Castaño C, Casal C, Guiu A, Daudén E. Outcome of patients with serology suggestive of past hepatitis B virus infection during antitumor necrosis factor therapy for psoriasis. Int J Dermatol. 2014;53:909–911. doi: 10.1111/ijd.12313. [DOI] [PubMed] [Google Scholar]
- 59.Nakamura J, Nagashima T, Nagatani K, Yoshio T, Iwamoto M, Minota S. Reactivation of hepatitis B virus in rheumatoid arthritis patients treated with biological disease-modifying antirheumatic drugs. Int J Rheum Dis. 2016;19:470–475. doi: 10.1111/1756-185X.12359. [DOI] [PubMed] [Google Scholar]
- 60.Tamori A, Hino M, Kawamura E, et al. Prospective long-term study of hepatitis B virus reactivation in patients with hematologic malignancy. J Gastroenterol Hepatol. 2014;29:1715–1721. doi: 10.1111/jgh.12604. [DOI] [PubMed] [Google Scholar]
- 61.Nakamoto S, Kanda T, Nakaseko C, et al. Reactivation of hepatitis B virus in hematopoietic stem cell transplant recipients in Japan: efficacy of nucleos(t)ide analogues for prevention and treatment. Int J Mol Sci. 2014;15:21455–21467. doi: 10.3390/ijms151121455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Ballanti E, Conigliaro P, Chimenti MS, et al. Use of anti-tumor necrosis factor alpha therapy in patients with concurrent rheumatoid arthritis and hepatitis B or hepatitis C: a retrospective analysis of 32 patients. Drug Dev Res. 2014;75(Suppl 1):S42–S45. doi: 10.1002/ddr.21193. [DOI] [PubMed] [Google Scholar]
- 63.Barone M, Notarnicola A, Lopalco G, et al. Safety of long-term biologic therapy in rheumatologic patients with a previously resolved hepatitis B viral infection. Hepatology. 2015;62:40–46. doi: 10.1002/hep.27716. [DOI] [PubMed] [Google Scholar]
- 64.Seto WK, Chan TS, Hwang YY, et al. Hepatitis B reactivation in patients with previous hepatitis B virus exposure undergoing rituximab-containing chemotherapy for lymphoma: a prospective study. J Clin Oncol. 2014;32:3736–3743. doi: 10.1200/JCO.2014.56.7081. [DOI] [PubMed] [Google Scholar]
- 65.Oh MJ, Lee HJ. A study of hepatitis B virus reactivation associated with rituximab therapy in real-world clinical practice: a single-center experience. Clin Mol Hepatol. 2013;19:51–59. doi: 10.3350/cmh.2013.19.1.51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Koo YX, Tan DS, Tan IB, Tao M, Chow WC, Lim ST. Hepatitis B virus reactivation and role of antiviral prophylaxis in lymphoma patients with past hepatitis B virus infection who are receiving chemoimmunotherapy. Cancer. 2010;116:115–121. doi: 10.1002/cncr.24742. [DOI] [PubMed] [Google Scholar]
- 67.Mori S. Past hepatitis B virus infection in rheumatoid arthritis patients receiving biological and/or nonbiological disease-modifying antirheumatic drugs. Mod Rheumatol. 2011;21:621–627. doi: 10.1007/s10165-011-0458-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Yağci M, Ozkurt ZN, Yeğin ZA, Aki Z, Sucak GT, Haznedar R. Hepatitus B virus reactivation in HBV-DNA negative and positive patients with hematological malignancies. Hematology. 2010;15:240–244. doi: 10.1179/102453309X12583347114059. [DOI] [PubMed] [Google Scholar]