

Abstract
Background:
Body image, as an important factor in quality of life (QOL) satisfaction, in amputee patients is strongly affected by amputation, which can put the patient at risk of psychological disorders such as depression. Hence, this study was conducted to investigate the effect of spiritual care on body image in patients with type 2 diabetes-related amputation.
Materials and Methods:
In this study, an experimental pretest-posttest design with two groups was used. A total of 54 participants (Males = 41, Females = 13) aged between 40 and 72 who had diabetes-related amputation participated in the study. The participants were randomly assigned to the meditation and control group. For the experimental group, three sessions of meditation, and for control group, three sessions regarding prevention of diabetic foot ulcer were conducted. The participants in the experimental group were asked to perform meditation exercises for a month. The data was collected via Amputee Body Image Scale before and 4 weeks after the intervention.
Results:
There were no significant differences between groups on demographic variables. After intervention, the meditation group showed lower levels of body image disturbance compared with the control group, which was significant (t=3.41, p = 0.001).
Conclusions:
It can be concluded that meditation can improve body image in patients with diabetes-related amputation. In addition, because of no side effects and high acceptance of spiritual care, this method can be used as a way to improve the condition of patients.
Keywords: Amputation, body image, Iran, nursing, spiritual care, type 2 diabetes
Introduction
Diabetes mellitus (DM) is a metabolic disorder [1] which has affected more than 230 million people worldwide.[2] It is one of the disasters of the present century which increases cardiovascular diseases, peripheral vascular diseases, retinopathy, neuropathy, diabetic foot, amputation, and depression.[1] Disorders related to the lower extremities affect nearly one-third of diabetics.[3] Statistics indicate that 50–75% of amputations occur due to diabetes.[1] Amputations are performed on 41.5% of the patients with diabetes in Iran.[4] Lower limb amputation significantly affects the life of individuals; it endangers their body integrity and affects their overall quality of life (QOL). The loss of a part of the body changes ones’ understanding of and feeling towards his/her appearance and body image.[5]
Body image is an important aspect of self-evaluation that has a complex psychological effect on its entire meaning.[6] This is one of the important factors of satisfaction with QOL in patients who have undergone amputations and is strongly influenced by its occurrence.[7,8] Coffey et al. have reported that individuals who have undergone amputations due to diabetes are at a greater risk of developing mental distress.[9] Spiritual health, as a health aspect, has a unique position in Iran;[10] therefore, it can be used as a strategy to improve the body image of patients.
Meditation can also be used as part of spiritual care. It has been considered as one of the most effective methods of relaxation. The sense of relief achieved through meditation not only controls pain, but also increases the ability to deal with physical and psychological problems. Learning this technique is very simple and affordable. Because it does not interfere with an individual's spiritual beliefs and faith, it has a high acceptance rate in the society. In addition, no side effects have been reported for this procedure, and it can be performed at any place and time.[11] According to a study in 2014 by Albertson et al., meditation can improve body image and reduce dissatisfaction with appearance and feeling of shame.[12] Moreover, the results of the study conducted by Hartmann et al. in 2012 indicated the positive influence of meditation on depression, stress, and general health status in patients with type 2 diabetes.[13] However, Boyatzis et al.[14] and Hayman et al.[15] observed no positive correlation between spiritual beliefs and body image. Furthermore, van Son et al. reported that meditation had no effect on the psychological distress associated with diabetes.[16]
Diabetes affects all aspects of life and health of an individual.[17] According to the World Health Organization (WHO), health is defined as a dynamic state of well-being, and physical, mental, social, and spiritual balance, and not merely an absence of disease.[18] Therefore, taking care of individuals with diabetes should be comprehensive and holistic. It is the duty of the medical staff to provide the needs of patients when at risk for depression and body image related disorders.[9] The destruction of the body image in patients who have undergone an amputation is to the extent that even hardware advancement in the field of prosthetics are not able to compensate for the disruptions in the body images of these patients.[19] Considering the conflicting results of studies in this field, this study aimed to evaluate the effect of spiritual care on the body image of patients who have undergone an amputation due to type 2 diabetes.
Materials and Methods
This study was a randomized clinical trial (Registry code: IRCT2014090219015N1). Sample size was calculated according to power analysis with Z1=1.96, Z2=0.84, d=0.80 in patients who had undergone amputations due to type 2 diabetes, who had referred to the rehabilitation centers and clinics of Alzahra Hospital, Isfahan, Iran, in 2014, and who met the inclusion criteria. The inclusion criteria included being older than 18 years, suffering from type 2 diabetes, and having undergone amputation surgery of the fingers, wrist, leg, below the knee, or above the knee. The inclusion criteria also consisted of at least 3 months since the amputation (passing the period of mourning and achieving relative stability); lack of use of other forms of alternative medicine in the past 3 months; being able to speak, read, and write Persian; absence of mental retardation, blindness, deafness, and active mental disease according to patient records; lack of physical limitations for performing the intervention; and having audiovisual facilities to perform the intervention at home. The data collection tool consisted of a two-part questionnaire. The first part contained items related to demographic information including age, gender, marital status, education, and occupation, as well as information on the level and place of the amputation, length of time passed since the amputation surgery, and use or lack of the use of prosthesis. The second part of the questionnaire contained the Amputee Body Image Scale (ABIS).
This questionnaire was designed in 1997 by Breakey et al.[20] to assess the body image of patients who have undergone an amputation. It contains 20 items and is scored based on a 5-point Likert scale from never to always. It has a minimum score of 20 and a maximum score of 100, and higher scores indicate more impairment in relation to body image. In the ABIS, questions 3, 12, and 16 were reversely scored, implying that a higher score in the intended item reflects the absence of impairment in relation to body image. Content validity of the ABIS in amputees was approved by 15 members of the Faculty of Nursing and Midwifery of Isfahan Medical University. To confirm its reliability, the questionnaire was handed to 10 individuals who had undergone lower limb amputation and met the inclusion criteria, and a Cronbach's alpha coefficient of 0.87 was obtained. Among the study population, 60 patients who were eligible for the study and referred to Alzahra Hospital were selected via convenient sampling, and were divided into two groups of 30 using the experimental and control packages. The participants were asked to randomly choose a card from a box with control or experimental written on them, and then, the individuals with the control card were placed in the control group and those with the experimental card were placed in the experimental group.
Before the intervention, the ABIS was completed by participants in both the groups. Then, each group was divided into 3 groups of 10. For each subgroup of 10 participants, 3 transcendental meditation sessions were conducted by a qualified instructor and the researcher. At the end of the sessions, the audio file of the meditation sessions, the content of which was approved by a faculty member and specialist in this field, was played for the patients, and the patients’ correct performance of the transcendental meditation techniques was studied by the researcher and educator. All the participants in the experimental group were provided the audio files of the meditation. They were asked to meditate for 15 minutes every day for 4 weeks in a quiet environment and take notes of their practices in their checklist. The technique used in this study was the transcendental meditation technique. Transcendental meditation does not compromise individuals’ beliefs, but improves their spiritual beliefs.
For transcendental meditation training, first, the conference room of the Sedighe Tahereh Center was chosen, which had a quiet and serene environment. Then, the participants were asked to sit in a comfortable position, leaning against a chair with their feet placed on the ground, and choose a word to calm their mind. They were trained on relaxing and stiffening the muscles and regarding deep breathing and inhaling and exhaling. Then, they were asked to close their eyes during meditation, empty their mind, and bring their thoughts only on the selected word. The participants’ meditation lasted for 15 minutes and was monitored by the researcher and trainer.
In the control group, for each subgroup of 10 individuals, 3 sessions of training courses were organized on diabetes care. Topics covered in the training sessions included foot and diabetic ulcer care with an emphasis on the symptoms and reasons for diabetic foot ulcers, simple and understandable explanation of wound pathophysiology, and principles of foot care and personal hygiene. After the sessions, educational CDs and pamphlets on the prevention of diabetic foot ulcers, approved by the professors, were distributed among the participants. Follow-up was performed for each group by the researcher through phone calls every week. Questions regarding meditation were asked from the participants in the experimental group and regarding foot hygiene in the control group; participants’ questions were also answered. After 4 weeks, all participants, who had completed the care program, completed the ABIS.
Data obtained from the ABIS in the two groups were analyzed using the Statistical Package for the Social Sciences software (version 16, SPSS Inc., Chicago, IL, USA) using descriptive and inferential statistics.
To comply with ethical principles in the present study, an official license was obtained from the Research Ethics Committee of Isfahan University of Medical Sciences, Iran. Written consent forms were also obtained from all participants to conduct the research. The participants were assured of the confidentiality of information received and safety of interventions.
Ethical considerations
The ethical and scientific contents of this study have been approved by research ethics committee of Isfahan University of Medical Sciences. A written and informed consequent was obtained from the patients, and they were free to withdraw from the study at any time.
Results
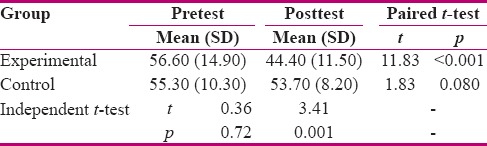
There was no significant difference between the groups regarding underlying characteristics [Table 1]. The mean score of body image before the intervention had no significant difference between the two groups (t = 0.36, p = 0.72). At the end of the 4 weeks, there were 28 patients in the experimental group and 26 patients in the control group. In the experimental group, 2 patients were excluded due to not practicing meditation. In addition, 4 patients were excluded from the control group due to unwillingness to continue participating in the study. Thus, 54 patients were present by the end of the study. After the intervention, the mean and standard deviation of the body image score in the experimental and control groups was 44.40 (11.50) and 53.70 (8.20), respectively. The results showed a significant difference between the two groups (t = 3.41, p = 0.001). Moreover, in the control group, the mean score of body image before and after the intervention were not significantly different (t = 1.83, p = 0.08). Nevertheless, in the experimental group, the mean body image score after the intervention was significantly lower than that before the intervention (t = 11.83, p < 0.001) [Table 2]. The mean changes in the body image score in the control group were not significant, however, in the experimental group, the mean changes in the body image score were significant (p < 0.001, t = 7.81).
Table 1.
Demographic characteristics of the subjects in the experimental and control groups
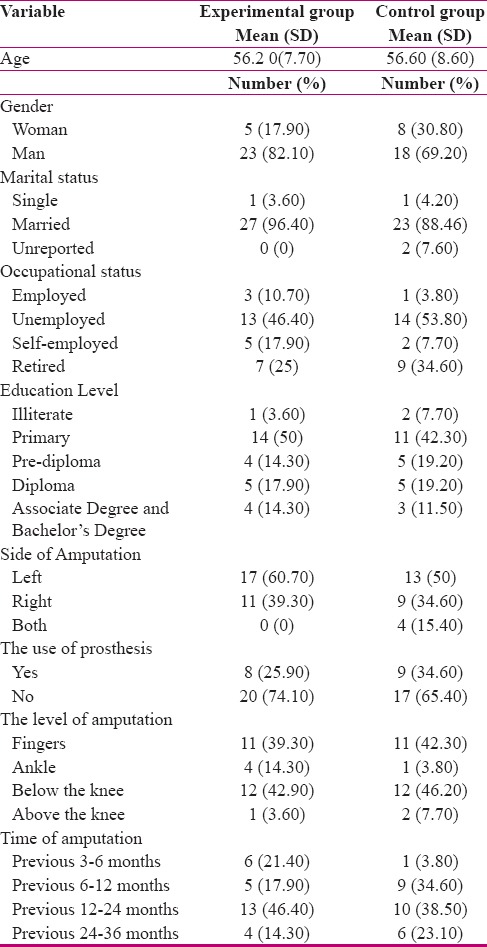
Table 2.
Average score of body image before and after the intervention in the experimental and control groups
Discussion
Because of the emphasis of the WHO on providing holistic and comprehensive care, the number of studies in the field of spiritual care has increased in recent years. The results of these studies showed the impact of these interventions on the physical and mental health of patients with chronic diseases such as diabetes, cancer, and acquired immunodeficiency disease syndrome (AIDS). The evidence showed that spirituality can improve individuals’ body image of their body and assist in acceptance of the changes in their appearance.
The participants of the experimental group were in a better status in terms of their body image after the intervention compared to the control group. The results of the study by Dreger et al.[21] on evaluation of the effect of meditation on the physical and mental health of patients with type 2 diabetes in Canada showed a significant difference (p < 0.05) between the experimental and control groups after the intervention. This finding was in accordance with the results of the present study. In addition, in the study by Alberts et al. in 2014 on women with body image problems, the results indicated the positive impact of meditation on the body images of the studied participants.
Nonetheless, the results of some studies suggested the absence of a positive relationship between body image and spirituality. For example, in assessment studies conducted by Boyatzis et al.[14] and Hayman et al.,[15] no positive relationship was observed between spirituality and body images. Leurent et al.[22] also found that there was no significant relationship between spirituality, religious rituals, and improvement of psychological condition. It appeared that cultural differences and differences in the religious beliefs of the studied population, sample size, and the type of disease were the possible reasons for these contradictions. Furthermore, in the study by Teixeira et al.[23] in 2010 on the effect of meditation on neuropathy pain caused by diabetes, sleep quality, and QOL in patients with diabetes, no significant differences were observed in the scores of QOL (p = 0.22), pain intensity (p = 0.16), and feeling of dissatisfaction (p = 0.96). It appeared that the difference in sample size of this study and the present study was the reason for their conflicting results. The sample size in the mentioned study was almost one-third of the sample size of the present study. This caused the difference in the results and the lack of significant difference between the two groups. Moreover, the differences in the study participants and the nature of the studied variables were other reasons for the different results.
Chan et al. have offered a definition of health.[24] In this definition, health is considered as a dynamic process of achieving higher levels of human well-being in all aspects, including physical, psychological, social, and spiritual aspects. This definition appears in a specific form in nursing because nurses are in constant contact with the patient and can identify and meet their needs in this constant contact. Care is the core of nursing, and caring behaviors encompass both the physical and spiritual aspects. Nurses who practice holistic care should include their spiritual care activities in their interventions. These activities include complementary therapies, presence, active listening, praying, etc. Nursing care may enable the individual to transcend the current condition and understand its meaning and experience relationship with others.[25] Spirituality as a supportive care leads to better acceptance of the changes in appearance and enables patients to easily adapt to the new conditions caused by the disease.[26] The limitations of this study included a shortage of available samples and Lack of prior research studies on the topic.
Conclusion
The results of this study suggested that the emphasis on spirituality and implementation of spiritual care can improve individuals’ body image and their mental condition. Considering the importance and high prevalence of diabetes in Iran, insufficient attention to spiritual care and patients’ psychospiritual needs, time limitation in this study, physical intolerance of the participants in this study to remain in one physical state, and thus, reduction of the number and duration of training sessions, implementation of further researches in more favorable conditions in patients with diabetes is necessary.
Financial support and sponsorship
Isfahan University of Medical Sciences, Isfahan, Iran.
Conflicts of interest
Nothing to declare.
Acknowledgments
This study is part of a research project in the Nursing and Midwifery Care Center of Isfahan University of Medical Sciences with the code 393479. We would like to thank all the staff and personnel of the Alzahra hospital of Isfahan, especially its management who truly cooperated with us during this research.
References
- 1.Smeltzer S, Boyer MJ. Study Guide for Brunner and Suddarth's Textbook of Medical-surgical Nursing. 12th ed. Wolters Kluwer Health; 2009. [Google Scholar]
- 2.Abdoli S, Ashktorab T, Ahmadi FA, Parvizi S. Diabetes diagnosis: Identity break. Iran J Endocrinol Metab. 2011;13:26–35. [Google Scholar]
- 3.Frykberg RG, Zgonis T, Armstrong DG, Driver VR, Giurini JM, Kravitz SR, et al. Diabetic foot disorders: A clinical practice guideline (2006 revision) J Foot Ankle Surg. 2006;45:S1–S66. doi: 10.1016/S1067-2516(07)60001-5. [DOI] [PubMed] [Google Scholar]
- 4.Tabatabaei Malazi A, Mohajerani Tehrani M, Pajouhi M, Larijani B. The performance report of diabetes foot research team. J Diabetes Metab Disord. 2008;8 [Google Scholar]
- 5.Holzer LA, Sevelda F, Fraberger G, Bluder O, Kickinger W, Holzer G. Body image and self-esteem in lower-limb amputees. PLoS One. 2014;9:e92943. doi: 10.1371/journal.pone.0092943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Srivastava K and Chaudhury S. Rehabilitation after Amputation: Psychotherapeutic Intervention Module in Indian Scenario. ScientificWorldJournal 2014. 2014:469385. doi: 10.1155/2014/469385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Akkaya N, Atalay NŞ, Selcuk ST, Akkaya S, Ardıç F. Impact of body image on quality of life and mood in mastectomized patients and amputees in Turkey. Asian Pac J Cancer Prev. 2011;12:2669–73. [PubMed] [Google Scholar]
- 8.Zidarov D, Swaine B, Gauthier-Gagnon C. Quality of life of persons with lower-limb amputation during rehabilitation and at 3-month follow-up. Arch Phys Med Rehabil. 2009;90:634–45. doi: 10.1016/j.apmr.2008.11.003. [DOI] [PubMed] [Google Scholar]
- 9.Coffey L, Gallagher P, Horgan O, Desmond D, MacLachlan M. Psychosocial adjustment to diabetes-related lower limb vamputation. Diabetic Med. 2009;26:1063–7. doi: 10.1111/j.1464-5491.2009.02802.x. [DOI] [PubMed] [Google Scholar]
- 10.Salehi SA, Ghodousi and Ojaghloo K. The spiritual experiences of patients with diabetes-related limb amputation. Iran J Nurs Midwifery Res. 2012;17 [PMC free article] [PubMed] [Google Scholar]
- 11.Golian Tehrani Sh, Vasegh Rahimpour F, Mehran A, Nikkhah A. The effect of meditation on pain and length of labor in nulliparous women. J Nurs Midwifery Tehran Univ Med Sci. 2006;12:51–61. [Google Scholar]
- 12.Albertson ER, Neff KD, Dill-Shackleford KE. Mindfulness. 2015;6:444. Doi:101007/s12671-014-0277-3. [Google Scholar]
- 13.Hartmann M, Kopf S, Kircher C, Faude-Lang V, Djuric Z, Augstein F, et al. Sustained effects of a mindfulness-based stress-reduction intervention in type 2 diabetic patients design and first results of a randomized controlled trial (the Heidelberger Diabetes and Stress-Study) Diabetes Care. 2012;35:945–7. doi: 10.2337/dc11-1343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Boyatzis CJ, Trevino KM, Manning AE, Quinlan KB. The role of religion and spirituality in women's body image and eating behavior: Qualitative and quantitative approaches and clinical implications. Counseling Spiritualité. 2006;25:29–51. [Google Scholar]
- 15.Hayman JW, Kurpius SR, Befort C, Nicpon MF, Hull-Blanks E, Sollenberger S, et al. Spirituality Among College Freshmen: Relationships to Self-Esteem, Body Image, and Stress. Counsel Values. 2007;52:55–70. [Google Scholar]
- 16.van Son J, Nyklíček I, Pop VJ, Blonk MC, Erdtsieck RJ, Spooren PF, et al. The Effects of a Mindfulness-Based Intervention on Emotional Distress, Quality of Life, and HbA1c in Outpatients With Diabetes (DiaMind): A randomized controlled trial. Diabetes Care. 2013;36:823–30. doi: 10.2337/dc12-1477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Tal A, Majlesi F, Rahimi Forushani A, Shojaeizade D, Mohebbi B. Check protectionist barriers and Living with diabetes and risk factors in type 2 diabetic patients referred to hospitals affiliated to Tehran University of Medical Sciences. J Health Syst Res. 2013;8:1088–97. [Google Scholar]
- 18.WHO. Noncommunicable diseases. [Last accessed September 2012]. Available from: http://www.who.int/nmh/countries/irn_en.pdf_ua=1.
- 19.Washington J. The Relations among Psychological and Demographic Factors in Individuals with Lower Limb Amputation. Senior Theses, Trinity College, Hartford, CT 2013. Trinity College Digital Repository. http://digitalrepository.trincoll.edu/theses/337.
- 20.Breakey JW. Body image: The lower-limb amputee. J Prosthet Orthot. 1997;9:58–66. [Google Scholar]
- 21.Dreger LC, Mackenzie C, McLeod B. Feasibility of a Mindfulness-Based Intervention for Aboriginal Adults with Type 2 Diabetes. Mindfulness. 2013:1–17. [Google Scholar]
- 22.Leurent B, Nazareth I, Bellón-Saameño J, Geerlings MI, Maaroos H, Saldivia S, et al. Spiritual and religious beliefs as risk factors for the onset of major depression: An international cohort study. Psychol Med. 2013;43:2109–20. doi: 10.1017/S0033291712003066. [DOI] [PubMed] [Google Scholar]
- 23.Teixeira E. The effect of mindfulness meditation on painful diabetic peripheral neuropathy in adults older than 50 years. Holistic Nurs Pract. 2010;24:277–83. doi: 10.1097/HNP.0b013e3181f1add2. [DOI] [PubMed] [Google Scholar]
- 24.Chan ML, Chung A, Lee W, Wong G, Lee C, Lau W, et al. Investigating spiritual care perceptions and practice patterns in Hong Kong nurses: Results of a cluster analysis. Nurse Educ Today. 2006;26:139–50. doi: 10.1016/j.nedt.2005.08.006. [DOI] [PubMed] [Google Scholar]
- 25.Cavendish R, Konecny L, Naradovy L, Luise BK, Como J, Okumakpeyi P, et al. Patients’ perceptions of spirituality and the nurse as a spiritual care provider. Holistic Nurs Pract. 2006;20:41–7. doi: 10.1097/00004650-200601000-00010. [DOI] [PubMed] [Google Scholar]
- 26.Kalra SG, Sridhar Y, Balhara RK, Sahay G, Bantwal MP, Baruah M, et al. National recommendations: Psychosocial management of diabetes in India. Indian J Endocrinol Metab. 2013;17:376. doi: 10.4103/2230-8210.111608. [DOI] [PMC free article] [PubMed] [Google Scholar]