

Abstract
Introduction:
This review provides a national summary of what is currently known about the Canadian opioid crisis with respect to opioid-related deaths and harms and potential risk factors as of December 2017.
Methods:
We reviewed all public-facing opioid-related surveillance or epidemiological reports published by provincial and territorial ministries of health and chief coroners’ or medical examiners’ offices. In addition, we reviewed publications from federal partners and reports and articles published prior to December 2017. We synthesized the evidence by comparing provincial and territorial opioid-related mortality and morbidity rates with the national rates to look for regional trends.
Results:
The opioid crisis has affected every region of the country, although some jurisdictions have been impacted more than others. As of 2016, apparent opioid-related deaths and hospitalization rates were highest in the western provinces of British Columbia and Alberta and in both Yukon and the Northwest Territories. Nationally, most apparent opioid-related deaths occurred among males; individuals between 30 and 39 years of age accounted for the greatest proportion. Current evidence suggests regional age and sex differences with respect to health outcomes, especially when synthetic opioids are involved. However, differences between data collection methods and reporting requirements may impact the interpretation and comparability of reported data.
Conclusion:
This report identifies gaps in evidence and areas for further investigation to improve our understanding of the national opioid crisis. The Public Health Agency of Canada will continue to work closely with the provinces, territories and national partners to further refine and standardize national data collection, conduct special studies and expand information-sharing to improve the evidence needed to inform public health action and prevent opioid-related deaths and harms.
Keywords: opioid, overdose, crisis, harms, deaths, fentanyl, Canada
Highlights
The opioid crisis is growing in Canada, driven by both illegal and prescription opioid use. Fentanyl and analogues appear to be fuelling the rise in opioid-related deaths.
This crisis is having a devastating impact on the health and lives of Canadians, their families and communities across the country. In 2016 alone, there were 2861 opioidrelated deaths and 16 opioid-related hospitalizations each day.
While the opioid crisis has affected every region of the country, western Canada (British Columbia and Alberta) and the northern territories (Yukon and Northwest Territories) have experienced the highest burden.
Nationally, most apparent opioidrelated deaths occurred among males (74%); individuals between 30 and 39 years of age accounted for the greatest proportion (28%).
Evidence reveals that this crisis is not restricted to opioids; 82% of apparent opioid-related deaths from January 2016 to June 2017 also involved one or more non-opioid substances.
Introduction
The opioid crisis is growing in Canada, driven by both illegal and prescription opioids. In 2016, there were 2861 apparent opioid-related deaths* in Canada, which is equivalent to eight people dying each day,1 and is greater than the average number of Canadians killed daily in motor vehicle collisions in 2015.2 However, this statistic represents just the tip of the iceberg; on average, 16 Canadians were hospitalized each day due to opioid-related poisonings in Canada in 2016.3 This is not a problem restricted to persons who use illegal or street drugs; rather, this is a national public health crisis that affects people in communities across Canada, across all ages and across all socioeconomic groups.
An apparent opioid-related death (AORD) is “a death caused by intoxication/toxicity (poisoning) as a result of drug use, where one or more of the drugs involved is an opioid.”1
Methods
The purpose of this review was to provide a summary of the existing body of evidence on the Canadian opioid crisis, based on available data, to assist with identifying trends and gaps in knowledge and to provide policy makers with a national perspective. In order to better understand the crisis and its impact on Canadians across the country, we reviewed all public-facing, opioid-related surveillance and epidemiological reports published by provincial and territorial ministries of health and chief coroners’ and medical examiners’ offices. In addition, we reviewed available reports and published articles from federal partners and external organizations mentioning opioid-related harms, opioids, opiates, fentanyl, fentanyl analogues or synthetic opioids published or shared prior to December 2017. We synthesized the data by comparing provincial and territorial historical opioid-related mortality and morbidity trends (where available), and by comparing current provincial and territorial rates with the national rates to identify regional trends and differences. Information collected through bilateral discussions with the provinces and territories on opioid-related health outcomes and data from Health Canada on prescribing practices and analysis of seized drug shipments were included to provide the context for the national synthesis.
At the time of this review, all provinces and territories were reporting opioidrelated mortality data to the Public Health Agency of Canada (PHAC) through the Opioid Overdose Surveillance Task Group (OOSTG). The OOSTG includes federal, provincial and territorial (FPT) partners, as well as other national partners. The OOSTG is responsible for coordinating national surveillance of opioid-related harms, including the development of national case definitions (such as “apparent opioid-related deaths”).
Individually, six provinces had reported historical data on opioid-related mortality. Eight provinces had published reports on the opioid crisis, with all reporting on mortality; four reported data from emergency medical services (EMS) or first responders; and four reported data on communitybased naloxone distribution programs. Three of the provinces included analysis of potential risk factors in their published reports. The information from these reports forms the basis of this synthesis.
Results
Prescription opioids: use, supply and access
The current opioid epidemic follows on the enormous growth in use of prescription opioids in Canada in recent decades. Since the early 1980s, the volume of opioids sold to hospitals and pharmacies for prescriptions in Canada has increased by more than 3000%.4 In 2016, over 20 million prescriptions for opioids were dispensed, 5 which is equivalent to nearly one prescription for every adult over the age of 18 years, making Canada the second-largest consumer of prescription opioids in the world, after the USA.6
In Canada, prescription opioid–related harms and rates of nonmedical prescription opioid use (“misuse”) have been increasing since 1999.6 According to estimates, by 2008 nonmedical prescription opioid use was the fourth most prevalent form of substance use (after alcohol, tobacco and cannabis), making it more common to misuse a prescription opioid than to use heroin or cocaine.7
The prevalence of prescription opioid use in Canada (“within the previous 12 months”) is estimated to be one in six (from the 2015 Canadian Tobacco, Alcohol and Drugs Survey [CTADS]).8 While the CTADS found just 2% of those who used a prescription opioid reported misusing them, a more recent online survey from Health Canada (2017) found that nearly one-third of those who had used an opioid in the past year did not always have a prescription. This proportion increased to almost half in teens younger than 18 years and 88% among persons using illegal drugs.9
There are many routes that allow for prescription opioids to be diverted for nonmedical use, including sharing with family members, “double doctoring,” prescription fraud and forgery, street drug markets, thefts and robberies and Internet purchases, making it difficult to estimate the proportion diverted.7 Through its surveys, Health Canada found that the most common source of opioids used without a prescription was a family member.9
No national measures of prevalence of illegal opioid use were found. Nationally, in 2015 the prevalence of illicit drug use (“within the previous 12 months”) was 2% (1% females; 3% males). This included use of crack, cocaine, ecstasy, speed or methamphetamines, hallucinogens or heroin and therefore was not specific to opioids.8
The rising presence of fentanyl and other synthetic opioids: evidence from illegal drug seizures and death investigations
In 2016, opioids were among the top 10 controlled substances most frequently detected by Health Canada’s Drug Analysis Service (DAS), ranking just below marijuana, cocaine and methamphetamines among all samples tested from substances confiscated by police and border security from across the country. Heroin, fentanyl and its analogues, hydromorphone, oxycodone and morphine were the most frequently detected opioids in samples analyzed by DAS.10
Synthetic opioids such as fentanyl, W-18 and U-47700, to name but a few, are extremely potent. Fentanyl and its analogues (e.g. carfentanil, furanylfentanyl, acetylfentanyl) are becoming more prevalent on the illegal drug market and are increasingly combined with other controlled substances, which increases their potential toxicity and the risk of an overdose. In 2017, Health Canada found fentanyl or an analogue in more than 50% of heroin samples tested by DAS (tested between January 2012 and September 2017), and has also started to detect it in samples of methamphetamines and cocaine (2% each).11 A review of available literature found that fentanyl was first reported in British Columbia and Alberta in 2011.12,13 Since then, the proportion of deaths involving fentanyl in these provinces has risen dramatically.12,13
The pattern of apparent opioid-related deaths is changing along with the increasing presence of synthetic opioids in the illegal market. Fentanyl has now been detected in the illegal drug supply in all Canadian jurisdictions.10,14Nationally, the proportion of reported apparent opioidrelated deaths involving fentanyl or an analogue was 53% in 20161 and appears to be on the rise, according to preliminary reports for 2017.
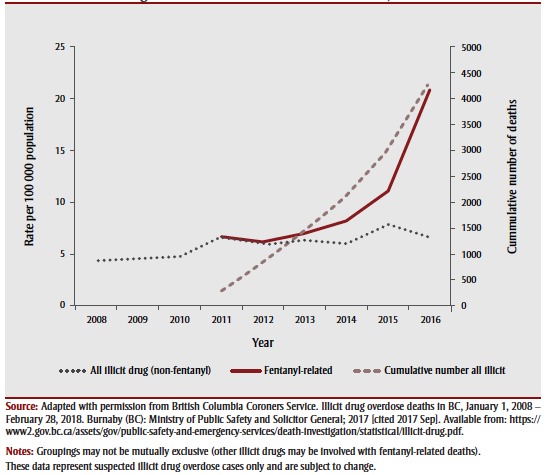
In British Columbia, fentanyl was involved in 68%1 of the 985 illicit drug deaths† in 2016, up from 4% in 2012.12,15 During the first half of 2017, the proportion of deaths involving fentanyl or an analogue in the province rose to 83%.1 In contrast, the number of illicit drug overdose deaths not involving fentanyl has remained relatively stable, at 300 per year15 (Figure 1).
Figure 1. Illicit drug overdose death rates in British Columbia, 2008–2016.
In Alberta, there were 611 apparent opioid- related deaths in 2016.1,16 From 2014 to 2016, the proportion of deaths involving fentanyl or an analogue increased from 26% to 63%,16 while deaths due to other opioids remained constant and non-opioidrelated overdose deaths declined by almost 200%.16 This trend continued during the first six months of 2017 in Alberta, with the proportion of opioid-related overdose deaths involving fentanyl or an analogue rising to almost 80%.1,16
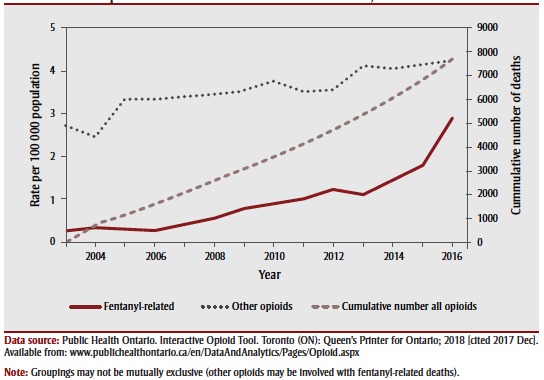
Ontario has also reported a rising proportion of fentanyl-related deaths.1,17 In 2016, there were 867 apparent opioid-related deaths. From 2012 to 2016, the proportion of deaths involving fentanyl increased from 26% to 41%17 (Figure 2).
Figure 2. Opioid-related overdose death rates in Ontario, 2003–2016.
Carfentanil, which is 100 times more powerful than fentanyl, presents another growing concern and has been detected in British Columbia,15,18 Alberta,16 Manitoba19and Ontario.17 In 2016/17, DAS tested 91 seized samples of carfentanil: 56% from British Columbia, 17% from Alberta, 19% from Manitoba and 7% from Ontario.20 In Alberta, there were 29 deaths in 2016 involving carfentanil, and in the first six months of 2017 there were at least 89 deaths.16
Health outcomes: apparent opioid-related deaths
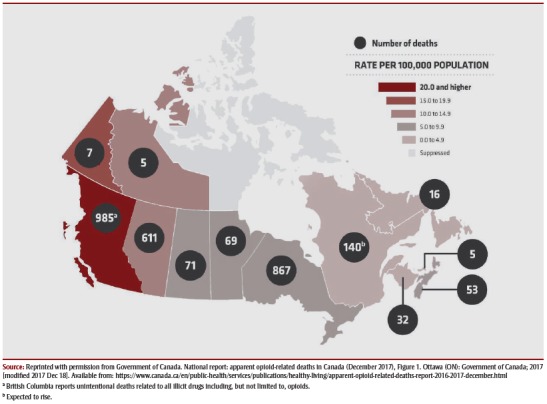
By 2016, apparent opioid-related death rates revealed a national public health crisis. The opioid epidemic had affected communities across the country (Figure 3). Nationally, the rate of apparent opioidrelated deaths was 7.9 per 100 000 population in 2016.1 However, there were pronounced regional differences, with western provinces reporting some of the highest death rates: British Columbia reported a rate of 20.7 per 100 000 population (985 illicit drug overdose deaths) and Alberta reported a rate of 14.4 per 100 000 population (611 opioid-related overdose deaths). Based on available data, these two provinces alone accounted for the majority (56%) of opioid-related deaths in 2016.1 Yukon and the Northwest Territories also reported high rates of 18.4 and 11.2 per 100 000 population, respectively.1 Rates for apparent opioid-related deaths were relatively lower in the other jurisdictions, but suggest a possible rise in some provinces, including Ontario.1,17,19,21,22
Figure 3. Apparent opioid-related death rates (per 100 000 population) by province or territory, Canada, 2016.
Age and sex
In 2016, the highest percentage (28%) of apparent opioid-related deaths in Canada occurred among individuals between the ages of 30 and 39.1 Though age at death does not appear to vary greatly across jurisdictions, age may be a factor when the type of opioid is considered. In Alberta, when fentanyl and its analogues were involved, younger men represented more deaths (mean age: 38 years) as compared to deaths involving other opioids (mean age: 42 years).16
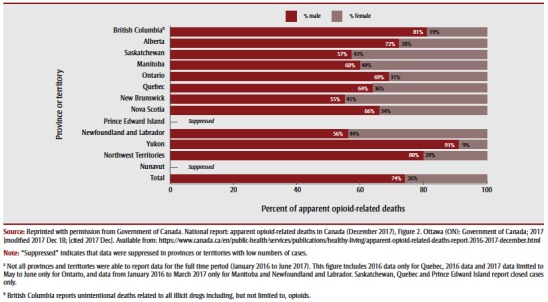
From January 2016 to June 2017, most apparent opioid-related deaths in the nation occurred among males (74%). However, information collected from the provinces and territories indicates that the sex of individuals dying from an apparent opioid-related overdose may vary by region. In the western jurisdictions of British Columbia, Alberta, Yukon and the Northwest Territories, more men are dying than women (approximately 4:1); in Ontario, men are also more likely to die than women (2:1). However, in some Prairie and eastern provinces (Saskatchewan, Manitoba, New Brunswick, Nova Scotia and Newfoundland and Labrador), women represent nearly as many opioid-related deaths as do men (1:1 to 3:2)1 (Figure 4).
Figure 4. Sex distribution of apparent opioid-related deaths by province or territory, Canada, January 2016 to June 2017a.
In some jurisdictions there appear to be other important variations by age and sex. In Alberta and Ontario, where data segregated by age and sex were presented, older women (aged 44 years and older) represented more deaths from an opioidrelated overdose than their younger male counterparts.16,17 This pattern was also reflected in recent studies of registered First Nations in British Columbia and Alberta, where First Nations women dying of an opioid-related overdose were on average 15 to 20 years older than their male counterparts.23,24
These differences in death rates may reflect some jurisdictional differences in the death investigation process, death classification method, toxicology testing or type of data reported (e.g. the inclusion or exclusion of suicide deaths) and thus caution should be used when interpreting these numbers.
Risk factors for apparent opioid-related deaths
Several reports published by the provinces also looked at risk factors. The reports we reviewed from British Columbia, Alberta and Manitoba showed that the majority of opioid-related overdose deaths occurred indoors, in private residences, in larger urban centres, though many deaths also occurred on the periphery of these urban centres and in a large number of smaller communities as well.15,16,18,19 In Alberta and Ontario, those who died tended to reside in lowerto middle-income neighbourhoods; however, deaths occurred in neighbourhoods across all socioeconomic groups.16,25
Combined use of opioids with non-opioid substances, such as alcohol, benzodiazepines, cocaine and W‑18, to name a few, may also be a risk factor. According to available data, approximately 82% of apparent opioid-related deaths from January 2016 to June 2017 also involved one or more non-opioid substances.1
Previous access to certain prescribed medications was also analyzed by three provinces. In Manitoba, a chart review performed by the Office of the Chief Medical Examiner found the most frequently prescribed medications, six months prior to an apparent opioid-related death, were an opioid (60%), an antidepressant (52%) and a benzodiazepine (47%).19
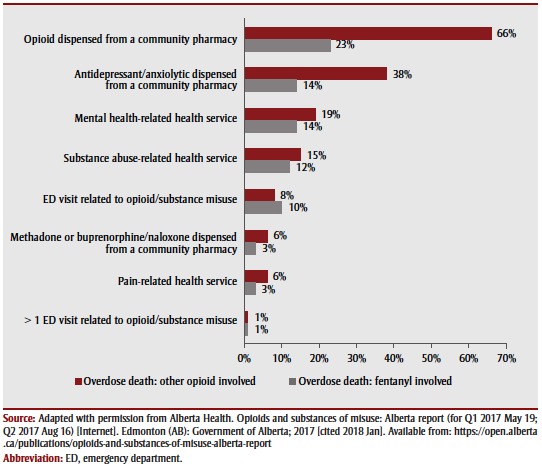
The Alberta report also found differences in the proportions of deaths from an opioid- related overdose involving an opioid other than fentanyl, and deaths in which fentanyl was involved. Specifically, individuals who died of an opioid-related overdose involving an opioid other than fentanyl were nearly twice as likely to have accessed a (listed) health care service (77% vs. 41%),16 or to have been dispensed an opioid (66% vs. 23%) or antidepressant (38% vs. 14%) from a community pharmacy in the 30 days prior to their death (Figure 5). This suggests that there may be differences in the risk factors for opioid-related deaths when fentanyl is involved and those involving other opioids.
Figure 5. Proportion of apparent opioid-related accidental toxicity deaths by medical history within 30 days before death, January 1–September 30, 2017, Alberta, Canada.
Special populations
First Nations‡ populations across the country are heavily impacted by high rates of problematic substance use.26 As early as 2014, First Nations communities were raising the alarm about the number of opioidrelated overdose deaths on reserves in southern Alberta.27 The provinces of British Columbia and Alberta published reports highlighting the impact of the opioid crisis on First Nations communities from January 2016 to March 2017. Both reported similar findings: First Nations people were five times more likely than their non–First Nations counterparts to experience an opioid- related overdose event and three times more likely to die from an opioid-related overdose.23,24 In Alberta, fentanyl was involved in 18% more opioid-related deaths among First Nations people than non–First Nations.23 No distinction for type of opioid involved was available from the British Columbia report.
In both provinces, First Nations men and women were almost equally likely to experience an opioid-related overdose event.23,24 In Alberta, First Nations men and women were also equally likely to die from an opioid-related overdose, while in British Columbia, First Nations males were more likely to die than females (5:3) from an opioid-related overdose. In both provinces, First Nations women were more likely to die than non–First Nations women, who represented less than 30% of non–First Nations deaths.1 In both British Columbia and Alberta, older First Nations women (aged 50 to 54 years) represented a higher proportion of all opioidrelated deaths in both provinces, whereas First Nations men were younger (30 to 34 years),23,24 which is in keeping with apparent opioid-related death rates for men in the general Canadian population.1
Alberta’s report also examined hospitalizations and emergency department (ED) visits. In Alberta, First Nations individuals were five times more likely than non–First Nations people to be hospitalized and six times more likely to present at an ED for an opioid poisoning. First Nations people were also twice as likely to be dispensed an opioid as non–First Nations individuals, and tended to be at least five years younger at the time the drug was dispensed than non–First Nations individuals. 23 Because information from First Nations and other ethnic populations are not readily available in other jurisdictions, regional comparisons were not possible at this time.
Homeless populations are also at risk of opioid-related harms. In British Columbia, data collected in EDs found that unstable housing (i.e. no fixed address or unknown address) was reported by approximately 30% of those presenting for a known or suspected overdose, and by almost 50% of young people aged 13 to 18 years.12
Another at-risk population resides in provincial and territorial prisons and federal penitentiaries. These institutions house populations with a high prevalence of problematic substance use. From 2011/12 to 2013/14, Correctional Service Canada reported 92 unintentional overdose events, 12% of which were fatal. In 2014/15, there were 6 fatal overdoses (13.5 per 100 000 population). Male inmates with a reported prior substance use problem were most likely to overdose. Illegally obtained (as opposed to prescription) drugs were most commonly linked with fatal overdoses.28
Health outcomes: hospitalizations
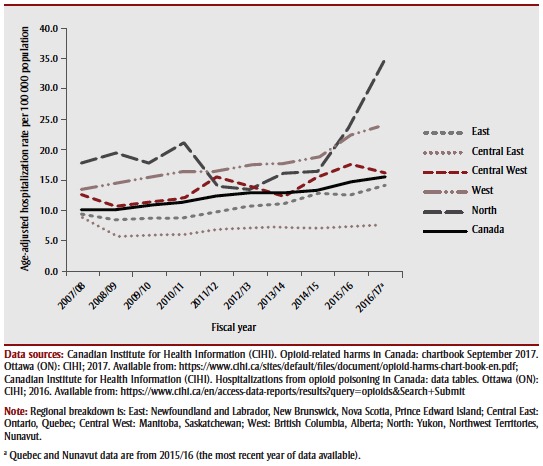
Hospitals use the term opioid poisoning to describe an opioid-related overdose, according to International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10-CAii) version 2015 coding.§ The Canadian Institute for Health Information (CIHI) extracts data from the Hospital Morbidity Database (HMDB) for hospitalizations (100% national reporting). From March 2016 to March 2017, opioid poisonings were responsible for an average of 16 hospitalizations per day in Canada. This represents an increase of over 50% nationally in the past 10 years, with the largest increases occurring in the past three years.3 Adults aged 45 years and older had the highest rates of hospitalization for opioid poisonings, although the fastest growing rates were seen in the younger age groups (15 to 44 years). Rates varied across the country. The highest rates for opioid-related hospitalizations (in 2016/17) as well as the fastest growing rates (occurring between 2014 and 2017) were in the western provinces of British Columbia (25.0 per 100 000 population) and Alberta (23.1 per 100 000 population) and in the territories (34.5 per 100 000 population) excluding Nunavut3 (Figure 6). In 2016/17, more than half of the hospitalizations for opioid poisonings were considered unintentional, 31% were considered intentional and 17% were of unknown intent.3 The majority (63%) of the unintentional poisonings occurred in people aged 65 years and older while intentional poisonings were more prevalent in the younger age group of 15 to 24 years.3 Nationally, hospitalization rates have increased by 24% over the past three years for men and 10% for women. In 2016/17, the rate of hospitalization of males surpassed that of females for the first time.3 There did not appear to be notable regional differences with respect to age or sex for opioid-related hospitalizations.25
Figure 6. Age-standardized rates per 100 000 population for significant opioid-poisoning hospitalizations in Canada, by region and fiscal year, 2007/08 to 2016/17.
Health outcomes: emergency department (ED) visits
Data are collected by EDs and reported to CIHI to the National Ambulatory Care Reporting System (NACRS) (64% national coverage; 100% coverage in ON, AB, YK)3 using ICD10-CAii version 2015 coding. As these data are not nationally representative, where possible they have been supplemented by surveillance reports from provinces where available. In light of these different data sources, regional comparisons are not possible for ED visits.
In Alberta, over the past five years, opioid- related ED visits have more than doubled, reaching 88.6 per 100 000 population in 2016/17. Contributing to this increase, heroin and synthetic opioid (including fentanyl) poisonings rose nearly tenfold each to approximately 20 per 100 000 population (for both) in 2016/17. During this same time period, opioid-related ED visits tripled for males and almost doubled for females. The greatest increases were observed in the younger age groups (15 to 44 years), for which rates have tripled, reaching more than 150 per 100 000. Most of these increases have occurred over the past three years.3
In Ontario, over the past five years, opioid- related ED visits increased by almost 50%. More specifically, ED visits for heroin rose fourfold to 5.7 per 100 000 population and more than doubled for synthetic opioid poisonings (including fentanyl), reaching 5.5 per 100 000 population in 2016/17. Rates have increased by 65% among males and 30% among females. The increases were greatest in the younger age groups (25 to 44 years), where rates almost doubled, reaching 57 per 100 000 population in 2016/17. Again, these increases mostly occurred over the past three years.3
In British Columbia, males made up 66% of ED visits for suspected opioid overdoses. Nearly two-thirds of the patients were aged 20 to 39 years, and most ED visits occurred in larger urban centres. (This information was reported from 47 EDs in three regional health authorities between June 2016 and March 2017).12
In Manitoba, over the past five years, agestandardized ED admission rates for the Winnipeg Regional Health Authority have remained stable. In 2016, females represented 65% of all ED visits for suspected opioid overdoses; over half of them were younger than 24 years.19
Health outcomes: emergency medical services (EMS), first responders and 911 calls
Information from EMS and first responders is collected in most provinces and territories at either the provincial/territorial level or, as in Ontario and Quebec, within municipalities.29 This is a rich data source that may provide a glimpse into overdoses in communities. British Columbia, Alberta and Manitoba have analyzed and reported on these data, while other jurisdictions and municipalities are collecting and sharing EMS data with their respective health departments.
In British Columbia, during 2016, the estimated rate of illicit drug overdoses attended by paramedics was 190 per 100 000, which means that for every illicit drug overdose death in the province, paramedics responded to almost 10 overdose events. With the emergence of fentanyl into the illegal drug supply, the severity of overdose events where naloxone is administered has been increasing along with the number of repeat overdoses in both sexes.12
In Alberta, during 2016, EMS responded to over 1600 opioid-related events, which means that for every apparent opioidrelated death in the province, EMS responded to almost three opioid-related overdose events. Eighty percent of these events occurred in the non-central urban cores of Edmonton and Calgary.16
In Manitoba, between 2015 and 2016, EMS calls for opioid-related events increased by 70%. The majority of cases were males aged 20 to 29 years; females were on average substantially older (≥ 50 years). Of the suspected overdose events attended by EMS, 18% were never transported to an ED or a hospital.19
Health outcomes: Community-based naloxone distribution and use
Additional information on opioid-related harms and overdoses occurring in communities may come from monitoring the distribution and use of naloxone takehome kits (“kits”) in communities and from data collected at supervised injection sites and overdose prevention sites (BC). Kit distribution and use are currently being monitored in approximately half of the provinces and territories by collecting information on opioid-related overdose events reported when used kits are replaced.29 Currently, British Columbia, Alberta and Manitoba report on the numbers of kits distributed and used in communities and provide some information on overdose events. In British Columbia, from August 2012 to June 26, 2017, 459 303 kits were distributed and 10 000 were reported used to reverse an overdose on self or other.30 Between January 1, 2016, and June 30, 2017, 18 852 kits were dispensed in Alberta and 1707 overdoseevent reversals were reported.16 Between December 29, 2016, and March 31, 2017, 258 kits were distributed across Manitoba and 30 kits were reported used during overdose events.19 Because information collected on kit use is not consistently reported across the country, regional comparisons were not possible at this time.
British Columbia reports on all illicit drug overdoses and deaths, including but not limited to opioids, and includes “street drugs” (both controlled and illegal drugs); “medications not prescribed to the decedent but obtained/purchased on the street, from unknown means or where the origin of the drug [was] not known”; and combinations of the previous two with prescribed medications.15,p.1
The reports cited in this section for First Nations populations concerned individuals self-identifying as First Nations and did not include data on Métis or Inuit.
ICD-10-CAii version 2015 codes used to identify opioid poisonings that resulted in hospitalizations and ED visits (T40.0–T40.4, and T40.6) (excluding “suspected” diagnosis). Hospitalizations and ED visits were categorized as: accidental (X42), intentional (X62) and unknown (Y12 and “missing data”). This analysis was limited to “significant opioid poisonings,” using the diagnosis types M, 1, 2, 6, W, X and Y.3
Discussion
The objective of this review was to synthesize the published evidence to describe the epidemic of opioid-related harms occurring in Canada. The current body of evidence points to a national opioid crisis— no region is unaffected by opioids; however, there are notable regional differences. In 2016, rates of apparent opioidrelated deaths and hospitalization were highest in the western provinces of British Columbia and Alberta and in both Yukon and the Northwest Territories; preliminary data from 2017 suggest that rates are continuing to climb in parts of the country. Nationally, most apparent opioid-related deaths occurred among males; individuals between 30 and 39 years of age accounted for the greatest proportion. While there did not appear to be regional differences with respect to age and sex for opioidrelated hospitalizations and ED visits, increasing rates in the younger age groups are a source of concern.
Prescription opioid use appears to be an early driver of the current crisis. However, the increasing toxicity of substances on the illegal market is likely driving the recent rise in deaths in many Canadian jurisdictions. As of September 2016, fentanyl was detected in the illegal drug supply in all Canadian jurisdictions and is increasingly being detected in other illegal drugs as well. The impact of this trend in the illegal market can be observed in available data on health outcomes. In 2016, the proportion of reported apparent opioid-related deaths involving fentanyl or an analogue was 53% nationally, and this trend appears to be continuing in 2017. In both British Columbia and Alberta, the provinces hardest hit by this crisis to date, it has become more and more evident that illegally manufactured fentanyl and its analogues are responsible for the observed increases in drug overdose deaths. Dr. Perry Kendall, the former Provincial Health Officer for British Columbia who was at the forefront of the crisis, summed up the evolving situation concisely: “If we’ve got fentanyl and carfentanil now replacing heroin and other safer opioids on the streets, then this might be the new normal in terms of danger and a toxic drug supply.”31
Initial analysis of potential risk factors found the majority of opioid-related deaths occurred when the individual was alone, indoors in a private residence located in a larger urban centre; those who died tended to reside in lower- to middle-income neighbourhoods; and more than 80% of deaths involved one or more non-opioid substances. The first reports focusing on First Nations communities in western Canada confirmed that First Nations people are more likely than their non–First Nations counterparts to experience and die from an opioid-related overdose event, especially First Nations women. Other at-risk communities appear to be individuals with unstable or unknown housing status and incarcerated populations. Additional research is necessary to understand underlying risk factors and the effect of health issues such as mental health on health outcomes.
Available data from first responders, EMS, supervised injections sites and harm reduction agencies were not sufficient to make regional comparisons on opioid-related overdoses occurring in communities at this time. However, preliminary information from EMS and community-based kit distribution and use monitoring programs are beginning to reveal the extent of opioidrelated overdose events not captured through the health care system, and suggest that we are only seeing the tip of the iceberg of impact on health outcomes from opioids. At the time of this report, the three provinces collecting data on kit use combined reported a total of almost 12 000 kits used to reverse opioid overdoses in communities.
Obtaining reliable information on overdose events in the community is a challenge. It is complicated by the stigma attached to opioid use and the lack of knowledge in the general population of problematic substance use and overdoses. A recent survey by Statistics Canada found that less than one-third of Canadians would recognize the signs of an overdose and only 7% would know how to obtain and administer naloxone to treat an overdose.32 Another national study, by the Canadian Centre on Substance Use and Addiction (CCSA), that looked at the use of kits in the community found that 911 was not called in 30% to 65% of the instances when naloxone was administered by a member of the community. The reason most commonly cited (33%) for not calling was concern about police involvement and possible arrest.33
This report also identified gaps in evidence and areas for further investigation to improve our understanding of the opioid- related harms. These gaps include risk factors; accurate estimates of prevalence of opioid use; nonfatal opioid-related events occurring outside the health care system; national estimates of opioid-related ED visits; and data on special populations including but not limited to Indigenous and other ethnic groups more broadly, as well as marginalized groups such as homeless individuals.
Strengths and limitations
For this report, we reviewed all publicfacing, opioid-related surveillance and epidemiological reports published by provincial and territorial ministries of health and chief coroners’ and medical examiners’ offices on opioid-related deaths, harms and potential risk factors.
There are, however, limitations to the evidence we reviewed. Data sources were constantly being updated throughout the writing of this article, and new, more comprehensive evidence published after January 2018 is not included in this review. This synthesis does not present new information, and extensive reviews of health outcomes, the nonmedical use of prescription opioids, and risk factors for problematic substance use were beyond its scope. It is also important to underscore the significant role of stigma around problematic substance use and marginalized communities, which may contribute to underreporting and subsequent underestimates of the prevalence of use of opioids in the Canadian population. In addition, technology for toxicology screening is constantly improving to keep pace with new drugs. This may impact capacity to detect synthetic opioids such as fentanyl and its analogues and should be considered when evaluating trends. Furthermore, jurisdictional differences in case investigation methods, case definitions, classification methods and toxicology testing may also limit the extent to which comparisons can be made. Therefore, caution should be used when drawing conclusions at this time.
Conclusion
In this review we endeavoured to synthesize available evidence in order to provide a national summary that might be used to support public health action. We also identified gaps in evidence and areas for further investigation to improve our understanding of the national opioid crisis.
A more comprehensive evidence base is essential to inform a concerted, national response to prevent and reduce further opioid-related harms. To provide the evidence necessary to inform and tailor an effective public health response, PHAC will continue to work with federal, provincial and territorial partners to further refine and standardize national data collection as well as to explore the expansion of information sharing to include nontraditional data sources. PHAC will also continue to support our federal partners through the Federal Action on Opioids,34and collaborate with provincial and territorial officials through the Special Advisory Committee on the Epidemic of Opioid Overdoses and its Surveillance Task Group (OOSTG) to improve the quality and accessibility of evidence. Better quality evidence will lead to an improved understanding of which populations are at greater risk of death and harms related to the problematic use of opioids, and will allow for more informed and targeted programs and policies to effectively reduce the impact of this crisis on Canadians.
Acknowledgements
The data presented in this synthesis represent the published work of health and justice officials, first responders and community leaders across the country who are working tirelessly and collaborating extensively to contribute to the knowledge base in order to combat this crisis.
Conflicts of interest
The authors declare no conflicts of interest.
Authors’ contributions and statement
JH conceived the review and provided guidance and input throughout the process. LB designed the methodology, researched and synthesized the information and wrote the paper.
The content and views expressed in this article are those of the authors and do not necessarily reflect those of the Government of Canada.
References
- Public Health Agency of Canada. Ottawa(ON): 2017. National report: apparent opioid-related deaths in Canada (January 2016 to June 2017) (Internet) Available from: https://www.canada.ca/en/public-health/services/publications/healthy-living/apparent-opioid-related-deaths-report-2016-2017-december.html. [Google Scholar]
- Public Health Agency of Canada. Ottawa(ON): 2017. What can CHIRPP tell us about the opioid crisis. [Google Scholar]
- CIHI. Ottawa(ON): 2017. Opioid-related harms in Canada: chartbook, September 2017. Available from: https://www.cihi.ca/sites/default/files/document/opioid-harms-chart-book-en.pdf. [Google Scholar]
- University of Wisconsin. Madison(WI): 2015. Canada: opioid consumption in morphine equivalence (ME), mg per person (Internet) Available from: http://www.painpolicy.wisc.edu/sites/www.painpolicy.wisc.edu/files/country_files/morphine_equivalence/canada_me_methadone.pdf. [Google Scholar]
- Laroche J, et al. Health Canada. Ottawa(ON): (Health Canada) [Google Scholar]
- Report of the International Narcotics Control Board for 2013. United Nations. 2014 Available from: www.incb.org/documents/Publications/AnnualReports/AR2013/English/AR_2013_E.pdf. [Google Scholar]
- Fischer B, Rehm J, et al. Deaths related to the use of prescription opioids. CMAJ. 2009;181((12)):881–2. doi: 10.1503/cmaj.091791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Government of Canada. Ottawa(ON): 2015. Canadian Tobacco, Alcohol and Drugs Survey (CTADS): 2015 Summary (Internet) Available from: https://www.canada.ca/en/health-canada/services/canadian-tobacco-alcohol-drugs-survey/2015-summary.html. [Google Scholar]
- Prepared by Earnscliffe Strategy Group for Health Canada. Ottawa(ON): 2017. Baseline survey on opioid awareness, knowledge and behaviours for public education research report. [Google Scholar]
- Health Canada. Ottawa(ON): Drug Analysis Service: summary report of samples analysed (Internet) Available from: https://www.canada.ca/en/health-canada/services/health-concerns/controlled-substances-precursor-chemicals/drug-analysis-service/2016-drug-analysis-service-summary-report-samples-analysed.html. [Google Scholar]
- Health Canada. Ottawa(ON): Ottawa (ON): Health Canada; 2017 Oct 26. [Google Scholar]
- BCOPPH/BCCDC. Vancouver(BC): 2017. The BC public health opioid overdose emergency: March 2017 update (Internet) Available from: http://www.bccdc.ca/resource-gallery/Documents/Educational%20Materials/Epid/Other/Public%20Surveillance%20Report_2017_03_17.pdf. [Google Scholar]
- CCSA. Ottawa(ON): 2015. CCENDU bulletin: deaths involving fentanyl in Canada, 2009–2014. Available from: http://www.ccdus.ca/Resource%20Library/CCSA-CCENDU-Fentanyl-Deaths-Canada-Bulletin-2015-en.pdf#search=Death%20Involving%20Fentanyl%20in%20Canada%2C%202009%2D2014. [Google Scholar]
- Government of Nunavut. Kugluktuk(NU): Fentanyl in Kugluktuk (Internet) Available from: http://www.gov.nu.ca/health/news/fentanyl-kugluktuk. [Google Scholar]
- BC Coroners Service. Burnaby(BC): Statistical reports into BC fatalities: illicit drug overdose deaths in BC (Internet) Available from: http://www2.gov.bc.ca/assets/gov/public-safety-and-emergency-services/death-investigation/statistical/illicit-drug.pdf. [Google Scholar]
- Government of Alberta. Edmonton(AB): Opioids and subs¬tances of misuse: Alberta report (for Q1 May 19, 2017, Q2 Aug 16, 2017, Q3, Nov 27, 2017) (Internet) Available from: https://open.alberta.ca/publications/opioids-and-substances-of-misuse-alberta-report. [Google Scholar]
- Public Health Ontario. Toronto(ON): Opioid-related morbidity and mortality in Ontario (Internet) Available from: http://www.publichealthontario.ca/en/DataAndAnalytics/Pages/Opioid.aspx#/drug. [Google Scholar]
- BC Coroners Service. Burnaby(BC): Statistical reports into BC fatalities: fentanyl-detected illicit drug overdose deaths in BC (Internet) Available from: https://www2.gov.bc.ca/assets/gov/public-safety-and-emergency-services/death-investigation/statistical/fentanyl-detected-overdose.pdf. [Google Scholar]
- Government of Manitoba. Winnipeg(MB): 2017. Surveillance of opioid misuse and overdose in Manitoba: January 1–March 31, 2017 (Manitoba Health, Seniors and Active Living epi-report) (Internet) Available from: http://www.manitoba.ca/health/publichealth/surveillance/docs/q1_opioid.pdf. [Google Scholar]
- Archambault A, Laing R, et al. Update on DAS analyses and activities related to the opioid crises. Archambault A, Laing R [Google Scholar]
- Apparent deaths related to opioid overdose in New Brunswick (2016 and 2017 (Quarter 1) Data.) (cited 2017 Aug and Dec) Government of New Brunswick. Available from: http://www2.gnb.ca/content/dam/gnb/Departments/h-s/pdf/en/MentalHealth/ApparentDeathsRelatedOpioidOverdose.pdf. [Google Scholar]
- Décès attribuables aux intoxications par opioïdes au Québec, 2000 à 2012: mise à jour 2013–2016 (Internet) INSPQ. :mise à jour 2013–2016 (Internet)–2. Available from: https://www.inspq.qc.ca/publications/2298. [Google Scholar]
- Government of Alberta. Edmonton(AB): Opioids and substances of misuse among First Nations people in Alberta: Alberta report, 2017 (Internet) Available from: open.alberta.ca/dataset/cb00bdd1-5d55-485a-9953-724832f373c3/resource/31c4f309-26d4-46cf-b8b2-3a990510077c/download/Opioids-Substances-Misuse-Report-FirstNations-2017.pdf. [Google Scholar]
- Overdose data and First Nations in BC: preliminary findings (Internet) First Nations Health Authority. 2017 Available from: http://www.fnha.ca/newsContent/Documents/FNHA_OverdoseDataAndFirstNationsInBC_PreliminaryFindings_FinalWeb.pdf. [Google Scholar]
- PHAC. Ottawa(ON): 2017. Analysis of opioid related poisonings/ hospitalizations from the Discharge Abstract Database. [Google Scholar]
- resolution no, et al. 2016 Special Chiefs Assembly—Gatineau, QC: final resolutions (Internet) (QC resolution no. 2016 [Google Scholar]
- Fentanyl brings tragedy to Blood Tribe (Internet) Calgary Herald. Available from: http://calgaryherald.com/news/local-news/fentanyl-brings-tragedy-to-blood-tribe. [Google Scholar]
- Government of Canada. Ottawa(ON): Annual report on deaths in custody 2014/15 (Internet) Available from: http://www.csc-scc.gc.ca/research/005008-3008-eng.shtml. [Google Scholar]
- Summary of bilateral discussions on data sources and opportunities for opioid-related harms surveillance. Public Health Agency of Canada [Google Scholar]
- BC Centre for Disease Control. Vancouver(BC): 2017. The history of the take home naloxone in British Columbia (Internet) Available from: http://www.bccdc.ca/resource-gallery/Documents/THN%20timeline%20bw%2020170628.pdf. [Google Scholar]
- Bell R, et al. CBC News. Toronto(ON): Little pills, big trouble: how Alberta’s fentanyl crisis escalated des¬pite years of warning (Internet) Available from: http://www.cbc.ca/news2/interactives/fentanyl-crisis-alberta/ [Google Scholar]
- Statistics Canada. Ottawa(ON): 2018. Results of the Survey on Opioid Awareness, November, 2017 (Internet) Available from: http://www.statcan.gc.ca/daily-quotidien/180109/dq180109a-eng.pdf. [Google Scholar]
- CCENDU. Ottawa(ON): 2017. CCENDU Bulletin: Calling 911 in drug poisoning situations (Internet) Available from: http://www.ccsa.ca/Resource%20Library/CCSA-CCENDU-Calling-911-Drug-Poisoning-2017-en.pdf. [Google Scholar]
- Government of Canada. Ottawa(ON): Government of Canada actions on opioids: 2016 and 2017 (Internet) Available from: https://www.canada.ca/en/health-canada/services/publications/healthy-living/actions-opioids-2016-2017.html. [Google Scholar]