

Abstract
Objective
HPV vaccination could prevent most HPV-associated cancers, but few U.S. adolescents are vaccinated according to guidelines. To inform efforts to counsel parents more effectively, we sought to quantify their views on the best and worst reasons for guideline-consistent HPV vaccination. We hypothesized that parents’ views would differ according to their confidence in adolescent vaccination.
Methods
We developed a best-worst scaling experiment to evaluate 11 reasons healthcare providers commonly give for HPV vaccination. The instrument was administered in 2016 via a national, online survey to 1,177 parents of adolescents ages 11-17. Parents completed 11 choice tasks of 5 reasons each, indicating the best and worst reason in each task. We used conditional logistic regression to rank reasons for the sample overall and by vaccination confidence (low/high).
Results
Parents viewed cancer prevention as the best reason for HPV vaccination (p<0.001). Other commonly endorsed reasons were preventing a common infection, having lasting benefits, or being a safe vaccine (all p<0.001). Reasons viewed as worst were: it is a scientific breakthrough; I got it for my own child; and your child is due (all p<0.001). Stratified analyses indicated small differences in how often parents with low versus high vaccination confidence endorsed messages (p<0.001), but the two groups ranked reasons similarly overall.
Conclusions
Providers should emphasize cancer prevention when discussing HPV vaccination, as recommended by CDC, the President’s Cancer Panel, and others. Several other common reasons, including having vaccinated one’s own child, may warrant additional testing.
Keywords: adolescent health, human papillomavirus infections/prevention & control, human papillomavirus vaccine, health communication, persuasive communication, choice behavior
INTRODUCTION
Human papillomavirus (HPV) vaccination could prevent most HPV-associated cancers,1 but relatively few U.S. adolescents are vaccinated at ages 11 or 12, as per the recommended schedule for routine administration.2 By 2016, only about one-third (34%) of 13-year-olds were up-to-date nationally, even after accounting for the recent transition from a 3-dose to 2-dose schedule for this age group.2 This suboptimal level of coverage is due, in part, to the way healthcare providers communicate about HPV vaccination.3–12 Although a provider’s recommendation is highly influential, many providers do not consistently endorse HPV vaccination for eligible patients at the recommended age.3–6 Research suggests that providers’ hesitancy stems from factors including discomfort with talking about HPV, as a sexually transmitted infection, and the misconception that many parents have serious concerns about the vaccine.3–4,6–7,13 Strategies are needed to help providers more effectively and efficiently deliver guideline-consistent recommendations within the complex communication surrounding HPV vaccination.
Message testing to understand how parents prioritize reasons for HPV vaccination offers one opportunity to support provider communication. To date, many quantitative and qualitative studies, including our own, have assessed parents’ decision making about HPV vaccination.14–19 However, few have directly compared the persuasiveness of the many possible reasons parents may have for vaccinating. Such an approach could help providers focus their communication efforts and discuss reasons for HPV vaccination that are most compelling to parents, while simultaneously testing whether reasons appeal differently to different audiences. Thus, we sought to quantify parents’ views on the best and worst reasons that providers commonly give for guideline-consistent HPV vaccination, using a preference elicitation method known as best-worst scaling (BWS). We also hypothesized that parents would prioritize reasons differently depending on their level of vaccination confidence, given that health behavior theories such as the Health Belief Model emphasize the importance of individual perceptions on parents’ vaccination decisions.20 By identifying high priority messages for key populations of parents, findings can inform quality improvement efforts to increase HPV vaccination coverage through provider outreach and communication training.
MATERIALS AND METHODS
Participants and procedures
The Adolescent Cancer Prevention Communication Study was a national survey of parents of adolescents ages 11-17, conducted in September 2016. Respondents were members of a standing online panel of U.S. adults maintained by a survey research company.21 The company constructs the panel using a probabilistic, address-based sampling approach that allows for coverage of households with and without landline telephones. To facilitate the participation of lower-income respondents, the company provides Internet access and an Internet-enabled device to households without these resources; this incentive is provided across multiple surveys for the duration of participation in the panel. Households with established Internet access instead receive points towards small cash incentives. Additional methodological information related to the panel is reported elsewhere.21
Of 2,580 parents invited via email to participate in our study, 1,523 responded by visiting the survey website, completing an eligibility screener to confirm having an age-eligible child, and indicating informed consent electronically (without a signature). A total of 1,259 were eligible and completed the survey. The resulting response rate was 59%, calculated using the American Association for Public Opinion Research (AAPOR) formula 4.22 For the present analysis, we excluded respondents who did not fully complete choice tasks related to provider communication about HPV vaccination (n = 82), resulting in a final analytic sample of 1,177 parents. Harvard Pilgrim Health Care Institute’s Institutional Review Board approved the study protocol.
Experimental design and measures
We used BWS to assess parents’ views on the best and worst reasons providers give for guideline-consistent HPV vaccination. BWS is a stated-preference method used to prioritize a list of ideas, attributes, or messages.23 When the number of messages to be tested is relatively long, this approach offers several important advantages to more traditional methods. For example, best-worst scaling is less burdensome for participants than rank ordering and is not susceptible to the problems of scale bias that are inherent in rating.23–25
We first developed a list of 11 reasons that providers commonly give for recommending guideline-consistent HPV vaccination (Table 1). These reasons came from two sources: 1) educational materials developed by government agencies and professional organizations that offer providers guidance about how to counsel patients and their parents about HPV vaccination26,27; and 2) prior research on messages that providers use to motivate HPV vaccination at the recommended ages of 11 or 12 years.7,15,28,29 Prior to fielding our survey, we conducted cognitive interviewing with a convenience sample of parents (n = 13) to improve readability and interpretation of reasons as intended.
Table 1.
Reasons a doctor might give for HPV vaccination.
| The doctor could say… | This means…. | Source |
|---|---|---|
| I think it is important. [personal endorsement] | Doctors may give their own medical opinion about whether to get the HPV vaccine. | 7, 27–29 |
| Your child is due for it. [Due for it] | Public health experts and professional medical organizations recommend that all children receive the HPV vaccine by age 12. | 27 |
| I got it for my own child. [My own child] | Doctors may say whether they decided to get the HPV vaccine for their own children. | 26, 28, 29 |
| It can prevent some types of cancer. [Cancer prevention] | The HPV vaccine can prevent cancer in both men and women. Cancers caused by HPV include cancers of the cervix, head and neck, anus, vagina, and penis. | 7, 15, 26–28 |
| It should be given before sexual contact. [Before sex] | HPV is spread through sexual contact, including intercourse and oral sex. To work best, the HPV vaccine must be given before someone becomes sexually active. | 7, 15, 27–29 |
| It can prevent a common infection. [Infection prevention] | HPV is an extremely common infection. Almost everyone will get HPV at some point in their lives. | 26, 28 |
| It is a safe vaccine. [Safety] | The safety of HPV vaccine has been closely studied. There are no long-term side effects. Short-term side effects, like pain and redness, are similar to other vaccines. | 26, 28 |
| It is a scientific breakthrough. [Scientific breakthrough] | The HPV vaccine is one of the first vaccines developed to prevent cancer. | 28 |
| It works best at this age. [Best age] | The HPV vaccine provides the most protection when given before children become teenagers. | 27, 28 |
| Getting it on time may mean fewer shots. [Fewer shots] | Guidelines for HPV vaccination may soon change. In the future, children who get the HPV vaccine at age 12 may only need 2 shots. Older children may still need 3 shots. | 26 |
| It has lasting benefits. [Lasting benefits] | Children who get the HPV vaccine are protected into adulthood. For this reason, even people who wait until marriage to have sex can benefit from HPV vaccination. | 28 |
Note. Italics indicate message labels and were not shown to respondents.
Next, we developed the experiment with three parts: a scenario, an orientation to the 11 reasons to be tested, and a series of choice exercises. First, respondents read a scenario about a family attending a well child visit:
“Mr. and Mrs. Williams are at the doctor’s office with their child, Sam. Sam is a healthy 12-year-old who is seeing the doctor for a checkup. During the visit, the doctor talks with Mr. and Mrs. Williams about the HPV vaccine. Below are reasons the doctor might give for getting the HPV vaccine.”
Next, respondents read the list of reasons. Reasons were presented in a random order and accompanied by a brief explanation that gave additional background information (Table 1). Finally, respondents completed 11 choice tasks that each consisted of a subset of 5 messages (Figure 1). For each choice task, respondents indicated the best and the worst reason the doctor could give for getting the HPV vaccine at that visit. To construct the experiment, we used a balanced incomplete block design (BIBD) which ensured that reasons occurred and co-occurred an equal number of times for each respondent. We pretested our experiment with online panel members (n = 30) to ensure proper functioning. Parents who participated in pretesting or cognitive interviewing were excluded from further participation in the study.
Figure 1.
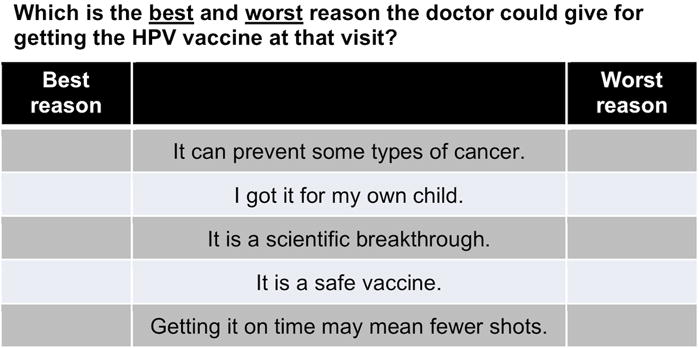
Example of a best-worst scaling choice task.
Figure 1 shows an example choice task. Parents completed 11 tasks, indicating the best and worst reason for HPV vaccination in each subset of 5 reasons.
The survey assessed parents’ vaccination confidence using the short form of the Vaccination Confidence Scale, a validated measure of parents’ beliefs about adolescent vaccination.30,31 Developed using data from the National Immunization Survey-Teen, this scale consists of 4 items assessing perceptions of vaccine necessity (“Vaccines are necessary to protect the health of teenagers”), safety (“Vaccines are safe”), and effectiveness (“Vaccines do a good job in preventing the diseases they are intended to prevent”), as well as the consequences of not vaccinating (“If I do not vaccinate my teenager, he or she may get a disease such as meningitis.”). Parents rated items using response options ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). We averaged responses to the scale’s 4 items to create a composite score and then categorized parental vaccination confidence as low (1-4) or high (4.25-5), based on the mean composite score of 4.2. Vaccination confidence items preceded the BWS experiment.
Data on demographic characteristics were assessed via additional survey items or provided by the survey company. These measures included the respondents’ sex, age, race/ethnicity, and educational attainment, as well as the sex, age, and HPV vaccination status (≥1 dose) of the respondents’ children. Measures also included households’ annual income and geographic region.
Analysis
Using data from the choice tasks, we analyzed parents’ prioritization of reasons for HPV vaccination using conditional logistic regression to model choice as the dependent variable. We assumed sequential best-worst decision-making, which means that respondents’ first chose the best reason among the five messages and then the worst reason among the remaining four messages. Effects coding was used to estimate scores for each reason. To test our hypothesis that parents’ with low versus high vaccination confidence would prioritize reasons differently, we repeated these analyses after stratifying on this variable. To probe our findings, we examined different cut-points to define categories of Vaccination Confidence Scale scores; because results did not differ from the primary analysis, we do not report further on the findings of this sensitivity analysis. In exploratory analyses, we also stratified our findings by children’s vaccination status, sex, and age. We conducted analyses using Stata Version 13 (College Station, TX). Statistical tests were two-tailed with a critical alpha of 0.05.
RESULTS
Sample characteristics
Parents reported on similar numbers of children by sex (53% male) and age (mean=14 years; Table 2). Most children were non-Hispanic white (63%), non-Hispanic black (9%), or Hispanic (20%). Over half (57%) had initiated HPV vaccination (≥1 dose). Our sample included parents of both sexes (51% female), as well as those with lower socioeconomic status (40% with a high school degree or less education; 20% with household income less than $35,000). Parents resided in all regions of the U.S.
Table 2.
Sample characteristics (n=1,177).
| n | (%) | |
|---|---|---|
| Child characteristics | ||
| Sex | ||
| Male | 620 | (53) |
| Female | 557 | (47) |
| Age (years) | ||
| 11-12 | 318 | (27) |
| 13-15 | 479 | (41) |
| 16-17 | 380 | (32) |
| Race | ||
| Non-Hispanic white | 740 | (63) |
| Non-Hispanic black | 100 | (9) |
| Hispanic | 241 | (20) |
| Other | 96 | (8) |
| HPV vaccination status | ||
| 0 doses | 508 | (43) |
| 1+ doses | 669 | (57) |
| Parent characteristics | ||
| Sex | ||
| Male | 576 | (49) |
| Female | 601 | (51) |
| Educational attainment | ||
| High school degree or less | 470 | (40) |
| Some college, no degree | 307 | (26) |
| College degree or more | 400 | (34) |
| Household characteristics | ||
| Annual income | ||
| <$35,000 | 240 | (20) |
| $35,000-$74,999 | 332 | (28) |
| ≥$75,000 | 605 | (51) |
| Region | ||
| Northeast | 211 | (18) |
| Midwest | 287 | (24) |
| South | 403 | (34) |
| West | 276 | (23) |
Best and worst reasons for HPV vaccination
Table 3 shows reasons for HPV vaccination ranked according to results of the conditional logit analysis. In the overall sample, parents viewed cancer prevention as the best reason for guideline-consistent HPV vaccination (β=2.07). Other highly ranked reasons were preventing a common infection (0.68), having lasting benefits (0.67), or being a safe vaccine (0.41). Reasons for HPV vaccination that parents viewed as worst were: it is a scientific breakthrough (−0.67); I got it for my own child (−0.98); and your child is due for it (−1.08).
Table 3.
Relative persuasiveness of reasons for HPV vaccination, overall and by vaccination confidence.
| Overall | Low vaccination confidence | High vaccination confidence | |||||||
|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|||||||
| β | SE | Rank | β | SE | Rank | β | SE | Rank | |
| Cancer prevention | 2.07 | 0.03 | 1st | 1.78 | 0.04 | 1st | 2.30 | 0.03 | 1st |
| Infection prevention | 0.68 | 0.02 | 2nd | 0.70 | 0.04 | 2nd | 0.66 | 0.03 | 3rd |
| Lasting benefits | 0.67 | 0.02 | 3rd | 0.66 | 0.04 | 3rd | 0.67 | 0.03 | 2nd |
| Safety | 0.41 | 0.02 | 4th | 0.34 | 0.04 | 4th | 0.45 | 0.03 | 4th |
| Best age | 0.04 | 0.02 | 5th | 0.03 | 0.04 | 5th | 0.04 | 0.03 | 5th |
| Before sex | −0.05 | 0.02 | 6th | −0.11 | 0.04 | 6th | 0.00 | 0.03 | 6th |
| Personal endorsement | −0.49 | 0.02 | 7th | −0.44 | 0.04 | 8th | −0.52 | 0.03 | 7th |
| Fewer shots | −0.60 | 0.02 | 8th | −0.40 | 0.04 | 7th | −0.74 | 0.03 | 9th |
| Scientific breakthrough | −0.67 | 0.02 | 9th | −0.61 | 0.04 | 9th | −0.73 | 0.03 | 8th |
| My own child | −0.98 | 0.02 | 10th | −0.89 | 0.04 | 10th | −1.04 | 0.03 | 10th |
| Due for it | −1.08 | 0.02 | 11th | −1.05 | 0.04 | 11th | −1.11 | 0.03 | 11th |
Note. Shading indicates difference from overall ranking.
Stratified analyses indicated differences in how parents with low versus high vaccination confidence viewed reasons for HPV vaccination (p<0.001, Table 3, Figure 2). Parents with low less often endorsed cancer prevention, fewer shots, or I got it for my own child. However, these differences were small and resulted in few differences in overall rankings. In exploratory analyses, we found similarly few differences in parents’ overall ranking of reasons when we stratified our findings by child’s vaccination status, sex, or age (Supplemental Tables 1-3).
Figure 2.
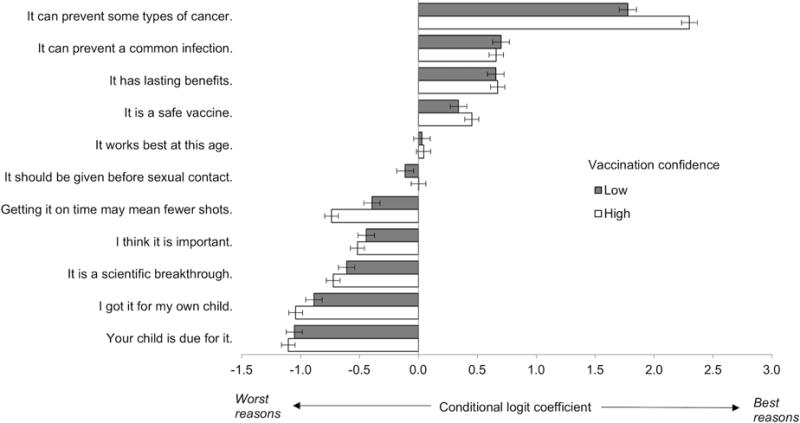
Best and worst reasons for HPV vaccination by vaccination confidence.
Parents with low and high vaccination confidence prioritized messages similarly. Both groups endorsed cancer prevention as the best reason for HPV vaccination. Bars show 95% confidence intervals
DISCUSSION
Using data from a national sample, we found that parents of adolescents prioritized cancer prevention as the best reason healthcare providers commonly give for guideline-consistent HPV vaccination. This finding is consistent with a large body of work that highlights the value parents place on protecting their children from cancer,7,14,15,26,27 but also extends prior research in several important ways. First, by using best-worst scaling, this study quantifies the extent of parents’ preference for cancer prevention through direct comparison with other common reasons. Furthermore, through stratified analyses, we found that prioritization did not vary by vaccination confidence; although parents with low versus high confidence somewhat less often selected cancer prevention as a best reason, both groups favored it far more highly than any of the other reasons we tested. In this way our findings provide empirical support for the guidance given by public health and professional organizations, including the Centers for Disease Control and Prevention, the American Academy of Pediatrics, and the President’s Cancer Panel, which urge providers to frame HPV vaccination as cancer prevention.26,27,32 Interestingly, other high-performing reasons, including lasting benefits, were also related to HPV vaccination’s ability to protect, and may be useful for supplementing the primary cancer prevention message.
In contrast to cancer prevention, several other reasons for HPV vaccination tested poorly among parents. For example, it is a scientific breakthrough ranked near the bottom of our list, despite being perceived as an effective message by pediatricians and family physicians in a prior study.28 Given that parents still invoke the “newness” of HPV vaccine as a concern more than a decade post-licensure,33 it is likely that references to scientific novelty, although understandably appealing to medical professionals, are best avoided with parents. I got it for my own child was another low-ranked reason, which is surprising given that both providers and professional organizations promote this message as being effective for motivating HPV vaccination.26,28,29 Parents have also given this message relatively low marks in a traditional message rating study,14 raising the possibility that providers should prioritize their professional versus personal experience unless explicitly asked about their own vaccination decisions. Finally, your child is due for it was similarly ranked poorly. It may be that this message is effective for introducing the topic of adolescent vaccination, but is not viewed by parents as a reason for vaccinating per se. We also interpret our findings with care to acknowledge that reasons with low rankings were not necessarily “bad” messages; rather, they were reasons parents chose not to prioritize in relation to other available options.
Contrary to our hypothesis, we found relatively little evidence to suggest that parents with low versus high vaccination confidence prioritized reasons for HPV vaccination differently. In several cases, we found that parents with low confidence expressed less extreme preferences for or against individual reasons. However, the two groups ranked the 11 reasons similarly overall, suggesting that, although parents with low confidence may find top reasons for HPV vaccination less compelling, they would not necessarily benefit from targeted messaging. These findings may give busy providers more confidence in communicating about HPV vaccination, enabling them to begin conversations uniformly with messages about cancer prevention and then tailoring the conversation to address each parent’s specific concerns only if necessary. Given that this study is specific to provider communication, future research is needed to determine how messaging in other contexts, such as social media, may inform the decision making of parents with low vaccination confidence.
This study used BWS to provide novel data on parents’ views on HPV vaccination. Strengths include a large, national sample of parents of adolescents, with coverage for HPV vaccine initiation similar to the national average in 2016 (64% versus 60%, respectively, for ages 13-17).2 Best-worst scaling methodology is becoming increasingly common in health-related research,34–36 and offers advantages to traditional rating or ranking techniques as a low-burden method for quantitatively prioritizing a relatively large number of messages.23–25 Similar to many other approaches to message testing, the primary limitation of best-worst scaling is its focus on “stated” preferences, or parents’ perceptions of what constitutes a good reason for HPV vaccination, which may be different from “revealed” preferences, or the messages that would motivate them to vaccinate in an actual encounter with their adolescent’s provider. Most notably, our BWS scenario was not designed to test preferred messages to address specific parental concerns. Similarly, we were not able to assess how parents’ prioritization of reasons was influenced by contextual factors, such as visit type or patient-provider relationship quality, or other communication factors, such as the use of “bundled” recommendations for all vaccines in the adolescent platform. For this reason, continued intervention research is needed to extend the present study, including work to identify efficient strategies for training providers to improve their communication about HPV vaccination and to assess the impact of such training on parents’ HPV vaccine decision making.
Conclusion
HPV vaccination could substantially reduce the burden of HPV-related cancers in the U.S., but to achieve widespread coverage, healthcare providers need strategies for more effectively and efficiently communicating its value. Message testing to identify ways of motivating guideline-consistent vaccination while also meeting parents’ communication preferences may be especially valuable. Findings of this best-worst scaling study provide support for prioritizing cancer prevention as a reason for HPV vaccination, even among parents with low vaccination confidence. At the same time, this study identifies several commonly suggested reasons for HPV vaccination that parents perceived as less compelling and may warrant additional testing. This study illustrates the value of using stated-preference methods to inform public health communication strategies. Our findings provide an evidence base for efforts to support providers in recommending HPV vaccination and addressing parents’ concerns so as to increase guideline-consistent uptake of this important preventive service.
Supplementary Material
Acknowledgments
This study was funded by the National Cancer Institute (K22 CA186979 for M. B. Gilkey). Funders played no role in the design and conduct of the study; collection, management, analysis, and interpretation of data; preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication.
Footnotes
Conflicts of interest: The authors declare no potential conflicts of interest.
References
- 1.Saraiya M, Unger ER, Thompson TD, Lynch CF, Hernandez BY, Lyu CW, et al. US assessment of HPV types in cancers: implications for current and 9-valent HPV vaccines. J Natl Cancer Inst. 2015;107:djv086. doi: 10.1093/jnci/djv086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Walker TY, Elam-Evans LD, Singleton JA, Yankey D, Markowitz LE, Fredua B, et al. National, Regional, State, and Selected Local Area Vaccination Coverage Among Adolescents Aged 13-17 Years - United States, 2016. Morb Mortal Wkly Rep. 2017;66:874–82. doi: 10.15585/mmwr.mm6633a2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.McRee AL, Gilkey MB, Dempsey AF. HPV vaccine hesitancy: findings from a statewide survey of health care providers. J Pediatr Health Care. 2014;28:541–9. doi: 10.1016/j.pedhc.2014.05.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gilkey MB, Malo TL, Shah PD, Hall ME, Brewer NT. Quality of physician communication about human papillomavirus vaccine: findings from a national survey. Cancer Epidemiol Biomarkers Prev. 2015;24:1673–9. doi: 10.1158/1055-9965.EPI-15-0326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Vadaparampil ST, Malo TL, Sutton SK, Ali KN, Kahn JA, Casler A, et al. Missing the Target for Routine Human Papillomavirus Vaccination: Consistent and Strong Physician Recommendations Are Lacking for 11- to 12-Year-Old Males. Cancer Epidemiol Biomarkers Prev. 2016;25:1435–46. doi: 10.1158/1055-9965.EPI-15-1294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kulczycki A, Qu H, Shewchuk R. Primary care physicians’ adherence to guidelines and their likelihood to prescribe the human papilomavirus vaccine for 11- and 12-year-old girls. Women’s Health Issues. 2016;26:34–9. doi: 10.1016/j.whi.2015.07.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Alexander AB, Best C, Stupiansky N, Zimet GD. A model of health care provider decision making about HPV vaccination in adolescent males. Vaccine. 2015;33:4081–6. doi: 10.1016/j.vaccine.2015.06.085. [DOI] [PubMed] [Google Scholar]
- 8.Gilkey MB, Calo WA, Moss JL, Shah PD, Marciniak MW, Brewer NT. Provider communication and HPV vaccination: The impact of recommendation quality. Vaccine. 2016;34:1187–92. doi: 10.1016/j.vaccine.2016.01.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Dempsey AF, Pyrzanowski J, Lockhart S, Campagna E, Barnard J, O’Leary ST. Parents’ perceptions of provider communication regarding adolescent vaccines. Hum Vaccin Immunother. 2016;12:1469–75. doi: 10.1080/21645515.2016.1147636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kester LM, Zimet GD, Fortenberry JD, Kahn JA, Shew ML. A national study of HPV vaccination of adolescent girls: rates, predictors, and reasons for non-vaccination. Matern Child Health J. 2013;17:879–85. doi: 10.1007/s10995-012-1066-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Rosenthal SL, Weiss TW, Zimet GD, Ma L, Good MB, Vichnin MD. Predictors of HPV vaccine uptake among women aged 19-26: importance of a physician’s recommendation. Vaccine. 2011;29:890–5. doi: 10.1016/j.vaccine.2009.12.063. [DOI] [PubMed] [Google Scholar]
- 12.Gilkey MB, McRee AL. Provider communication about HPV vaccination: A systematic review. Hum Vaccin Immunother. 2016;12:1454–68. doi: 10.1080/21645515.2015.1129090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Healy CM, Montesinos DP, Middleman AB. Parent and provider perspectives on immunization: are providers overestimating parental concerns? Vaccine. 2014;32:579–84. doi: 10.1016/j.vaccine.2013.11.076. [DOI] [PubMed] [Google Scholar]
- 14.Malo TL, Gilkey MB, Hall ME, Shah PD, Brewer NT. Messages to motivate human papillomavirus vaccination: national studies of parents and physicians. Cancer Epidemiol Biomarkers Prev. 2016;25:1383–91. doi: 10.1158/1055-9965.EPI-16-0224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Perkins RB, Clark JA, Apte G, Vercruysse JL, Sumner JJ, Wall-Haas CL, et al. Missed opportunities for HPV vaccination in adolescent girls: a qualitative study. Pediatrics. 2014;134:e666–74. doi: 10.1542/peds.2014-0442. [DOI] [PubMed] [Google Scholar]
- 16.Griffioen AM, Glynn S, Mullins TK, Zimet GD, Rosenthal SL, Fortenberry JD, et al. Perspectives on decision making about human papillomavirus vaccination among 11- to 12-year-old girls and their mothers. Clin Pediatr (Phila) 2012;51:560–8. doi: 10.1177/0009922812443732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Alexander AB, Stupiansky NW, Ott MA, Herbenick D, Reece M, Zimet GD. What parents and their adolescent sons suggest for male HPV vaccine messaging. Health Psychol. 2014;33:448–56. doi: 10.1037/a0033863. [DOI] [PubMed] [Google Scholar]
- 18.Mullins TL, Griffioen AM, Glynn S, Zimet GD, Rosenthal SL, Fortenberry JD, et al. Human papillomavirus vaccine communication: perspectives of 11-12 year-old girls, mothers, and clinicians. Vaccine. 2013;31:4894–901. doi: 10.1016/j.vaccine.2013.07.033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Gilkey MB, Calo WA, Marciniak MW, Brewer NT. Parents who refuse or delay HPV vaccine: Differences in vaccination behavior, beliefs, and clinical communication preferences. Hum Vaccin Immunother. 2017;13:680–86. doi: 10.1080/21645515.2016.1247134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Rosenstock IM. Historical origins of the Health Belief Model. Health Educ Behav. 1974;2(4):328–35. [Google Scholar]
- 21.GfK. Knowledgepanel Design Summary. 2013 doi: http://www.knowledgenetworks.com/knpanel/docs/knowledgepanel(R)-design-summary-description.pdf. Accessed September 27, 2017.
- 22.American Association for Public Opinion Research. Standard definitions: final dispositions of case codes and outcome rates for surveys. 2016 doi: http://www.aapor.org/AAPOR_Main/media/publications/Standard-Definitions20169theditionfinal.pdf. Accessed September 27, 2017.
- 23.Flynn T. Valuing citizen and patient preferences in health: recent developments in three types of best–worst scaling. Exp Rev Pharmacoeconomics Outcomes Res. 2010;10:259–67. doi: 10.1586/erp.10.29. [DOI] [PubMed] [Google Scholar]
- 24.Feudtner C, Walter JK, Faerber JA, Hill DL, Carroll KW, Mollen CJ, et al. Good-parent beliefs of parents of seriously ill children. JAMA Pediatr. 2015;169:39–47. doi: 10.1001/jamapediatrics.2014.2341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ozawa S, Wonodi C, Babalola O, Ismail T, Bridges J. Using best-worst scaling to rank factors affecting vaccination demand in northern Nigeria. Vaccine. 2017;35:6429–37. doi: 10.1016/j.vaccine.2017.09.079. [DOI] [PubMed] [Google Scholar]
- 26.Centers for Disease Control and Prevention. Talking to parents about HPV vaccine. 2016 https://www.cdc.gov/hpv/hcp/for-hcp-tipsheet-hpv.html. Accessed October 1, 2017.
- 27.American Academy of Pediatrics. Be a champion for HPV vaccination. 2017 https://www.aap.org/en-us/Documents/HPV_ChampionTipIn_Oct_2015.pdf. Accessed October 1, 2017.
- 28.Gilkey MB, Malo TL, Hall ME, Calo WA, Brewer NT. Physicians’ rhetorical strategies for motivating HPV vaccination. doi: 10.1016/j.socscimed.2020.113441. Under review. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Sturm L, Donahue K, Kasting M, Kulkarni A, Brewer NT, Zimet GD. Pediatrician-parent conversations about human papillomavirus vaccination: an analysis of audio recordings. J Adolesc Health. 2017;61:246–51. doi: 10.1016/j.jadohealth.2017.02.006. [DOI] [PubMed] [Google Scholar]
- 30.Gilkey MB, Magnus BE, Reiter PL, McRee AL, Dempsey AF, Brewer NT. The Vaccination Confidence Scale: a brief measure of parents’ vaccination beliefs. Vaccine. 2014;32:6259–65. doi: 10.1016/j.vaccine.2014.09.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Gilkey MB, Reiter PL, Magnus BE, McRee AL, Dempsey AF, Brewer NT. Validation of the Vaccination Confidence Scale: a brief measure to identify parents at risk for refusing adolescent vaccines. Acad Pediatr. 2016;16(1):42–9. doi: 10.1016/j.acap.2015.06.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.President’s Cancer Panel Annual Report. Accelerating HPV vaccine uptake: urgency for action to prevent cancer A report to the President of the United States from the President’s Cancer Panel. Bethesda, MD: National Cancer Institute; 2014. [Google Scholar]
- 33.Galbraith-Gyan KV, Lechuga J, Jenerette CM, Palmer MH, Moore AD, Hamilton JB. HPV vaccine acceptance among African-American mothers and their daughters: an inquiry grounded in culture. Ethn Health. 2017;29:1–18. doi: 10.1080/13557858.2017.1332758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Peay HL, Hollin IL, Bridges JF. Prioritizing parental worry associated with Duchenne muscular dystrophy using best-worst scaling, J Genet Couns. 2016;25:305–13. doi: 10.1007/s10897-015-9872-2. [DOI] [PubMed] [Google Scholar]
- 35.Oakes AH, Garmo VS, Bone LR, Longo DR, Segal JB, Bridges JFP. Identifying and prioritizing the barriers and facilitators to the self-management of type 2 diabetes mellitus: a community-centered approach. Patient. 2017;10:773–83. doi: 10.1007/s40271-017-0248-6. [DOI] [PubMed] [Google Scholar]
- 36.Cheung KL, Wijnen BF, Hollin IL, Janssen EM, Bridges JF, Evers SM, et al. Using best-worst scaling to investigate preferences in health care. Pharmacoeconomics. 2016;34:1195–209. doi: 10.1007/s40273-016-0429-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.