

Abstract
Objective
To test the variability of the volume measurements when different segmentation methods are applied in pulp volume reconstruction.
Materials and methods
Osirix® and ITK-SNAP software were used. Different segmentation methods (Part A) and volume approaches (Part B) were tested in a sample of 21 dental CBCT’s from upper canines. Different combinations of the data set were also tested on one lower molar and one upper canine (Part C) to determine the variability of the results when automatic segmentation is performed.
Results
Although the obtained results show correlation among them(r>0.75), there is no evidence that these methods are sensitive enough to detect small volume changes in structures such as the dental pulp canal (Part A and Part B). Automatic segmentation is highly susceptible to be affected by small variations in the setting parameters (Part C).
Conclusions
Although the volumetric reconstruction and pulp/tooth volume ratio has not shown better results than methods based on dental radiographs, it is worth to persevere with the research in this area with new development in imaging techniques.
Keywords: age estimation, pulp volume calculation, image segmentation
INTRODUCTION
Since 1950 different methods have been proposed to estimate dental age in adults. (1) Most of them are based on the formation of secondary dentine and the decrease of the pulp chamber size with age. (2, 3) Methods that have an invasive approach, (for example aspartic acid racemization and cementum annulation), are not of preference, as they often require the physical damage of the sample. (4) With the evolution of different diagnostic imaging techniques, non-invasive methods for dental age estimation have become the preferred methods, (5) starting with the use of periapical dental radiographs, (2, 3) then panoramic radiographs (6) and more recently cone beam computed tomography (CBCT). (7)
Micro-Computer Tomography (µCT) was introduced in the early 20th century (8) to determine age related three-dimensional changes in pulp cavities, from maxillary first premolar teeth. Consistent with early histological research, µCT study’s findings indicate that decrease in pulp volume is not linear. It demonstrates a quicker reduction between the 20 and 40 years and then it slows down thereafter. Further research correlating the ratio between pulp and tooth volume with the chronological age, using µCT and linear regression models to estimate dental age in adults, found promising outcomes. (8) However, in light of the high radiation doses associated with µCT, only extracted teeth can be measured in this way. (9) More recently CBCT has been used for dental age estimation calculating the volumes from tooth and pulp chamber. Since then, volumetric reconstruction from CBCT with different software have been reported in various studies for dental age estimation in adults. (10-13) The most recent studies document the use of CBCT from single- (5, 13) and multi-rooted teeth. (14). However, these new methods have not shown superior accuracy to the methods based on dental radiographs. (2, 15) It is evident that within each type of software there are a series of sensitivity settings that influences the mathematical approach to measure the baseline volumetric data. These settings clearly have consequences for the outcome and may well be in part the cause of the substantial variation. The primary aim of this study was to test the variability of the volume measurements when different segmentation methods were applied to pulp volume reconstruction. This study is designed to ensure that the underpinning assumptions of a commonly used age estimation approach based on pulp volume calculation are as accurate as possible.
MATERIALS AND METHODS
Ethics approval for this study was obtained from the Human Research Ethics Committee of the University of Western Australia (Ref: RA/4/1/6797). This study has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki.
Study sample
A total of 22 anonymized dental CBCT’s were used in this study. All of them were recorded with therapeutic purposes, with the consent of the participants, and there was no unnecessary or repeated radiation exposure. All the images were previously unidentified, and age and sex of each individual was the only known information. From these, 57% (n=12) were female, age range 17-63 years, mean age 33.7, and 43% (n=9) were male, age range=15-52 years, mean age 36.7. The CBCT’s were obtained from the radiology department of the University of Kebangsaan, Malaysia, and the research group INVIENDO from the National University of Colombia, In both cases the images were obtained using the 9000 3D Extraoral Imaging System (Carestream Dental, Atlanta, GA, USA) which had a 180˚ rotation and a field of view (FOV) of 50 mm by 37 mm. The radiation exposure parameters were 8-10 mA, 70 Kv, with a slice thickness of 0.076mm. The images were saved in DICOM format. The selected tooth to apply the different segmentation approaches was the upper right canine, or the left when the right was absent (with Federation Dentaire International (FDI) notation 13 and 23) reconstructing one tooth per subject. Only sound teeth, free of any restorations with completed apex formation were included.
Measurement software ITK-SNAP version 3.4 (open source software, www.itksnap.org) and Osirix® (OnDemand 3D software CyberMed Inc, Seoul, South Korea) were used in this study. All the segmentations were completed by a single observer (TYM). All data was collated using Excel (version 2013 Microsoft Redmont, USA) and statistical analysis was completed using R Core Team version 3.1.3 (2015). (R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL http://www.R-project.org/.)
Description of the method
This study tested the comparative outcome of three different ways of estimating the pulp volume, (5, 13, 14) dental age indicator used in adults. The tests were carried out on the root pulp chamber of upper canines (n=21), to calculate the correlation between automatic (14) and manual segmentation (5) (Part A)(Table 1) and cone shape approach volume calculation (13) (Part B)(Table 2). The final part of the study (Part C)(Table 3) tested the variability of the results obtained with different setting parameter values combinations for automatic segmentation of the pulp canal of one multi-rooted tooth, as previously reported in the literature (14) and one single rooted tooth. (Figure 1)
Table 1. Volume results of using automatic segmentation (Vol 1), manual segmentation using just the first and last slice (Vol 2) and manual segmentation each forth slice (Vol3), of cone beam computer tomography from upper canines (FDI 13, 23).
| Individual | Vol 1 (mm3) | Vol 2 (mm3) | Vol 3 (mm3) |
|---|---|---|---|
| 1 | 10.87 | 10.6 | 13.2 |
| 2 | 16.03 | 17 | 19.7 |
| 3 | 16.4 | 20.9 | 19.8 |
| 4 | 9.309 | 12.9 | 14.8 |
| 5 | 5.478 | 7.1385 | 8.04 |
| 6 | 11.25 | 12.5 | 12.6 |
| 7 | 13.26 | 25.9 | 16.3 |
| 8 | 16.72 | 17 | 23.2 |
| 9 | 37.01 | 32.6 | 41.9 |
| 10 | 16.98 | 23.4 | 28.9 |
| 11 | 11.77 | 19.2 | 17.7 |
| 12 | 5.857 | 8.7131 | 11.7 |
| 13 | 9.107 | 13.3 | 28.3 |
| 14 | 17.24 | 33 | 29.8 |
| 15 | 12.76 | 27.5 | 21.1 |
| 16 | 15.87 | 16.1 | 27 |
| 17 | 13.2 | 19.7 | 22.6 |
| 18 | 11.61 | 19.7 | 16.5 |
| 19 | 24.52 | 35.3 | 40 |
| 20 | 15.51 | 22.1 | 22.1 |
| 21 | 17.6 | 29.3 | 35.5 |
| Mean | 14.68 | 20.18 | 22.41 |
Table 2. Cone shape approach results using the tool polygon (Pol) and oval (Oval). Pulp area (in mm2) at the CEJ level and volume (in mm3) calculation with the measured root length (in mm).
| Area | Area Pol | Area Oval | Root length | Vol Pol | Vol Oval |
|---|---|---|---|---|---|
| 1 | 22 | 20 | 1.55 | 11.2 | 10.2 |
| 2 | 29 | 30.5 | 1.46 | 14.1 | 14.8 |
| 3 | 28 | 24.5 | 1.46 | 13.6 | 11.9 |
| 4 | 20 | 9.85 | 1.51 | 10.0 | 4.9 |
| 5 | 21 | 16 | 1.04 | 7.3 | 5.5 |
| 6 | 16 | 13.5 | 1.56 | 8.3 | 7.0 |
| 7 | 46 | 29 | 1.86 | 28.6 | 18.0 |
| 8 | 37 | 20.5 | 1.64 | 20.3 | 11.2 |
| 9 | 52 | 41 | 1.38 | 24.0 | 18.9 |
| 10 | 32 | 26.5 | 1.63 | 17.4 | 14.4 |
| 11 | 30 | 17 | 1.28 | 12.8 | 7.2 |
| 12 | 34 | 16 | 1.38 | 15.8 | 7.4 |
| 13 | 32 | 22 | 2.10 | 22.4 | 15.4 |
| 14 | 28 | 14 | 1.71 | 16.1 | 8.0 |
| 15 | 42 | 28.5 | 1.79 | 24.9 | 16.9 |
| 16 | 27 | 16 | 1.71 | 15.4 | 9.1 |
| 17 | 25 | 17.5 | 1.96 | 16.2 | 11.3 |
| 18 | 35 | 25.5 | 1.47 | 17.2 | 12.5 |
| 19 | 58 | 44.5 | 1.73 | 33.9 | 26.0 |
| 20 | 39 | 26.5 | 1.52 | 19.8 | 13.4 |
| 21 | 46 | 24.5 | 2.17 | 33.3 | 17.7 |
| SD | 8.7 | 10.86 | 7.45 | 5.2 |
Table 3. Setting parameter combinations used in part C.
| Repetition | Scale of Gaussian | Edge contrast | Edge transformation exponent. | Smoothing force | Average molar volume mm3 | Average canine volume mm3 |
|---|---|---|---|---|---|---|
| 1 | 2.14 | 0.09 | 4 | 0.2 | 38.415 | 36.58 |
| 2 | 3 | 0.05 | 3 | 0.2 | 45.775 | 49.7 |
| 3 | 2.05 | 0.05 | 3 | 0.2 | 34.525 | 49.7 |
| 4 | 2.5 | 0.05 | 3 | 0.2 | 46.075 | 41.81 |
| 5 | 2.5 | 0.1 | 2.5 | 0.2 | 49.38 | 48.87 |
| 6 | 2.5 | 0.2 | 2.05 | 0.2 | 53.74 | 48.94 |
| 7 | 2 | 0.1 | 2.5 | 0.2 | 43.55 | 39.27 |
| 8 | 2.15 | 0.09 | 4 | 0.2 | 36.53 | 40.26 |
| 9 | 2.15 | 0.09 | 4 | 0.3 | 38.94 | 39.76 |
| 10 | 2.15 | 0.09 | 4 | 0.35 | 42 | 39.38 |
| 11 | 3 | 0.05 | 3 | 0.3 | 47.29 | 50.89 |
| 12 | 3 | 0.05 | 3 | 0.35 | 43.555 | 48.92 |
| 13 | 3 | 0.05 | 3 | 0.4 | 44.69 | 48.9 |
| 14 | 2.05 | 0.05 | 3 | 0.3 | 38.695 | 35.98 |
| 15 | 2.05 | 0.05 | 3 | 0.35 | 38.79 | 35.89 |
| 16 | 2.05 | 0.05 | 3 | 0.4 | 38.46 | 36.04 |
| 17 | 1.5 | 0.05 | 2.51 | 0.2 | 34.3 | 31.92 |
| 18 | 1.5 | 0.05 | 2.5 | 0.2 | 34.955 | 30.08 |
| 19 | 1 | 0.1 | 3 | 0.2 | 31.73 | 29.83 |
| 20 | 2 | 0.05 | 4 | 0.2 | 36.405 | 35.10 |
| SD | 0.53 | 0.03 | 0.59 | 0.07 | 5.74 | 7.12 |
| Variance | 0.28 | 0.001 | 0.35 | 0.005 | 32.94 | 50.75 |
There are 3 parameters available in ITK-SNAP software that are not listed, as they were constant for all the reconstructions: Edge attraction force (=2) and step size (=1) and smoothing force which was changed from 1 to 0.5 only for the 18th combination.
Fig.1.
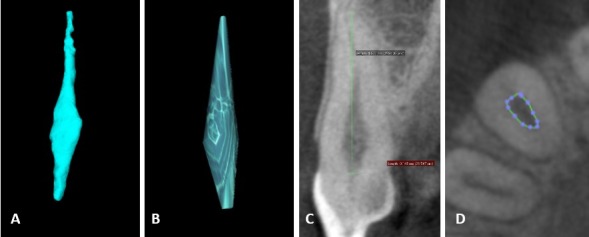
Volumetric reconstructions, upper right canine using different methods Volumetric reconstruction of tooth 13 from a female individual, 36 years old, using the different methodologies mentioned in this paper. A: Semiautomatic recontruction using ITK-SNAP software. B: Manual segmentation using Osirix ® software. C and D: Cone shape geometric approximation, following the methodology reported by the author doing area measurement of he root canal at the level of the CEJ (D) and length measurement of the root from the CEJ up to the root apex (C), using Osirix ® software.
Part A. Automatic and manual segmentation
Automatic segmentation was performed using the software ITK-SNAP. (Figure 1. A). Manual segmentation used software Osirix ® and its 2D viewer, (Figure 1. B) which allows the observer to go slice by slice and manually select the boundaries of the space to reconstruct, using the tool polygon. The automatic segmentation process in ITK-SNAP is called seed region-growing. To apply it, the observer sets up a “seed” inside the structure to reconstruct, in this case the pulp chamber. This seed grows and a volume is finally obtained.
Automatic segmentation of the pulp was generated using the same combination of setting parameters through the entire sample: Scale of Gaussian blurring: 3.0, edge transformation contrast: 0.2, edge transformation exponent: 4.0, expansion (balloon) force: 1.0, smoothing (curvature) force: 0.2, edge attraction (advection) force 2.0. In three cases the edge transformation exponent needed to be adjusted to 0.05.
Regression models were run to establish which of the setting parameters would have the most significant influence on the final results. Little changes in the Scale of Gaussian generated the bigger changes in the final obtained values (p< 0.001).
With manual segmentation two approaches were used. Firstly, every fourth slice was analysed as for the published method. Secondly, the first and last slice was used as the sample. To analyse the same length of root in the automatic and manual approaches, a length defined in the automatic approach was set for the manual approach.
Part B. Cone shape geometric approximation
The geometric approximation of the root canal to cone is a simple conservative method and has been used for dental age estimation in adults. Using Osirix®, ovals of best fit were formed in the root canal at the cemento-enamel junction (CEJ) level, following the reported method. (13) Secondly, instead of best fit ovals, the boundaries of the pulp canal were drawn using the tool polygon. (Figure 1, C) The root length was measured from the CEJ to the apex, (Figure 1, D) and finally two different volumes of cones were calculated per tooth with a mathematical formula.
Part C. Automatic segmentation and different setting parameters combinations
As observed in part A, it is not possible to apply the same combination of setting parameters values to all teeth with automatic segmentation. Taking into account the advantage of this automatic process (16) twenty combinations of different values for all the setting parameters (Table 3) were used to reconstruct the pulp chamber of one lower first molar (FDI 36, Male 23 year old Malaysian origin, slice thickness 0.2mm) and an upper canine (FDI 23, Male 31 year old Colombian origin). The volumetric reconstruction with each combination was completed twice per tooth. The variation among the obtained volume from the same tooth was calculated.
Statistical analysis
Shapiro Wilk normality test, mean, standard deviation (SD), paired t-Test and Pearson correlation coefficient, were calculated to compare the results obtained using the different segmentation methods (Part A), cone shape volume approach (Part B), and the obtained results when different parameters are used to do the automatic segmentation of the same tooth (Part C).
RESULTS
Part A. Automatic and manual segmentation
Three data-sets were obtained from the volumetric reconstruction of the root canal of the canines using the different methods (Table 1).
When automatic and manual segmentation using each fourth slice were compared, the Pearson’s correlation coefficient (r=0.83), shows a greater correlation between them, than between automatic and manual segmentation using only the first and the last slice (r=0.75) or between the two manual segmentation methods (r=0.79). However, this does not mean that manual segmentation using every fourth slice and automatic segmentation produce comparable results. The paired t test shows that there is a statistically significant difference between the means of the results of both manual segmentations and automatic segmentation (p<0.001).
When comparing the obtained volumes, it was observed that manual segmentation produced volumes that are larger than those obtained with automatic segmentation. To facilitate the understanding of this difference, a simple mathematical analysis was used, taking the obtained volume with automatic segmentation as 100% of the volume. Then the difference between the volumes obtained with automatic segmentation and both manual segmentation, were used in a rule of three to calculate the percentage this difference represents.
The results of this calculation showed that the volumes obtained using every fourth slice are in average 25% (1%-53%) larger than those obtained with automatic segmentation. Also, that using the first and the last slice are in average 57% (12% to 210%) larger than those obtained with automatic segmentation. The average of the obtained volumes from both manual segmentation methods is in general 41% larger than automatic segmentation.
The volumes obtained doing manual segmentation of each fourth slice were in average 28% larger than those obtained using only the first and the last slice. However, some of them were in average 16% smaller (p>0.05). The mathematical analysis was like the previously described, but in this case, the volume obtained with manual segmentation using only the first and last slice was taken as 100% in the rule of three.
Part B. Cone shape geometric approximation
It was expected to obtain similar area and volume values when using ovals of best fit and the tool polygon following the outline of the pulp chamber. Different than expected, it was observed that with the tool polygon the obtained areas and volumes were noticeably larger (50%) than with the ovals (Table 2). However, there is a strong correlation coefficient between both measured areas using the tools oval and polygon (r=0.84) at the CEJ and the obtained volumes (r=0.88).
When the obtained areas using the two different tools are compared the data show a big variability and a high SD, this effect is diminished once the volume is calculated. In this way, the length of the root is what really determines the final obtained volume.
Part C. Automatic segmentation and different setting parameters combinations
Repeatability of the automatic segmentation for the first and the second repetition for both teeth was evaluated with the paired t test (r=0.7, p=0.99) showing that there is no statistically difference between both repetitions with a 95% level of confidence. The average between the obtained volumes in both repetitions was calculated. The volumes obtained for the molar pulp chamber (FDI 36), ranged from 31.7mm3 to 53.74mm3, with a SD of 5.7and a variance of 33.
For the volumetric reconstruction of the canine (FDI 23), the volume value ranged between 29.8 mm3 to 50.8 mm3, SD=7.12 and variance of 50.75. The SD for the different parameters was not bigger than 0.6 and the sample variance was not greater than 0.3
DISCUSSION
With the introduction of computer vision techniques for medical imaging and their application in dentistry and forensic sciences, the possibilities to propose methods for age and sex estimation are almost unlimited. Owed to the apposition of secondary dentine, the anthropometric assessment of the variation in the ratio between size of the pulp chamber and size of the tooth is still an acceptable dental age predictor. (14) The aim of this study was to test the variability of the volume measurements when different segmentation methods are applied in pulp volume reconstruction, because although it would be expected that with volume measurements the results for age estimation were more reliable, the literature shows the opposite. To find out an explanation to the lower accuracy of the methods based on volume reconstruction, in this study we tested three different methods doing only pulp volume reconstruction.
The methodology analysed in this study, using CBCT, seems to be no more accurate than those methods based on radiographs for dental age estimation in adults, regardless the sample size of the study which ranges from 19 individuals, analysing only 12 canines (7) to 403 individuals analysing only the pulp chamber of first molars. (14) This is clear when the reported accuracy of the different methods is compared. The reported mean absolute error using automatic segmentation of the first molar’s pulp chamber is 6.26 years at best. (14) The cone shape geometric approach of pulp and tooth has a standard error of estimation of ± 11.45 years, (13) and finally, manual segmentation of pulp and tooth, has a prediction interval of ± 12 years. (5)
Other methods also using automatic segmentation of canines reported a prediction interval of 3.47 years at best. (17) When these reported results are compared with some of the most commonly used adult age estimation methods utilising dental radiographs, such as Cameriere et al. (3) (with reported mean predictor errors of 2.37 years (18) to 11.01 years (19) (tooth/pulp area ratio)), or the method developed by Kvaal et al. (2) (pulp/tooth-linear measurements ratios with reported standard estimation errors of ±9.367 years, (20)) it is possible to observe that the use of CBCT and dental structures volume reconstruction, do not improve the final results for adult age estimation. The relation between the lack of the accuracy of the mentioned methods for age estimation and the different methods for volume reconstruction are presented as follow:
Part A. Manual and automatic segmentation may produce similar results, as observed in this study (r=0.83). Manual segmentation is time consuming, difficult to perform and prone to be influenced by the subjectivity of the observer, and personnel trained in this aspect is necessary. (21) Additionally, it is not accurate enough to estimate the variation of the volume in small anatomic structures, such as the root canal, as observed in this study. Although there are different methods for automatic image segmentation, the first problem faced in the bio-medical area, is the exclusive dependence on gradient or intensity analysis without using anatomical information. (21) In the case of automatic segmentation, with ITK-SNAP software, although the software chooses which pixels will be included in the segmentation, the observer finally decides how to adjust the parameters to control the algorithms in the segmentation, making this method prone to a certain degree of subjectivity from the observers. These parameters may change from one CBCT to another. Unfortunately, in the previous study using this software the values of the setting parameters were not mentioned. (14) In this study it was also observed that although all the CBCT were obtained from machines with the same reference, and under similar exposure conditions (slice thickness, Kv, mA and time of exposure), and the same parameters for automatic segmentation, the interaction of the seed region-growing with the boundaries of the structure to reconstruct may also differ from one CBCT to another. For this reason, it is not possible to follow the recommendations of the ITK-SNAP manufacturer, who recommends to keep the same parameters among different CBCT, and it is neither possible to guarantee the uniformity of the segmentations obtained. (14)
In this study, we also observe that small changes in the values of the setting parameters can generate significant variation in the final obtained volumes with automatic segmentation, even though the segmentation was made on the same CBCT, same tooth and same anatomic region.
Which means that the final volume will be always the same under the same parameters in the same CBCT and anatomic region, but these parameters generally need to be modified from one CBCT to another, and in the same way, small changes in the parameters alter the final volume.
Part B. With the aim of simplifying the measurement of the tooth structure volume, a cone shape geometric approach was proposed (Part B). (13) The developers of this method were aware of the main disadvantages of this proposal: measurements inaccuracy and subjectivity. They also reported that this method tends to underestimate the real volume of the tooth structures (56% to 67%), which in theory would not affect the final pulp/tooth ratio that was calculated to estimate the age.
To test this method, we used two differ approaches for doing the volume calculation. The first, following the published methodology (13) displaying ovals at the CEJ, and a second one selecting manually the outline of the root canal at the CEJ, using the tool polygon. As observed in the results section, despite the difference between both area measurements, at the CEJ, once the volume is calculated the difference decreases. Neither of these two approaches is recommended to carry outpulp volume measurements,, firstly because of the subjectivity of the observer, who only counts with the naked eye to display one or another and secondly, because both bring a distorted representation of the root canal, ignoring the different variations in its internal shape.
Part C. In this study, it has been shown, that there are different parameters that affect the final volumetric reconstruction of any anatomical region. The scale of Gaussian, or blurrier factor (22) was found to be the most relevant when doing automatic segmentation. To increase the value of the Gaussian scale, allows the observer to eliminate certain noises in the image, which affect the “growing of the seed”. However, the bigger the value the Gaussian scale is, the more principal structures and details will be lost. (23) This would mean that the initial volume of the pulp chamber will be magnified. (16)
Although automatic segmentation is less prone to the subjectivity of the observer than manual segmentation, in this study we observed that it is not possible to keep the same volume reconstruction parameters for all the CBCT, and that minimum changes may produce significant variations even though they are done on the same tooth. The volume obtained with this tool must be understood as an approximation to the real volume of the structure being measured
Taking into consideration the reported rate of secondary dentin formation is 6.5 μm/year for the crown and 10 μm/year for the root, (24) the analysed methods in this study are not sensitive enough to detect such small dimension changes, generating a big variation of the measurements, which could explain the greater error of pulp/tooth volume based methods for age estimation when compared with simpler methods based on linear (2) or area measurements (3) on dental radiographs.
Previous research in the biomedical area have highlighted the problems related to semi-automatic segmentation, and specifically, to the process that the software uses to select which pixels or voxels to be included in the final volume reconstruction. To overcome this problem, they have elaborated the probabilistic anatomic atlas, which facilitates the segmentation of an organ of interest. (21) When doing the semi-autographic segmentation of teeth and pulp chambers, different obstacles were observed. Firstly, owing to the similar density of dentine and bone and the irregularity of the periodontal ligament, it was not possible to obtain a volumetric reconstruction of the tooth as it is in for the pulp chamber. This is the reason why the automatic tooth volume reconstruction was not analysed. Secondly, owing to the large variety in the shape of the pulp chamber in the apical third of the tooth, there was always a leak of the seed region -growing in to the dentine. To create a probabilistic atlas for dentistry could help to overcome these issues, and help the dentist and forensic dentist to implement more accurate and easier methods for automatic segmentation and volume reconstruction. Thirdly, although the automatic reconstruction of the pulp chamber of molars may be understood as a simple process, it may be more reliable to use other methods for age estimation when using molars.
CONCLUSION
Based on the results of this study, it is possible to affirm that the obtained volume measurements with any segmentation method must be understood as an approximation of the measured structure and not as the real volume. In the same way, manual segmentation could produce volume values that are even more inaccurate, and should be avoided in future studies.
Although the volumetric reconstruction and P/T volume ratio has not shown better results than methods based on dental radiographs, it is worth to persevere with the research in this area with an interdisciplinary team to build software that can reliably reconstruct pulp and tooth volumes for forensic purposes.
ACKNOWLEDGEMENTS
The authors of the study want to thank to Nurul Firdaus, Dr Shahida Mohd Said and Dr Shalini Kanagasingam from the Radiology Unit, Dental Faculty University of Kebangsaan Malaysia. To the Forensic Science Centre from The University of Western Australia and to the research group INVIENDO from the National University of Colombia.
Footnotes
CONFLICT OF INTEREST: The authors declare that they have no conflict of interest.
REFERENCES
- 1.Gustafson G. Age determination on teeth. J Am Dent Assoc. 1950;41(1):45–54. 10.14219/jada.archive.1950.0132 [DOI] [PubMed] [Google Scholar]
- 2.Kvaal SI, Kolltveit KM, Thomsen IO, Solheim T. Age estimation of adults from dental radiographs. Forensic Sci Int. 1995;74(3):175–85. 10.1016/0379-0738(95)01760-G [DOI] [PubMed] [Google Scholar]
- 3.Cameriere R, Ferrante L, Cingolani M. Variations in pulp/tooth area ratio as an indicator of age: a preliminary study. J Forensic Sci. 2004;49(2):317–9. 10.1520/JFS2003259 [DOI] [PubMed] [Google Scholar]
- 4.Vandevoort FM, Bergmans L, Van Cleynenbreugel J, Bielen DJ, Lambrechts P, Wevers M, et al. Age calculation using X- ray microfocus computed tomographical scanning of teeth: a pilot study. J Forensic Sci. 2004;49(4):787. 10.1520/JFS2004069 [DOI] [PubMed] [Google Scholar]
- 5.De Angelis D, Gaudio D, Guercini N, Cipriani F, Gibelli D, Caputi S, et al. Age estimation from canine volumes. Radiol Med (Torino). 2015;•••:731–6. [DOI] [PubMed] [Google Scholar]
- 6.Paewinsky E, Pfeiffer H, Brinkmann B. Quantification of secondary dentine formation from orthopantomograms—a contribution to forensic age estimation methods in adults. Int J Legal Med. 2005;119(1):27–30. 10.1007/s00414-004-0492-x [DOI] [PubMed] [Google Scholar]
- 7.Yang F, Jacobs R, Willems G. Dental age estimation through volume matching of teeth imaged by cone-beam CT. Forensic Sci Int. 2006;159 Suppl 1:S78–S83. 10.1016/j.forsciint.2006.02.031 [DOI] [PubMed] [Google Scholar]
- 8.Oi T, Saka H, Ide Y. Three-dimensional observation of pulp cavities in the maxillary first premolar tooth using micro-CT. Int Endod J. 2004;37(1):46–51. 10.1111/j.1365-2591.2004.00757.x [DOI] [PubMed] [Google Scholar]
- 9.Agematsu H, Someda H, Hashimoto M, Matsunaga S, Abe S, Kim H-J, et al. Three-dimensional Observation of Decrease in Pulp Cavity Volume Using Micro-CT: Age-related Change. Bull Tokyo Dent Coll. 2010;51(1):1–6. 10.2209/tdcpublication.51.1 [DOI] [PubMed] [Google Scholar]
- 10.Someda H, Saka H, Matsunaga S, Ide Y, Nakahara K, Hirata S, et al. Age estimation based on three-dimensional measurement of mandibular central incisors in Japanese. Forensic Sci Int. 2009;185(1–3):110–4. 10.1016/j.forsciint.2009.01.001 [DOI] [PubMed] [Google Scholar]
- 11.Jagannathan N, Neelakantan P, Thiruvengadam C, Ramani P, Premkumar P, Natesan A, et al. Age estimation in an Indian population using pulp/tooth volume ratio of mandibular canines obtained from cone beam computed tomography. J Forensic Odontostomatol. 2011;29(1):1–6. [PMC free article] [PubMed] [Google Scholar]
- 12.Star H, Thevissen P, Jacobs R, Fieuws S, Solheim T, Willems G. Human Dental Age Estimation by Calculation of Pulp–Tooth Volume Ratios Yielded on Clinically Acquired Cone Beam Computed Tomography Images of Monoradicular Teeth. J Forensic Sci. 2011;56 Suppl 1:S77–82. 10.1111/j.1556-4029.2010.01633.x [DOI] [PubMed] [Google Scholar]
- 13.Pinchi V, Pradella F, Buti J, Baldinotti C, Focardi M, Norelli G-A. A new age estimation procedure based on the 3D CBCT study of the pulp cavity and hard tissues of the teeth for forensic purposes: A pilot study. J Forensic Leg Med. 2015;36:150–7. 10.1016/j.jflm.2015.09.015 [DOI] [PubMed] [Google Scholar]
- 14.Ge ZP, Ma R-h, Li G, Zhang J-z, Ma X-c. Age estimation based on pulp chamber volume of first molars from cone-beam computed tomography images. Forensic Sci Int. 2015;253:133.e1–e7. 10.1016/j.forsciint.2015.05.004 [DOI] [PubMed] [Google Scholar]
- 15.Cameriere R, Ferrante L, Belcastro MG, Bonfiglioli B, Rastelli E, Cingolani M. Age Estimation by Pulp/Tooth Ratio in Canines by Mesial and Vestibular Peri-Apical X-Rays. J Forensic Sci. 2007;52(5):1151–5. 10.1111/j.1556-4029.2007.00530.x [DOI] [PubMed] [Google Scholar]
- 16.Yushkevich PA, Piven J, Hazlett HC, Smith RG, Ho S, Gee JC, et al. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage. 2006;31(3):1116–28. 10.1016/j.neuroimage.2006.01.015 [DOI] [PubMed] [Google Scholar]
- 17.Tardivo D, Sastre J, Catherine J-H, Leonetti G, Adalian P, Foti B. Age determination of adult individuals by three-dimensional modelling of canines. Int J Legal Med. 2014;128(1):161–9. 10.1007/s00414-013-0863-2 [DOI] [PubMed] [Google Scholar]
- 18.Cameriere R, Cunha E, Sassaroli E, Nuzzolese E, Ferrante L. Age estimation by pulp/tooth area ratio in canines: Study of a Portuguese sample to test Cameriere's method. Forensic Sci Int. 2009;193(1-3):128.e1–e6. [DOI] [PubMed] [Google Scholar]
- 19.Babshet M, Acharya AB, Naikmasur VG. Age estimation in Indians from pulp/tooth area ratio of mandibular canines. Forensic Sci Int. 2010;197(1–3):125.e1–e4. [DOI] [PubMed] [Google Scholar]
- 20.Karkhanis S, Mack P, Franklin D. Age estimation standards for a Western Australian population using the dental age estimation technique developed by Kvaal et al. Forensic Sci Int. 2014;235(0):104.e1–e6. 10.1016/j.forsciint.2013.12.008 [DOI] [PubMed] [Google Scholar]
- 21.Dong C, Chen Y-w, Foruzan AH, Lin L, Han X-h, Tateyama T, et al. Segmentation of liver and spleen based on computational anatomy models. Comput Biol Med. 2015;67:146–60. 10.1016/j.compbiomed.2015.10.007 [DOI] [PubMed] [Google Scholar]
- 22.Tschirsich M, Kuijper A. Notes on Discrete Gaussian Scale Space. J Math Imaging Vis. 2015;51(1):106–23. 10.1007/s10851-014-0509-0 [DOI] [Google Scholar]
- 23.Guerrero González N. Segmentación de imágenes empleando el espacio de escala Gaussiano. Diss. Universidad Nacional de Colombia-Sede Manizales.
- 24.Murray PE, Stanley HR, Matthews JB, Sloan AJ, Smith AJ. Age-related odontometric changes of human teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;93(4):474–82. 10.1067/moe.2002.120974 [DOI] [PubMed] [Google Scholar]