

Abstract
Background
Since it was introduced as an Olympic sport in 1998, snowboarding has drawn the participation of individuals of all ages. Despite the growing popularity of this sport, individuals can suffer from a number of musculoskeletal injuries. The specific goals of the study were to: (I) compare the number of injuries and trends of snowboarding injuries; (II) identify the injury occurrences, trends, and incidence of snowboarding-related fractures; and (III) identify the injury occurrences and trends of snowboarding-related fractures by body part.
Methods
The National Electronic Injury Surveillance System (NEISS) database was queried for snowboarding injuries and snowboarding-related fractures treated in US emergency departments (EDs) from 2010–2016. The weighted estimate of the number of injuries were obtained by using the NEISS statistical weight calculations that were provided in the data. An estimated total of 248,388 patients (mean age =20 years) experienced a snowboarding-related injury. Linear regression analysis was used to analyze annual trends of snowboarding-related fractures and the snowboarding-related fractures by body part; reported as the correlation coefficient (r) and the coefficient of determination (R2).
Results
The estimated annual number of injuries decreased from 56,223 injuries in 2010 to 17,667 injuries in 2016 (r=−0.967, R2=0.936, P<0.001). The most common types of injuries were fractures (31.7%), strains/sprains (25.2%), contusions (10.9%), concussions (10.0%), internal injuries (7.2%), and dislocations (4.0%). From 2010 to 2016, the estimated annual number of fractures decreased from 18,757 in 2010 to 4,539 in 2016 (r=−0.978, R2=0.957, P<0.001), and the annual incidence of snowboarding-related fractures decreased by 23.1%. The most common location of snowboarding-related fractures was the upper extremity, more specifically the wrist (32.3%). There was a decrease in the estimated annual number of fractures of the wrist (r=−0.965, R2=0.932, P<0.001), forearm (r=−0.821, R2=0.861, P=0.023), shoulder (r=−0.872, R2=0.760, P=0.011), elbow (r=−0.901, R2=0.813, P=0.006), and lower leg (r=−0.929, R2=0.864, P=0.002).
Conclusions
With the growing popularity of snowboarding in the US, it is important to know the common types of injuries that occur. This study found that fractures were the most common injuries, especially of the upper extremity.
Keywords: Snowboarding, fractures, injuries, trends
Introduction
Snowboarding has grown to be one of the most popular winter sports in the United States (1). It has risen in popularity since its introduction in the 1998 Winter Olympics, and has drawn the participation of individuals at different ages and skill levels (2), having attracted participation from approximately 7.6 million Americans during the 2015–2016 season (1). Moreover, there are a variety of snowboarding styles that have evolved that require an increased level of skill (3). Concomitant with increased participation in the sport, there has been a growth in the injury rates among both recreational and elite snowboarders (4,5).
Many epidemiological studies often focus on identifying injury trends in snowboarding in comparison to skiing (5-7). While these studies have identified upper extremity injuries as the most prevalent among snowboarders, they do not offer a broader understanding of these specific injuries. Other investigations have compared injury patterns between professional and recreational participants of snowboarding, and have found an increase in injury distribution throughout the lower extremity of professional athletes (4,8). While a few studies have focused on examining injuries of specific body regions (2,7), there is paucity of literature that has reported on the most common types of injuries to all body parts, such as fractures, that can be generalized to the public.
Therefore, the purpose of this study was to focus on trends of snowboarding-related injuries in patients who presented to emergency departments (EDs) in the United States. The specific goals of the study were to: (I) compare the number and annual trends of different types of snowboarding injuries; (II) identify the number, annual trends, and incidence of snowboarding-related fractures; and (III) identify the number and annual trends of snowboarding-related fractures for each body part.
Methods
Data source
ED data from snowboarding-related injuries in the United States from 2010 to 2016 were identified and reviewed using the National Electric Injury Surveillance System (NEISS) database. The NEISS database is a national database that is obtained from a sample of approximately 100 hospitals in the United States and its territories, and is managed by the United States Consumer Product Safety Commission (CPSC) (9). Information was collected on all injuries that presented to the 100 hospitals that make up the stratified probability sample. The hospitals are grouped into five strata, of which four are based on the hospital size (i.e., annual number of ED visits), and one that is comprised of children’s hospitals. The CPSC performs annual sampling frames of all hospitals that have ED’s in the United States, including the total number of ED visits. Data for each case collected from NEISS hospitals are assigned a sample weight that is determined by the inverse of the probability of selection for the hospitals in each stratum. Adjustments are made to these data to make sure that hospitals comply with required specifications, and new sampling frames are used to ratio-adjust the sample’s statistical weights for the present sample of NEISS hospitals to more accurately represent the total number of annual ED visits for the entire United States population (10). The ratio adjustment is the ratio of the known total number of hospital ED visits in a population frame over the estimated total ED visits in the sample of hospitals (11). At each hospital, the variables that are collected include age, sex, race, date, diagnosis category, body part injured, injury location, disposition, and a narrative field for describing the injury (11).
Patient selection
The NEISS database was queried for all patients who were between the ages of 2 and 81 years and presented to the ED with a snowboarding-related injury (NEISS Manual, product code 5031) between January 1, 2010 and December 31, 2016. The weighted estimate of the number of injuries was obtained by using the NEISS statistical weight calculations included within the data.
Study population
An estimated total of 248,388 patients experienced a snowboarding-related injury. The sample included 182,498 (73.5%) men and 65,890 (26.5%) women who had a mean age of 20±8.87 years, with a racial distribution of 73.8% White, 2.4% Asian, 1.9% Other (predominantly Hispanic), 1.0% Black, 0.1% American Indian, 0.1% Native Hawaiian, and 20.7% were missing the race category. Patients between the ages of 10 and 19 years accounted for the highest proportion of injuries (51.4%).
Outcomes
The outcomes studied were the estimated number and annual trends of snowboarding-related injuries, and number, annual trends, and estimated incidence of snowboarding-related fractures, and the number and annual trends of the most commonly affected body parts for snowboarding-related fractures. The sum of the weighted values provided in the NEISS database was used to determine the number of the injuries, and allowed us to estimate the annual trends and incidence of snowboarding-related fractures and the annual trends of the body parts affected by snowboarding-related fractures.
Data analysis
All of the data was compiled in an excel spreadsheet (Microsoft Corporation, Redmond, Washington, USA). Data was analyzed using SPSS version 24 (IBM Corporation, Armonk, New York, USA). A P value of less than 0.05 was the threshold for statistical significance. Descriptive statistics were performed and reported as frequencies and percentages or means and standard deviations. A linear regression analysis was performed to analyze annual trends of snowboarding-related fractures and the snowboarding-related fractures by body part; this was reported as the correlation coefficient (r) and the coefficient of determination (R2).
Results
Snowboarding-related injuries
The sample contained an estimated total of 248,388 snowboarding-related injuries that presented to EDs in the United States from 2010 to 2016. The estimated annual number of injuries decreased from 56,223 injuries in 2010 to 17,667 injuries in 2016 (r=−0.967, R2=0.936, P<0.001) (Figure 1). The most common types of injuries were fractures (31.7%), strains and sprains (25.2%), contusions (10.9%), concussions (10.0%), internal organ injuries (7.2%), and dislocations (4.0%) (Figure 2).
Figure 1.
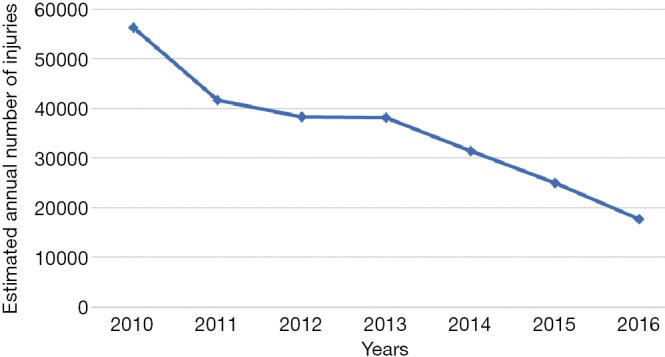
Trends of all snowboarding-related injuries.
Figure 2.
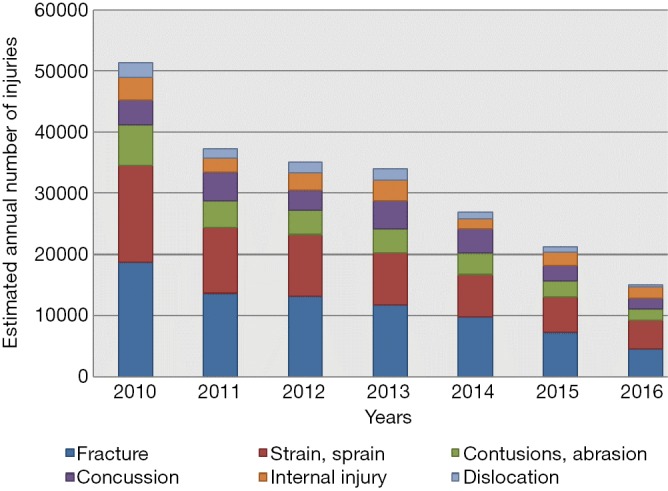
Snowboarding-related injury trends from 2010 to 2016 for six most common injury types.
Snowboarding-related fractures
There were an estimated total of 78,920 snowboarding-related fractures that presented to the ED from 2010 to 2016. The estimated annual number of snowboarding-related fractures decreased from 18,757 in 2010 to 4,539 in 2016 (r=−0.978, R2=0.957, P<0.001). The annual snowboarding-related fracture incidence decreased by 23.1%, from 33.4% in 2010 to 25.7% in 2016.
Snowboarding-related fractures by body part
The most common locations of snowboarding-related fractures were identified to be the wrist (32.3%), forearm (22.5%), shoulder (19.3%), elbow (3.9%), upper trunk (3.7%), upper arm (3.6%), lower leg (2.8%), and the lower trunk (2.5%) (Table 1). From 2010 to 2016, there were significant decreases in the estimated annual number of snowboarding-related fractures of the wrist (r=−0.965, R2=0.932, P<0.001), forearm (r=−0.821, R2=0.861, P=0.023), shoulder (r=−0.872, R2=0.760, P=0.011), elbow (r=−0.901, R2=0.813, P=0.006), and lower leg (r=−0.929, R2=0.864, P=0.002). However, the estimated annual number did not significantly change for snowboarding-related fractures of the upper trunk (r=−0.585, R2=0.342, P=0.168), upper arm (r= −0.439, R2=0.193, P=0.324), and lower trunk (r=−0.626, R2=0.394, P=0.132) (Figure 3).
Table 1. Estimated number of snowboarding-related fractures of different body parts.
| Body location | Number (%) |
|---|---|
| Wrist | 25,469 (32.3) |
| Forearm | 17,781 (22.5) |
| Shoulder | 15,267 (19.3) |
| Elbow | 3,082 (3.9) |
| Upper trunk | 2,959 (3.7) |
| Upper arm | 2,833 (3.6) |
| Lower leg | 2,211 (2.8) |
| Lower trunk | 1,977 (2.5) |
| Ankle | 1,806 (2.3) |
| Hand | 1,392 (1.8) |
| Finger | 1,418 (1.8) |
| Face | 833 (1.1) |
| Foot | 581 (0.7) |
| Knee | 405 (0.5) |
| Upper leg | 458 (0.6) |
| Neck | 184 (0.2) |
| Head | 125 (0.2) |
| Toe | 75 (0.1) |
| Pubic region | 64 (0.1) |
Figure 3.
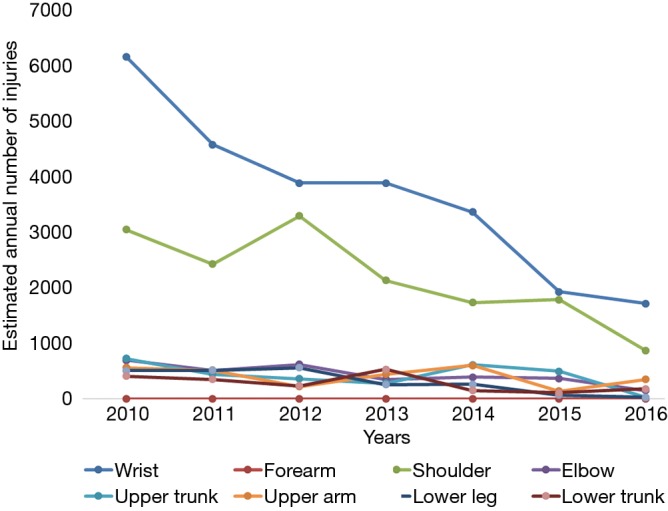
Annual trends of the most common snowboarding-related fractures.
Discussion
Snowboarding has consistently attracted increased participation by millions of Americans over the last 30 years. As is the case with skiing, the inherent nature of snowboarding predisposes participants to an increased risk of various musculoskeletal injuries with unique injury patterns. Several studies have compared the injury patterns of snowboarding and skiing, yet few recent studies have attempted to examine the incidence and trends of snowboarding-related fractures within the United States population. The present study found that from 2010 to 2016, there was an overall decrease in snowboarding-related injuries. Additionally, the most prevalent types of injuries were fractures involving the upper extremity; specifically, the wrist, forearm, and shoulder.
There were several limitations to this study. The NEISS database employs a probability model to extrapolate injury trends within the population based on data from a collection of EDs in the United States. The database was compiled by sampling a fixed number of hospitals and using these samples to generate a weighted approximation of the total number of injuries for the population. This data may lead to inaccurate injury estimates because the data must be ratio-adjusted based on the hospitals used for the sample to create valid statistical weights. However, this process of sampling hospitals throughout the United States may permit this study’s findings to be more applicable to the general population. Additionally, the database cannot account for injuries that were seen or addressed outside of the ED, such as patients who were seen at outpatient clinics or by their primary care physicians. As with any large dataset, the NEISS database may also be subject to errors in data collection or entry. Despite these limitations, the findings of this study provide snowboarding participants with pertinent information that may help identify trends and rates of activity-related injuries, and might contribute to measures to further reduce the incidence of snowboarding-related injuries.
The decreased rate of snowboarding-related injuries that presented to hospital EDs noted in this study may be due to snowboarders receiving better training lessons, or also may be a result of ski resorts having on-site clinics, which may decrease the number of patients who are seen in the ED (12). The results of the present study are in accordance with prior studies that reported on snowboarding-related injuries, which have shown fractures to be the most commonly encountered types of injuries (13,14). Yamagami et al. (14) reported on 3,102 snowboarding-related injuries that occurred across 5 different resorts from 1992 to 1999, and found that 998 injuries (32.1%) were fractures. Additionally, they reported that 625 (62%) of the fractures were fractures of the upper extremity. Idzikowski et al. (13) surveyed injuries from 47 medical facilities near Colorado ski resorts and showed that of 7,430 snowboarding-related injuries, 3,645 (49.06%) were upper extremity injuries and 56.43% of these were fractures. Moreover, several studies have reported that wrist injuries were the most common type of injury associated with snowboarding (5,15). Kim et al. (5) collected injury data from 1988 to 2006 from a base-lodge clinic in Vermont and found that wrist injuries accounted for 27.6% of all snowboarding injuries. In another study, Basques et al. (15) used the National Trauma Data Bank and identified 2,704 snowboarders who presented to EDs between 2011 and 2012, and found that most common injuries were upper extremity fractures, which accounted for 26% of injuries, particularly of the distal radius, which accounted for 10.5% of injuries. Machold et al. (16) surveyed a group of snowboarders who had a mean age of 15 years, and found that 6% of snowboarders had a mean of 10.6 injuries per 1,000 snowboard days, where 61% of the injuries affected the upper extremity, particularly the wrist, which accounted for 32% of the injuries. Similarly, Bladin et al. (17) reported on the injury profile of snowboarding and found that wrist injuries contributed to 22% of all snowboarding injuries. Dohjima et al. (18) reported on a total of 2,552 snowboarding injuries that occurred in patients who had a mean age of 23 years and found that the most common injuries were fractures (39%), and the most likely injured area was the upper extremity (77%), and the radius accounted for 48% of fractures. Additionally the results of the present study corroborate those found by Sacco et al. (19), who described a total of 40 snowboarders who presented to a trauma center over a 6-year period, and found that upper extremity injuries were the most common injuries and accounted for 24% of the snowboarding-related injuries. For snowboarders, injuries to the upper extremity have been reported to be more common than lower extremity injuries, and may be related to the feet being attached to a single board; when falls occur, the natural reaction is to protect oneself with one’s hands/arms, which could result in upper extremity injuries (5,20).
The results of our study are in contrast to those that have shown higher snowboarding-related injury rates for body parts other than the upper extremity. Major et al. (21) described a cohort of 1,432 snowboarders who had a total of 574 injuries that occurred over a period of 6 years, and they found that the most commonly injured body part was the knee (18%). However, their study focused only on elite World Cup snowboarders, whereas the present study evaluated injury incidence at a national level, without level of skill taken into consideration. In another study, Prall et al. (22) reported on 37 consecutive patients who had severe snowboarding injuries, and found that head injuries were the most common injuries (54%). Yet these injuries were all defined as severe injuries, all of which warranted referral to a level I trauma center, as opposed to the larger demographic/representation of hospital and ED sizes included in this study, which may not receive injuries of such severity. Also, Bladin et al. (23) reported on a total of 276 snowboarding injuries that occurred over a 4-year period in patients who had a mean age of 21 years, and they found that fractures accounted for 24% of the injuries, and that the most common injuries were to the knee (23%) and foot/ankle (23%). This investigation did not report on the race of included patients, which along with the reliance on data from only three ski resort medical centers, may have biased these results. Wasden et al. (24) reported on a total of 348 snowboarding injuries that occurred in patients who had a mean age of 23 years who presented to the ED over a 6-year period, and they found that the most common types of injuries involved the head (27.3%), lower extremities (26.2%), abdomen/pelvis (22.4%), and the spine (20.7%). The higher rate of head, abdomen/pelvis, and spine injuries found in their study differed from the present study, and may also be related to their study being performed at a level I trauma center.
Conclusions
Snowboarding is one of the most popular winter sports in America and has grown in popularity over the past two decades. The increased participation in this sport has led to a substantial number of snowboarding-related injuries. However, the incidence of snowboarding-related injuries seen in United States EDs has declined from 2010 to 2016. Additionally, the most common snowboarding-related injuries seen in the ED were fractures, with fractures of the upper extremity being most likely, particularly of the wrist, which was most commonly fractured. Further studies should explore strategies to reduce the risk of upper extremity fractures in snowboarding through safer techniques or improved safety equipment. This study has demonstrated an overview of the most common snowboarding-related injuries, and may provide the foundation upon which preventative measures can be developed.
Acknowledgements
None.
Ethical Statement: This study used publicly available de-identified data that was exempt by the hospital’s Institutional Review Board.
Footnotes
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- 1.SIA Snow Sports Industry Insights Study. SnowSports Ind Am Res 2017. Available online: https://www.snowsports.org/sia-research-industry-insights-study/
- 2.McCall D, Safran MR. Injuries about the shoulder in skiing and snowboarding. Br J Sports Med 2009;43:987-92. 10.1136/bjsm.2009.068767 [DOI] [PubMed] [Google Scholar]
- 3.Steenstrup SE, Bakken A, Bere T, et al. Head injury mechanisms in FIS World Cup alpine and freestyle skiers and snowboarders. Br J Sports Med 2018;52:61-9. 10.1136/bjsports-2017-098240 [DOI] [PubMed] [Google Scholar]
- 4.Ehrnthaller C, Kusche H, Gebhard F. Differences in injury distribution in professional and recreational snowboarding. Open Access J Sports Med 2015;6:109-19. 10.2147/OAJSM.S78861 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kim S, Endres NK, Johnson RJ, et al. Snowboarding injuries: trends over time and comparisons with alpine skiing injuries. Am J Sports Med 2012;40:770-6. 10.1177/0363546511433279 [DOI] [PubMed] [Google Scholar]
- 6.Xiang H, Kelleher K, Shields BJ, et al. Skiing- and snowboarding-related injuries treated in U.S. emergency departments, 2002. J Trauma 2005;58:112-8. 10.1097/01.TA.0000151270.26634.DD [DOI] [PubMed] [Google Scholar]
- 7.DeFroda SF, Gil JA, Owens BD. Epidemiology of lower extremity injuries presenting to the emergency room in the United States: Snow skiing vs. snowboarding. Injury 2016;47:2283-7. 10.1016/j.injury.2016.07.005 [DOI] [PubMed] [Google Scholar]
- 8.Wijdicks CA, Rosenbach BS, Flanagan TR, et al. Injuries in elite and recreational snowboarders. Br J Sports Med 2014;48:11-7. 10.1136/bjsports-2013-093019 [DOI] [PubMed] [Google Scholar]
- 9.National electronic injury surveillance system (NEISS). United States Consum Prod Saf Comm 2016. Available online: https://www.cpsc.gov/Research--Statistics/NEISS-Injury-Data
- 10.NEISS. The National Electronic Injury Surveillance System A Tool for Researchers. Div Hazard Inj Data Syst US Consum Prod Saf Comm 2000:1-38. [Google Scholar]
- 11.Schroeder T, Ault K. The NEISS sample (design and implementation) 1997 to Present. Washington, DC: US Consumer Product Safety Commission, 2001. [Google Scholar]
- 12.Patrick E, Cooper JG, Daniels J. Changes in Skiing and Snowboarding Injury Epidemiology and Attitudes to Safety in Big Sky, Montana, USA: A Comparison of 2 Cross-sectional Studies in 1996 and 2013. Orthop J Sports Med 2015;3:2325967115588280. 10.1177/2325967115588280 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Idzikowski JR, Janes PC, Abbott PJ. Upper extremity snowboarding injuries. Ten-year results from the Colorado snowboard injury survey. Am J Sports Med 2000;28:825-32. 10.1177/03635465000280061001 [DOI] [PubMed] [Google Scholar]
- 14.Yamagami T, Ishihara H, Kimura T. Clinical features of snowboarding injuries. J Orthop Sci 2004;9:225-9. 10.1007/s00776-004-0776-5 [DOI] [PubMed] [Google Scholar]
- 15.Basques BA, Gardner EC, Samuel AM, et al. Injury patterns and risk factors for orthopaedic trauma from snowboarding and skiing: a national perspective. Knee Surg Sports Traumatol Arthrosc 2016. [Epub ahead of print]. 10.1007/s00167-016-4137-7 [DOI] [PubMed] [Google Scholar]
- 16.Machold W, Kwasny O, Gässler P, et al. Risk of injury through snowboarding. J Trauma 2000;48:1109-14. 10.1097/00005373-200006000-00018 [DOI] [PubMed] [Google Scholar]
- 17.Bladin C, McCrory P, Pogorzelski A. Snowboarding injuries : current trends and future directions. Sports Med 2004;34:133-9. 10.2165/00007256-200434020-00006 [DOI] [PubMed] [Google Scholar]
- 18.Dohjima T, Sumi Y, Ohno T, et al. The dangers of snowboarding: a 9-year prospective comparison of snowboarding and skiing injuries. Acta Orthop Scand 2001;72:657-60. 10.1080/000164701317269111 [DOI] [PubMed] [Google Scholar]
- 19.Sacco DE, Sartorelli DH, Vane DW. Evaluation of alpine skiing and snowboarding injury in a northeastern state. J Trauma 1998;44:654-9. 10.1097/00005373-199804000-00016 [DOI] [PubMed] [Google Scholar]
- 20.Kirkpatrick DP, Hunter RE, Janes PC, et al. The snowboarder’s foot and ankle. Am J Sports Med 1998;26:271-7. 10.1177/03635465980260021901 [DOI] [PubMed] [Google Scholar]
- 21.Major DH, Steenstrup SE, Bere T, et al. Injury rate and injury pattern among elite World Cup snowboarders: a 6-year cohort study. Br J Sports Med 2014;48:18-22. 10.1136/bjsports-2013-092573 [DOI] [PubMed] [Google Scholar]
- 22.Prall JA, Winston KR, Brennan R. Severe snowboarding injuries. Injury 1995;26:539-42. 10.1016/0020-1383(95)00085-N [DOI] [PubMed] [Google Scholar]
- 23.Bladin C, Giddings P, Robinson M. Australian snowboard injury data base study. A four-year prospective study. Am J Sports Med 1993;21:701-4. 10.1177/036354659302100511 [DOI] [PubMed] [Google Scholar]
- 24.Wasden CC, McIntosh SE, Keith DS, et al. An Analysis of Skiing and Snowboarding Injuries on Utah Slopes. J Trauma 2009;67:1022-6. 10.1097/TA.0b013e3181b0d559 [DOI] [PubMed] [Google Scholar]