

Abstract
Background:
This study aims to assess the impact that physiotherapy (PT) has on the quality of life (QoL) of patients who have undergone coronary artery bypass grafting (CABG) surgery. The objective of this study was to assess the effect of PT on physical and mental aspects of patients’ QoL.
Materials and Methods:
The study population consisted of 50 patients who aged between 60 and 70 years and who had previously undergone CABG surgery. The patients were randomly allocated to two groups: a PT group (n = 25) and a control group (n = 25). The physical characteristics of the participants were recorded at the outset of the study. The patients who were allocated to the PT group completed 16 sessions of classic PT. QoL assessments of all participants were performed before and after the program in the form of a short form-36 health survey. An independent sample t-test and an ANCOVA were performed for the purpose of statistical analyses.
Results:
The QoL scores of the patients (mean age = 62.08 years) who underwent PT significantly improved after the intervention (P < 0.001). A significant difference between groups was observed (P < 0.001) in both the mental component summary and physical component summary variables.
Conclusion:
PT can help relieve pain, reduce depression, help patients more effectively perform the tasks of everyday living, and help ease the symptoms of other disabilities associated with cardiac surgery. In the current study, the implementation of a PT program improved the patient's mental health and increased their QoL.
Keywords: Coronary artery bypass, physiotherapy, quality of life
INTRODUCTION
Physiotherapy (PT) has been commonly employed as a therapeutic approach for many years.[1] PT can improve the response of the autonomic system and as such represents an effective multipurpose technique by which it is possible to recover the normal function of connective tissues and muscles following injury.[2] PT can also reduce pain and prevent overreliance on the use of analgesic medications.[3,4] However, some studies have found that while PT can immediately relieve pain,[5,6] it does not have any significant impact on functional ability.[7,8] As previous research findings have indicated that PT may have a positive impact on cardiovascular injuries,[9] there is a possibility that it may be beneficial for patients who have undergone coronary artery bypass graft (CABG).
The pain and discomfort following CABG can differ from patient to patient. In addition, some patients are required to engage in bed rest following CABG so that their condition can be monitored. Following CABG, patients often report feelings of depression, a lack of patience, a loss of general well-being, and an inability to function at the same level as that enjoyed before the procedure. These feelings, in isolation or combination, can seriously undermine a patient's quality of life (QoL).
Chest PT can be performed using proven clinical PT principles.[10] While it is widely accepted that psychological conditions can have a direct impact on the QoL of patients who have experienced chronic heart failure,[11] researchers have yet to specifically determine the relationship between anxiety, depression, and QoL.
One study examined the impact on PT on the QoL of patients with type 2 diabetes[12] and concluded that this intervention moderately improved the QoL of these patients.[13] The aim of the current study was to evaluate the effect of chest PT on the QoL of postoperative off-pump CABG surgery patients.
MATERIALS AND METHODS
Study design
The study consisted of a randomized placebo-controlled trial that employed a two-arm parallel design through which patients were divided into an intervention and a control group on a 1:1 basis.
Ethical issues
This study was approved by the Local Medical Ethics Committee of Shahid Sadoughi University of Medical Sciences under the ID number 746/G/T. The clinical trial was registered with the Iranian Registry of Clinical Trials (IRCT) and allocated a unique code: IRCT2016010925913N1. All participants signed written informed consent to confirm their agreement to participate in the research.
Participants
All participants in the study had undergone a CABG operation that was performed by the same cardiothoracic surgeon. During the sampling process, the patients who had undergone elective off-pump CABG at the Afshar Cardiovascular Surgery Center in Yazd were screened against the inclusion and exclusion criteria. A total of 50 patients were selected to participate in the study following the application of these screening criteria. Of these, 25 were allocated to the control group, and 25 were allocated to the experimental PT group.
Inclusion and exclusion criteria
Participants who were found to be medically fit to undergone PT postoperatively from March 5, 2016, to April 3, 2016, were included in the initial study population. The inclusion criteria were similar in both groups. Patients were excluded if they experienced chest pain caused by trauma, history of cardiac surgery, chronic pain syndrome, psychiatric disorders, history of taking analgesic drugs, renal failure, and/or prolonged bleeding in excess of 200 cc per h during the hospital stay.
Procedures
A computer-based block randomization list was employed to randomly allocate the participants to the experimental and control group. A block of four was applied in the study. The researchers, patients, and statisticians were blind to the allocation. The participants who were allocated to the experimental group underwent 16 sessions of PT. The techniques were performed by qualified physiotherapists who were experienced in providing PT to patients who have undergone cardiac surgery. The control group did not complete any PT sessions. The medication schedule and diet of the patients in both groups remained unchanged. At the 1-month follow-up session, the participants completed a questionnaire that was designed to evaluate the patients’ QoL.
Intervention
The patients in the PT group underwent 16 sessions of 15-min PT in total: four sessions of PT 2–5 days after surgery and 12 sessions thereafter (3 times a week for 1 month). The methods that were employed to conduct the PT were customized to each individual patient according to his or her psychological, physical, and other underlying conditions. The techniques that were employed with the members of the experimental group included positioning and postural drainage, chest tapotement, coughing (and huffing) exercises, breathing exercises (diaphragmatic breathing, segmental breathing, local expansion, and pursed lip breathing), and thorax mobilization exercises. Patients who had been randomly allocated to the control group received the standard post-CABG surgery care; however, to homogenize the two groups, the patients in the control group completed four 15-min sessions of quiet time in the 2–5 days immediately following surgery.
Outcome measures
Questionnaire
A two-part questionnaire was employed in the current study. Part 1 included questions that were designed to elicit the demographic information of the participants, while part 2 consisted of the standard short form-36 (SF-36) questionnaire that measures QoL via a questionnaire that consists of 36 items. Previous research has found that the statistical difference in self-reported health status between groups is greater than that of the objective health status.[14] The SF-36 questionnaire is designed to measure both physical (physical component summary [PCS]) and mental (mental component summary [MCS]) health constructs. The PCS of the questionnaire includes physical function (PH) (10 questions), physical role (PR) (4 questions), bodily pain (BP) (2 questions), and general health (GH) (5 questions), while the MCS aspect determines vitality (4 questions), social function (SP) (2 questions), emotional role (ER) (3 questions), and mental health (MT) (5 questions) dimensions.[15,16] SF-36 questionnaire refilled three times: after surgery (pretest), before discharge (posttest) and 1-month after discharge (follow-up). Reliability of the questionnaire was calculated by means of alpha Cronbach's coefficient. Reliability coefficient for MCS and PCS was 0.84 and 0.88, respectively. The rest of dimensions are as follows: PH (0.93), MT (0.74), vitality (0.70), PH (0.88), GH (0.73), SP (0.72), BP (0.74), and ER (0.85). Since coefficients for all dimensions were calculated >0.7, this shows an optimal intraclass correlation coefficient for all items which can result in reliability of the questionnaire as well.[17]
Data analysis
SPSS20 software (Statistical Package for the Social Sciences Version 20 SPSS Inc., Chicago, Illinois, USA) was used to analyze the data collated via the questionnaires. An independent-sample t-test and ANCOVA were applied to test the statistical differences between the QoL in control and experimental group A P < 0.05 was considered statistically significant.
RESULTS
Patients’ characteristics
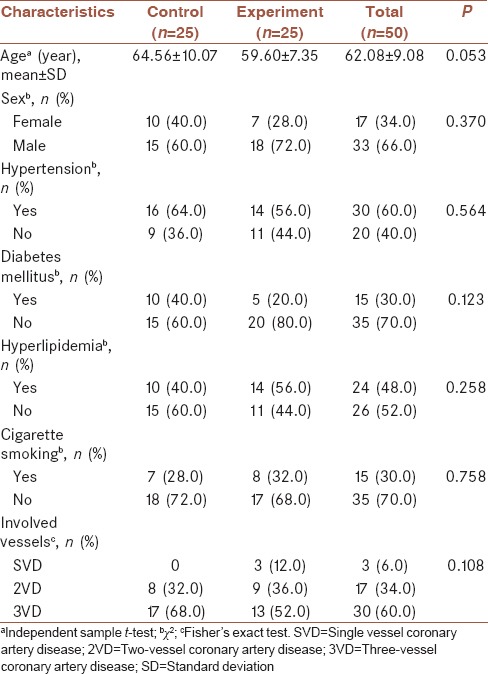
The study population consisted of 50 participants who had undergone elective off-pump CABG. Of these, 25 were allocated to an experimental group that underwent PT, and the remaining 25 were allocated to a control group. The characteristics of the patients are presented in Figure 1. Of the 50 participants, 66% were male (n = 33) and 44% were female (n = 17), and the average age was 62.08 ± 9.08 years. The demographic information and baseline characteristics of both groups are presented in Table 1. There were no statistical differences in terms of the demographic characteristics of the patients in the two groups (P > 0.05). All patients participated for the full duration of the study.
Figure 1.

CONSORT flow diagram
Table 1.
Demographic information of the participants
Outcomes
The PH, PR, BP, GH, vitality, SP, ER, and MT of all participants were measured three times: after surgery (pretest), before discharge (posttest), and 1-month after discharge (follow-up). According to the outcomes of the t-test and ANCOVA, there was a statistical difference in the QoL measures (SF-36) between the two groups. While the QoL scores of the patients in the experimental group increased, those of the control group did not [Table 2].
Table 2.
Comparison of quality of life scales between two groups
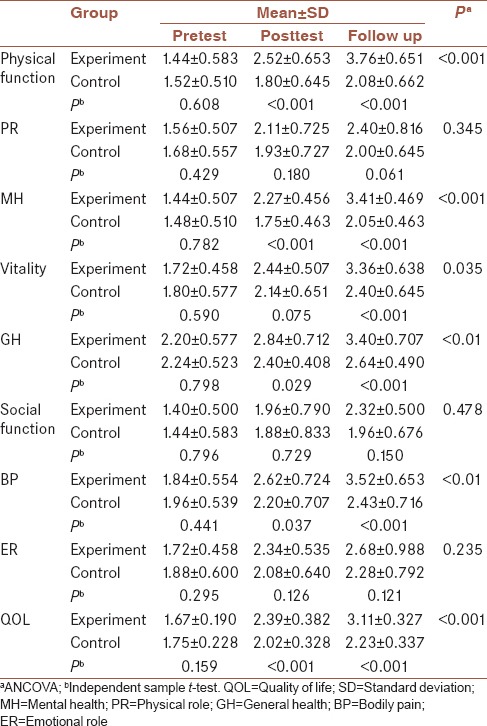
Figure 2a highlights the differences in the SF-36 domains for both groups. The experimental group scored higher on the QoL assessment than the control group after 16 sessions of PT. Within this group, improvements in many domains of the QoL were observed with the exception of PR (P = 0.345), SP (P = 0.478), and ER (P = 0.235). These improvements were sustained until the point of 1-month follow-up. The changes in the QoL scores were statically insignificant for the control group [Figure 2b].
Figure 2.

(a) Spider gram shows differences in short form-36 domains between two groups. PA = Physical function; VT = Vitality; MH = Mental health; PR = Physical role; GH = General health; SP = Social function; BP = Bodily pain; ER = Emotional role; QL = Quality of life. (b) Comparison of two major dimensions of quality of life. PCS = Physical component summary; MCS = Mental component summary; Exp = Experimental; Con = Control
DISCUSSION
A number of research studies have previously examined the clinical effects of PT as a treatment modality for patients who have undergone cardiac surgery.[18,19,20] However, to the best of the researchers’ knowledge, this study represents the first of its kind to examine the effect of PT as a complementary therapy impacts the clinical outcomes of CABG patients. The results outlined above indicate that complementary therapy can be combined with clinical practice to achieve positive results in terms of patient's QoL. Previous research has found that the benefits of PT are not limited to postsurgery; as a treatment intervention strategy, PT can prevent the need for invasive surgery by modulating hypertension or improving the status of cardiac patients.[21,22]
The postintervention QoL scores revealed that a significant improvement was observed in the QoL of the patients who underwent a course of PT after elective CABG surgery. This effect seemed to be related directly to the treatment because most patients reported improvements in their symptoms after 1 month. Furthermore, in the majority of cases, the positive effect of PT was maintained throughout the study period.
In some cases, the patients who underwent PT reported an increase in pain on day 3. This pain may have resulted from the soft-tissue releases and increased mobility after the first session, which subsequently increased achiness and pain the day after. This conclusion indicates that recess PT should potentially be delayed until day 3 or 4 of the hospital stay as opposed to day 2. Deferring PT would also eliminate the need for the physiotherapist to attempt to perform the massage while maneuvering around multiple central intravenous lines and chest drainage tubes. Furthermore, patients are often dazed on postoperative day 2, which minimizes their ability to reap the full benefits of PT intervention. By days 3 and 4, many lines and tubes had been removed, and patients enjoy greater freedom of movement. However, as the reports show, postoperative pain was reported to be chronic[23] and this chronic pain had a negative effect on QoL.[24] However, the intensity and duration of PT sessions must be appropriately controlled. The patients’ ability to engage in social activities was also improved as a result of the therapy.
Other types of PT, such as home-based exercise therapy, have also been found to be effective.[11,25] However, undergoing professional PT sessions is preferable. Patients who wish to continue this treatment could, for example, complete a combination of home-based and professional sessions. This is entirely feasible as the program was completed in a total time of 1 h and did not require the use of expensive equipment. In addition, as PT has been proven to be safe, most patients who have a compromised physical condition could complete the intervention without exhibiting any negative contrary effects.[26] Furthermore, Chen et al. previously reported that back PT can reduce anxiety and increase comfort and physiologic responses in patients suffering from congestive heart failure (CHF).[27] Patients with metastatic bone pain have also benefited from undergoing a course of PT.[28]
The fact that the QoL scores significantly improved following the PT intervention represents an important finding. As our previous studies have found, QoL is an increasingly useful method of assessing the outcome of any surgical intervention. However, information about the QoL outcomes of patients following cardiac surgery is limited due to the lack of studies and variations in how research studies have been designed and implemented. One potential explanation for the lack of focus on QoL following surgery is that QoL is frequently viewed as a “soft” endpoint. Soft endpoints are difficult and subjective to measure.[29,30] Vainiola et al. observed how different factors can explain QoL after cardiac surgery. Pain and restlessness during intensive care unit treatment have a negative impact on QoL scores; as such, these factors should be given appropriate attention during treatment.[31] As the baseline QoL was correlated with follow-up QoL, it was of significance when evaluating the effect different factors had on both the follow-up QoL score and consequently, treatment effectiveness. The follow-up QoL score was adapted for the baseline score.[32]
In the present study, follow-up measurements were taken 1 month after the completion of the PT intervention. A comparison of the pre- and post-treatment SF-36 scale scores revealed an improvement in the QoL of patients. Specifically, those who underwent PT exhibited a significant improvement in QoL following this intervention in comparison to those who received standard care. There is evidence to suggest that the beneficial effects of PT could be sustained over a period of several weeks after a course of treatment. We predict that, in addition to alleviating pain and improving the symptoms of patients following elective CABG surgery, PT also has a positive impact on QoL.
Limitations and suggestions
Further clinical studies that include larger populations of patients undergoing elective CABG surgery are recommended to confirm the positive correlation between PT interventions and QoL identified in this study. Besides the small sample size, the current study had some limitations. It is difficult to confirm that the improvement in QoL of the patients in the experimental group was solely attributable to the PT alone or was the result of the combined effects of PT and the conventional rehabilitation program. A further limitation of the current study was that it was difficult to coordinate the 1-month follow-up assessments of all the patients who participated in this study. In addition, further studies are required that confirm the safety and efficacy of PT as an adjustable rehabilitation tool for patients who have undergone elective CABG or those suffering from certain conditions such as CHF or chronic obstructive pulmonary disease.
CONCLUSION
The findings of the current research indicated that PT is an impressive complementary therapy that demonstrates good tolerability. Treating patients who had undergone elective CABG surgery with PT over a period of 4 consecutive weeks increased their QoL, as indicated by improvements in the SF-36 scale scores. As such, there is strong evidence to suggest that the application of PT in combination with standard care represents a simple, yet highly effective and noninvasive, technique that reduces pain and negative symptoms and increases QoL in cardiac surgery patients without any contrary effects.
Financial support and sponsorship
Vice-chancellor for Research of Shahid Sadoughi University of Medical Sciences, Yazd, Iran, supported the study.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
This study was supported by Shahid Sadoughi University of Medical Sciences, Yazd, Iran. We would like to thank the AndishehNik ICU nurses and all the study participants for their participation and the Afshar Hospital Research Committee.
REFERENCES
- 1.Stockton J. The history of massage and physiotherapy in the royal navy. Physiotherapy. 1994;80:40A–2A. [Google Scholar]
- 2.Luedecke U. History, basis and techniques of connective tissue massage. Aust J Physiother. 1969;15:141–8. doi: 10.1016/S0004-9514(14)61083-7. [DOI] [PubMed] [Google Scholar]
- 3.Silva Gallo RB, Santana LS, Jorge Ferreira CH, Marcolin AC, Polineto OB, Duarte G, et al. Massage reduced severity of pain during labour: A randomised trial. J Physiother. 2013;59:109–16. doi: 10.1016/S1836-9553(13)70163-2. [DOI] [PubMed] [Google Scholar]
- 4.van den Dolder PA, Roberts DL. Six sessions of manual therapy increase knee flexion and improve activity in people with anterior knee pain: A randomised controlled trial. Aust J Physiother. 2006;52:261–4. doi: 10.1016/s0004-9514(06)70005-8. [DOI] [PubMed] [Google Scholar]
- 5.Brosseau L, Wells GA, Tugwell P, Casimiro L, Novikov M, Loew L, et al. Ottawa panel evidence-based clinical practice guidelines on therapeutic massage for neck pain. J Bodyw Mov Ther. 2012;16:300–25. doi: 10.1016/j.jbmt.2012.04.001. [DOI] [PubMed] [Google Scholar]
- 6.Brosseau L, Wells GA, Poitras S, Tugwell P, Casimiro L, Novikov M, et al. Ottawa panel evidence-based clinical practice guidelines on therapeutic massage for low back pain. J Bodyw Mov Ther. 2012;16:424–55. doi: 10.1016/j.jbmt.2012.04.002. [DOI] [PubMed] [Google Scholar]
- 7.Kong LJ, Zhan HS, Cheng YW, Yuan WA, Chen B, Fang M, et al. Massage therapy for neck and shoulder pain: A systematic review and meta-analysis. Evid Based Complement Alternat Med 2013. 2013:613279. doi: 10.1155/2013/613279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.van den Dolder PA, Ferreira PH, Refshauge KM. Effectiveness of soft tissue massage and exercise for the treatment of non-specific shoulder pain: A systematic review with meta-analysis. Br J Sports Med. 2014;48:1216–26. doi: 10.1136/bjsports-2011-090553. [DOI] [PubMed] [Google Scholar]
- 9.Yang X, Zhao H, Wang J. Chinese massage (Tuina) for the treatment of essential hypertension: A systematic review and meta-analysis. Complement Ther Med. 2014;22:541–8. doi: 10.1016/j.ctim.2014.03.008. [DOI] [PubMed] [Google Scholar]
- 10.Cassar MP. 2nd ed. UK: Elsevier Churchill Livingstone; 2004. Handbook of Clinical Massage: A Complete Guide for Students and Practitioners. [Google Scholar]
- 11.Chien CL, Lee CM, Wu YW, Wu YT. Home-based exercise improves the quality of life and physical function but not the psychological status of people with chronic heart failure: A randomised trial. J Physiother. 2011;57:157–63. doi: 10.1016/S1836-9553(11)70036-4. [DOI] [PubMed] [Google Scholar]
- 12.Wändell PE, Carlsson AC, Gåfvels C, Andersson K, Törnkvist L. Measuring possible effect on health-related quality of life by tactile massage or relaxation in patients with type 2 diabetes. Complement Ther Med. 2012;20:8–15. doi: 10.1016/j.ctim.2011.09.007. [DOI] [PubMed] [Google Scholar]
- 13.Wändell PE. Quality of life of patients with diabetes mellitus. An overview of research in primary health care in the nordic countries. Scand J Prim Health Care. 2005;23:68–74. doi: 10.1080/02813430510015296. [DOI] [PubMed] [Google Scholar]
- 14.Angel R, Gronfein W. The use of subjective information in statistical models. Am Sociol Rev. 1988;53:464–73. [Google Scholar]
- 15.Antonescu I, Carli F, Mayo NE, Feldman LS. Validation of the SF-36 as a measure of postoperative recovery after colorectal surgery. Surg Endosc. 2014;28:3168–78. doi: 10.1007/s00464-014-3577-8. [DOI] [PubMed] [Google Scholar]
- 16.Keller DS, McGee MF, Goyal S, Nobel T, O’Brien Ermlich B, Cheruvu VK, et al. Construct validation and comparison of a novel postoperative quality-of-life metric and the short form-36 in colorectal surgery patients. Surgery. 2013;154:690–5. doi: 10.1016/j.surg.2013.06.037. [DOI] [PubMed] [Google Scholar]
- 17.Yang Z, Li W, Tu X, Tang W, Messing S, Duan L, et al. Validation and psychometric properties of Chinese version of SF-36 in patients with hypertension, coronary heart diseases, chronic gastritis and peptic ulcer. Int J Clin Pract. 2012;66:991–8. doi: 10.1111/j.1742-1241.2012.02962.x. [DOI] [PubMed] [Google Scholar]
- 18.Boitor M, Martorella G, Arbour C, Michaud C, Gélinas C. Evaluation of the preliminary effectiveness of hand massage therapy on postoperative pain of adults in the Intensive Care Unit after cardiac surgery: A pilot randomized controlled trial. Pain Manag Nurs. 2015;16:354–66. doi: 10.1016/j.pmn.2014.08.014. [DOI] [PubMed] [Google Scholar]
- 19.Wang AT, Sundt TM, Cutshall SM, Bauer BA. Massage therapy after cardiac surgery. Semin Thorac Cardiovasc Surg. 2010;22:225–9. doi: 10.1053/j.semtcvs.2010.10.005. [DOI] [PubMed] [Google Scholar]
- 20.Dion L, Rodgers N, Cutshall SM, Cordes ME, Bauer B, Cassivi SD, et al. Effect of massage on pain management for thoracic surgery patients. Int J Ther Massage Bodywork. 2011;4:2–6. doi: 10.3822/ijtmb.v4i2.100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Givi M. Durability of effect of massage therapy on blood pressure. Int J Prev Med. 2013;4:511–6. [PMC free article] [PubMed] [Google Scholar]
- 22.Rajati F, Mostafavi F, Sharifirad G, Sadeghi M, Tavakol K, Feizi A, et al. A theory-based exercise intervention in patients with heart failure: A protocol for randomized, controlled trial. J Res Med Sci. 2013;18:659–67. [PMC free article] [PubMed] [Google Scholar]
- 23.van Gulik L, Janssen LI, Ahlers SJ, Bruins P, Driessen AH, van Boven WJ, et al. Risk factors for chronic thoracic pain after cardiac surgery via sternotomy. Eur J Cardiothorac Surg. 2011;40:1309–13. doi: 10.1016/j.ejcts.2011.03.039. [DOI] [PubMed] [Google Scholar]
- 24.Gjeilo KH, Klepstad P, Wahba A, Lydersen S, Stenseth R. Chronic pain after cardiac surgery: A prospective study. Acta Anaesthesiol Scand. 2010;54:70–8. doi: 10.1111/j.1399-6576.2009.02097.x. [DOI] [PubMed] [Google Scholar]
- 25.Moholdt T, Bekken Vold M, Grimsmo J, Slørdahl SA, Wisløff U. Home-based aerobic interval training improves peak oxygen uptake equal to residential cardiac rehabilitation: A randomized, controlled trial. PLoS One. 2012;7:e41199. doi: 10.1371/journal.pone.0041199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Martorella G, Boitor M, Michaud C, Gélinas C. Feasibility and acceptability of hand massage therapy for pain management of postoperative cardiac surgery patients in the Intensive Care Unit. Heart Lung. 2014;43:437–44. doi: 10.1016/j.hrtlng.2014.06.047. [DOI] [PubMed] [Google Scholar]
- 27.Chen WL, Liu GJ, Yeh SH, Chiang MC, Fu MY, Hsieh YK, et al. Effect of back massage intervention on anxiety, comfort, and physiologic responses in patients with congestive heart failure. J Altern Complement Med. 2013;19:464–70. doi: 10.1089/acm.2011.0873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Jane SW, Wilkie DJ, Gallucci BB, Beaton RD, Huang HY. Effects of a full-body massage on pain intensity, anxiety, and physiological relaxation in Taiwanese patients with metastatic bone pain: A pilot study. J Pain Symptom Manage. 2009;37:754–63. doi: 10.1016/j.jpainsymman.2008.04.021. [DOI] [PubMed] [Google Scholar]
- 29.Kurfirst V, Mokráček A, Krupauerová M, Canádyová J, Bulava A, Pešl L, et al. Health-related quality of life after cardiac surgery – The effects of age, preoperative conditions and postoperative complications. J Cardiothorac Surg. 2014;9:46. doi: 10.1186/1749-8090-9-46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Eagle KA, Guyton RA, Davidoff R, Edwards FH, Ewy GA, Gardner TJ, et al. ACC/AHA 2004 guideline update for coronary artery bypass graft surgery: Summary article: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to update the 1999 guidelines for coronary artery bypass graft surgery) Circulation. 2004;110:1168–76. doi: 10.1161/01.CIR.0000138790.14877.7D. [DOI] [PubMed] [Google Scholar]
- 31.Vainiola T, Roine RP, Suojaranta-Ylinen R, Vento A, Sintonen H. Can factors related to mortality be used to predict the follow-up health-related quality of life (HRQoL) in cardiac surgery patients? Intensive Crit Care Nurs. 2013;29:337–43. doi: 10.1016/j.iccn.2013.04.003. [DOI] [PubMed] [Google Scholar]
- 32.Manca A, Hawkins N, Sculpher MJ. Estimating mean QALYs in trial-based cost-effectiveness analysis: The importance of controlling for baseline utility. Health Econ. 2005;14:487–96. doi: 10.1002/hec.944. [DOI] [PubMed] [Google Scholar]