

Abstract
Objective:
Health-care waste has not attended much attention in developing countries. Staff is involved in cleaning and collect waste may often be at greater risk due to their less education and training. The current intervention study was conducted to improve knowledge and practice skills for medical waste handlers in some selected hospitals of Alexandria, Egypt.
Methods:
An intervention study was conducted on medical waste handlers from some selected hospitals who accepted to participate in the study in the period of May 2015 to June 2016. A predesigned questionnaire was developed to measure knowledge, skills, and practice on medical waste management pre- and post-intervention.
Results:
Analysis of pre-intervention data revealed that 9.6%, 80.8%, and 9.6% of participants had high, moderate, and low knowledge levels, respectively. Whereas post-intervention, data revealed that 97.3%, 2.2%, and 0.5% of workers had high, moderate, and low knowledge levels, respectively. A significant increase in knowledge after the intervention was detected among all knowledge items except in four items which were related to the necessity to segregate medical waste, knowledge of color coding system for segregation, disposal of general waste in black bags and disposal of infectious waste in red bags. Regarding practice of waste handlers, 80% were in poor practice category pre-training and changed to 0.8% post-training; 1.1% were in good practice category and increased to 92.1% post-training.
Conclusion:
The current findings emphasize the role of educative skill-raising training in enhancing knowledge and practice skills of medical waste handlers.
Keywords: Medical waste handling, medical waste, safety climate, safety performance
Introduction
Hospitals are health institutions providing patient care services. In the process of health care, waste is generated.[1] Poor management of health-care waste potentially exposes health care workers, waste handlers, patients, and the community to infection, injuries, and toxic pollutants with a great possibility risk for polluting the environment.[2] The impacts of poor health-care waste management differ from one group of workers to another. The staff that cleans the hospital and collects waste may often be at greater risk than a medical staff that produces it.[3] Health-care waste handlers can come into contact with medical waste during the process of segregation, collection, transport, storage, and final disposal. They are at greatest risk of infectious hazards, especially sharps. The risk of acquiring a secondary infection following needlestick injury from a contaminated sharp depends on the amount of contamination and nature of infection from a source patient. The risk of infection with hepatitis B is more than 10 times greater than for hepatitis C, and up to 100 times greater than for human immunodeficiency virus. Other hazards to health-care waste workers include chemical exposures and ergonomic hazards. In addition, mismanagement of health-care waste poses risks to people and the environment.[2]
Health-care waste workers should be trained before starting and on a routine basis to update their knowledge of prevention and control measures. Training in health and safety is intended to ensure that workers know and understand the potential risks associated with health-care waste, and rules and procedures required for safe management. They should be informed of the importance of consistent use of personal protective equipment and should be aware of where to obtain post-exposure follow-up in case of a needlestick injury or other blood exposure.[4,5]
In developing countries, health-care waste has not gained much attention, and the levels of awareness among health care workers of hazards and potential risks of health-care waste are much lower.[6,7] The impacts of poor health-care waste management differ from one group of workers to another. The staff that cleans the hospital and collects waste may often be at greater risk than a medical staff that produces it. These workers are usually poorly educated and least trained with little attention paid to their safety. Vaccination or proper protective equipment is uncommon for them to have.[3] They can be affected by direct contact with waste every day of their working lives as a result of poor health-care waste management practices.[8]
To the best authors’ knowledge, no past studies have been done to assess the effectiveness of training program on hospital waste management among medical waste handlers in Egypt. There have been only two published Egyptian studies that assessed the knowledge and practice related to waste management among doctors, nurses, and housekeepers.[9,10] One of them assessed the knowledge and practice related to waste management among doctors, nurses, and housekeepers in the surgical departments, at Al-Mansoura University Hospital.[9] The second one was planned to examine knowledge, attitudes, and practices of physicians, nurses, and housekeepers toward waste disposal management at Ein-Shams University Hospitals, Cairo.[10] Thus, the present intervention study was designed to improve knowledge and practice skills for medical waste management among handlers in some selected hospitals of Alexandria, Egypt, with a planned survey for pre- and post-training assessment.
Methods
Study design
Two parallel designs were adopted to accomplish this study; the first one was cross-sectional design to describe and identify the current status of medical waste management in the studied hospitals. The second was intervention study that was designed for medical waste handlers in some selected hospitals to raise their understanding, knowledge, skills, and expertise for the proper and safe handling of medical waste.
Study setting
The study was conducted to target medical waste handlers of 11 governmental hospitals in Alexandria Governorate, Egypt. The selected hospitals were chosen randomly who accepted to participate in this study, considering the constraints of accessibility. Different administrative affiliations were filled out and submitted to perform the study, directed to directorate of health affairs (DOHA), specified medical centers (SMC), health insurance organization (HIO), and curative care organization (CCO). The study was conducted from May 2015 to June 2016.
Study sample
The study sample constituted 365 medical waste handlers from different departments of the studied hospitals, who accepted to participate in the study. A sample size of 340 medical waste handlers was calculated to be efficiently represented to underlying study to estimate an average rate of safety climate among medical waste handlers (52.3%), as described by Hakim et al., 2014,[9] with a precision rate of 7%, alpha error of 0.05 and design effect of 2, using Epi Info 7 software.
Study tools
After reviewing the relevant literature,[11-19] the following tools were developed and used in this study for data collection.
Tool I
Observational checklist
Observational checklist was developed to obtain an initial indication of the current status of health-care waste management at each of the participated hospital. Data were collected on organization policy and planning related to medical waste management in the studied hospitals regarding training; occupational health and safety; infectious waste bags and sharp containers; classification and segregation; waste generation data; collection and handling; transportation inside hospital; storage; handling of hazardous chemical waste, pharmaceutical and radioactive waste; treatment and disposal; wastewater/liquid discharge; registers; contracts; and licenses.
Tool II
Pre-training self-structured questionnaire
A pre-training self-structured questionnaire was developed based on scientific literature.[11-19] The questionnaire was developed in Arabic using simple language and pictures. All questions were a closed-end type which was easy to analyze and may achieve a quicker response from participants. It consisted of five parts. First part covered demographic data of the targeted workers. The second part included multiple choice four items to assess the attitude of participants toward medical waste management. The third part was designed to provide self-administered knowledge questionnaire. It consisted of multiple choice 27 items; such as identification of biohazard symbol. The forth part contained multiple choice six questions evaluating the self-practicing of waste handlers, such as sealing infectious waste bags when they are three-quarters. While the fifth part was observational part to report wearing the uniform and protective footwear for each targeted worker.
Tool III
Post-training self-structured questionnaire
The same questionnaire as pre-training questionnaire was designed, excluding the attitude questionnaire part, to assess knowledge and practices of medical waste handlers after the intervention.
Pilot study
A pilot study was conducted on 12 medical waste handlers to test the predesigned questionnaire and was carried out before starting the actual data collection. A pilot sample was excluded from the final study sample size. The purpose of the pilot study was to ascertain the clarity, applicability of the questionnaire to ensure its validity and reliability; to estimate the time needed to fill in the questionnaire; to identify the possible obstacles or problems that may hinder data collection; to identify measures to overcome obstacles; and perform any required changes to questionnaire.
Permission and official consents
For accomplishing the underlying study, official permissions were obtained from Research Ethics Committee, Central Directorate for Research and Health Development, Ministry Of Health and Population; Directorate General of Training and Cultural Relations, General Authority for Health Insurance; CCO, Alexandria; and all general managers in the studied hospitals. Verbal consent was obtained from each participated medical waste handler to be involved in this study.
Training package
Training sessions were designed to provide information that is feasible to the levels of education of medical waste handlers, through:
Teaching and learning method: Lectures and discussion
Teaching and learning aids projector or laptop computer or iPad; PowerPoint presentations and videos; and eye-catching teaching aids.
Content of training: After reviewing the relevant literature[2,11,20-24] content of training program was developed including the following topics: Training overview; categories of health-care waste; overview of hazards associated with health-care waste; key steps in health-care waste management for hospitals that use centralized off-site treatment; roles and responsibilities of waste handlers in health-care waste management; some health and safety practices for waste handlers; and respond to a health-care waste-related accident or incident.
Data collection
Observational checklist and a pre-tested self-structured questionnaire were used for data collection. Site visits, key informant interviews with hospitals’ authorities and survey questionnaires were employed to collect information regarding various aspects of medical waste management. To facilitate filling out of the questionnaire, interviews with participated workers were performed, as most of the targeted workers were illiterate or had limited educational level.
Statistical analysis
After data were collected it was revised, coded and fed to statistical software IBM SPSS version 20. The given graphs were constructed using Microsoft Excel software. All statistical analysis was performed using two-tailed tests and an alpha error of 0.05. P ≤ 0.05 was considered to be statistically significant. Scoring system was adopted, each correct answer was given a score of 1 otherwise, zero was given. The overall score was calculated by summing discrete scores for all items then the score percent was calculated as follow: “Score% = (actual score/maximum score)*100.” Descriptive statistics included means, standard deviations, and percent of scores to describe the scale and categorical data, respectively. While median was used for skewed data as mean is usually affected by extreme values and give biased average. Analysis of numeric data was performed using one-sample Kolmogorov-Smirnov test, independent sample t-test, Pearson’s Chi-square test, Monte Carlo and Fisher’s exact tests, marginal homogeneity test, and multiple stepwise linear regression.
Results
Reliability
The reliability of the questionnaire was assessed by applying reliability test using Cronbach alpha. Values of Cronbach’s alpha for knowledge domain and practice domains were 0.810 and 0.857, respectively, showing strong correlation, indicating that the questionnaire was convenient and well-structured for the selected sample.
Demographic information
Ages of participants varied from 19 to 70 years old. Majority of participants (69.6%) were in the age group of 40–70 years, 9.3% were in the age group of 19–29 years and 21.1%, were in the age group of 30–39 years. Most of the studied participants were females (71.0%). Regarding the educational status, it was found that 45.2% were illiterate while 17.8% could read and write and 14.2% had primary education. The rest of the studied subjects had basic education or above; 10.4% preparatory, 1.1 secondary, and 11.2 diploma. Concerning marital status, 67.1% of studied subjects were married, 16.4% were widows, 8.5% were divorced, and 7.9% were single. It was also found that 50.7% of participants had nonpermanent employment. Approximately half of studied participants (49.9%) had 10 years or more working experience; 21.9% had 1–4 years of experience, 19.2% had 5–9 years of experience, and only 9.0% participants had <1 year of experience. About 73% of the studied participants didn’t attend in-service related training in past 12 months. On observation of targeted workers, it was found that 32.1% of the participants did not wear suitable uniform for waste handling and 70.4% did not wear protective footwear (note: Protective footwear in this study refers to rubber sandal with closed toe, and waterproof, resistant to sharps puncture, and prevents slipping and easy to disinfect).
Pre- and post-training knowledge of participants
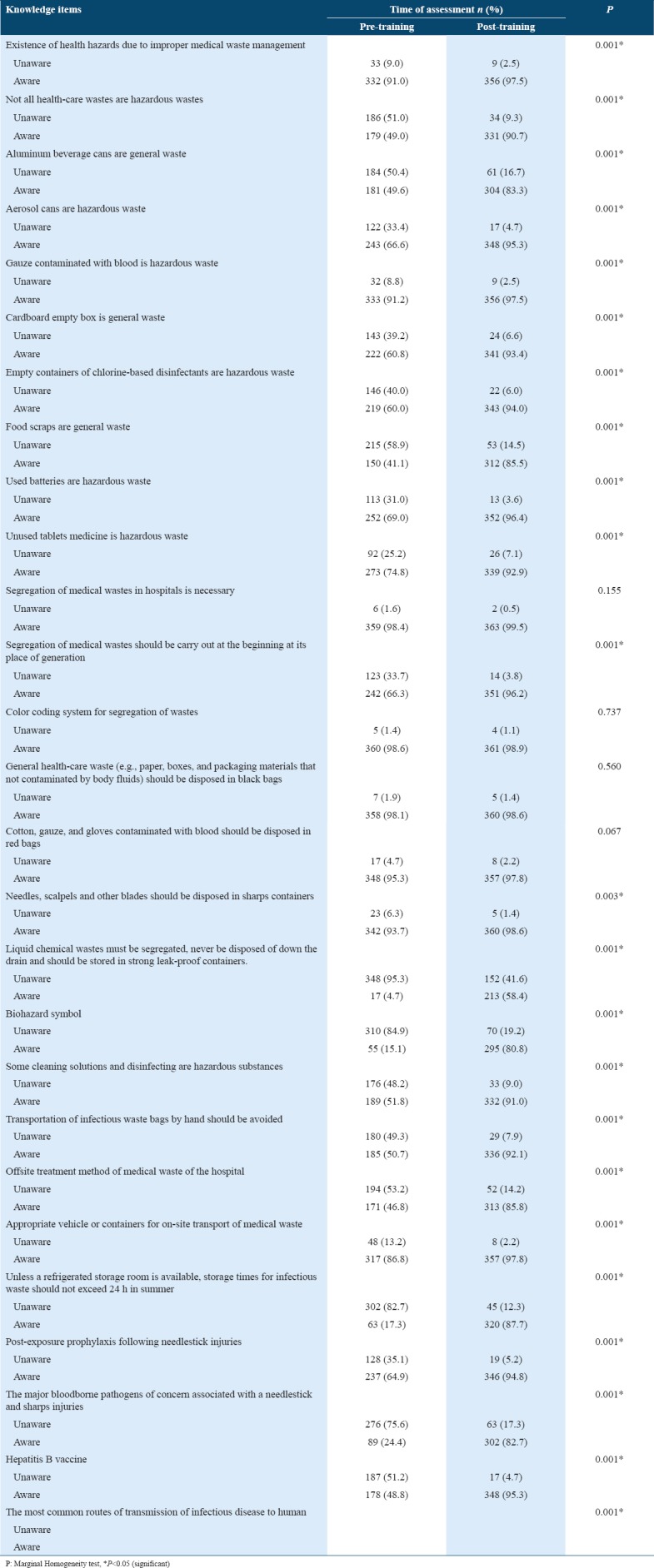
Table 1 summarizes the pre- and post-training knowledge level of participants. Pre-training, 91.0% of studied subjects were aware of the existence of health hazards due to improper medical waste management, and the awareness was increased up to 97.5% after training. These differences were statistically significant at P ≤ 0.05, using marginal homogeneity test. It was found that 49.0% of participants knew that not all health-care wastes are hazardous and their level of knowledge was significantly increased to 90.7% after getting awareness through training. When targeted workers were asked about different constituents of hazardous health-care wastes, only 8.8% was unaware that gauze contaminated with blood is hazardous waste compared to 33.4%, 40%, 31%, and 25.2% were unaware that aerosol cans, empty containers of chlorine-based disinfectants, used batteries and unused tablets medicine are hazardous, respectively. The knowledge was increased after training, and it was statistically significant at P ≤ 0.05, using marginal homogeneity test. For different constituents of general health-care wastes, 49.6%, 41.1%, and 60.8% of subjects knew that aluminum beverage cans, food scraps, and cardboard empty box are general wastes, respectively. After training, the knowledge was increased up to 83.3%, 85.5%, and 93.4%, respectively, and the levels of increase were statistically significant at P ≤ 0.05, using marginal homogeneity test. Majority of subjects (98.4%) had already pre-knowledge about the necessity of segregation of medical wastes in hospitals, and this percentage increased to 99.5% after training, but it was not statistically significant. About 66% of the participants were aware that segregation of waste should be carried out at the point of generation and it was significantly increased to 96.2% post-training. The majority of subjects (98.6%) were already aware of color coding system for segregation of wastes, and the knowledge was increased after giving training (P = 0.737). Before training, 98.1% and 95.3% of the studied subjects knew that general health-care waste should be disposed in black bags and cotton, gauze and gloves contaminated with blood disposed in red bags, respectively. After training, there was an increase in knowledge, but it was not statistically significant. About 94.0% of participants had knowledge about the disposal of needles, scalpels, and other blades in sharps containers and the awareness were increased up to 98.6% after training (P = 0.003). Few of the participants (4.7%) had already knowledge (before training) that liquid chemical wastes must be segregated, never be disposed of down the drain and should be stored in strong leak-proof containers and the awareness significantly increased up to 58.4% after training. Only 15.1% of participates could identify the biohazard symbol before training while, after training 80.8% of them knew the biohazard symbol (P = 0.001). It was found that 51.8% knew that some cleaning solutions and disinfecting are hazardous substances and 50.7% knew that transportation of infectious waste bags by hand should be avoided. The knowledge was increased up to 91.0% and 92.1%, respectively, after getting awareness program and it was statistically significant. About 47% of the participants had knowledge about the offsite treatment method of medical waste of her/his hospital and after training level of knowledge among participants was increased significantly to involve 85.8% of the sample. A majority of the subjects (86.8%) could identify the appropriate vehicle for on-site transport of medical wastes. After training the awareness was raised among 97.8% of participants and the increase was found to be statistically significant. The results showed that 17.3% of the subjects knew correct storage time for biomedical waste before the training and the knowledge was significantly increased to 87.7% after having training. Approximately 65% of the training participants were aware of post-exposure prophylaxis following needlestick injuries, and the awareness was increased up to 94.8% after training (P = 0.001). The results revealed a significant increase in knowledge among participants, after training, for the major three bloodborne pathogens of concern associated with a needlestick and sharps injuries from 24.4% to 82.7%. Furthermore, before the intervention, there was 18.9% of subjects knew routes of transmission of infectious disease to human while after the intervention, there were 81.4% participants aware of it (P = 0.001). As a summary, for all 27 studied knowledge items, there was an improvement in a percentage of workers answering them correctly after the intervention. In general, there was a statistically significant increase in all knowledge items after training except in the following four items; the necessity of segregation of medical wastes, color coding system for segregation, disposal of general health-care waste and disposal of cotton, gauze, and gloves contaminated with blood.
Table 1.
Knowledge level of participants toward safe management of medical waste pre- and post-training
Pre- and post-training practice of participants
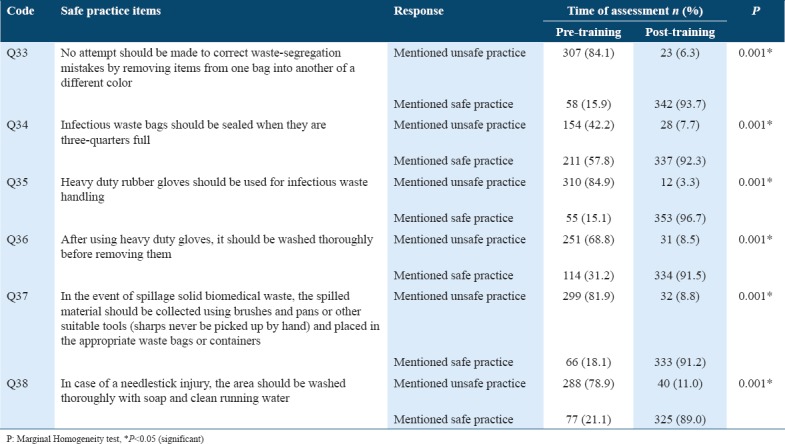
Table 2 summarizes the pre- and post-training practices of participants. Before the intervention, 84.1% of subjects did not mention the correct performance in case of waste-segregation mistakes occur. After training, this percentage was decreased to 6.3% which was found to be statistically significant. Before training, 57.8% of subjects were pointed to the correct practice regarding seal infectious waste bags when they are three-quarters full compared to 92.3% after intervention. The increased percentage was statistically significant at P = 0.001. Only 15.1% of participates mentioned correct performance regarding wear the appropriate gloves (heavy duty gloves) while handling infectious waste and the percentage was significantly increased up to 96.7% after training sessions. Before training, 31.2% of the subjects indicated the safe performance regarding wash, thoroughly, heavy duty gloves before removing them. However, after training only 8.5% of them did not mention the appropriate practice after using heavy duty gloves and it was statistically significant at P ≤ 0.05. Regarding practice in the event of spillage solid biomedical waste, only 18.1% of the study subjects mentioned the correct practice before training. While, after training this percentage was increased to 91.2% which was statistically significant at P = 0.001. Concerning to the immediate practice in case of a needlestick injury, less than quarter (21.1%) of the studied subjects pointed to the correct performance before intervention compared to 89.0% of them after training. The increase was statistically significant at P = 0.001. Thus, there was a statistical significant improvement in all studied practice’s items after training when compared to before training.
Table 2.
Practice of subjects for safe management of medical waste pre- and post-training
Knowledge and practice scores pre-training versus post-training
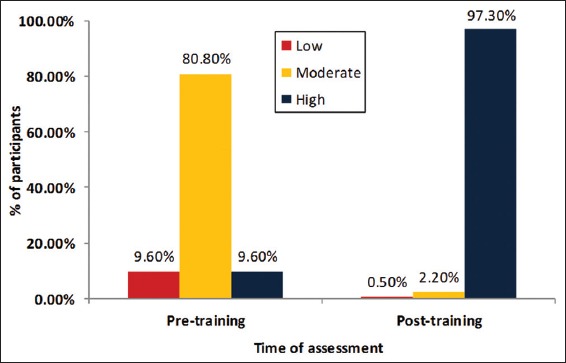
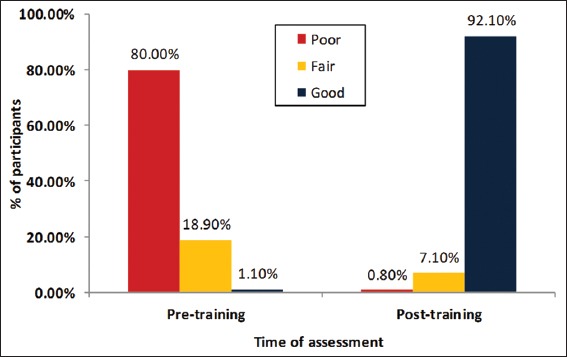
Medical waste handlers were grouped into three categories according to their knowledge scores into low, moderate, and high, for pre- and post-training assessment, as shown in Figure 1. Pre-training there were 9.6% of waste handlers in the low score category which decreased to 0.5% of participants post-training. There were also 9.6% in the high level of knowledge which was increased to 97.3% after training. Regarding practices categories, medical waste handlers were grouped into three categories; poor, fair, and good level of practice in pre- and post-training assessment, as shown in Figure 2. Initially, there were 80% of waste handlers in the poor score category which decreased to only 0.8% post-training. There was only 1.1% in a good category which increased to 92.1% in good category after training.
Figure 1.
Percent change of subjects according to knowledge categories before and after intervention
Figure 2.
Percent change among the studied subjects in practice in medical waste handling before and after intervention
Pre- and post-training Chi-square test
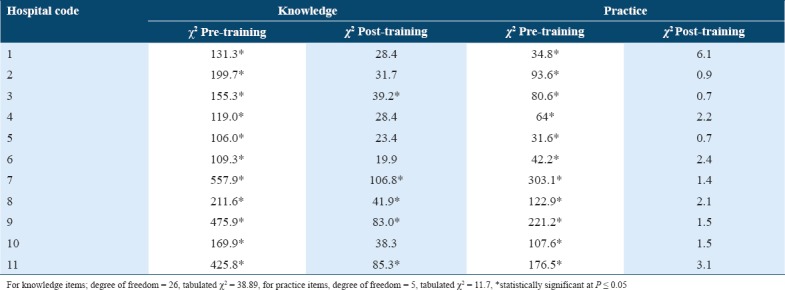
Chi-square test was performed to the given answers of the studied sample pre- and post-training. The assumption was made that the given answers should be compared to optimum correct answers to identify levels of differences in knowledge and practice in the handling of medical waste. As showed in Table 3, comparing given to optimum knowledge answers before training, the studied sample showed a significant difference at P ≤ 0.05, indicating lack of awareness levels for medical waste handling among participants. These results were reversed after training in six hospitals, as given and optimum answers showed insignificant differences, indicating that knowledge was enhanced after training sessions. However, five hospitals need further training to raise the level of knowledge as although the differences among variables were decreased, values showed statistically significant differences at P ≤ 0.05. Comparing the given to optimum practice answers before training, the studied sample showed significant differences at P ≤ 0.05, indicating incorrect practices among participants. The results were reversed after training where the given and optimum answers showed insignificant differences at P ≤ 0.05 for all of the studied hospitals, indicating that the training sessions enhanced the skills for proper practices.
Table 3.
Chi-square (χ2) test for knowledge and practice on medical waste handling pre- and post- training among participants of each hospital
Multiple linear regression analysis
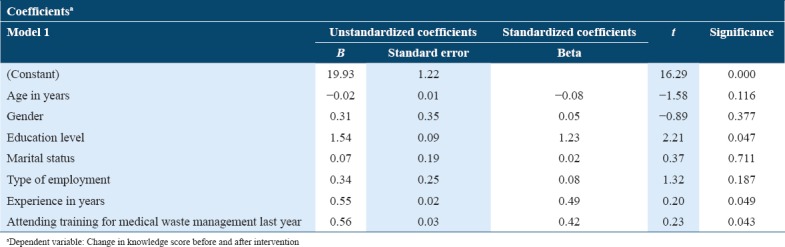
Multiple stepwise linear regression analysis was used to analyze the predictors of the change in knowledge and practice before and after the intervention of participants toward safe management of medical wastes. As presented in Table 4, there was a significant relationship between educational level and change in knowledge scores before and after intervention while keeping all other factors constant (B = 1.54, P = 0.047). A significant relationship existed between the total experience of participants and change in their knowledge scores while keeping all other factors constant (B = 0.55, P = 0.049). There was a significant relationship between attending related training during past 12 months and change in knowledge scores among the studied participants while keeping all other factors constant (B = 0.56, P = 0.043). All other predictors of knowledge change, different demographic criteria, were not statically significant with a change in knowledge.
Table 4.
Multiple stepwise linear regression analysis for the predictors of the change in knowledge scores of participants of medical waste handling pre- and post-intervention
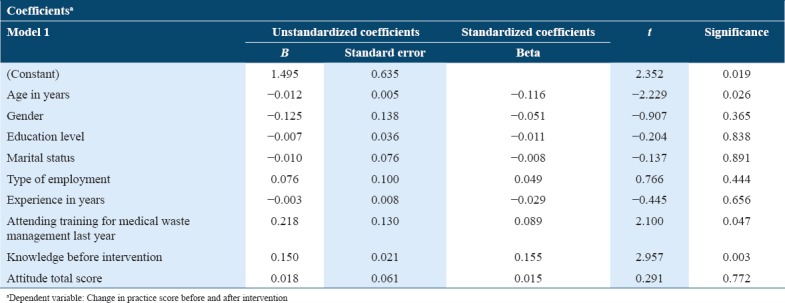
As presented in Table 5, there was a significant inverse association between age of tested participants and change in practice score before and after the intervention, if keeping all other factors constant (B = −0.012, P = 0.026). A significant relationship was also found between attending training by participants in last year and practice score change that while keeping all other factors constant (B = 0.218, P = 0.047). A significant relationship also existed between baseline knowledge of targeted subjects and change in their practice score while keeping all other factors constant (B = 0.150, P = 0.003). On the other hand, none of the other studied predictors were significantly associated with the change in practice.
Table 5.
Multiple stepwise linear regression analysis for the predictors of the change in practice scores of participants of medical waste handling pre- and post-intervention
Discussion
The findings of the present study showed that there is a female preponderance (71.0%) among 365 workers participating in the study and 45.2% of targeted workers were illiterate. About 70% of subjects were in the age group of 40–70 years old, and 49.9% had more than 10 years of experience. About 51% had nonpermanent employment. This fact leads to higher turnover of these workers and lower experience. About 72% of participates did not attend related training in last year.
This study showed that the majority of waste workers (80.8%) had moderate knowledge before training. These findings are greater than results recorded by other studies.[25,26] Amouei et al., 2015,[25] showed that 60% of service workers had medium knowledge on biomedical waste management. Bansal et al., 2011[26] in the district of Madhya Pradesh in India reported that 70.73%, 24.39%, and 4.87% of waste handlers and sweepers had poor, average and good knowledge on biomedical waste management, respectively. However, after implementation of the training program, there were significant improvements with an increased number of participants who achieved high scores, post-intervention, from 9.6% to 97.3%. The improvement in knowledge scores indicates that the program succeeded to achieve its targeted goals. This may be attributed to one or more causes, which include the comprehensive content of the educational training program, waste workers are interested and eagerness to know and change, consideration of the rules of adult learning, encouragement of questions, interactive talk with use of multimedia and repetition of the message through a variety of materials. This result is consistent with the findings presented in a previous study reported by Zagade and Pratinidhi, 2014,[27] who implemented an educational program on medical waste management for biomedical waste handlers in Krishna Hospital, Karad, revealed that percentage of participants had excellent knowledge increased from 0.5% pre-intervention to 79.1% after implementing the program.
The current study showed a significant increase after intervention among all knowledge items except four items which were related to the necessity to segregate medical waste, knowledge of color coding system for segregation, disposal of general waste in black bags and disposal of infectious waste in red bags. It may be due to the majority of the studied subjects were already having knowledge about those items before training. This significant increase in the majority of knowledge items is indicating that all points in training were illustrated in a simple and clear way suitable to the targeted group.
Concerning the practice scores for medical waste workers, the results of the present study showed that 80.0% of the studied group had poor practice score regarding health-care waste management before implementation of the educational training program. While 18.9% and 1.1% of participates had fair and good practice score, respectively, the finding is not consistent with the result reported by Mostafa et al., 2009[10] in Surgical Departments at Al-Mansoura University Hospital, Egypt, reported that only 7.1% of the housekeepers had adequate practice. A study conducted by Gupta et al., 2015,[28] showed that practice score was poor in 62% of sanitary workers and was average in 38% of them. After implementation of the training program, there was a significant decrease in numbers of participants who had poor practice scores (from 80% to 0.8%). This finding pointed to that the educational intervention was very effective and clarity of practical skills offered in such programs. Improvement of practices score obtained in the present study is in agreement with Pratinidhi et al., 2014,[13] found that in pre-training observation there were 83.9% of biomedical waste handlers in the poor practice category which decreased to 2.1% post-training.
For all six questions, related to medical waste management practices, there was a significant improvement in a proportion of workers answering them correctly after the intervention. The percentage of improvement ranged from 34.5% to 81.6%. These findings indicated that using videos and eye-catching teaching aids were effective to illustrate the practices during training on practice items. This was inconsistency with the results of Kumar et al., 2013,[29] Chethana et al., 2013[30] and Kumar et al., 2010[31] who stressed that practices could be improved by proper regular training and by allocating the proper budget for concerned staff.
The results of Chi-square test of the current study indicated the need for further training for workers of the studied hospitals regarding knowledge of safe medical waste management. Chi-square test for all items of attitude indicated that categorical variables differ significantly from optimum attitude at P ≤ 0.05 in all of the studied hospitals. The significant differences revealed inefficient skills and urgent demands for enhancing proper attitude among the targeted medical waste handlers.
Regression analysis revealed a significant relationship between educational levels, total working experience, and attending related training during last year, with the change in knowledge scores before and after the intervention. Regression analysis also showed a significant relationship between age of tested participants, attending training during last year, and baseline knowledge of targeted subjects with a change in practice scores pre- and post-intervention. Although there was no previous literature to correlate the change in knowledge and practice scores of medical waste handlers with various factors to help to take into consideration in designing the training materials to obtain the maximum effectiveness of training.
This research has the limitations that are inherent in studies using perceptions and self-reported response data. It would have been much better if more hospitals are involved in the study. Since this study was a cross-sectional that was carried out during a short period of time; there is a scope for a longitudinal study to validate the findings and measure workers’ skills post-training.
Conclusion
Training in this study enhanced awareness of knowledge and practices among medical waste handlers in the studied hospitals to achieve the desired objectives. However, this improvement can be sustained in long-term with good administration and organization that requires adequate legislation and financing. Furthermore, the training programs should be conducted more frequently because the waste handlers’ turnover rate in hospitals is quite high. Hence, there should be ongoing training to ensure adequate knowledge and proper practice skills for new workers as well as a continuous reminder for old workers.
Acknowledgment
Authors acknowledge the cooperation of DOHA, SMC, HIO, and CCO for making this work feasible.
References
- 1.Patil GV, Pokhrel K. Biomedical solid waste management in an indian hospital:A case study. Waste Manag. 2005;25:592–9. doi: 10.1016/j.wasman.2004.07.011. [DOI] [PubMed] [Google Scholar]
- 2.Chartier Y, Emmanuel J, Pieper U, Prüss A, Rushbrook P, Stringer R, et al. Safe management of wastes from health care activities. 2nd ed. Geneva: World Health Organisation; 2014. [Google Scholar]
- 3.World Health Organization. Regional office for South-East Asia. Regional workshop on Health-Care Waste Management, Kathmandu, Nepal, 7-9 December 2011. New Delhi, India: WHO-SEARO; 2012. [Google Scholar]
- 4.Department of Health. Environment and sustainability Health Technical Memorandum 07-01:Safe Management of Healthcare Waste. London: Department of Health; 2013. [Google Scholar]
- 5.Department of Health. Safe Management of Healthcare Waste. Version 2.0. London: Department of Health; 2011. [Google Scholar]
- 6.Sawalem M, Selic E, Herbell JD. Hospital waste management in libya:A case study. Waste Manag. 2009;29:1370–5. doi: 10.1016/j.wasman.2008.08.028. [DOI] [PubMed] [Google Scholar]
- 7.Taru P, Kuvarega AT. Solid medical waste management:The case of Parirenyatwa Hospital, Zimbabwe. Rev Biomed. 2005;16:153–8. [Google Scholar]
- 8.Appleton J, Ali M. Leicestershire. UK: Water Engineering and Development Centre Lough borough University; 2000. Healthcare or Health Risks?Risks from Healthcare Waste to the Poor. [Google Scholar]
- 9.Hakim SA, Mohsen A, Bakr I. Knowledge, attitudes and practices of health-care personnel towards waste disposal management at ain shams university hospitals, cairo. East Mediterr Health J. 2014;20:347–54. [PubMed] [Google Scholar]
- 10.Mostafa GM, Shazly MM, Sherief WI. Development of a waste management protocol based on assessment of knowledge and practice of healthcare personnel in surgical departments. Waste Manag. 2009;29:430–9. doi: 10.1016/j.wasman.2007.12.009. [DOI] [PubMed] [Google Scholar]
- 11.Ministry of Health, Republic of Kenya. Guide for Training Health Workers in Health Care Waste Management. Nairobi, Kenya: Government of Kenya; 2015. [Google Scholar]
- 12.Madhukumar S, Ramesh G. Study about awareness and practices about health care waste management among hospital staff in a medical college hospital, Bangalore. Int J Basic Med Sci. 2008;26:297–303. [Google Scholar]
- 13.Pratinidhi AK, Zagade TB, Kakade SV. Assessment of effectiveness of educational intervention on practice among biomedical waste handlers. Int J Sci Appl Res. 2014;3:1885–91. [Google Scholar]
- 14.Pratinidhi AK, Zagade TB. Assessment of effectiveness of educational intervention on knowledge among bio-medical waste handlers. Int J Sci Appl Res. 2014;3:37177. [Google Scholar]
- 15.Al-Emad AA. Assessment of medical waste management in the main hospitals in yemen. East Mediterr Health J. 2011;17:730–7. doi: 10.26719/2011.17.10.730. [DOI] [PubMed] [Google Scholar]
- 16.Tariq N, Rajput AM, Azad AH, Afzal M, Rizvi F. Awareness and practices regarding waste management in health care staff of hospitals of Rawalpindi. ISRA Med J. 2014;6:136–41. [Google Scholar]
- 17.Sanjeev R, Kuruvilla S, Subramaniam R, Prashant PS, Gopalakrishnan M. Knowledge, attitude, and practices about biomedical waste management among dental healthcare personnel in dental colleges in Kothamangalam:A cross-sectional study. Health Sci. 2014;1:1–12. [Google Scholar]
- 18.Rudraswamy S. Hospital waste management training among the staff of dental teaching hospitals in Bangalore City:Hospital waste management. Hamburg, Germany: Anchor Academic Publishing; 2014. [[Last cited on 2016 May 29]]. Available from: https://www.amazon.de/Hospital-Management-Training-Hospitals-Bangalore/dp/3954891549 . [Google Scholar]
- 19.Bathala LR, Sangur R, Mahajan T, Chawla PS, Mehrotra A, Singhal P. Bio-medical waste disposal:A Survey to assess the knowledge, attitude and behaviour among Dental Personnel in Kanpur City, Utter Pradesh, India. Int J Sci Res Sci Technol. 2015;2:90–3. [Google Scholar]
- 20.Ministry of Health, Republic of Kenya. An Orientation Guide for Health Care Service Providers in Health Care Waste Management. Nairobi, Kenya: Government of Kenya; 2015. [Google Scholar]
- 21.Egyptian Ministry of State for Environmental Affairs. Healthcare waste Management in Egypt, Guideline. Egypt: Ministry of State for Environmental Affairs; 2015. [Google Scholar]
- 22.Prüss A, Townend WK. Management of wastes from health-care activities. Geneva: World Health Organization; 1998. Teacher's Guide. [Google Scholar]
- 23.National Guidelines for Infection Control. Part 1. Standard Precautions. 2nd ed. Cairo: MOHP, ARE; 2008. Ministry of Health and Population (MOHP), Arab Republic of Egypt. [Google Scholar]
- 24.National Guidelines for Infection Control. Part 2. Infection control in specialty settings. 2nd ed. Cairo: MOHP, ARE; 2008. Ministry of Health and Population (MOHP), Arab Republic of Egypt. [Google Scholar]
- 25.Amouei A, Fallah SH, Asgharnia HA, Gholami M, Jafarian S. Knowledge and attitude of hospital personnel regarding medical waste management. Int Arch Health Sci. 2015;2:75–81. [Google Scholar]
- 26.Bansal M, Mishra A, Gautam P, Changulani R, Srivastava D, Gour NS. Biomedical waste management:Awareness and practices in a district of Madhya Pradesh. Natl J Community Med. 2011;2:452–6. [Google Scholar]
- 27.Zagade T, Pratinidhi A. Effectiveness of educational intervention on knowledge and practice among biomedical waste handlers. Int J Sci Res. 2014;3:285–95. [Google Scholar]
- 28.Gupta V, Mohapatra D, Kumar V. Study to assess the knowledge, attitude and practices of biomedical waste management among health care personnel at tertiary care hospital in Haryana. Int J Basic Appl Med Sci. 2015;5:102–7. [Google Scholar]
- 29.Kumar R, Somrongthong R, Shaikh BT. Knowledge, attitude and practices of health staff regarding infectious waste handling of tertiary care health facilities at metropolitan city of Pakistan. J Ayub Med Coll Abbottabad. 2013;25:109–12. [PubMed] [Google Scholar]
- 30.Chethana T, Thapsey H, Gautham MS, Sreekantaiah P, Suryanarayana SP. Situation analysis and issues in management of biomedical waste in select small health care facilities in a ward under Bruhat Bengaluru Mahanagara Palike, Bangalore. Indian J Community Health. 2013;39:310–15. doi: 10.1007/s10900-013-9761-2. [DOI] [PubMed] [Google Scholar]
- 31.Kumar R, Khan EA, Ahmed J, Khan Z, Magan M, Nousheen, et al. Healthcare waste management (HCWM) in pakistan:Current situation and training options. J Ayub Med Coll Abbottabad. 2010;22:101–5. [PubMed] [Google Scholar]