

Abstract
Background:
Few studies have documented expected time to return to athletic participation after stress fractures in elite athletes.
Hypothesis:
Time to return to athletic participation after stress fractures would vary by site and severity of stress fracture.
Study Design:
Retrospective cohort study.
Level of Evidence:
Level 3.
Methods:
All stress fractures diagnosed in a single Division I collegiate men’s and women’s track and field/cross-country team were recorded over a 3-year period. Site and severity of injury were graded based on Kaeding-Miller classification system for stress fractures. Time to return to full unrestricted athletic participation was recorded for each athlete and correlated with patient sex and site and severity grade of injury.
Results:
Fifty-seven stress fractures were diagnosed in 38 athletes (mean age, 20.48 years; range, 18-23 years). Ten athletes sustained recurrent or multiple stress fractures. Thirty-seven injuries occurred in women and 20 in men. Thirty-three stress fractures occurred in the tibia, 10 occurred in the second through fourth metatarsals, 3 occurred in the fifth metatarsal, 6 in the tarsal bones (2 navicular), 2 in the femur, and 5 in the pelvis. There were 31 grade II stress fractures, 11 grade III stress fractures, and 2 grade V stress fractures (in the same patient). Mean time to return to unrestricted sport participation was 12.9 ± 5.2 weeks (range, 6-27 weeks). No significant differences in time to return were noted based on injury location or whether stress fracture was grade II or III.
Conclusion:
The expected time to return to full unrestricted athletic participation after diagnosis of a stress fracture is 12 to 13 weeks for all injury sites.
Clinical Relevance:
Athletes with grade V (nonunion) stress fractures may require more time to return to sport.
Keywords: stress fracture, stress reaction, bone, track and field, runner
Stress fractures occur along a spectrum of severity that can affect treatment and prognosis.12-14 These injuries are extremely common in track and field athletes, with an annual incidence of up to 20%.4,5,10 As athletes become more competitive and focus solely on 1 sport, the incidence of stress fractures continues to increase. Though much has been published on the diagnosis and treatment of bony stress fractures, few studies have documented the expected time to return to athletic participation after stress fractures in elite athletes.
The tibia and metatarsals are the most common sites for stress fractures, which are responsible for a significant amount of time away from sport.4,5 The ability to correlate the severity of stress injury with time to recovery is crucial for management of these injuries. Furthermore, having a reliable expectation of time to return to sports after these injuries can temper anxiety of athletes, coaches, and sports medicine providers alike.
In 2013, Kaeding and Miller11 proposed a classification system for grading stress fracture severity that included both clinical and radiographic parameters (Table 1). Their system was validated for intra- and interobserver reliability among sports medicine practitioners for grading stress fractures.11 However, the utility of the system for predicting an athlete’s expected time to return to sport has not been evaluated to date.
Table 1.
| Grade | Pain | Radiographic Findings (CT, MRI, Bone Scan, or Radiograph) |
|---|---|---|
| I | − | Imaging evidence of stress fracture No fracture line |
| II | + | Imaging evidence of stress fracture No fracture line |
| III | + | Nondisplaced fracture line |
| IV | + | Displaced fracture (>2 mm) |
| V | + | Nonunion |
CT, computed tomography; MRI, magnetic resonance imaging.
Combined clinical and radiographic classification system for stress fractures is shown.
The purposes of this study were to determine the expected time to return to athletic participation in Division I collegiate track and field athletes after the diagnosis of a stress injury to bone and to evaluate the effect of fracture site and severity as well as sex on time to return to sport. We hypothesized that time to return to athletic participation would vary based on the site and severity grade of the stress fracture.
Methods
Written approval was obtained from the Biomedical Institutional Research Board of The Ohio State University Wexner Medical Center as well as the athletic department’s Sports Medicine Administration Group. All stress fractures diagnosed in athletes on a single Division I collegiate men’s and women’s track and field and cross-country teams were recorded over a 3-year period, between August 2011 and June 2014. Inclusion criteria were any athlete who participated on the team during the aforementioned timeframe and was diagnosed on imaging with a bony stress fracture.
A retrospective chart review was completed on all athletes who met the study’s inclusion criteria. Site and severity of the injury were recorded and graded based on the Kaeding-Miller classification system for stress fractures.7 The senior author graded each of the images based on this system. Time to return to full, unrestricted athletic participation was recorded for each athlete.
Statistical Analysis
Student t tests were used to compare time to return to unrestricted sports participation based on patient sex and fracture grade according to the Kaeding-Miller classification. Because of the small number of grade V injuries (2 injuries), statistical comparisons by grade were only performed between grade II and III. A 1-way analysis of variance was used to evaluate the influence of stress fracture site on time to return to sport.
Results
Fifty-seven stress fractures were diagnosed in 38 athletes (mean age, 20.48 years; range, 18-23 years) over a 3-year period. There were 10 athletes who sustained recurrent or multiple stress fractures. Thirty-seven injuries occurred in women and 20 occurred in men. Thirty-three stress fractures occurred in the tibia, 10 occurred in the second through fourth metatarsals, 3 occurred in the fifth metatarsal, 6 in the tarsal bones (2 navicular), 2 in the femur, and 5 in the pelvis. There were 31 grade II stress fractures, 11 grade III stress fractures, and 2 grade V stress fractures (in the same patient). No grade I or IV stress fractures were noted.
The mean time to return to unrestricted sport participation was 12.9 ± 5.2 weeks (range, 6-27 weeks). A trend toward increased time to return to sport was noted in women (13.9 ± 5.7 weeks) compared with men (11.3 ± 3.8 weeks), but this was not statistically significant (P = 0.068). No significant differences in time to return to sport were noted based on stress injury location or whether the stress fracture was classified as grade II or III (Table 2). The patient with the bilateral grade V stress fractures required 17 weeks for return to sport compared with 12.3 and 14.1 weeks for patients with grade II and III injuries, respectively. Radiographic examples of grades II, III, and V stress fractures are provided in Figures 2, 1, and 3, respectively.
Table 2.
Mean time to return to sport based on injury site and Kaeding-Miller injury grade
| Mean Time to Return, Weeks | Significance | |
|---|---|---|
| Site | P = 0.99 | |
| Pelvis | 13.0 | |
| Tibia | 13.3 | |
| Tarsal | 12.1 | |
| 2nd-4th metatarsal | 11.7 | |
| 5th metatarsal | 11.7 | |
| Grade | P = 0.42 | |
| II | 12.3 | |
| III | 14.1 | |
| V | 17 |
Figure 2.

T2-weighted axial magnetic resonance image of a Kaeding-Miller grade II stress fracture of the fourth metatarsal in a 20-year-old female long-distance runner.
Figure 1.
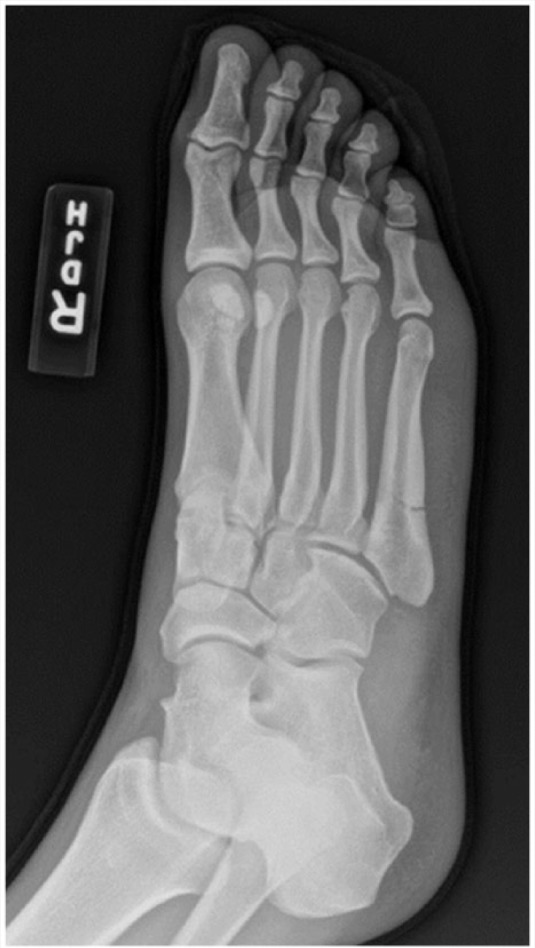
Oblique radiograph of a 21-year-old male long jumper with Kaeding-Miller grade III stress fracture of the fifth metatarsal proximal diaphysis.
Figure 3.

Kaeding-Miller grade V stress fracture of the anterior tibial cortex in a 19-year-old female middle-distance runner who required intramedullary rodding to allow for complete healing.
Discussion
This study analyzed the distribution and severity of all stress fractures in a collegiate track and field and cross-country team over a 3-year period. While many classification systems have been proposed for stress fractures, there is limited literature linking recovery time to these systems. This study compared stress fracture severity on the Kaeding-Miller classification system with time to return to sport.2,6,7,9,17,20,21,23,24
The Kaeding-Miller classification system was first described in 2012 and includes both clinical and radiographic parameters.5,16 The goal of this system was to create something that is easily remembered, easily applied, and could affect prognosis and treatment. It allows for the use of any imaging modality and has been validated for inter- and intraobserver reliability among sports medicine providers.5
Nattiv et al18 were able to validate a different classification system and correlate it with expected return to sport in track and field athletes. However, this system was based on very specific magnetic resonance imaging (MRI) findings that may be difficult for all practitioners caring for these athletes to interpret and apply. Kijowski et al15 were able to validate their MRI classification system for correlation with injury severity and clinical outcome; however, unlike the Kaeding-Miller classification system, this system was only applicable to tibial injuries and was not generalizable. In 2003, Arendt et al1 and Arendt and Griffiths2 reviewed 68 collegiate athletes with stress fractures. They concluded that their MRI-based classification system was helpful in predicting time to return to sport.1,2 A standardized rehabilitation protocol was proposed to return the athletes to pain-free competition based on their findings.1 To summarize, fundamental differences in these alternative systems, including site of application and imaging modality of choice, make direct comparison with the Kaeding-Miller classification system difficult and impractical.
Safe return to athletic participation after stress fractures is multifactorial and has been written about extensively.12-14 However, specific timeframes for expected return to Division I track and field and cross-country participation have not been clearly delineated. Diehl et al8 suggested that the bony pathophysiology, the athlete’s biomechanics, and the site and severity of the injury are all key factors in effective return-to-sport decision-making. This series of stress fractures indicates that time to return to participation in Division I track and field correlates with increasing severity on the Kaeding-Miller classification system and that the time to recovery is 12 to 13 weeks regardless of injury site. These findings help provide a timeframe for when the athlete is likely to safely return to sport without increased chance of recurrence.
Furthermore, the current case series showed that the majority of stress injuries took place in women. This supports the findings of previous sports medicine literature that stress fractures are more common in female runners than in males. In a 2002 series of stress fractures published by Nelson and Arciero,19 the authors determined that runners and track and field athletes are particularly susceptible to stress fractures, and female athletes sustain stress fractures more frequently than their male counterparts. More recently, Tenforde et al22 and Barrack et al3 have identified sex-specific risk factors that increase the risk of developing stress fractures in female athletes, specifically those related to the female triad of disordered eating, amenorrhea, and osteopenia. Additionally, in this study, there was a trend toward increased time to recovery in women compared with men, which has not been described in the literature and warrants further investigation.
There are several limitations to this study. Though this case series included 57 stress fractures, making it one of the largest case series in the current literature, there were still small numbers in each severity grade, particularly grades IV and V. There were in fact no displaced (grade IV) stress fractures, making it impossible to compare this group with other severity grades. Additionally, there were only 2 grade V injuries identified during the collection period, and these occurred bilaterally in the same athlete, making predicting time to return difficult. However, without question, both of these injuries required surgery and extensive time for healing and return to track and field participation. Finally, this study included all track and field and cross-country athletes regardless of event in which the athletes participated (sprints, jumps, or distance running). The variety of events in which track and field athletes compete may have affected their ability to return to sport and the time to return to unrestricted participation.
Conclusion
The expected time to return to full, unrestricted athletic participation after diagnosis of a stress fracture in elite runners is 12 to 13 weeks for all injury sites. Further research is required to determine potential differences in time to return to full participation among different severities of injuries on the Kaeding-Miller classification, as well as between male and female athletes. However, the classification system is a reliable prognostic tool for communicating injury severity between medical professionals and for estimating time to return to athletic participation in elite athletes.
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.
References
- 1. Arendt E, Agel J, Heikes C, Griffiths H. Stress injuries to bone in college athletes: a retrospective review of experience at a single institution. Am J Sports Med. 2003;31:959-968. [DOI] [PubMed] [Google Scholar]
- 2. Arendt EA, Griffiths HJ. The use of MR imaging in the assessment and clinical management of stress reactions of bone in high-performance athletes. Clin Sports Med. 1997;16:291-306. [DOI] [PubMed] [Google Scholar]
- 3. Barrack MT, Gibbs JC, De Souza MJ, et al. Higher incidence of bone stress injuries with increasing female athlete triad-related risk factors: a prospective multisite study of exercising girls and women. Am J Sports Med. 2014;42:949-958. [DOI] [PubMed] [Google Scholar]
- 4. Bennell KL, Malcolm SA, Thomas SA, et al. Risk factors for stress fractures in female track-and-field athletes: a retrospective analysis. Clin J Sport Med. 1995;5:229-235. [DOI] [PubMed] [Google Scholar]
- 5. Bennell KL, Malcolm SA, Thomas SA, et al. Risk factors for stress fractures in track and field athletes. A twelve-month prospective study. Am J Sports Med. 1996;24:810-818. [DOI] [PubMed] [Google Scholar]
- 6. Boden BP, Osbahr DC. High-risk stress fractures: evaluation and treatment. J Am Acad Orthop Surg. 2000;8:344-353. [DOI] [PubMed] [Google Scholar]
- 7. Boden BP, Osbahr DC, Jimenez C. Low-risk stress fractures. Am J Sports Med. 2001;29:100-111. [DOI] [PubMed] [Google Scholar]
- 8. Diehl JJ, Best TM, Kaeding CC. Classification and return-to-play considerations for stress fractures. Clin Sports Med. 2006;25:17-28, vii. [DOI] [PubMed] [Google Scholar]
- 9. Gaeta M, Minutoli F, Vinci S, et al. High-resolution CT grading of tibial stress reactions in distance runners. AJR Am J Roentgenol. 2006;187:789-793. [DOI] [PubMed] [Google Scholar]
- 10. Iwamoto J, Sato Y, Takeda T, Matsumoto H. Analysis of stress fractures in athletes based on our clinical experience. World J Orthop. 2011;2:7-12. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 11. Kaeding CC, Miller TL. The comprehensive description of stress fractures: a new classification system. J Bone Joint Surg Am. 2013;95:1214-1220. [DOI] [PubMed] [Google Scholar]
- 12. Kaeding CC, Najarian RG. Stress fractures: classification and management. Phys Sportsmed. 2010;38:45-54. [DOI] [PubMed] [Google Scholar]
- 13. Kaeding CC, Spindler KP, Amendola A. Management of troublesome stress fractures. Instr Course Lect. 2004;53:455-469. [PubMed] [Google Scholar]
- 14. Kaeding CC, Yu JR, Wright R, Amendola A, Spindler KP. Management and return to play of stress fractures. Clin J Sport Med. 2005;15:442-447. [DOI] [PubMed] [Google Scholar]
- 15. Kijowski R, Choi J, Shinki K, Del Rio AM, De Smet A. Validation of MRI classification system for tibial stress injuries. AJR Am J Roentgenol. 2012;198:878-884. [DOI] [PubMed] [Google Scholar]
- 16. Miller T, Kaeding CC. Stress fractures. In: Buchholz R, Heckman JD, eds. Rockwood and Green’s Fractures in Adults. Philadelphia, PA: Lippincott Williams & Wilkins; 2012:651-666. [Google Scholar]
- 17. Miller T, Kaeding CC, Flanigan D. The classification systems of stress fractures: a systematic review. Phys Sportsmed. 2011;39:93-100. [DOI] [PubMed] [Google Scholar]
- 18. Nattiv A, Kennedy G, Barrack MT, et al. Correlation of MRI grading of bone stress injuries with clinical risk factors and return to play: a 5-year prospective study in collegiate track and field athletes. Am J Sports Med. 2013;41:1930-1941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Nelson BJ, Arciero RA. Stress fractures in the female athlete. Sports Med Arthrosc. 2002;45:1843-1851. [Google Scholar]
- 20. Savoca CJ. Stress fractures. A classification of the earliest radiographic signs. Radiology. 1971;100:519-524. [DOI] [PubMed] [Google Scholar]
- 21. Saxena A, Fullem B, Hannaford D. Results of treatment of 22 navicular stress fractures and a new proposed radiographic classification system. J Foot Ankle Surg. 2000;39:96-103. [DOI] [PubMed] [Google Scholar]
- 22. Tenforde AS, Sayres LC, McCurdy ML, Sainani KL, Fredericson M. Identifying sex-specific risk factors for stress fractures in adolescent runners. Med Sci Sports Exerc. 2013;45:1843-1851. [DOI] [PubMed] [Google Scholar]
- 23. Yao L, Johnson C, Gentili A, Lee JK, Seeger LL. Stress injuries of bone: analysis of MR imaging staging criteria. Acad Radiol. 1998;5:34-40. [DOI] [PubMed] [Google Scholar]
- 24. Zwas ST, Elkanovitch R, Frank G. Interpretation and classification of bone scintigraphic findings in stress fractures. J Nucl Med. 1987;28:452-457. [PubMed] [Google Scholar]