

ABSTRACT
Background
Ankle sprains are common musculoskeletal injuries in the athletic population that have been addressed with prevention strategies that include bracing and balance training. Many authors have examined ankle sprain incidence after bracing or balance training in athletes at different levels of competition and in various sports. No systematic review has analyzed the results of both interventions.
Purpose
The purpose of this review was to compare the effect of balance training and bracing in reducing the incidence and relative risk of ankle sprains in competitive athletes, with or without prior injury, across different sports.
Design
Systematic review, with meta-analysis
Methods
A literature search of four databases was conducted for randomized control trials that reported ankle sprain incidence published from 2005 through 2016. Included articles studied high school, college, or professional level athletes with or without a history of a prior sprain, who received bracing or balance training as an intervention compared to a non-intervention control group. Methodological study quality was assessed by two reviewers using the PEDro scale, with scores ≥5 considered moderate quality. Group incidence and relative risk were determined to assess the preventative effect of bracing or balance training compared to control.
Results
From 1832 total citations, 71 full-text articles were reviewed, and eight articles were included in the study. Methodological quality of the available evidence contained in the systematic review was moderate. Five studied the effect of balance training, two studied the effect of bracing, and one studied the effect of bracing and balance training compared to the control condition. In all eight studies, athletes in the control condition did not receive any intervention. Athletes who wore braces had fewer ankle sprains (p=0.0037) and reduced their risk of sprains by 64% (RR=0.36) compared to controls, based on analysis of 3,581 subjects. Athletes performing balance training had fewer ankle sprains (p=0.0057) and reduced their risk by 46% (RR=0.54) compared to controls, based on analysis of 3,577 subjects.
Conclusion
The findings of the current systematic review and meta-analysis support the use of bracing and balance training to reduce the incidence and relative risk of ankle sprains in athletic populations. Clinicians can utilize this information to educate their patients on wearing a brace or performing balance training exercises to decrease the risk of an ankle sprain.
Level of evidence
Level 1a
Keywords: Athlete, ankle sprain, balance training, bracing, incidence, prevention
INTRODUCTION
In the United States, approximately 23-25,000 ankles sprains occur daily, resulting in two billion dollars of health-care costs annually.1,2,3 Ankle sprains occur in sports that require quick direction changes, cutting movements, and rapid acceleration and deceleration4-7 and are one of the most common sport-related injuries. Inversion sprains comprise 80% of all cases.8 The National Electronic Injury Surveillance System for all ankles sprains admitted into American emergency departments reported 41% of the sprains originated from basketball, 9.3% from football and 7.9% from soccer. Higher level of activity and increased competition of high school, college, and professional team athletes increases an individual's risk of injury. For example, college athletes are seven times more likely to suffer an ankle sprain than their intramural counterparts.3
More than half of high school athletes who sustain an ankle sprain return to play in less than one week.9 A 2008 systematic review found mechanical stability did not occur until at least 6-12 weeks following an ankle sprain, and a substantial percentage of subjects continued to have mechanical laxity and subjective complaints of instability up to one year after injury.10 Diagnostic imaging studies have found an increase in anterior talofibular ligament thickness of approximately 16% in those who have sustained a lateral ankle sprains compared to an uninjured ankle. Increased ligament thickness can be attributed to scar tissue, which absorbs 60% less energy compared to healthy tissue and may be a factor in the high incidence of recurrent ankle sprains and chronic instability symptoms.11,12 After an ankle sprain, 35-73% report on-going symptoms of instability, decreased function, pain, and/or swelling;10,13-20 and the risk of a subsequent sprain was 70% more likely.10 The risk for reinjury or early development of osteoarthritis and long-term disability after an ankle sprain makes preventing ankle sprains a priority.21
The high incidence of ankle sprains in the athletic population has motivated sports teams to implement prophylactic measures to decrease the risk of ankle sprains. During the 1980s and 1990s, multiple researchers investigated the impact of semi-rigid ankle bracing, such as lace-up ankle stabilizing orthoses (ASO), on injury prevention. Results from one randomized control trial and two cohort studies found that semi-rigid bracing significantly reduced ankle sprain incidence in various athletic population.22-25 In 2001, a Cochrane Library systematic review found limited evidence to support balance training in reducing ankle sprains; though good evidence suggested bracing could reduce ankle sprain incidence, especially for those with a prior sprain.7
Currently, few studies26,27 and no reviews have compared the impact of bracing versus balance training on the incidence of ankle sprains in a competitive athletic population. Most studies lack a control group, investigate a single team or include a single sport, leaving unclear what the most effective approach is for reducing the incidence of ankle sprains in a broader athletic population. Thus, the purpose of this review was to compare the effect of balance training and bracing in reducing the incidence and relative risk of ankle sprains in competitive athletes, with or without prior injury, across different sports.
METHODS
Literature search and selection
A search of the literature was conducted for English language articles published from 2005-2016 using the Cochrane Library, PubMed, Web of Science, and PEDro databases. The following medical subject headings (MeSH terms) and clinically relevant keywords were used individually and in Boolean combinations: “ankle,” “instability,” “sprain,” “chronic,” “recurrent,” “prevention,” “athlete,” “proprioception,” and “bracing.” Articles were included in this review if they met the inclusion criteria listed in Table 1. Articles were excluded if the study did not recruit athletes, had no control group, did not define intervention groups, or lacked end of the season or year follow-up. Citations were screened for relevance, full-text articles were reviewed for inclusion by the first author, and included articles were then reviewed by both authors to reach consensus for inclusion and exclusion criteria. Bias was assessed independently using the Pedro scale, a study quality assessment measure for randomized control trials, with disagreements resolved through discussion.
Table 1.
Inclusion Criteria
| 1. Published after 2004 2. Randomized Control Trial with PEDro score of at least 4/10 3. Competitive high school or higher level athletes 4. Follow-up one year and/or post-season 5. Intervention group consisted of balance training, bracing or both 6. Non-treatment, control group 7. Primary outcome measures includes incidence of ankle sprains |
The authors operationally defined the following terms for this review: Athletes were considered individuals participating on competitive sports teams at the high school, college, or professional level. An ankle sprain included an acute inversion/supination (lateral ankle), eversion/pronation (medial ankle), and/or dorsiflexion/eversion (high ankle/syndesmotic) event during sports participation causing injury associated with pain, swelling, and difficulty weight bearing that resulted in the athlete having to cease sports activity in a game or practice. Balance training, sometimes referred to as proprioceptive training, included static or dynamic exercises on one or two legs, on a variety of surfaces, with or without perturbations, and with eyes open or closed. Ankle bracing was considered any type of orthosis applied specifically to the ankle joint; all types of taping were not considered as bracing in this review.
Data Analysis
Incidence of ankle sprains in a season or year and relative risk were utilized to assess the effect of balance training and bracing treatments in preventing injury compared to no-treatment control. Data was extracted by the first author and independently confirmed by the second author. Chi-Square was used to analyze differences in incidence between athletes receiving bracing or balance training compared to no-treatment; relative risk, the risk ratio for ankle sprains in the treatment groups compared to the control groups, was calculated and illustrated in a forest plot (Figures 2 & 3).
Figure 2.

Effects of Balance Training on the Relative Risk of Ankle Sprains.
Figure 3.

Effects of Bracing on the Relative Risk of Ankle Sprains.
Literature Synthesis and Methodological Quality
Electronic database searches yielded 1,832 articles. After citations were screened for relevance, a total of 71 full-text articles were reviewed for inclusion criteria. Sixty-three articles were excluded based on the inclusion criteria, leaving eight articles for review as presented in the PRISMA diagram (Figure 1). The PEDro scale was utilized to assess the methodological quality of each study (Table 2) with scores ≥ 5 considered to be moderate methodological quality.28 Five studies compared balance training to a control group, two studies compared bracing to a control group, and one study compared balance training, bracing (each separately) to controls (Table 3).26,29-35
Figure 1.

PRISMA Diagram.
Table 2.
Methodological Quality Assessment, per Pedro Scale
| Study | Criteria Met | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Verhagen et al. (2005)30 | 5 | Y | N | Y | N | N | N | Y | Y | N | Y |
| McGuine et al (2006)29 | 5 | Y | N | Y | N | N | U | Y | U | Y | Y |
| Emery et al. (2007)31 | 7 | Y | N | Y | N | Y | Y | Y | N | Y | Y |
| Hupperets et al. (2009)32 | 8 | Y | U | Y | N | Y | Y | Y | Y | Y | Y |
| Eils et al (2010)33 |
5 | Y | U | N | U | U | Y | U | Y | Y | Y |
| McGuine et al. (2011)34 | 6 | Y | N | Y | N | N | N | Y | Y | Y | Y |
| McGuine et al. (2012)35 | 6 | Y | N | Y | N | N | N | Y | Y | Y | Y |
| Mohammadi (2007)26 | 6 | Y | U | Y | U | N | U | Y | Y | Y | Y |
Maximum score: 10 points.
1. Randomization of groups 2. Concealed allocation 3. Similar group values/demographics at baseline 4. Subjects were blinded 5. Assessors were blinded 6. Blinding of assessors measuring outcome 7. Acceptable dropout rate 8. Intention to treat 9. Appropriate statistics 10. Point measure/measure of variability recorded. Y: Yes N: No U: Unknown
Table 3.
Description of Included Studies
| Study | Design | Participants | Interventions | Results | Relative Risk | Limitations |
|---|---|---|---|---|---|---|
| Verhagen et al (2005)30 | RCT Level 1b | 1127 Division III college volleyball players (643 females, 484 males). Mean age 24 years. Did not report if subjects had a history of prior sprain. |
Balance training group 36-week balance board “proprioceptive" program (n = 628) Control group (n = 494) | Incidence - 70 total sprains: Balance Training (29) vs. control (41). Incidence rate per exposure: Balance Training: 0.5/1000 hours; Control: 1.87/1000 hours. | 0.40 CI 95% 0.1-0.7 |
Reports differences between groups without providing p-value. Lacking blinding |
| McGuine et al (2006)29 | RCT Level 1b | 765 high school soccer and basketball players (523 females, 242 male). Mean age 16 years, with and without history of prior inversion sprain. |
Balance Training group 5-phase program during the pre- and sport season (n = 373) Control group (n = 392) |
Incidence - 62 total sprains: Balance Training (23) vs. Control (39). Incidence rate per exposure: Balance Training: 1.13/1000 hours; Control: 1.87/1000 hours. Intervention did not significantly reduce risk of sprain for those that did not have a prior sprain history (p = 0.059). | 0.56 CI 95% 0.33-0.95 p = 0.033 |
Recall bias, lacked blinding, ratio of females to males was 2:1 |
| Emery et al (2007)31 | RCT Level 1b | 920 high school basketball players (456 females, 464 males). Mean age 16 years, with or without history of prior ankle sprain. |
Balance Training group balance board 18-week warm-up and home program (n = 494) Control group (n = 426) | Incidence - 138 total sprains: Balance Training (62) vs. control (76). Incidence rate per exposure: Balance Training: 1.57/1000 hours; Control: 2.46/1000 hours. | 0.71 CI 95% 0.45-1.13 p = 0.15 |
Compliance, low power - to improve value would have required 980 subjects |
| Hupperets et al (2009)32 | RCT Level 1b | 522 mixed-level and sport athletes (248 females, 274 males). Mean age 28 years, with prior history of inversion sprain. |
Balance Training group unsupervised 8-week “proprioceptive” program (n = 256) Control group (n = 266) | Incidence – 145 total sprains: Balance Training (56) vs. Control (89). Incidence rate per exposure: Balance Training: 1.86/1000 hours; Controls: 2.90/1000 hours. | 0.63 CI 95% 0.45-0.88 |
Reported compliance 52%, some subjects lost to follow-up, did not specify type of sport, or hours/week of sport participation. |
| Eils et al (2010)3 | RCT Level 1b | 232 mixed-level German basketball players (all male). Mean age 25 years, did not report if subjects had a history of prior sprain. |
Balance Training group multi-station “proprioceptive” program through season (n = 96) Control group (n = 102) | Incidence – 28 total sprains: Balance Training (7) vs Control (21). Incidence rate per exposure: Balance Training: 1.53/1000 hours; 4.31/1000 hours | 0.35 CI 95% 0.15-0.84 p = 0.018 |
Lacked blinding, did not report compliance |
| Mohammadi (2007)26 | RCT Level 1b | 80 college Division I soccer players (all male). Mean age 24 years, with prior history of ankle inversion sprain |
1: Balance Training “proprioceptive” training program (n = 20) 2: Strengthening (n = 20) 3: Sports Stirrup Bracing (n = 20) 4: Control (n = 20) Performed through season. | Incidence - 15 total sprains: Balance Training (1), Strengthening (4), Bracing (2), Control (8). Balance Training reduced incidence (p = 0.02) vs. control; Bracing (p = 0.06) and Strengthening (p = 0.27) did not. Incidence rate per exposure: Balance Training: 0.0.418/1000 hours; Strengthening: 1.67/1000 hours; Bracing: 0.834/1000 hours; Controls: 3.35/1000 hours | Balance Training: 0.13 CI95% 0.003-0.93 Bracing: 0.25 CI95% 0.03-1.91 |
Small sample size, lacked blinding, lacked description of medical trainers’ experience |
| McGuine et al (2011)34 | RCT Level 1b | 1460 high school basketball players (736 females, 724 males). Mean age 16 years, with and without history of prior ankle sprain. |
Bracing group wore McDavid Ultralight lace-up orthosis for team organized conditioning, practice, and games for full season (n = 740) Control group: (n = 720) | Incidence - 265 total sprains: Bracing (117) vs. Control (148). Incidence rate per exposure: Bracing: 0.47/1000 hours; Controls: 1.41/1000 hours. | 0.32 CI 95%: 0.19-0.51 p<0.001 |
Did not account for different types of shoes, lacked blinding |
| McGuine et al (2012)35 | RCT Level 1b | 2081 high school football players (all male). Mean age 16 years, with and without history of prior ankle sprain |
Bracing group wore Don-Joy lace-up Ankle Stabilizing Orthosis, for team organized conditioning, practice, games for full season (n = 993) Control group: (n = 1088) | Incidence – 686 total sprains: Bracing (313) vs control (373). Incidence rate per exposure: Bracing: 0.48/1000 hours; Controls: 1.12/1000 hours. | 0.39 CI 95% 0.24-0.65 p<0.001 |
Did not account for different types of shoes, lacked blinding ack of subject and assessor blinding |
RESULTS
Study Quality
Overall, the quality of the combined evidence was moderate with all studies scoring ≥5 on the 10-point PEDro scale.28 Scores ranged from 5 (three studies)29,30,33 to 8 (one study), 32 with four studies scoring a 6 or a 7.26,31,34,35
Description of Included Studies
The included studies reported results for a total of 7,195 athletes (36% female, 64% male) ranging in levels of competition from high school to professional sports leagues. 26,29-35 The median age was 20 years. The proportion of females in the bracing group (42%) was less than in the balance training group (56%). For the six of eight studies that defined specific sport participation, the proportions of athletes participating in each sport were: 36% basketball, 29% football, 16% volleyball, and 1% soccer. One study reported that the athletes participated in either soccer or basketball without specific numbers;29 another did not specify the sports that the athletes participated in.32 The incidence of ankle sprains during sport activity was reported, although each study varied in the method of determining the occurrence of an ankle sprain. In seven of eight studies, medical professionals (athletic trainers, physical therapists and/or physicians) performed a physical exam to determine if a sprain had occurred.26,29,31-35 In one study, athletes used self-reported ankle sprain occurrences on forms that were assessed by two physicians—blinded to the study—to decipher if the subjective reports were consistent with an ankle sprain diagnosis.33
Bracing Treatment
Two of the three studies found that groups receiving bracing reported significantly lower incidence and risk of ankle sprains during athletic activity.34-35 The bracing group (n=20) in the Mohammadi study sustained fewer sprains than the control group (n=20), though this did not reach a statistically significant difference (Figure 2).26 The three braces utilized in the studies were the McDavid Ultralight34 brace (McDavid Inc, Woodridge, Illinoise), Don-Joy Ankle Stabilizing35 brace (Don-Joy Inc, Vista, California), and Sports Stirrup26 brace (Aircast Inc, Summit, New Jersey), which are shown in Appendix B. From the 3,581 combined subjects from the bracing group and control group, 432/1753 athletes sustained an ankle sprain when wearing a brace, compared to 529/1828 athletes spraining their ankle not wearing a brace. Overall, athletes wearing ankle braces had a significantly lower incidence of ankle sprains (p=0.0037) and a 64% reduced risk of ankle sprains (RR=0.36) compared to no-treatment control. (Table 3).
Balance Training Treatment
Five of the six studies found a significant decrease in the incidence of ankle sprains for athletes performing balance training compared to no-treatment controls.26,29,30,32,33 Three studies found similar values of reduced ankle sprains, ranging from 35-38%. 29,32,33 Although each of the articles utilized different balance exercises, progressions and time frames in how long to perform the exercises, they used similarly designed balance progressions to progressively challenge the visual, somatosensory, vestibular, and musculoskeletal systems. The exercises were progressed by decreasing the base of support from double to single limb stance, eyes open to eyes closed conditions, changing the surface from stable to unstable and adding perturbations, such as upper extremity motions (Appendix A). Of the combined 3,577 subjects, 178/1867 athletes in the balance training group sustained an ankle sprain compared to 274/1710 in the control group. Athletes performing balance training exercises had a significantly lower incidence of ankle sprains (p=0.0057) and a 46% reduced risk of an ankle sprain (RR=0.54) compared to no-treatment controls. (Table 3)
DISCUSSION
The results of this systematic review with meta-analysis indicate that athletes with or without a prior sprain receiving either bracing or balance training show reduced incidence and relative risk of ankle sprains compared to no-treatment controls. The results of this review demonstrated that bracing reduced the risk of a sprain by 64%, consistent with a previous systematic review that examined six randomized control trials and showed bracing reduced ankle sprains by 69%.36 The one study that compared bracing, balance training, and no-treatment was the smallest study (n=80) reviewed and both bracing and balance training reduced injury incidence compared to controls, without significant difference between bracing and balance training.26 The combined results from the three relevant studies indicate that balance training reduced risk of injury between 35-38% compared to no-treatment, which is consistent with an earlier review that found a 36% risk reduction for those athletes that participated in balance training.21
Two of the bracing studies also examined other lower extremity injuries occurrences in the bracing and control groups. 34,35 Interestingly, although ankle bracing decreased the risk of ankle injury by 64% compared to not bracing, the decreased risk for any lower extremity injury was only 25.5% compared to no treatment, leaving open the possibility that bracing at the ankle can contribute to other lower quarter injuries.34,35 Although not examined in this systematic review, the distant effects of ankle bracing should be considered. McGuine et al34 found an increased rate of injury in lower extremity injuries by 85% in the basketball players that braced compared to controls. Of these injuries, 51% were acute muscle or tendon strains in the lower leg (gastrocnemius, peroneals and Achilles), upper leg (quadriceps, hip flexor and hamstring) and hip/pelvis (adductors, gluteals). Additionally, 17.9% of the basketball players that braced at the ankle sustained an acute knee injury, in comparison to 8.8% of basketball players who did not brace. The two most common knee injuries were medial collateral ligament and anterior cruciate ligament sprains or tears.34 During peak dorsiflexion for a cutting task similar to basketball, lace-up ASO and ankle hinge braces increase peak internal rotation angle at the knee by approximately two degrees. Additionally, lace-up ASOs increase anterior knee forces during deceleration and increase knee compression forces during the peak ankle dorsiflexion moment during a cutting task.37 These increased knee forces may contribute to the higher incidence of knee injuries in athletes that braced compared to the controls in the two bracing studies.34,35 While bracing does reduce the risk of ankle sprains, an unintended consequence may be other lower extremity injuries.
The studies reviewed for the current systematic review used a variety of balance training exercises. Notable was a general progression to challenge multiple combinations of the four systems that influence postural control, including the musculoskeletal, visual, somatosensory, and vestibular systems. Conflicting (i.e. providing conflicting sensory input) one of the systems challenges another system to work harder to achieve upright balance. For example, the musculoskeletal and visual systems are challenged through the use of standing on an unstable surface with head turning, which provides conflicting information between the somatosensory and vestibular systems.38 It has been found that training on an unstable surface decreases the proprioceptive reflex, which indicates an increased reliance on visual and/or vestibular information to achieve balance.39 In the present review, the balance training exercises were progressed to incorporate the upper extremity and trunk movements in functional activities that simulate sports specific tasks. By having the athlete balance on an unstable surface, especially with perturbations, the visual system is challenged to compensate and the ankle is forced to respond in multiple planes and ranges.
Overall, both bracing and balance training demonstrated a significant effect on preventing ankle sprains in athletes from multiple sports at the competitive high school, college, and professional levels. The incidence of ankle sprains among athletes performing balance training was 10.6% while the incidence of sprains among athletes wearing braces was more than double at 24.6%. However, the relative risk for athletes wearing braces compared to controls was lower (RR=0.36) than the relative risk for athletes after balance training compared to controls (RR=0.54). Only the smallest study representing 1.1% of the pooled sample directly compared bracing to balance training, preventing any firm conclusions from being drawn with respect to which intervention was most effective. In addition, different levels of competition may present athletes of different levels of skill development, varied practice times and exposure to injury; however, there were insufficient data to compare the incidence rates per exposure among the different levels. Finally, most studies did not differentiate between athletes who did or did not have prior ankle sprains, precluding analysis between subgroups.
Limitations of this systematic review include heterogeneity of the included studies with respect to different sample sizes, statistical reporting, specific sport, competition levels, exercise protocols, and the orthoses that were utilized. In addition, this type of study poses challenges such as tracking subjects from large samples over long periods of time, lack of blinding and inconsistent compliance, and use of self-reported injury—which may miss more minor ankle sprains that did not result in reduced participation. Future research should investigate differences between subpopulations including athletes with and without prior injury or who those compete at different levels to add information regarding the effect of these interventions.
CONCLUSIONS
The results of this systematic review and meta-analysis demonstrate moderate quality of evidence for balance training or bracing to decrease the incidence and reduce the relative risk of ankle sprains in competitive athletes. Although it remains unclear whether bracing, balance training, or both combined provide the most protective effect, the results of this study may enhance clinical decision-making regarding the use of ankle braces and balance training to prevent ankle sprains among the athletic prevention.
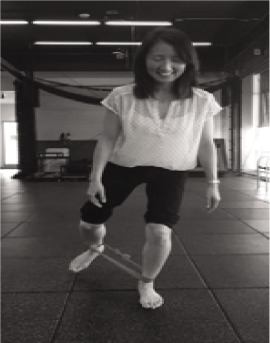
Appendix A
Exercises and variations of the balance training programs adapted from the available literature
| Exercise: Singlelegstance with the knee extended. | Exercise: Single leg stance with knee flexed (300) on foam pad | Exercise: Jump from oneleg to the other, control landing for 4 seconds | Exercise: Single leg stance performing functional activity (dribbling, catching, kicking) | Exercise: Jump from one leg to the other as you catch the ball, control landing, throw ball to partner |
| Variations: - Progress from eyes open to eyes closed. - Progress from extended knee to flexedknee - Progress contralateralleg to reaching in multiple directions (clocks) without and with theraband |
Variations: - Progress to eyes closed and/or head turning - Progress contralateralleg reaching in multiple directions (clocks) without and with theraband resistance |
Variations - Place theraband above knees while completing exercise - Jump from one leg to the other on an exercise mat without and with theraband |
Variations - Perform this activity on a foam pad |
Variations: - Place theraband above knees - Jump from one leg to other on exercise mat |
 |
 |
 |
 |
 |
Appendix B
Ankle braces utilized in the literature
| Flexible Lace-Dup | Semirigid uprights | Lace-DUp with SemiMgid stays |
|---|---|---|
| Multiplanar Support | Frontal Plane Support | Multiplanar Support |
 |
 |
 |
| McGuine et al 2011 | Mohammadi 2007 | McGuine et al 2012 |
| (McDavid Ultralight 195; McDavid Inc, Woodridge, Illinois) | (Sport-Stirrup; Aircast Inc, Summit, New Jersey) | (Don-Joy Ankle Stabilizing Brace; Don-Joy Inc., Vista, California) |
REFERENCES
- 1.McLeod MM Gribble PA Pietrosimone BG. Chronic ankle instability and neural excitability of the lower extremity. J Athl Train. 2015:50(8):847-853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mickel TM Bottoni CR Tsuji G, et al. Prophylactic bracing versus taping prevention of ankle sprains in high athletes: A prospective, randomized trial. J Foot Ankle Surg. 2006;25(6):360-365. [DOI] [PubMed] [Google Scholar]
- 3.McCriskin BJ Cameron KL Orr DJ, et al. Management and prevention of acute and chronic lateral ankle instability in athletic patient populations. World J Orthop. 2015;6(2):161-171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.American Academy of Orthopaedic Surgeons. The foot and ankle. American Academy of Orthopaedic Surgeons website. Available at http://orthoinfo.aaos.org/fact/hr_report.cfm?thread_id=100&topcategory=Foot.
- 5.Bahr R. Can we prevent ankle sprains? In: MacAuley D Best TM, eds. Evidence-Based Sports Medicine. London, England: BMJ Books; 2002:470-490. [Google Scholar]
- 6.Garrick JG. The frequency of injury, mechanism of injury, and epidemiology of ankle sprains. Am J Sports Med. 1977;5:241-242. [DOI] [PubMed] [Google Scholar]
- 7.Handoll HHG Rowe BH Quinn KM, et al. Interventions for preventing ankle ligament injuries. Cochrane Database Syst Rev. 2001;3:CD000018 Available at http://gateway2.ovid.com/ovidweb.cgi [DOI] [PubMed] [Google Scholar]
- 8.Fong DT Hong Y Chan LK, et al. A systematic review on ankle injury and ankle sprain in sports. Sports Med. 2007;37(1):73-94. [DOI] [PubMed] [Google Scholar]
- 9.Nelson AJ Collin CL Yard EE et al. Ankle injuries among United States high school sports athletes. 2005-2006. J Athl Train. 2007;42(3):381-387. [PMC free article] [PubMed] [Google Scholar]
- 10.Hubbard-Turner T Turner M. Physical activity levels in college students with chronic ankle instability. J Athl Train. 2015;50(7):742-747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Liu K Gustavsen G Royer T et al. Increased ligament thickness in previously sprained ankles as measured by musculoskeletal ultrasound. J Athl Train. 2015;50(2):193-198 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Frank C Amiel D Woo SL Akeson w. Normal ligament properties and ligament healing. Clin Orthop Related Res. 1985;196:15-25 [PubMed] [Google Scholar]
- 13.Lohrer H Nauck T Gehring D, et al. Differences between mechanically stable and unstable chronic ankle instability subgroups when examined by arthrometer and FAAM-G. J Orthop Surg Res. 2015;10:32. DOI: 10.1186/s13018-015-0171-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gabriner ML Houston MN Kirby JL, et al. Contributing factors to star excursion balance test performance in individuals with chronic ankle instability. Gait Posture. 2015;41:912-916. [DOI] [PubMed] [Google Scholar]
- 15.Springer S Gottlieb U Moran U, et al. The correlation between postural control and upper limb position sense in people with chronic ankle instability. J Foot Ankle Res. 2015;8:23. DOI: 10.1186/s13047-015-0082-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ridder R Willems TM Vanrenterghem J, et al. Effects of a home-based balance training protocol on dynamic postural control in subjects with chronic ankle instability. Int J Sports Med. 2015;36:596-602. [DOI] [PubMed] [Google Scholar]
- 17.Hoch MC Farwell KE Gaven SL et al. Weight-bearing dorsiflexion range of motion and landing biomechanics in individuals with chronic ankle instability. J Athl Train. 2015;50(8):833-839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wikstrom EA Brown CN. Minimum reporting standards for copers in chronic ankle instability research. Sports Med. 2014;44:251-268. [DOI] [PubMed] [Google Scholar]
- 19.Guillo S Bauer T Lee JW, et al. Consensus in chronic ankle instability: Aetiology, assessment, surgical indications and place for arthroscopy. Orthop Traumatol Surg Res. 2013;99S:S411-S419. [DOI] [PubMed] [Google Scholar]
- 20.Webster KA Gribble PA. Functional rehabilitation interventions for chronic ankle instability: A systematic review. J Sport Rehabil. 2010;19:98-114. [DOI] [PubMed] [Google Scholar]
- 21.Hübscher M Zech A Pferifer K, et al. Neuromuscular training for sports injury prevention: A systematic review. Med Sci Sports Exerc. 2010;42(3):413-421. [DOI] [PubMed] [Google Scholar]
- 22.Greene TA Hillman SK. Comparison of support provided by a semi-rigid orthosis and adhesive ankle taping before, during and after exercise. Am J Sports Med. 1990;18:498-506. [DOI] [PubMed] [Google Scholar]
- 23.Rovere GD Clarke TJ Yates CS et al. Retrospective comparison of taping and ankle stabilizers in preventing injuries. Am J Sports Med. 1988;16:228-233. [DOI] [PubMed] [Google Scholar]
- 24.Surve I Schwellnus MP Noakes T et al. A fivefold reduction in the incidence of recurrent ankle sprains in soccer players using the Sport-Stirrup orthosis. Am J Sports Med. 1994;22:601-606. [DOI] [PubMed] [Google Scholar]
- 25.Gross MT Liu HY. The role of ankle bracing for prevention of ankle sprain injuries. J Orthop Sports Phys Ther. 2003;33:572-577. [DOI] [PubMed] [Google Scholar]
- 26.Mohammadi F. Comparison of 3 preventive methods to reduce the recurrent of ankle inversion sprains in male soccer players. Am J Sports Med. 2007;35(6):922-926. [DOI] [PubMed] [Google Scholar]
- 27.Janssen K van Mechelen W Verhagen E. Bracing superior to neuromuscular training for the prevention of self reported recurrent ankle sprains: a three-arm randomized controlled trial. Br J Sports Med. 2014;48:1235-1239 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Moseley AM Herbert RD Sherrington C Maher CG (2002). Evidence for physiotherapy practice: A survey of the physiotherapy Evidence Database (PEDro). Australian J Physiother. 48:43-49 [DOI] [PubMed] [Google Scholar]
- 29.McGuine TA Keene JS. The effect of a balance training program on the risk of ankle sprains in high school athletes. Am J Sports Med. 2006;34(7):1103-1111. [DOI] [PubMed] [Google Scholar]
- 30.Verhagen EALM Van Tulder M Van der Beek AJ, et al. An economical evaluation of a proprioceptive balance board training program for the prevention of ankle sprains in volleyball. Br J Sports Med. 2005;39(2):111-115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Emery CA Rose SM McAllister JR, et al. A prevention strategy to reduce the incidence of injury in high school basketball: A cluster randomized controlled trial. Clin J Sport Med. 2007;17(1):17-24. [DOI] [PubMed] [Google Scholar]
- 32.Hupperets MD Verhagen EA Mechelen MV. Effect of unsupervised home based proprioception training on recurrences of ankle sprains: randomized control trial. Br Med J. 2009;339:b2684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Eils E Schröter R Schröder M, et al. Multistation proprioceptive exercise program prevents ankle injuries in basketball. Med Sci Sports Exerc. 2010;42(11):2098-2105. [DOI] [PubMed] [Google Scholar]
- 34.McGuine TA Brooks A Hetzel S. The effect of lace-up braces on injury rates in high school basketball players. Am J Sports Med. 2011;39(9):1840-1848. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.McGuine TA Hetzel S Wilson J et al. The effect of lace-up ankle braces on injury rates in high school football players. Am J Sports Med. 2012;40(1):49-57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Dizon JM Reyes JJ. A systematic review on the effectiveness of external ankle supports in the prevention of inversion ankle sprains among elite and recreational players. J Sci Med Sport. 2010;13:309-317. [DOI] [PubMed] [Google Scholar]
- 37.Klem NR Wild CY Williams SA et al. Effect of external ankle support on ankle and knee biomechanics during the cutting maneuver in basketball players. Am J Sports Med. Epub 2016 Nov. 21. DOI: 10.1177/0363546516673988 [DOI] [PubMed] [Google Scholar]
- 38.Rogers M Page P Takeshima N. Balance training for the older athlete. Int J Sports Phys Ther. 2013;8(4):517-530. [PMC free article] [PubMed] [Google Scholar]
- 39.Van Dieen J van Leeuwen M Faber G. Learning to balance on one leg: motor strategy and sensory weighting. J Neurophysiol. 2015;114(5):2967-2982 [DOI] [PMC free article] [PubMed] [Google Scholar]