

Abstract
Recently, firearm injuries in the United States have taken center stage in political debates and in the media. Much of the past epidemiological research on firearm injuries has focused primarily on the urban landscape. This study was undertaken to highlight the unique spectrum of firearm injuries seen at a rural level 1 trauma center to provide insight into prevalence, mechanism of injury, and seasonal variation. An IRB-approved retrospective study was performed of the trauma registry at a rural Level 1 hospital to identify all patients with firearm injuries from January 2002 to May 2014. Data obtained for each patient included demographics, injury date, a brief injury summary, and results of drug/ alcohol screening. Chart review was performed to confirm accuracy of the database and descriptive statistics were calculated to compare subgroups. During the 12 year study period, 408 patients with firearm injuries were treated at our hospital. There were 360 males and 48 females. Ages ranged from an infant to 90 years. Handguns were the most common type of firearm (49%). Mortality in this series was 19%. The median age for fatal and non-fatal wounds was 44 and 27 years, respectively. The three main causes of injury were accidental (36%), self-inflicted (33%), and assault (26%). Alcohol and drugs were commonly present. Hunting incidents accounted for 26% of accidents and most of these occurred while deer hunting in November and December. The demographics and mechanism of firearm injuries vary across the urban-rural continuum and it is important to identify these subgroups so targeted interventions can be pursued.
Keywords: firearm inuries, rural trauma center
Background
Recently, firearm injuries in the United States have taken center stage in political debates and in the media. This discussion often focuses on violent crimes and law enforcement, but fails to highlight unintentional injuries that are often seen in a rural community. Much of the past epidemiological research on firearm injuries has focused primarily on the urban landscape.
One may expect firearm death rates in urban areas to dwarf that of rural areas, but multiple studies have shown that population adjusted mortality rates are nearly equivalent in both settings.1 This phenomenon is not limited to the adult population, as shown by Nance et al., who found that this trend also persists in the pediatric population.2 However, the mechanism of injury differs, with the adjusted death rate in rural areas predominated by self-inflicted injuries and unintentional injuries, whereas homicide is the dominant factor in urban areas.1 The rural setting is unique, and unintentional injuries account for a significant proportion of gun related injuries.3
This study was undertaken to highlight the unique spectrum of firearm injuries seen at a rural Midwestern level 1 trauma center to provide insight into prevalence, mechanism of injury, and seasonal variation. Our goal is to identify characteristics of preventable firearm injuries to guide firearm education and public policy.
Methods
Data was gathered from a 730 bed facility located in a rural Midwestern hospital. It is the only dual certified Level 1 Adult and Level 1 Pediatric trauma center in the state.4 The facility is located in a small Midwestern town which predominantly serves a rural population in a state with a large population of hunters.
After institutional review board approval, hospital admission records following emergency department (ED) admission were retrospectively reviewed to include patients in the trauma registry at our institution. This registry was reviewed for record identifiers indicating a firearm related injury as outlined by the International Classification of Disease version 9 (ICD-9). ICD-9 utilizes the prefix “E” for external causes of injury. The firearm related E-Codes 922, 955, 965, 970, and 985 relate to accident, suicide, assault, legal intervention, and cause undetermined, respectively. Each of these codes has subsets which specify the type of weapon used in the act. Air guns are typically excluded in analyses of gunshot wounds (GSW) due to their perceived innocuous nature; however, they are included in our report to highlight their potential for significant injury. E-codes were collected from the trauma registry for the 12 year period from January 2002 to May 2014.
Data obtained for each patient included demographics, injury date, a brief injury summary, and an Abbreviated Injury Scale (AIS) score for each body region. The results of drug and alcohol screening tests were recorded. These tests were performed when the results were deemed relevant for patient care. This decision was made by the treating trauma surgeon. Additionally, the number of blood products received, intensive care unit (ICU) days, ventilator days, and hospital length of stay (LOS) were captured in addition to the ultimate incidence of in hospital mortality for the patient population. Discharge location from the hospital was also recorded for each patient. Chart review was performed to confirm accuracy of the database.
Descriptive statistics were calculated to compare subgroups in the analysis. Two-tailed T-tests were used for comparisons between groups with continuous variables and Fisher’s Exact test for comparisons between groups with categorical variables. Significance was considered p < 0.05.
Results
Demographics
During the 12 year period ranging from January 2002 to May 2014, 408 patients with firearm injuries were treated at our institution. There were 360 (88%) males and 48 (12%) females. Ages ranged from infancy to 90 years, with a mean age of 33.6 years and median of 29 years. Mortality in this series was 19% (79 patients). The median age for fatal wounds was 44 years and was significantly higher than the median age for non-fatal wounds, which was 27 years (p<0.0001). 300 (74%) patients were Caucasian (non-Hispanic), 65 (16%) were African-American, 15 (4%) were Hispanic, and 28 (7%) were Asian/ other. (Table 1)
Table I.
Demographics of patients with fatal and non-fatal injuries
| Fatal | Non-Fatal | ||
|---|---|---|---|
| N= 79 (19%) | N= 329 (81%) | ||
| Sex | |||
| Male | 71 (90%) | 289 (88%) | p=0.701 |
| Female | 8 (10%) | 40 (12%) | |
| Age (Mean/Median) | 44 / 44 | 31 / 27 | p<0.0001 |
| Race | |||
| White | 60(76%) | 240 (73%) | p=0.671 |
| Black | 6 (8%) | 59 (18%) | p=0.025 |
| Other | 13 (16%) | 30 (9%) | |
| Type of Firearm | |||
| Handgun | 52 (66%) | 146 (44%) | p=0.0007 |
| Shotgun | 7 (9%) | 65 (20%) | p=0.02 |
| Rifle | 10 (13%) | 30 (9%) | p=0.40 |
| Air Gun | 2 (3%) | 42 (13%) | p=0.007 |
| Other/ Unknown | 8 (10%) | 46 (14%) | p=0.461 |
| Toxicology (tested) | 34 (43%) | 247 (75%) | |
| ETOH | 12 (35%) | 88 (36%) | |
| Illicit Drugs | 3 (9%) | 25 (10%) | |
| ETOH+Illicit Drugs | 2 (6%) | 22 (9%) |
Type of Firearm
The firearm involved was a handgun in 198 (48%) cases, a shotgun in 72 (18%) cases, a rifle in 40 (10%) cases, an air gun in 44 (11%) cases, and a different type of weapon (other than the aforementioned; categorized as “Other”) or an unspecified weapon in 54 (13%) cases (Fig. 1). Assault was the mechanism of injury in 83% (39/47) of cases where the type of weapon was unknown. Handguns accounted for 66% of the fatal wounds and 44% of non-fatal wounds. Fatal injury was more commonly related to handgun injuries (p<0.001). (Table 1)
Figure 1:
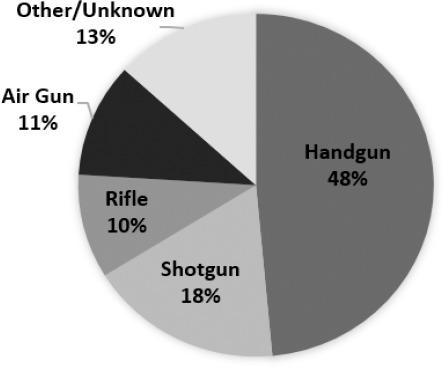
Type of firearm (408 patients)
Mechanism of Injury
The cause of injury was unintentional in 148 (36%) cases, self-inflicted in 135 (33%) cases, assault in 105 (26%) cases, police intervention in 12 (3%) cases, and undetermined in 8 (2%) cases (Fig. 2). Upon further analysis of the 148 cases that were classified as unintentional, 38 (26%) occurred while hunting.
Figure 2:
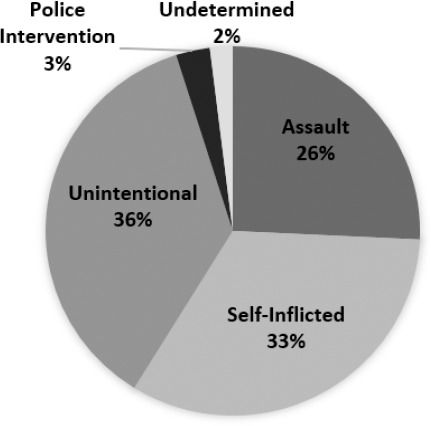
Mechanism of Injury (408 patients)
Unintentional injuries, self-inflicted injuries, and assaults accounted for 95% of all cases. Table 2 provides a breakdown of demographics among these mechanisms of injury. Males represent the majority of cases in all mechanisms of injury, but a higher rate of females were injured in cases of assault compared to other mechanisms. The mean and median age for accident and assault are in the mid to upper 20s, while the median age for self-inflicted injury is significantly higher at 44 years (p<0.0001). Caucasian individuals accounted for the majority of unintentional injuries and self-inflicted wounds with 84% and 86% of cases, respectively, while 46% of African-American individuals were assault victims. Over 93% of unintentional wounds and assaults resulted in non-fatal injuries, while nearly half of self-inflicted injuries (47%) resulted in death.
Table II.
Demographics based on mechanism of injury
| Mechanism of Injury | Significance of Association | ||||||
|---|---|---|---|---|---|---|---|
| Assault Self-Inflicted | Unintentional | Assault vs. Self-Inflicted | Assault vs. Unintentional | Self-Inflicted vs. Unintentional | |||
| N= 105 (26%) | N= 135 (33%) | N= 148 (36%) | Hunting N=38 (26%) | ||||
| Sex | |||||||
| Male | 81 (77%) | 123 (91%) | 138 (93%) | 37 (97%) | p=0.003 | p=0.0003 | p=0.515 |
| Female | 24 (23%) | 12 (9%) | 10 (7%) | 1 (3%) | |||
| Age - Mean (Median) | 29 (27) | 44 (44) | 28 (24) | 35 (33) | p<0.0001 | p=0.75 | p<0.0001 |
| Race | |||||||
| White Black | 43 (41%) 48 (46%) | 116 (86%) 5 (4%) | 125 (84%) 9 (6%) | 35 (92%) - | p<0.0001 p<0.0001 | p<0.0001 p<0.0001 | p=0.741 p<0.0001 |
| Other | 14 (13%) | 14 (10%) | 14 (9%) | 3 (8%) | |||
| Type of Firearm | |||||||
| Handgun | 55 (52%) | 86 (64%) | 42 (28%) | - | p=0.087 | p=0.0001 | p<0.0001 |
| Shotgun | 10 (10%) | 25 (19%) | 36 (24%) | 27 (71%) | p=0.07 | p=0.003 | p=0.25 |
| Rifle | 1 (1%) | 19 (14%) | 20 (14%) | 9 (24%) | p=0.0002 | p=0.0001 | p=1 |
| Air Gun | - | 1 (1%) | 42 28%) | - | p<0.0001 | ||
| Other/ Unknown | 39 (37%) | 4 (3%) | 8 (5%) | - | |||
| Outcome | |||||||
| Fatal | 7 (7%) | 64 (47%) | 6 (4%) | 1 (3%) | p<0.0001 | p=0.395 | p<0.0001 |
| Non-Fatal | 98 (93%) | 71 (53%) | 142 (96%) | 37 (97%) | |||
| ISS (Med) | 14 (9) | 21 (25) | 9 (4) | - | |||
| Toxicology (tested) | 89 (85%) | 83 (61%) | 117 (79%) | 24 (63%) | |||
| ETOH | 41 (46%) | 32 (39%) | 32 (27%) | 11 (46%) | |||
| Illicit Drugs | 25 (28%) | 23 (28%) | 34 (29%) | 10 (42%) | |||
| ETOH + Illicit Drugs | 7 (8%) | 9 (11%) | 10 (9%) | 4 (17%) | |||
The ages for the 135 self-inflicted injuries ranged from 9 to 90 years old with a mean age of 44 years. Caucasian males accounted for the majority of these injuries (105 patients, 78%). Toxicology tests were performed on 83 self-inflicted cases (61%) and of those tested, 32 individuals (39%) were positive for alcohol, 23 (28%) had illicit drugs, and 9 patients (11%) had a combination of both illicit drugs and alcohol. In comparison, toxicology tests in those 117 patients (79%) with unintentional firearm injuries who were tested indicated that 32 individuals (27%) were positive for alcohol, 34 (29%) had illicit drugs, and 10 patients (9%) had both illicit drugs and alcohol.
Injury location
The locations of the GSWs were characterized as head/ neck, face, chest, abdomen, extremities, and skin. In 153 patients (38%) there were multiple locations of injury. There was a single injury location in the other 255 cases (63%), with extremity injuries accounting for 77 cases, 51 cases of skin injuries, 47 cases of head injuries, 42 cases of facial injuries, 21 cases of abdominal injuries, and 17 cases of chest injuries. The primary location of injury was evaluated for rifle, shotgun, and handgun injuries by recording the body location with the highest AIS score. (Table 4) The head/ neck region was the most common primary site of injury in handgun (43%) and rifle (40%) wounds, with p values of p<0.001 and p=0.05, respectively, when compared to shotgun wounds. Extremity injuries were the most common primary injury location in shotgun wounds (39%).
Table IV.
Demographics based on type of firearm
| Firearm | Significance of Association | ||||||
|---|---|---|---|---|---|---|---|
| Total Patients N=408 | Handgun N= 198 | Shotgun N=72 | Rifle N=40 | Handgun vs. Shotgun | Handgun vs. Rifle | Shotgun vs. Rifle | |
| Primary Injury Location | |||||||
| Head/ Neck | 86 (43%) | 18 (25%) | 16 (40%) | p<0.001 | p=0.73 | p=0.05 | |
| Face | 10 (5%) | 6 (8%) | 1 (3%) | p=0.38 | p=0.70 | p=0.42 | |
| Chest | 22 (11%) | 8 (11%) | 4 (10%) | p=1 | p=1 | p=1 | |
| Abdomen | 17 (9%) | 4 (6%) | 2 (5%) | p=0.61 | p=0.75 | p=1 | |
| Extremity | 42 (21%) | 28 (39%) | 12 (30%) | p=0.005 | p=0.22 | p=0.41 | |
| Skin | 21 (11%) | 8 (11%) | 5 (13%) | p=1 | p=0.78 | p=1 | |
| Disposition | |||||||
| Admitted | 372 (91%) | 146 (74%) | 65 (90%) | 30 (75%) | p=0.003 | p=1 | p=0.05 |
| Home, no assistance | 218 (59%) | 91 (62%) | 33 (51%) | 23 (77%) | p=0.13 | p=0.15 | p=0.02 |
| Additional Assistance Healthcare | 94 (25%) | 45 (31%) | 29 (45%) | 6 (20%) | p=0.06 | p=0.28 | p=0.02 |
| Skilled Nursing | |||||||
| Facility/Rehab/Acute Care Hosp. | 50 (13%) | 25 (17%) | 11 (17%) | 3 (10%) | |||
| Home, w/ home health | 28 (8%) | 9 (6%) | 16 (25%) | - | |||
| Inpatient Psychiatry | 13 (3%) | 9 (6%) | 1 (2%) | 3 (10%) | |||
| Home Hospice | 3 (<1%) | 2 (1%) | 1 (2%) | - | |||
| Other | |||||||
| Jail/Prison | 15 (6%) | 9 (6%) | 3 (5%) | - | |||
| Left AMA | 2 (<1%) | 1 (<1%) | - | 1 (3%) | |||
Medical Utilization
As seen in Table 3, multiple metrics outlining hospital resource utilization including total LOS, ICU LOS, blood product utilization, and ventilator days were captured and analyzed. In total, 372 (91%) of patients were admitted, including over 90% of victims within the three mechanistic subsets. The LOS for self-inflicted wounds was significantly greater than assault and unintentional victims, p<0.002 and p<0.0001, respectively. Blood products were administered to 130 (32%) patients and more self-inflicted wounds received blood than all other modalities combined. Patients with self-inflicted injuries received blood products in 50% of cases and were significantly more likely to receive blood than the other injury modalities (vs. assault p=0.0037 & vs. unintentional p<0.0001). Overall, 179 (44%) patients were admitted to an ICU. Self-inflicted injuries were the most likely to result in ICU admission as seen 97 patients (72%) (p<0.0001). There was not a significant difference between the injury cause with respect to the number of blood products received, ICU LOS, or ventilator days (all p>0.05).
Table III.
Hospital resource utilization
| Mechanism of Injury | Significance of Association | ||||||
|---|---|---|---|---|---|---|---|
| Total Patients N=408 | Assault N= 105 | Self-Inflicted N=135 | Unintentional N=148 | Assault vs. Self-Inflicted | Assault vs. Unintentional | Self-Inflicted vs. Unintentional | |
| Resource Utilization | |||||||
| Total Length of Stay | |||||||
| Admitted (%) | 372 (91%) | 97 (92%) | 126 (93%) | 134 (91%) | p=0.80 | p=0.66 | p=0.514 |
| Mean / Median LOS (days) | 6.5 / 4 | 11.5 / 4 | 5.3 / 3 | p<0.002 | p=0.25 | p<0.0001 | |
| Blood Products | |||||||
| Packed patients Red (%) Blood Cells, | 130 (32%) | 33 (31%) | 68 (50%) | 29 (20%) | p=0.0037 | p=0.39 | p<0.0001 |
| Mean patient) / Median (units per | 8.1 / 3 | 6.9 / 4 | 5.6 / 4 | p=0.56 | p=0.36 | p=0.55 | |
| Intensive Care Unit | |||||||
| Admitted to ICU (%) | 179 (44%) | 49 (47%) | 97 (72%) | 33 (22%) | p=0.0001 | p<0.0001 | p<0.0001 |
| Mortality (%) | 6 (12%) | 43 (44%) | 5 (15%) | ||||
| Mean / Median LOS (days) | 3.7 / 2 | 4.2 / 2 | 6.3 / 3 | p=0.63 | p=0.14 | p=0.20 | |
| Ventilator (patients) | 155 (42%) | 35 (36%) | 89 (71%) | 23 (17%) | |||
| Mean / Median (days) | 3.7 / 1 | 3.2 / 1 | 5.3 / 2 | p=0.70 | p=0.40 | p=0.21 | |
| Disposition (if admitted) | |||||||
| Home, no assistance | 218 (59%) | 65 (67%) | 26 (21%) | 118 (80%) | p<0.0001 | p=0.00014 | p<0.0001 |
| Additional Assistance Healthcare | 94 (25%) | 27 (28%) | 40 (32%) | 23 (17%) | p=0.558 | p=0.074 | p=0.009 |
| Skilled Nursing Facility/ | |||||||
| Rehab/Acute | |||||||
| Care Hosp. | 50 (13%) | 19 (20%) | 16 (13%) | 15 (11%) | |||
| Home, w/ home health | 28 (8%) | 8 (8%) | 9 (7%) | 8 (6%) | |||
| Inpatient Psychiatry | 13 (3%) | - | 12 (10%) | - | |||
| Home Hospice | 3 (<1%) | - | 3 (2%) | - | |||
| Other | |||||||
| Jail/Prison | 15 (4%) | 5 (5%) | 5 (4%) | - | |||
| Left AMA | 2 (<1%) | 1 (<1%) | - | 1 (<1%) | |||
Temporal Association and Hunting
As seen in Figure 3, the months of November and December account for 34% of all unintentional injuries, while the months of January, February, May, and June show slightly higher rates of self-inflicted injuries (Figure 3 depicts the incidence of hunting accidents by month. Hunting firearm injuries occurred primarily while deer hunting (22/38; 58%). The other unintentional hunting accidents were associated with pheasant (8), raccoon (1), waterfowl (1) and 6 were undetermined.
Figure 3:
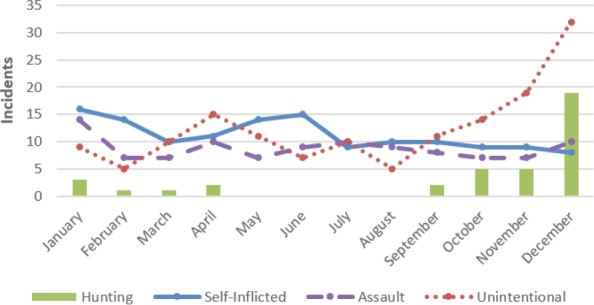
Seasonal variation based on mechanism of injury
Firearm injuries associated with hunting accounted for 38 (26%) of the unintentional cases. This subset exhibits notable variations from the data set as a whole. Demographically, 37 of the patients (97%) were male, 35 (92%) were Caucasian, and age ranged from 15 to 68 years with a mean of 35 years and median of 33 years. The type of firearm implicated in hunting injuries was a shotgun in 27 cases (71%) and a rifle in 9 (24%) cases. Toxicology tests were performed on 24 (63%) of the patients, and of those tested, 11 individuals (46%) had alcohol, 10 (42%) had illicit drugs, and 4 patients (17%) had a combination of both illicit drugs and alcohol. In 8 hunting cases (21%) there were multiple locations of injury. There was a single injury location in the other 30 incidents, with extremity injuries accounting for 26 cases.
Discharge Disposition
Disposition for admitted patients was analyzed in the data set and 218 (59%) patients were discharged home with no assistance, while 94 (25%) patients required higher level care (Table 3 and 4). Victims of unintentional injuries and assaults were dispositioned home with no assistance in 80% and 67% of cases, respectively, which was significantly more often than victims with self-inflicted wounds (32%) (p<0.0005). Shotgun injuries resulted in admission 90% of the time, which was significantly more than handgun (p=0.003) and rifle (p=0.05) injuries. The majority of handgun, shotgun, and rifle injuries went home with no assistance. Shotgun injuries had the largest cohort (45%) which required additional healthcare assistance compared to handgun (p=0.06) and rifle (p=0.02) injuries.
Age of Patient
Analysis of the data by age highlighted trends in mechanism of injury, sex, race, and mortality rate. Unintentional injuries are most common in the 2nd and 3rd decades of life, while self-inflicted injuries are most common between the 3rd and 6th decades of life, peaking in the 5th decade. Furthermore, self-inflicted injuries accounted for 73% of cases after the age of 59. The data indicates assaults are common among young people with 87% of cases occurring between the 2nd and 4th decade of life.
Discussion
Firearm violence in this country is increasingly highlighted in the media, stirring social activism, and has become a contentious debate in national politics. This public focus on gun violence requires a detailed look at the entire spectrum of these unique injuries in various regions of the country. The variability in firearm injuries between urban and rural areas has garnered increasing interest over the past decade. Reports have looked at this problem through a number of different lenses to include urban-rural differences in unintentional fatalities, pediatric fatalities, intentional fatalities (suicide and homicide), and other trends at a national level. Fatalities from firearm injuries do not capture the majority of injuries and only represent 19% of the cases in our data set, 20-36% in other rural data sets, and 33% on the national level.3,5 Thus, comparison across studies reporting solely on fatalities is problematic and using this viewpoint as a measure of this public health problem can greatly underestimate the magnitude of the issue.
Demographic and Regional Variation
As highlighted in our data set, the predominant mechanism of injury varies between urban and rural settings. Additionally, the demographics and firearms also vary among mechanism of injury. Few studies have looked at this issue from the perspective of a rural trauma center. This snapshot into firearm injuries at our institution may not be directly generalizable at a national rural level, as highlighted by Fowler et al. who showed that significant geographic variation is present nationally, with 46% of firearm fatalities occurring in the south compared to approximately 20% in the Midwest and Western U.S., respectively.5 As such, our analysis of rural Midwest firearm injuries at a level 1 trauma center provides valuable insight into this issue and, to our knowledge, stands alone as the only report of its kind.
Similar to other studies, our data showed a disproportionate male predominance representing 88% of total cases, which is consistent with numerous previous studies across both rural and urban settings.5,7 However unlike other studies, females in our environment were disproportionally more at risk for assault. Compared to a national study conducted by Fowler et al. in 2010-2012 which noted 11% of assaults were perpetrated against females, our rural data set recorded a value more than double that at 23%.5 This was also more than another rural analyses, which noted 14% of assault victims were female.7
One study at a rural level 2 trauma center demonstrated that long guns resulted in injury in 60% of cases but in our population handguns were the most common type of firearm, representing 48% of cases and accounting for 66% of fatalities.3 Other rural analyses in North Carolina and Washington also demonstrated handguns as the predominate firearm used in fatal cases, however at a lower level of 51% and 53%, respectively.8 This data shows that handgun violence is not restricted to urban inner city environments since it was common and often lethal in our series.
Drug and Alcohol Association
Our data indicates drug and alcohol use are commonly associated with firearm injuries in a rural environment. Of those individuals tested, our data set indicates 71% of hunters and 55% of patients with self-inflicted injuries had alcohol and/ or drugs in their system. Alcohol was present in 39% of tested patients with self-inflicted injuries. Alcohol and drug use have widely been accepted as lubricants to unintentional trauma. However, at a national level, Loder et al. evaluated a dataset of 1.8 million firearm injuries and found alcohol involvement in 6.7% of non-hunting cases and 1.5% of hunters.9 Branas et al. explored the relationship with firearms and noted an association between acute alcohol consumption and higher incidence of firearm suicide.10 Nationally, the CDC reported that nearly 35% of homicide and suicide victims in 2007 tested positive for alcohol.11
Medical Utilization
Self-inflicted firearm injuries accounted for over a third of the patient in our series. Injuries caused by this mechanism required higher medical resource utilization by multiple metrics. These patients had more blood transfusions (50%), more likely to be admitted to the ICU, and had a longer hospital length of stay. This significant difference compared to patients that suffered unintentional injuries or assaults can be accredited to the fact that these injuries more likely involved critical body areas including the head or chest.
Unintentional Injuries
Unintentional injuries are the most common type of firearm injury in our rural dataset. However, this mechanism represents the smallest fatality rate amongst the three mechanisms of injury at 8%. Dresang et al. also noted this trend in their series, highlighting that 3% of fatalities in a rural setting were unintentional.8 Fowler et al. on a national level also found that unintentional firearm injuries account for 2% of urban fatalities.5 The months of November and December had a spike in incidents which accounted for over one-third of all accidents, with 47% of those cases related to hunting. Data from the 2014 International Hunter Education Association shows that Iowa has the highest percentage of firearms accidents nationally as a function of total license holders.12
Hunting Injuries
Hunting accidents were common in our series and are often associated with long guns, similar to previously reported series.3 Hunting and sport shooting beyond being merely a recreational activity are a way of life in many rural parts of the country, as evidenced by 13.7 million hunters across the United States in 2011.13 Residents of a metropolitan area greater than 1 million hunted at a rate of 3% compared to 18% of those in cities of less than 50,000.13 Successful completion of a hunter’s safety course is a state requirement for a hunting license in Iowa, which many individuals complete in their teenage years. However, the median age of hunting accidents from our data was 32 years old, which suggests that an impactful public health intervention could include a requirement for a refresher course and warnings for hunters in an effort to reduce complacency and reinforce safe practices later in life.
Diversity
Demographically, our region lacks the racial and ethnic diversity that one would expect to find in an urban environment. Data from the 2010 census for the county in which our institution resides estimated the population as 83% Caucasian, 7% Asian, 6% African American, and the remaining 4% as Other.14 As shown in Table 2, the rates of unintentional and self-inflicted injuries align with the demographic data from the census bureau and are dominated by Caucasian individuals. However, African American individuals are more commonly victims of assault. These demographic correlations among the three mechanistic categories were also found in a rural North Carolina investigation with comparable demographics.7
Gun deaths by suicide have topped those via homicides over the past 30 years, with 61% of gun deaths in 2010 attributable to suicide.11 Self-inflicted injury, as a percentage of total fatalities, was a common mechanism in our series, accounting for 81% of the fatalities, which was higher than 59% in another rural data set and 64% nationally.5,7 However, the mortality of self-inflicted injuries in our series was only 47% compared to 85% of suicides by firearm nationally.5 Our data did not show significant seasonal variation of suicides or annual variation correlated with economic downturns.
Unknown Firearm Type
One weakness of our series is the substantial number of cases that had an unknown firearm type. There were 47 cases that despite further chart review we were unable to determine the type of firearm. The majority (39/47 cases) were from assaults where the perpetrator’s weapon was not noted. We can assume that handguns were the predominant weapon used given that 83% of assaults with a known weapon type were with a handgun.
Conclusion
Unintentional firearm injuries are common in rural Midwestern hospitals. A higher percentage of firearm injuries are unintentional compared to urban centers and there are significant modifiable risk factors unique to this region that could have an impact on the incidence of these costly injuries. This series highlighted the seasonal variation of firearm injuries seen at these centers associated with hunting season. Unintentional injuries occurred most commonly in the fourth decade of life and refresher hunting courses and warnings may be beneficial later in life for hunters. The danger of combining drugs and alcohol use with firearms is strongly highlighted in this series. The over representation of African-American individuals and women as the victims of assault emphasizes the need for interventions for these high risk groups. We hope this information will be used to identify avenues for improved firearm safety in rural environments.
References
- 1.Branas CC, Nance ML, Elliott MR, Richmond TS, Schwab CW. Urban-rural shifts in intentional firearm death: different causes, same results. Am J Public Health. 2004;94(10):1750–5. doi: 10.2105/ajph.94.10.1750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Nance ML, Denysenko L, Durbin DR, Branas CC, Stafford PW, Schwab CW. The rural-urban continuum: variability in statewide serious firearm injuries in children and adolescents. Arch Pediatr Adolesc Med. 2002;156(8):781–5. doi: 10.1001/archpedi.156.8.781. [DOI] [PubMed] [Google Scholar]
- 3.Dodge GG, Cogbill TH, Miller GJ, Landercasper J, Strutt PJ. Gunshot wounds: 10-year experience of a rural, referral trauma center. Am Surg. 1994;60(6):401–4. [PubMed] [Google Scholar]
- 4. University of Iowa Healthcare 2015. Basic Facts. [Available from: www.uihealthcare.org.
- 5.Fowler KA, Dahlberg LL, Haileyesus T, Annest JL. Firearm injuries in the United States. Prev Med. 2015;79:5–14. doi: 10.1016/j.ypmed.2015.06.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Carr BG, Nance ML, Branas CC, Wolff CS, Kallan MJ, Myers SR, et al. Unintentional firearm death across the urban-rural landscape in the United States. J Trauma Acute Care Surg. 2012;73(4):1006–10. doi: 10.1097/TA.0b013e318265d10a. [DOI] [PubMed] [Google Scholar]
- 7.Sadowski LS, Munoz SR. Nonfatal and fatal firearm injuries in a rural county. JAMA. 1996;275(22):1762–4. doi: 10.1001/jama.1996.03530460066034. [DOI] [PubMed] [Google Scholar]
- 8.Dresang LT. Gun deaths in rural and urban settings: recommendations for prevention. J Am Board Fam Pract. 2001;14(2):107–15. [PubMed] [Google Scholar]
- 9.Loder RT, Farren N. Injuries from firearms in hunting activities. Injury. 2014;45(8):1207–14. doi: 10.1016/j.injury.2014.04.043. [DOI] [PubMed] [Google Scholar]
- 10.Branas CC, Richmond TS, Ten Have TR, Wiebe DJ. Acute alcohol consumption, alcohol outlets, and gun suicide. Subst Use Misuse. 2011;46(13):1592–603. doi: 10.3109/10826084.2011.604371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Centers for Disease Control and Prevention. Surveillance for violent deaths-National Violent Death Reporting System, 16 states, 2007. MMWR Morb Mortal Wkly Rep 2010 59:1-50. (No. SS-4). [PubMed]
- 12. International Hunter Education Association. 2015 Program Profile. [Available from: http://www.ihea.com/news-and-events/news/program-profile.
- 13. U.S. Department of the Interior FaWS, and U.S. Department of Commerce, U.S. Census Bureau. 2011 National Survey of Fishing, Hunting, and Wildlife-Associated Recreation. [Available from: http://www.census.gov/prod/2012pubs/fhw11-nat.pdf.
- 14. Bureau USC. State & County QuickFacts. [Available from: https://www.census.gov/quickfacts/table/PST 045215/1938595,00.