

Abstract
Objectives:
The Brooker classification is a commonly used tool to characterize the extent of heterotopic ossification (HTO), which is the dystrophic formation of mature lamellar bone in non-osseous tissues such as muscles, connective tissue or nerves. We aim to provide illustrative cases to describe the limitations and challenges of this system.
Methods:
A retrospective review was conducted in all patients who had retrieved hip and/or pelvic radiotherapy for HTO prophylaxis at Sunnybrook Health Sciences Centre between July 1998 and August 2016. An independent musculoskeletal radiologist who was blinded to the condition of the patient and the clinical outcome evaluated the imaging studies based on the Brooker classification.
Results:
22 patients were identified for analysis. Three patient cases were presented to illustrate the discrepancies between the Brooker classification and radiographic images, CT images and different radiographical projections. Two patient cases were presented to demonstrate the inability of the Brooker classification to account for volumetric differences in HTO and arthroplasty lengths.
Conclusion:
Although the Brooker classification for HTO is a widely used quantitative and qualitative assessment tool given its simplicity and familiarity, it possesses several limitations. Utilization of other radiographic modalities, such as CT, and orthogonal projections may reduce ambiguities from using the HTO system. Development of a classification method that can appropriately correspond to the clinical outcomes such as functional capabilities to further HTO development is warranted.
Advances in knowledge:
The present study critically evaluated the Brooker classification system, and identified areas in which improvement is warranted on characterizing HTO. This is important in further research that aims to improve the accuracy of HTO classification guidelines.
Keywords: Heterotopic ossification, Brooker Classification
Introduction
Heterotopic ossification (HTO) is the dystrophic formation of mature lamellar bone in non-osseous tissues such as muscles, connective tissue or nerves.1,2 It is a potential consequence of traumatic injury, elective surgery, neurological insult or severe burns and is most commonly found in the hips followed by the elbow, knees and temporomandibular joint.3 Although mild HTO may be asymptomatic, higher degrees of ossification may result in severe pain, limited mobility, functional impairment and an overall reduction in quality of life.4 Common risk factors for HTO development include the male gender, diffuse idiopathic skeletal hyperostosis, ankylosing spondylitis, osteoarthritis and previous HTO formation.2,5
The Brooker classification (Figure 1) was one of the earliest proposed schemes employed to stratify the degree of hip HTO formation and it remains widely used in contemporary literature.6,7 This classification system divides the extent of HTO formation into four grades. Grade I describes small separate small foci of bony islands within the soft tissues about the hip. Grade II consists of ossifications projecting from the proximal femur or pelvis with at least 1 cm between opposing bone surfaces. Grade III includes bone spurs originating from the proximal femur or pelvis with a separation distance of less than 1 cm. Grade IV describes complete ossification bridging between the proximal femur and pelvis.
Figure 1.
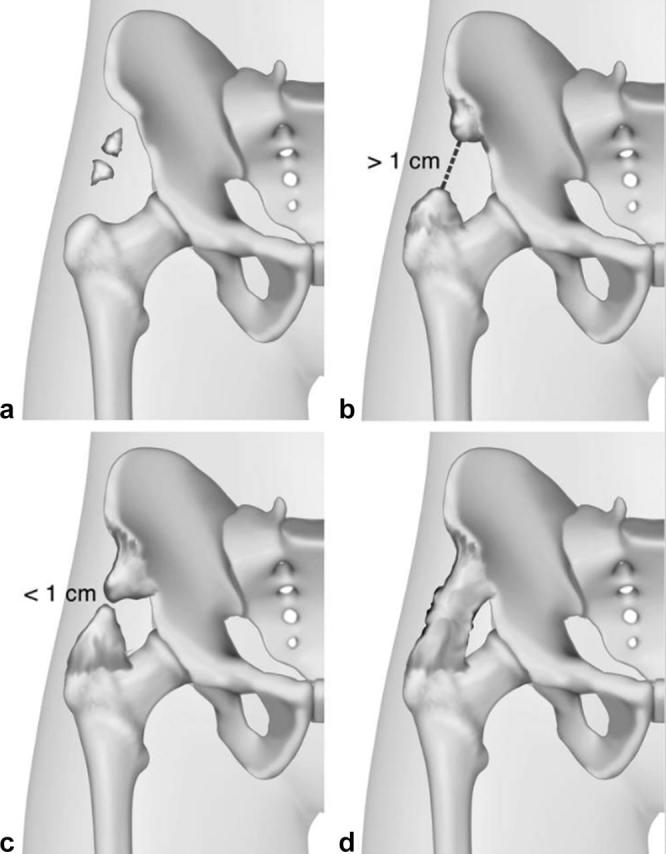
The Brooker classification of hip heterotropic ossification.6,7
Despite its widespread use, the Brooker classification is not without its limitations. To our knowledge, this is the first study that provides illustrative cases highlighting such limitations and challenges.
Methods and materials
Institutional Research Ethics Board approval was obtained to perform a retrospective review of all patients who had retrieved hip and/or pelvic radiotherapy for HTO prophylaxis at Sunnybrook Health Sciences Centre between July 1998 and August 2016. A total of 22 patients were identified for analysis. Only illustrative cases were included for the purpose of this case series. An independent musculoskeletal radiologist who was blinded to the condition of the patient and the clinical outcome evaluated the imaging studies based on the Brooker classification.
Results
Brooker classification discrepancies between radiographic and CT images
Case 1
The radiographic and CT findings of a paraplegic patient with extensive HTO are shown in Figures 2, 3. This patient initially presented with bilateral hip pain stemming from the ossification and decided to undergo radiotherapy for management as he was not a suitable candidate for surgical treatment. He subsequently underwent a single 8 Gy radiation treatment to the pelvis and bilateral hips which provided him with symptomatic relief.
Figure 2.

AP radiograph of the pelvis demonstrating heterotopic ossification in both hips with Grade III Brooker classification in the right hip and Grade IV in the left hip.
Figure 3.

Coronal reformatted CT image (a) demonstrating incomplete fusion of ossification bilaterally with a corresponding absence of ankyloses at the left hip on the sagittal reformatted image (b).
The following images were obtained prior to the treatment with the plain radiograph 3 months prior to and CT images 2 weeks prior to the radiotherapy. Radiographically, the Brooker classification was Grade III for the right hip and Grade IV for the left hip as the bone spurs originating from the right pelvis and femur but did not completely ankylose but was less than 1 cm apart, whereas the left side appears to have completely fused with one another. Subsequent CT images demonstrated incomplete fusion of ossification bilaterally which effectively downgrades the previous classification grade.
Case 2
The following radiographic and CT findings (Figures 4, 5) depict a patient who was involved in a motor vehicle accident resulting in extensive fractures to the left pelvis, right pubic ramus and acetabulum requiring open reduction internal fixation with an extended iliofemoral approach. She received a single 7 Gy radiation treatment to the left hemipelvis on post-operative day 1 for prophylaxis of HTO development.
Figure 4.

AP radiograph of the pelvis demonstrating acetabular reconstruction plate with multiple screw fixations and heterotopic ossification (Brooker Grade I) at left hip.
Figure 5.

Coronal reformatted CT image (a) and axial CT image (b) demonstrating extensive HTO (Brooker Grade III) spanning the left proximal femur to the acetabular surface without evidence of complete fusion.
The plain radiograph (Figure 4) 3 months post-operatively demonstrates the previous left acetabular fracture with posterior column reconstruction plates and multiple interfragmentary screw fixations. There is evidence of HTO development to the lateral hip that was classified as Grade I classification. A subsequent CT (Figure 5) was obtained for evaluation of possible avascular necrosis 6 days following the radiographic assessment revealed a Grade III classification given the extent of ossification on the axial and sagittal images.
Overall, the utilization of CT for evaluation of HTO has significantly expanded since the initial creation of the Brooker classification. In comparison with plain radiographs, CT scans have superior spatial and contrast resolution which enables the detection of subtle focal mineralization in the earlier stages of ossification.8 Typical CT findings include low-attenuation soft tissue masses or an enlarged muscle belly which is occasionally indistinct from adjacent soft tissue planes.9,10 This may in turn result in higher classification grades as seen in the second presented case. On the other hand, overlapping ossifications may grossly overestimate the grade classification on the anteroposterior radiograph which may be rectified with CT assessments as seen in the first presented case. Therefore, when CT images acquisitions are available for comparison, it is beneficial to make correlations with the existing plain radiographs in order to provide the most accurate HTO grade classification.
Brooker classification discrepancies between different radiographic projections
Case 3
The following radiographic images (Figure 6) illustrate a patient who sustained a motor vehicle accident resulting in multiple injuries including a double column fracture of the right acetabulum extending to the iliac margin of the right sacroiliac joint with medial displacement of the posterior column. The posterior column fracture was complex and involved a surgical reconstruction of the acetabulum using an iliofemoral approach. Given the extent of the surgery, he underwent a single 7 Gy on post-operative day 1 to minimize the risk of heterotopic bone formation.
Figure 6.

Anteroposterior projection (a) of the pelvis demonstrates an apparent fusion of the bony ossification at the right hip. A subsequent left posterior-oblique projection of the pelvis (b) demonstrates an incomplete heterotrophic ossification fusion at the right hip.
The plain radiograph shown in Figure 6a was taken 6 months following the irradiation treatment. It demonstrates open reduction internal fixation of the right acetabular fracture with multiple reconstruction plates and intrafragmentary screws across the acetabulum and right iliac wing. The HTOs were classified as Brooker Grade IV as it spanned the lateral joint margin without interruption. In the follow-up radiograph shown in Figure 6a,b, Judet left posterior-oblique projection was obtained along with the anteroposterior views. By placing the right hip to profile, it can be seen that there is in fact a small separation gap between the proximal and distal ossifications which in effect downgraded the previous classification.
As the Brooker classification is strictly based on a single anteroposterior radiographic projection, overlapping ossifications may be confused with complete fusions which may subsequently result in higher classification grades. Such ambiguities may be overcome with oblique radiographic projections, such as the Judet views, which will place the area of interest in profile and thus delineate superimposed structures.
Unaccountability of volumetric differences in heterotropic ossification in the Brooker classification
Case 4
The following radiograph (Figure 7) illustrates a patient who underwent a left hip total arthroplasty secondary to polyethylene liner wear. Following his initial operation, he developed significant HTO in the hip abductor muscles and vastus lateralis which was excised during this revision. Given the patient’s high propensity of HTO development, a single 8 Gy dose of radiotherapy was applied post-operatively to the left hip without complications.
Figure 7.
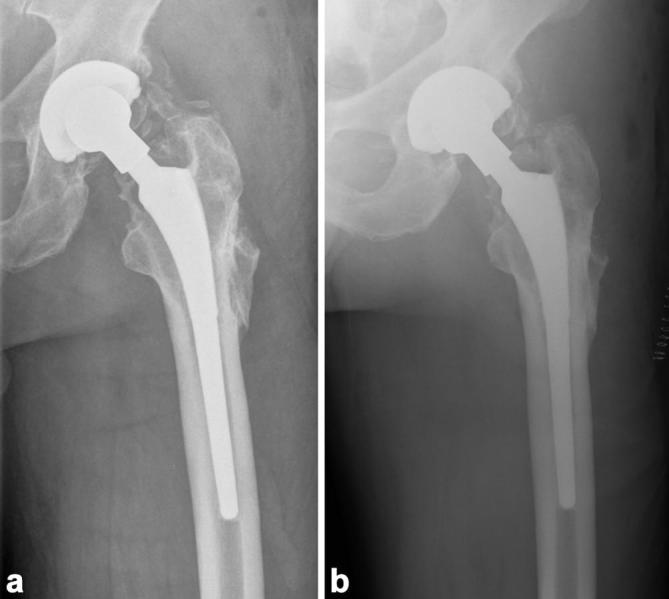
Anteroposterior radiograph of the left hip demonstrating HTO (Brooker Grade II) immediately post-operatively (a). A subsequent AP radiograph 2 months following the surgery illustrates an overall reduction in HTO volume, despite lack of reduction in separation distance between opposing bony surfaces (b).
The plain radiograph shown in Figure 7a was taken immediately following the hip revision. It demonstrates an uncemented total hip arthroplasty with HTO spanning between the pelvis and proximal femur. The separation between the bony spurs was greater than 1 cm in length which makes it a Brooker Grade II classification. A follow-up radiograph shown in Figure 7b was subsequently taken 2 months after the revision and radiotherapy. Irrespective of the differences in radiographic techniques, there is an overall reduction in HTO volume, despite no changes in the separation distance between the proximal and distal segments. As a result, the overall Brooker classification remained unchanged.
The criteria for the Brooker classification, especially with respect to Grade II and III, are quite limited as it is largely based on the absolute distance between opposing bony surfaces. Although it is difficult to perform exact volumetric quantification on plain radiographs, it is an important variable as it is related to the overall functional range of motion and ease of surgical excisions. Furthermore, variations in radiographic techniques are an important consideration as it may alter the apparent size of HTO or may completely render it undetectable.
Unaccountability of arthroplasty lengths in the Brooker classification
Case 5
The following patient has a complex history of right acetabular fracture following a motor vehicle accident requiring an open reduction internal fixation complicated by avascular necrosis, septic joint with debridement and insertion of antibiotic spacers, and multiple revisions. The radiographs depicted in Figure 8 were obtained before and immediately after the operation and involved removal of an antibiotic spacer and revision of right total hip arthroplasty. The bone spurs are less than 1 cm apart preoperatively which results in a Grade III classification compared with a Grade II classification post-operatively as the opposing ossification were more than 1 cm apart. Close examination does not demonstrate loss of HTO volume, rather lengthening of the arthroplasty resulting in a wider separation between the bony fragments which effectively accounts for the downgrading of Brooker classification. Again, as this classification system is based on the absolute measurements between opposing ossification surfaces, it is important to take into consideration potential, mechanical or iatrogenic causes for the apparent changes in distance separation.
Figure 8.
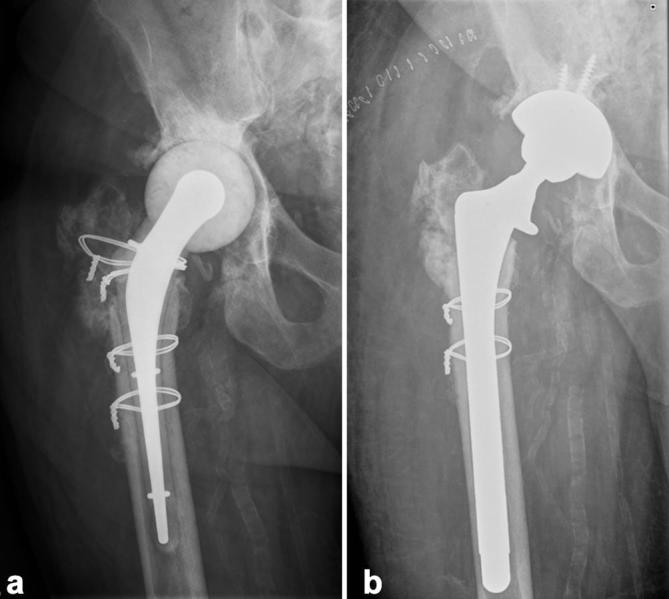
Anteroposterior radiograph (a) of the right hip demonstrating a cement mold femoral hemiarthroplasty with associated heterotrophic ossification (Brooker Grade II).(b) demonstrates interval surgery with removal of cement from mold arthroplasty and placement of a non-cemented total arthroplasty and apparent widening of opposing ossification surfaces (white arrow).
Discussion
The Brooker classification for HTO is a widely used quantitative and qualitative assessment tool given its simplicity and familiarity. However, there is limitation of the Brooker classification. Specific challenges include superimposing structures, variations in radiographic technique and unaccountability for differences in volumetric measurements and arthroplasty lengths. Utilization of other radiographic modalities, such as CT, and orthogonal projections may reduce such ambiguities. Ultimately, a good classification system should appropriately correspond to clinical outcomes. Few studies have explored the clinical significance of the Brooker classification as a prognosticator for functional capabilities or a further HTO development. Future studies examining such area are warranted.
Funding
We also thank the generous support of Bratty Family Fund, Michael and Karyn Goldstein Cancer Research Fund, Joey and Mary Furfari Cancer Research Fund, Pulenzas Cancer Research Fund, Joseph and Silvana Melara Cancer Research Fund and Ofelia Cancer Research Fund.
Acknowledgment
We thank Marko Popovic, Milica Milakovic, Dr Srini Raman, Stephanie Chan, Pearl Zaki, Rachel McDonald and Leigha Rowbottom in this project.
Contributor Information
Tao Mary Jiayi, Email: jiayi.tao@mail.utoronto.ca.
Probyn Linda, Email: linda.probyn@sunnybrook.ca.
Poon Michael, Email: mike.poon@mail.utoronto.ca.
Kreder Hans, Email: Hans.Kreder@sunnybrook.ca.
Nousiainen Markku, Email: Markku.Nousiainen@sunnybrook.ca.
Jenkinson Richard, Email: richard.jenkinson@sunnybrook.ca.
Wan Bo Angela, Email: angela.wan@sunnybrook.ca.
Tsao May, Email: may.tsao@sunnybrook.ca.
Barnes Elizabeth, Email: elizabeth.barnes@sunnybrook.ca.
Chow Edward, Email: edward.chow@sunnybrook.ca.
References
- 1.Baird EO, Kang QK. Prophylaxis of heterotopic ossification—an updated review. J Orthop Surg Res 2009; 4: 12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Popovic M, Agarwal A, Zhang L, Yip C, Kreder HJ, Nousiainen MT, et al. Radiotherapy for the prophylaxis of heterotopic ossification: a systematic review and meta-analysis of published data. Radiother Oncol 2014; 113: 10–17. [DOI] [PubMed] [Google Scholar]
- 3.Balboni TA, Gobezie R, Mamon HJ. Heterotopic ossification: pathophysiology, clinical features, and the role of radiotherapy for prophylaxis. Int J Radiat Oncol Biol Phys 2006; 65: 1289–99. [DOI] [PubMed] [Google Scholar]
- 4.Garland DE. A clinical perspective on common forms of acquired heterotopic ossification. Clin Orthop Relat Res 1991; 263: 13–29. [PubMed] [Google Scholar]
- 5.Taussky D, Cserhati M, Pescia R. Preoperative radiotherapy without femoral shielding for prevention of heterotopic ossification in hydroxyapatite-coated hip prostheses. Arch Orthop Trauma Surg 2001; 121: 271–3. [DOI] [PubMed] [Google Scholar]
- 6.Brooker AF, Bowerman JW, Robinson RA, Riley LH Jr. Ectopic ossification following total hip replacement. Incidence and a method of classification. J Bone Joint Surg Am 1973; 55: 1629–32. [PubMed] [Google Scholar]
- 7.Hug KT, Alton TB, Gee AO. Classifications in brief: Brooker classification of heterotopic ossification after total hip arthroplasty. Clin Orthop Relat Res 2015; 473: 2154–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Zagarella A, Impellizzeri E, Maiolino R, Attolini R, Castoldi MC. Pelvic heterotopic ossification: when CT comes to the aid of MR imaging. Insights Imaging 2013; 4: 595–603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bressler EL, Marn CS, Gore RM, Hendrix RW. Evaluation of ectopic bone by CT. AJR Am J Roentgenol 1987; 148: 931–5. [DOI] [PubMed] [Google Scholar]
- 10.Amendola MA, Glazer GM, Agha FP, Francis IR, Weatherbee L, Martel W. Myositis ossificans circumscripta: computed tomographic diagnosis. Radiology 1983; 149: 775–9. [DOI] [PubMed] [Google Scholar]