

Abstract
Objective
To describe the National Violent Death Reporting System (NVDRS). This is a surveillance system for monitoring the occurrence of homicides, suicides, unintentional firearm deaths, deaths of undetermined intent, and deaths from legal intervention (excluding legal executions) in the US.
Design
This report provides information about the history, scope, data variables, processes, utility, limitations, and future directions of the NVDRS.
Results
The NVDRS currently operates in 32 states, with the goal of future expansion to all 50 states, the District of Columbia, and US territories. The system uses existing primary data sources (death certificates, coroner/ medical examiner reports, and law enforcement reports), and links them together to provide a comprehensive picture of the circumstances surrounding violent deaths.
Conclusions
This report provides an overview of the NVDRS including a description of the system, discussion of its expanded capability, the use of new technologies as the system has evolved, how the data are being used for violence prevention efforts, and future directions.
INTRODUCTION AND RATIONALE FOR THE NATIONAL VIOLENT DEATH REPORTING SYSTEM
Violence is a major public health problem. The WHO reported that internationally in 2012 there were an estimated 475 000 homicide deaths1 and an estimated 804 000 suicide deaths.2 In 2013, >57 000 persons died violently in the USA; homicides accounted for 16 121 deaths3 and suicides accounted for 41 149 deaths.4 Suicide and homicide were the number 2 and 3 causes of death, respectively, among persons aged 15–34 in 2013.5 Each year, millions of people experience the physical, mental and economic consequences of violence.6 In the USA, violence-related death and injuries cost $107 billion a year in medical care and lost productivity.7
However, violence is preventable. Information regarding the circumstances surrounding violent deaths is needed to inform prevention programmes. There is currently no nationally representative surveillance system for violent deaths in the USA. Comprehensive surveillance data to monitor violent deaths are needed to help describe and characterise such incidents, describe associated risk factors and circumstances, and to provide information for prevention at the local, state and national levels.
HISTORY OF THE NATIONAL VIOLENT DEATH REPORTING SYSTEM
The establishment of the National Violent Death Reporting System (NVDRS) was a culmination of events and discussions regarding violence prevention that have taken place over the past several decades.8 In 1979, the US Surgeon General’s Report, Healthy People, identified violence and stress as priority areas for public health.9 In 1980, a Department of Health and Human Services Report, Promoting Health/Preventing Disease: Objectives for the Nation, established goals for violence prevention.10 Violence prevention efforts continued throughout the 1980s, and in 1985, the Surgeon General’s Workshop on Violence and Public Health focused the attention of the public health community on violence, encouraged all health professionals to become involved and called for better approaches to violence prevention, including improved reporting and data gathering.11 In 1990, ‘Violent and Abusive Behavior’ was included as one of 22 public health priority areas in Healthy People 2000.12
In 1999, in response to an Institute of Medicine report outlining the need for a national fatal intentional injury system13 a pilot programme called the National Violent Injury Statistics System (NVISS) was created. In 2000, the NVISS system was piloted at 12 sites (mostly universities) and was modelled after the National Highway Traffic Safety Administration’s Fatality Analysis Reporting System. Later that year, a meeting took place between Harvard University and the Joyce Foundation, and it was suggested that the CDC direct a publicly funded system.
In 2002, as a result of the pilot work, the NVDRS was developed to monitor the occurrence of violent deaths and provide information for the design, planning and evaluation of violence prevention programmes, and received its first appropriation from Congress. In 2003, six states (Maryland, Massachusetts, New Jersey, Oregon, South Carolina and Virginia) initiated NVDRS data collection. Two additional appropriations in 2003 and 2004 allowed 11 additional states to be funded (Alaska, California (only from 2005 to 2008 in six counties), Colorado, Georgia, Kentucky, New Mexico, North Carolina, Oklahoma, Rhode Island, Utah and Wisconsin) bringing the total to 17 states, and in 2010, 2 additional states (Michigan and Ohio) were funded. In 2014, Congress appropriated $7.5 million in funding and 14 additional states joined the NVDRS system (Arizona, Connecticut, Hawaii, Iowa, Illinois, Indiana, Kansas, Minnesota, Maine, New Hampshire, New York, Pennsylvania, Vermont and Washington) bringing the total to 32 states. The most recent expansion in 2014 is the largest in the history of the NVDRS. The 32 currently participating states (figure 1) account for 60.6% of the 2014 population and 55% of violent deaths in the USA. State health departments or their bona fide agents manage the state violent death reporting systems and serve as the point of contact to collect information from the major data sources. The programmatic goal of the system is to collect timely, integrated and comprehensive information on violent deaths and to disseminate the information to stakeholders who work on violence prevention efforts.
Figure 1.
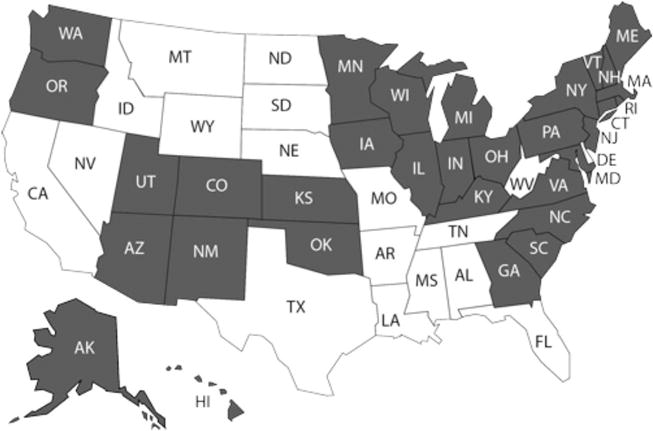
States participating in the National Violent Death Reporting System as of August 2015.
NVDRS DESIGN AND SCOPE
The conceptual definition of a violent death is “a death resulting either from the intentional use of physical force or power against oneself, another person, or a group or community”.14 The operational case definition for NVDRS is as follows: homicides, suicides, unintentional firearm deaths, deaths of undetermined intent, deaths due to legal intervention (excluding executions) and deaths due to terrorism (excluding acts of war). NVDRS cases are identified using the International Classification of Diseases, Tenth Revision (ICD-10) codes, or by using the manner of death assigned by the coroner, medical examiner or law enforcement.15 The corresponding ICD-10 codes used for the system are listed in table 1.
Table 1.
International Classification of Diseases, Tenth Revision, codes used in the National Violent Death Reporting System
| Manner of death | Death ≤1 year after injury | Death >1 year after injury |
|---|---|---|
| Intentional self-harm (suicide) | X60–X84 | Y87.0 |
| Assault (homicide) | X85–X99, Y00–Y09 | Y87.1 |
| Event of undetermined intent | Y10–Y34 | Y87.2, Y89.9 |
| Unintentional exposure to inanimate mechanical forces (firearms) | W32–W34 | Y86 determined to be attributable to firearms |
| Legal intervention (excluding executions, Y35.5) | Y35.0–Y35.4, Y35.6–Y35.7 | Y89.0 |
| Terrorism | U01, U03 | U02 |
Adapted from http://www.who.int/classifications/icd/en/
Prior to the inception of NVDRS, information on violent deaths was fragmented across a variety of data sources and was not collected in a standardised manner. One unique aspect of the NVDRS is that the system uses existing, unlinked data sources and makes better use of data that are already being collected by integrating (ie, linking) the data from these sources.16 The primary data sources used for the system are death certificates, coroner/medical examiner reports (including toxicology reports) and law enforcement reports. NVDRS is the only system of its kind that links this information together to create a comprehensive, detailed picture of the circumstances surrounding violent deaths. Coroner/medical examiner reports and law enforcement reports contain narratives that can provide detailed information regarding the circumstances and characteristics of incidents.
The system is incident-based, collects information on victims (deceased persons) and alleged perpetrators (deceased or live suspects), and has the capability to link events such as multiple homicides and homicide–suicide events together into one incident record.17 An incident can be defined as a single violent death, or multiple violent deaths if the deaths are related and the fatal injuries were inflicted <24 h apart.
The system has the capability to collect >600 variables for each death depending upon the content of the source documents and the various incident scenarios (See supplementary material – table 2). Information collected includes demographics (for victims and suspects), manner of death, ICD-10 codes, method of injury (eg, sharp instrument), place of injury, information on the victim’s life stressors, the victim–suspect relationship (eg, spouse or partner), the presence of intimate partner violence (IPV), toxicology (for victims), weapon information and whether other crimes occurred that are related to the incident (eg, robbery followed by homicide). Trained abstractors input information into the web-based NVDRS. In some cases, because the same variables are abstracted from multiple source documents, inconsistencies in information may exist across documents. Because of this, the system has primacy rules to resolve data inconsistencies.17 Primacy is established based upon assumed reliability of the sources and the primacy rule is death certificate, coroner/medical examiner report, then the law enforcement report.15 For the manner (ie, intent) of death for each decedent in NVDRS, the abstractor takes into account information from all source documents. The abstractor assigned manner of death must agree with at least one of the data sources. Typically these documents are consistent regarding the manner of death, and the abstractor assigned manner of death corresponds to that reported in all the source documents. On rare occasions, if a discrepancy exists, the abstractor assigns a manner of death on the basis of the preponderance of evidence in the source documents.15
The NVDRS is a complex surveillance system. As part of the NVDRS quality assurance process and to ensure that data are collected in a standardised manner, guidance is provided to states in the form of a coding manual. The NVDRS coding manual is a reference document that contains information regarding data structure such as data elements, variables and response options. The manual is used by the abstractor to define and characterise incidents, provide guidance for entering data and to assist the abstractor with checking data that are entered into the system. An NVDRS Help Desk is also available and staffed by the CDC so that participating VDRS states can ask questions related to the system (eg, coding questions, general web-based system questions).
The methodology of the NVDRS has been described previously in detail,17–19 and NVDRS overviews have been published in previous Injury Prevention articles or supplements in 2004 and 2006.8,17–19 Figure 2 illustrates the typical flow of information in NVDRS. When a violent death occurs, the victim’s body is taken to the coroner or medical examiner and an autopsy is performed. The coroner or medical examiner helps to complete the death certificate, and the certificate is submitted to the state’s vital records department. When a death certificate is issued in a state participating in the VDRS, state vital statistics programmes notify the VDRS programme about a violent death that meets the NVDRS case definition.
Figure 2.
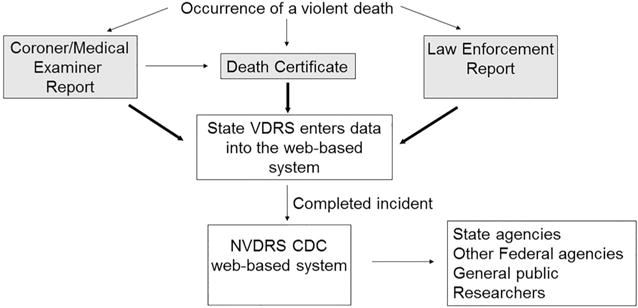
National Violent Death Reporting System information flow. Adapted with permission from BMJ Publishing Group Limited. The National Violent Death Reporting System: an exciting new tool for public surveillance. Steenkamp M, Frazier L, Lipskiy N, DeBerry M, Thomas S, Barker L, Karch D. Injury Prevention. 12(Supp 2):ii3–ii5. 2006. VDRS, Violent Death Reporting System; NVDRS, National Violent Death Reporting System; CDC, Centers for Disease Control and Prevention. Items in gray boxes denote required NVDRS data sources.
Most VDRS states initiate cases from the death certificate, although some states initiate incidents when a coroner/medical examiner report is issued and the VDRS programme is notified. The abstractor at the VDRS programme abstracts information from the death certificate (either through importing the information or entering it in manually) into the web-based system. The import function, a relatively new enhancement to the web-based system, makes it possible for the abstractor to upload death certificate information without having to enter it manually. Most victims will also have a law enforcement report generated. The VDRS programme staff then links the information from the death certificate with the coroner/medical examiner reports and the law enforcement report. Secondary (optional) data sources such as child fatality review team data, hospital data, emergency department data and information from Federal Bureau of Investigation databases (ie, homicide data from Uniform Crime Reports and the National Incident Based Reporting System) may also be used to add details about a specific incident. Data entered into the web-based system does not contain personal identifiers. Data published by the CDC are aggregated so that persons cannot be identified.
As NVDRS has evolved, several optional modules have been added in order to understand the circumstances related to specific kinds of deaths. In the first year of NVDRS, newly funded states examined the availability and utility of the data from child fatality review teams and a module was developed that was designed to collect detailed information from these teams. An optional IPV module was later added to the system for those states interested in collecting detailed information on IPV-related homicides. The IPV module allows states to capture additional detailed information on homicide incidents classified as IPV-related and is designed to collect further information on the victim, perpetrator and the circumstances (eg, relationship characteristics, history of IPV, system response) that contributed to the violent death. An incident may be determined to be IPV-related using law enforcement reports or other available information on the relationship history of the intimate partners. This definition includes cases in which there is a death of a third party that is directly linked to the intimate partner relationship (eg, the child of the intimate partner, friend of the victim, a bystander), regardless of whether the intimate partner is also killed in the incident.
Figure 3 is a Venn diagram that illustrates the scope of NVDRS. For the most part, NVDRS captures violent deaths where there was an intention to harm. Incidents captured by NVDRS are noted on the diagram. States participating in the NVDRS may decide to capture additional incidents that do not meet the case definition (eg, unintentional drug overdoses) depending upon programmatic needs, stakeholder needs, resources and interest.
Figure 3.
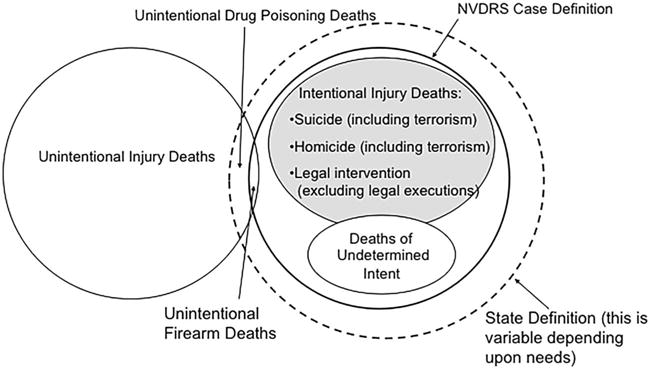
Scope of the National Violent Death Reporting System (NVDRS).
WEB-BASED NVDRS DATA COLLECTION SYSTEM
In 2013, NVDRS data collection was transitioned from a software-based system to a web-based system. The web-based system has helped to improve efficiency and help facilitate data entry. The system is accessed via an internet portal that provides secure external access for use by authorised persons only. Users (eg, trained abstractors) log in to the system to access data and to enter information about incidents. The primary system functions allow for creation of new incident records, importing of records (eg, death certificates) and searching on criteria to find specific incidents. CDC provides user guide documentation to navigate through the system and understand its functionality.
QUALITY ASSURANCE PROCEDURES
Several quality assurance procedures are in place for NVDRS, including (1) a real-time dashboard feature for monitoring performance (data metrics are presented in table and chart form), (2) automated validation checks, (3) warning messages that appear on the data entry screen if questionable values are entered, (4) re-abstraction of selected records conducted by state VDRS abstractors in order to limit variations in coding and to identify any areas for training, and (5) quality control checks that are performed at CDC. Staff at CDC check the data quality and timeliness of data submitted by VDRS states to assess performance metrics and provide feedback. CDC also reviews the coding of a subset of incidents to assess accuracy.
SYSTEM LIMITATIONS
As with any surveillance system, the NVDRS has some limitations that have been described previously.15 First, NVDRS data are not available from all states and are therefore not nationally representative. Second, the availability, completeness and timeliness of data from all three required sources (vital statistics, coroner/medical examiner report and law enforcement reports) depends upon partnerships and can be challenging for states with decentralised coroner/medical examiner systems and/or areas that have a large number of law enforcement jurisdictions. Third, for toxicology data, not all decedents are tested routinely, and results can be affected by differences in testing frequency across coroner/medical examiner offices.20 Fourth, abstractors are limited to the information they receive and data sources may not include all information about an incident, particularly in the case of homicides, which may have limited data while cases are still being adjudicated. Fifth, inconsistencies in the manner of death in source documents may pose challenges. However, NVDRS abstractors reconcile these cases using the aforementioned process described. Sixth, medical information regarding health conditions (eg, mental health status and treatment) is not often captured from medical records, and information may be limited depending upon the source of information or the knowledge of the informant (ie, family members, friends of the victims), which could affect completeness and accuracy of the information collected. Seventh, variations in coding may exist among abstractors. However, training and monitoring are provided by the CDC. Lastly, protective factors (ie, characteristics that reduce the risk of violent death) are not collected by NVDRS due to the nature of data sources, which usually only contain risk factor information.
UTILITY OF THE NVDRS
Public health surveillance is defined as the ongoing, systematic collection, analysis, interpretation and dissemination of data regarding a health-related event for use in public health action to reduce morbidity and mortality and to improve health.21–23 Findings from NVDRS data have been used to inform, develop, implement and evaluate violence prevention programmes to advance injury prevention practice. The following are some examples of how the data have been used in this regard.
Information from NVDRS has been used to inform and support homicide prevention efforts. Findings from the Oklahoma VDRS revealed that 43% of homicides among females in Oklahoma are IPV related.24 In Oklahoma, IPV data from VDRS are used to inform law enforcement when managing domestic violence incidents. Specifically, responding police officers conduct a brief 11-item lethality assessment, the Lethality Assessment Protocol (LAP), to determine whether the victim is at high risk for homicide, and if so, immediate coordination with a local collaborating domestic violence service provider occurs. If the results of the assessment indicate that the victim is at high risk, immediate coordination with the local domestic violence service provider occurs. To evaluate the effectiveness of the LAP, the Oklahoma NVDRS secured a grant from the National Institute of Justice to implement and evaluate a new strategy for responding to domestic violence calls. As a result, the Oklahoma Lethality Assessment study, a quasi-experimental field study, was conducted in seven sites from 2009 to 2013. It was hypothesised that the LAP would increase safety behaviours and decrease the severity and frequency of violence. Results are promising in that no homicides occurred during the study period, women’s violent victimizations were decreased and immediate protective actions were increased.25
Data from the Utah Violent Death Reporting System revealed that in domestic violence-related homicides 147 children <18 years of age were directly exposed to the homicide (eg, witnessed the homicide, were attacked during the homicide, heard the homicide, discovered the body), and of these children, 78.2% were 5 years old or younger.26 As a result of these findings, the Utah Department of Health’s Violence and Injury Prevention Program (VIPP) and Domestic Violence Fatality Review Committee (DVFRC) were used to help inform a policy change regarding services for children of domestic violence-related homicide victims.27 VIPP and DVFRC worked with the state Department of Children and Family Services (DCFS) on the process of providing immediate referrals to DCFS. The referrals enable children and families of domestic violence-related homicides to receive an assessment and get linked to intervention and follow-up services (eg, mental health services) to help cope with the post-traumatic sequelae of homicide and domestic violence issues.27
Information from NVDRS can also be used to inform suicide prevention efforts.
North Carolina Violent Death Reporting System data were used to inform the development of the 2015 North Carolina Suicide Prevention Plan. Stakeholders from across the state were involved in the development of the plan, and the data were used to inform stakeholders about statewide trends in suicide rates, populations at increased risk for suicide and the circumstances surrounding suicide deaths.28 The plan was completed, disseminated to partners and posted to the North Carolina Department of Health’s Injury and Violence Prevention Branch website. In addition to the plan, a PowerPoint presentation with the data has been posted to the Injury and Violence Prevention Branch website so that stakeholders can easily download it for use in presentations and reports.
VDRS data have also been used to study the circumstances surrounding suicides among veterans and active duty personnel to help develop and implement suicide prevention programmes.29–31 Several VDRS states are working with the Veterans Administration offices in their respective states to use the data for prevention in an effort to reduce suicides among this population.
FUTURE DIRECTIONS
Epidemiologic, statistical and informatics methods must continue to evolve for application to public health surveillance practice.32 The NVDRS system has evolved, is flexible and is able to adapt to changing needs. Improving the completeness and accuracy of data on important topics continues to be a priority for the NVDRS. For example, variables were recently added and modified to better capture sexual orientation (lesbian, gay, bisexual) and relationship status (eg, same-sex or opposite-sex relationships) to improve the accuracy of information that is collected on these topics. In response to state interest, the web-based system was also recently modified to enable states to voluntarily collect information on unintentional drug poisonings (including prescription drug overdoses) in order to understand the magnitude of the problem in their jurisdiction.
Following the 2014 expansion of NVDRS, new abstractor training methods have been explored to provide support for new state VDRS staff. In 2015, an interactive, electronic learning (e-learning) module was developed so that VDRS abstractors can receive training for the web-based data collection system remotely and on demand. This e-learning module supplements the current NVDRS coding manual. The module will likely decrease the time it takes a new abstractor to learn the web-based system, increase abstractor speed and accuracy in coding narrative data on the circumstances of a violent death, enhance efficiency by teaching the abstractor about key tips and shortcuts, and increase the consistency of coding across VDRS states.
Efforts have also been made to make NVDRS data more accessible to stakeholders. In 2007, the NVDRS Restricted Access Database (RAD) was created for researchers to request access to case-level microdata. The RAD includes detailed information from NVDRS such as the coroner/medical examiner and law enforcement narratives and is available to investigators who are part of research organisations, government agencies or institutions of higher education. RAD requests do not contain the complete NVDRS data set, but are customised in such a way that they only include the variables requested by the investigator. In 2008, NVDRS data were added to CDC’s Web-based Injury Statistics Query and Reporting System (WISQARS), allowing users such as researchers, the media, public health professionals and the general public to initiate web-based queries. WISQARS is an online database that provides fatal and non-fatal injury, violent death and cost of injury data from CDC. The WISQARS data are updated annually and are available at http://www.cdc.gov/injury/wisqars/nvdrs.html.
In 2015, the CDC held its first NVDRS Surveillance Academy to help current and potential data users understand how to access, analyse, interpret and report NVDRS data and to use the data to inform and enhance ongoing violence prevention initiatives. This provided participants with an opportunity to learn about NVDRS and how it fits within the larger context of injury surveillance.
Other goals for the future include enhancing stakeholder engagement to demonstrate the value of the system and better illustrate how data are helping with prevention and to respond to violence prevention concerns.
CONCLUSION
The system will continue to provide useful, actionable data. While the information obtained through NVDRS data collection has been critical to understanding the circumstances surrounding violent deaths in participating states, the ultimate goal is for the system to be expanded to all 50 states, the District of Columbia and US territories to help reach the goal of nationally representative data. It is also hoped that the NVDRS can serve as a model for other countries who choose to develop such a system to monitor the occurrence of violent deaths.
What is already known on the subject
-
▸
Ongoing surveillance is needed to monitor violent deaths and to support planning and evaluation for prevention.
-
▸
The National Violent Death Reporting System (NVDRS) is a surveillance system for monitoring the occurrence of homicides, suicides, unintentional firearm deaths, deaths of undetermined intent and deaths from legal intervention (excluding legal executions) in the USA.
-
▸
The NVDRS uses data from death certificates, coroner/ medical examiner reports and law enforcement reports to provide a complete picture of violent deaths.
-
▸
The system began in 2003 with 6 states and currently operates in 32 states, with a goal of future expansion to all 50 states, the District of Columbia and US territories.
What this study adds
-
▸
As surveillance technologies have evolved, so has the NVDRS. This report describes the evolution of the system and how it is adapting to meet stakeholder needs to advance violence prevention efforts.
-
▸
This report also provides examples of how state VDRS programmes are using the data to develop and inform violence prevention efforts.
-
▸
This report also describes future directions for the NVDRS.
Acknowledgments
A national reporting system such as the NVDRS requires the contributions of many agencies and organisations. The authors acknowledge the invaluable contributions of the participating state Violent Death Reporting Systems; participating state agencies, including state health departments, vital registrars’ offices, coroners’ and medical examiners’ offices, crime laboratories, and local and state law enforcement agencies; partner organisations, including the Safe States Alliance (formerly STIPDA), National Violence Prevention Network, National Association for Public Health Statistics and Information Systems, Council of State and Territorial Epidemiologists, and Association of State and Territorial Health Officials; federal agencies, including the Department of Justice (Bureau of Justice Statistics and the Federal Bureau of Investigation), the Department of the Treasury (Bureau of Alcohol, Tobacco, and Firearms); the International Association of Chiefs of Police; other stakeholders, researchers, and foundations, including Harvard University School of Public Health and the Joyce Foundation; and the National Institute for Occupational Safety and Health, and National Center for Health Statistics, CDC.
Footnotes
Contributors JMB and AEC: conception and design of the work, drafting the work and revising it critically for important intellectual content. KAF and SPDJ: design of the work, drafting the work and revising it critically for important intellectual content. All authors are accountable for all aspects of the work and have given their approval of the manuscript as part of the CDC scientific clearance process.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Disclaimer The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
References
- 1.World Health Organization. Global status report on violence prevention 2014. Geneva: World Health Organization; 2014. [Google Scholar]
- 2.World Health Organization. Preventing suicide: a global imperative. Geneva: World Health Organization; 2014. [Google Scholar]
- 3.Centers for Disease Control and Prevention. National Center for Health Statistics. http://www.cdc.gov/nchs/fastats/homicide.htm (accessed Aug 2015)
- 4.Centers for Disease Control and Prevention. National Center for Health Statistics. http://www.cdc.gov/nchs/fastats/suicide.htm (accessed Aug 2015)
- 5.Centers for Disease Control and Prevention (CDC) Web-based Injury Statistics Query and Reporting System (WISQARS) [Online] National Center for Injury Prevention and Control (CDC); 2013. (producer). http://www.cdc.gov/injury/wisqars/index.html. [Google Scholar]
- 6.Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Understanding and Preventing Violence: Summary of Research Activities. http://www.cdc.gov/violenceprevention/pdf/dvp-research-summary-a.pdf (accessed Aug 2015)
- 7.Centers for Disease Control and Prevention. Fact Sheet. http://www.cdc.gov/violenceprevention/pdf/nvdrs_factsheet-a.pdf (accessed Aug 2015)
- 8.Weiss HB, Gutierrez MI, Harrison J, et al. The US National Violent Death Reporting System: domestic and international lessons for violence injury surveillance. Inj Prev. 2006;12(Suppl 2):ii58–62. doi: 10.1136/ip.2006.013961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.US Department of Health, Education, and Welfare. Healthy people: the surgeon general’s report on health promotion and disease prevention. Washington DC: US Government Printing Office; 1979. [Google Scholar]
- 10.US Department of Health & Human Services. Promoting health/preventing disease; objectives for the nation. Washington DC: US Government Printing Office; 1980. [Google Scholar]
- 11.Cron T. The Surgeon General’s Workshop on violence and public health: review of the recommendations. Public Health Reports. 1986;101:8–14. [PMC free article] [PubMed] [Google Scholar]
- 12.Healthy People 2000 Priority Areas. http://www.cdc.gov/nchs/healthy_people/hp2000/hp2000_priority_areas.htm (accessed Aug 2015)
- 13.Bonnie RJ, Fulco CE, Liverman CT, editors. Reducing the burden of injury: advancing prevention and treatment. Washington DC: National Academies Press; 1999. Institute of Medicine. http://www.nap.edu/openbook.php?record_id=6321 (accessed Aug 2015) [PubMed] [Google Scholar]
- 14.Krug EG, et al., editors. World report on violence and health. Geneva: World Health Organization; 2002. [Google Scholar]
- 15.Parks SE, Johnson LL, McDaniel DD, et al. Centers for Disease Control and Prevention Surveillance for Violent Deaths—National Violent Death Reporting System, 16 States, 2010. MMWR Surveill Summ. 2014;63:1–33. [PubMed] [Google Scholar]
- 16.Azrael D, Barber C, Mercy J. Linking data to save lives: recent progress in establishing a National Death Reporting System. Harv Health Policy Rev. 2001;2:38–42. [Google Scholar]
- 17.Steenkamp M, Frazier L, Lipskiy N, et al. The National Violent Death Reporting System: an exciting new tool for public health surveillance. Inj Prev. 2006;12(Suppl 2):ii3–5. doi: 10.1136/ip.2006.012518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Paulozzi LJ, Mercy J, Frazier L, Jr, et al. CDC’s National Violent Death Reporting System: background and methodology. Inj Prev. 2004;10:47–52. doi: 10.1136/ip.2003.003434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mercy JA, Barker L, Frazier L. The secrets of the National Violent Death Reporting System. Inj Prev. 2006;12(Suppl 2):ii1–2. doi: 10.1136/ip.2006.012518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Karch D, Crosby A, Simon T, Centers for disease control and prevention Toxicology testing and results for suicide victims—13 states, 2004. MMWR. 2006;55:1245–8. [PubMed] [Google Scholar]
- 21.Thacker SB. Historical development. In: Teutsch SM, Churchill RE, editors. Principles and practice of public health surveillance. 2nd. New York, NY: Oxford University Press; 2000. [Google Scholar]
- 22.Buehler JW. Surveillance. In: Rothman KJ, Greenland S, editors. Modern epidemiology. 2nd. Philadelphia, PA: Lippincott-Raven; 1998. [Google Scholar]
- 23.Teutsch SM, Thacker SB. Planning a public health surveillance system. Epidemiol Bull. 1995;16:1–6. [PubMed] [Google Scholar]
- 24.Oklahoma State Department of Health, Injury Prevention Service. Violent Deaths in Oklahoma. Oklahoma Violent Death Reporting System, 2004–2010. 2014 Mar; http://www.ok.gov/health2/documents/OKVDRS_Violent_Deaths_2004-2010.pdf (accessed Aug 2015)
- 25.Brown S, Sullivan Wilson JS, Messing JT, et al. Translating research to practice to prevent intimate partner violence. Presented at the Safe States Annual Meeting. 2015 Apr; https://c.ymcdn.com/sites/safestates.site-ym.com/resource/resmgr/2015_AM_Presentations/Brown_4.30.15_0145PM.pdf (accessed Aug 2015)
- 26.Violence and Injury Prevention Program. Domestic Violence Fatalities in Utah 2003–2008. Salt Lake City, UT: Utah Department of Health; 2010. http://health.utah.gov/vipp/pdf/DomesticViolence/2003-2008%20Report.pdf (accessed Aug 2015) [Google Scholar]
- 27.NVDRS. Stories from the Frontlines of Violent Death Surveillance 2013. Atlanta, GA: Safe States Alliance; http://c.ymcdn.com/sites/www.safestates.org/resource/resmgr/NVDRS/NVDRS_Stories_complete_repor.pdf (accessed Aug 2015) [Google Scholar]
- 28.North Carolina Suicide Prevention Plan. 2015 http://www.injuryfreenc.ncdhhs.gov/preventionResources/docs/2015-NC-SuicidePreventionPlan-2015-0505-FINAL.pdf (accessed Aug 2015)
- 29.Oklahoma State Department of Health, Injury Prevention Service. Suicide among Veterans in Oklahoma. 2005–2012 http://www.ok.gov/health2/documents/OKVDRS_Brief_Suicide_Among%20Veterans.pdf (accessed Aug 2015)
- 30.Virginia Department of Health, Office of the Chief Medical Examiner. Military-Related Suicide in Virginia: A Report from the Virginia Violent Death Reporting System. 2003–2010 http://www.vdh.virginia.gov/medExam/documents/2012/pdf/Veterans%20and%20Suicide%20in%20Virginia_final.pdf (accessed August 2015)
- 31.Oregon Violent Death Reporting System, Oregon Health Authority, Public Health Division. Suicide Among Oregon Veterans. 2008–2012 http://public.health.oregon.gov/DiseasesConditions/InjuryFatalityData/Documents/NVDRS/suicide-among-oregon-veterans2008through2012.pdf (accessed Aug 2015)
- 32.Thacker SB. Historical development. In: Lee LM, Teutsch SM, Thacker SB, et al., editors. Principles and practice of public health surveillance. Oxford University Press; 2010. p. 14. [Google Scholar]