

ABSTRACT
Grounded in Emotional Cascade Theory, we explored whether rumination and multisensory imagery-based cognitions moderated the relationships between affect and both odds of non-suicidal self-injury (NSSI), and frequency of the behaviour. A sample of 393 university students completed self-report questionnaires assessing the constructs of interest. Contrary to expectations, rumination did not emerge as a significant moderator of the affect-NSSI relationship. However, the relationship between affect and frequency of NSSI was moderated by the use of imagery. Further, the relationship between negative affect and NSSI was moderated by positive affect, underscoring the need to consider both negative and positive affect in models of NSSI. Most youth who self-injured reported thinking in images while the urge to self-injure was strong, with 53% thinking in images at least half the time. Future work is needed to explore how positive and negative affect work in concert to govern NSSI, and how imagery might either exacerbate or reduce risk of NSSI.
KEYWORDS: NSSI, affect, rumination, imagery
Non-suicidal self-injury (NSSI), the deliberate destruction or alteration of body tissue, that is not socially sanctioned and is performed without conscious suicidal intent (Nock, 2009), is commonly engaged by adolescents and young adults to relieve intense emotional states (Bentley, Nock, & Barlow, 2014). Although forms of NSSI vary, common methods include skin cutting, burning and self-battery. Of concern, while NSSI is delineated from suicidal behaviour by definition, it is associated with significant psychological morbidity and later suicidal thoughts and behaviours (Whitlock et al., 2013). With approximately 13% of young adults, and up to 20% of university students reporting a history of NSSI (Swannell, Martin, Page, Hasking, & St John, 2014), concerted efforts are being made to better understand potential risk factors (e.g. Fox et al., 2015), with a view to informing effective prevention and early intervention initiatives. In this study we draw on Emotional Cascade Theory (Selby & Joiner, 2009) to propose that rumination moderates the relationship between both negative and positive affect and NSSI. Further, we consider both verbal cognitions (i.e. rumination), and multisensory imagery (i.e. visual pictures and associated auditory, gustatory, olfactory, and tactile senses), in moderating these relationships.
Emotional cascade theory
One of the more widely accepted theories of NSSI, Emotional Cascade Theory (Selby & Joiner, 2009), proposes that ruminating on even minute emotional stimuli can exacerbate the experience of negative emotion. Rumination involves repeatedly allocating attention to the negative stimuli, sustaining focus on, and fostering a re-experiencing of, the negative emotional impact. Continued rumination then results in a vicious cycle, or emotional cascade, that becomes increasingly distressing, as the negative emotion is amplified. Given the intensity of the emotion, distraction techniques like going for walk are not effective in interrupting the cascade. Rather, a more extreme form of distraction, such as NSSI, can be used to break this cycle, by directing attention away from the negative stimuli toward the sight of blood, the experience of pain, or the need to medically attend to the injury. The subsequent reduction in arousal and intense emotion negatively reinforces the behaviour, and over time, NSSI becomes a conditioned response to negative emotional stimuli or intense negative affect (Selby & Joiner, 2009). While other behaviours, such as drug use, might also serve this function, it seems NSSI is particularly effective in interrupting the emotional cascade, at least in the short term. The failure of NSSI to impact long term changes in rumination, coupled with the immediately reinforcing effect, may explain why NSSI is engaged repetitively to reduce intense emotion.
Both self-report and experimental work support Emotional Cascade Theory, with rumination distinguishing between people who self-injure and those who do not, and exacerbating the relationship between negative affect and NSSI (Arbuthnott, Lewis, & Bailey, 2015; Bresin & Verona, 2016; Nicolai, Wielgus, & Mezulis, 2016; Selby, Franklin, Carson-Wong, & Rizvi, 2013). While much of the work has explored negative affect in general, Emotion Cascade Theory proposes that the intensity of affect is key to the behaviour used as distraction. As such, efforts to determine whether rumination moderates the relationship between affect intensity, and psychological distress which may emerge from negative affect, are warranted.
While dysregulation of negative emotional experiences is clearly related to NSSI, individuals must also effectively regulate positive affect if an optimal emotional state is to be maintained. Whether positive and negative affect are polar opposites of a single affect dimension (i.e. valance), or whether they are orthogonal, independent dimensions has long been debated (e.g. Russell & Carroll, 1999; Watson, Clark, & Tellegen, 1988; Watson & Tellegen, 1999; Yik, 2007). While some argue that a bipolar model best explains the data (Russell & Carroll, 1999; Yik, 2007), others maintain that positive and negative affect are weakly correlated, and largely independent dimensions (Watson et al., 1988; Watson & Tellegen, 1999). Given that some affective terms are polar opposites (e.g. happy vs sad) while other positively and negatively valanced terms are not (e.g. enthusiastic vs angry), item selection strongly influences whether the dimensions are best conceptualised as bipolar or separable (Russell & Carroll, 1999). Given most studies in this field employ the PANAS (Watson et al., 1988) to assess emotion, which contains separate, but correlated, positive and negative affect scales, the potential for positive and negative affect to play different roles in NSSI can be investigated.
Adopting this independent view, it seems reasonable that a combination of decreased positive affect, and elevated negative affect may precede NSSI (Selby & Joiner, 2009). Yet, so far, tests of Emotional Cascade Theory have typically focused on the relationship between rumination and negative affect. Daily diary studies indicate that people who self-injure report less positive emotion than people who do not (Bresin, 2014; Victor & Klonsky, 2014). That some people report an increase in positive affect after NSSI, and that this is predictive of more severe NSSI, suggests that a lack of positive affect may be implicated in NSSI (Claes, Klonsky, Muehlenkamp, Kuppens, & Vandereycken, 2010; Jenkins & Schmitz, 2012; Nock & Prinstein, 2004). In this case people may self-injure in order to generate positive emotion (i.e. positive reinforcement), rather than reduce negative emotion (i.e. negative reinforcement, Nock & Prinstein, 2004). In early work Gratz, Rosenthal, Tull, Lejuez, and Gunderson (2006) noted that low positive emotion intensity reliably distinguished participants with a history of frequent NSSI from those with no history of NSSI. Using ecological momentary assessment. Muehlenkamp et al. (2009) also noted that positive affect decreased in the lead up to NSSI, and increased after NSSI in patients with bulimia nervosa. Recently, Cohen et al. (2015) noted that positive affect, and not negative affect, moderated the relationship between rumination and frequency of NSSI in adolescents, such that the relationship was only evident at low levels of positive affect. Together, these studies suggest that it is not just the intensity of the emotional experience that is related to NSSI, but that consideration of the emotional valence is also warranted.
Imagery and NSSI
The prominent role of rumination in Emotional Cascade Theory highlights the importance of cognitions in regulating emotional states. Recognising that Beck (1976) articulated a role for both verbal (i.e. thoughts) and imagery-based cognitive modes in experiences of emotional distress, researchers have recently explored the role of imagery in emotional experience. Rumination is typically conceptualised as a verbal-linguistic cognitive mode akin to self-talk, whereas mental imagery incorporates multi-sensory perceptual representations including auditory, visual, gustatory, tactile, and/or olfactory elements (Hackmann, Bennett-Levy, & Holmes, 2011; Holmes & Mathews, 2010). There is evidence that verbal-linguistic rumination suppresses mental imagery, which is more physiologically and affectively activating, thereby negatively reinforcing and maintaining verbal-linguistic thinking (Borkovec, Alcaine, & Behar, 2004). Within the context of NSSI, this theory suggests that individuals may engage in rumination as a strategy for avoiding more vivid and activating mental images of the stressor and feared aversive consequences. Evidence that multisensory imagery is more emotionally evocative and has stronger links to affect than verbal thoughts (e.g. Holmes & Mathews, 2010), has led to the development of efficacious imagery-enhanced cognitive–behavioural treatments for emotional disorders that aim to circumvent avoidance of multi-sensory imagery and thereby reduce rumination and facilitate emotional processing (Holmes et al., 2016; McEvoy & Saulsman, 2014; McEvoy, Erceg-Hurn, Saulsman, & Thibodeau, 2015). Arguably then, a tendency to think in images may result in even stronger emotional cascades than rumination, increasing risk of NSSI as a means of breaking this cycle.
That self-injury itself is such a multisensory expression of distress (i.e. visual images of past, current, and future injuries and associated somatic sensations), which can be exacerbated by visible scarring (Lewis & Mehrabkhani, 2016), suggests imagery may be particularly relevant to cascades of emotion that lead to NSSI. Recent evidence suggests a role for imagery in both the onset and prevention of self-injury: the desire to see blood is associated with more severe self-injury and associated psychopathology (Glenn & Klonsky, 2010), while decreases in negative emotionality are noted when participants imagine the moments after self-injury (Welch, Linehan, Sylvers, & Chittams, 2008). Recently, Cloos et al. (2016) examined the relationship between dysregulated behaviours (including NSSI), and negative mental images, which naturally occurred over the study period (2 weeks), in a mixed clinical and community-based sample. They observed both prevalence and vividness of negative imagery are higher among people reporting dysregulated behaviours, however how a general tendency to use imagery is related to NSSI remains to be seen.
Similarly, little is known about how the content of imagery might either exacerbate or reduce the risk of NSSI. As noted above, the sight of blood is related to the severity of NSSI (Glenn & Klonsky, 2010), but images of distressed family and friends might discourage someone from acting on the urge to self-injure (McEvoy, Hayes, Hasking, & Rees, 2017). Images displayed in popular media and online can be both triggering and comforting to individuals who self-injure. Positive aspects of photographs posted online include reducing a sense of loneliness, communicating shared experiences, and offering help to others (Baker & Lewis, 2013; Sternudd, 2012). Conversely, NSSI imagery displayed online can trigger urges to self-injure (Baker & Lewis, 2013; Lewis & Baker, 2011; Lewis, Heath, Michal, & Duggan, 2012). Yet, these external representations of NSSI cannot be compared to images that are generated internally. An exploration of how specific mental images are related to NSSI might offer useful insights into the cognitive patterns that precipitate NSSI.
The current study
In this study we aimed to expand Emotional Cascade Theory to explore whether the relationships between affective experience (positive and negative), general psychological distress and affect intensity, and history of NSSI are moderated by repetitive negative thinking (i.e. rumination), use of imagery in daily life, and general ability to produce vivid images. Further, we explored whether these relationships were related to frequency of NSSI among youth who do self-injure. Based on Emotional Cascade Theory we expected a positive relationship between negative affect intensity, psychological distress and both odds of NSSI, and frequency of the behaviour. Given emerging work suggesting a lack of positive affect is implicated in NSSI, we expect a negative relationship between positive affect and NSSI. We expected these relationships would be strengthened by repetitive negative thinking, use of imagery and vividness of imagery in daily life. Adopting an independent view of positive and negative affect, we were also interested in how these factors worked together, and thus explored the interaction between positive and negative affect in predicting NSSI. Finally, we explore the content of images that arise when participants experience the urge to self-injure.
Method
Participants
Sample size was not pre-determined; we allowed all interested students to enroll in the study over a two semester period. The sample comprised 393 (76% female) undergraduate students, aged between 17 and 30 years, (M = 20.01, SD = 2.58); 129 (33%) reported a history of self-injury. Of these, 18% (n = 22) self-injured five or more times in the last year. Cutting was reported as the primary form of self-injury by 44% (n = 54), followed by severe scratching (15.6%) and self-battery (10.7%). Age of onset ranged from 6 to 21 years (M = 14.34, SD = 2.41). History of NSSI was not related to gender, χ2(1) = 3.28, p = .07, or age, t(404) = .11, p = .91. After removing four outliers (e.g. 10,000 episodes of biting), average frequency of NSSI in the last year, across all methods, was 7.52 episodes of NSSI (range .08–79.58, SD = 15.97).
Materials
As part of a larger study participants completed the following self-report measures (complete list of measures in Sup 1).
Inventory of Statements about Self-Injury (ISAS; Klonsky & Olino, 2008). Section I of the ISAS was used to assess the nature and extent of NSSI, including primary method of NSSI and frequency of NSSI over the last 12 months. The ISAS has established test-retest reliability (r = .85; Klonsky & Olino, 2008) in samples of young adults.
Positive and Negative Affect Schedule (PANAS; Watson et al., 1988). The PANAS was developed to assess two independent dimensions of positive and negative affect. The PANAS presents participants with 20 emotions (10 positive, 10 negative) and asks them to rate the extent to which they have experienced each emotion over the past week. This widely used measure of positive and negative affect reliably measures the two constructs, and demonstrates invariance across demographic groups (Crawford & Henry, 2004). In this sample, internal consistency was sound for both positive (α = .96) and negative (α = .92) affect.
K10 (Kessler et al., 2002). The K10 asks participants to respond to 10 items that reflect symptoms of anxiety and depression. The K10 is routinely used as a screening tool in clinical settings and is designed to give a global assessment of distress. In the current sample α = .90.
Short Affect Intensity Measure (AIM; Larsen, 1984). Adapted from the 40-item measure (Larsen & Diener, 1987), the shortened AIM contains 20 items that assess how strongly people feel emotions, on a 6-point scale. Test-retest reliability of the unidimensional scale is excellent and the AIM correlates well with parent and peer report (Larsen & Diener, 1987). In the current study Cronbach’s alpha = .77.
The Repetitive Thinking Questionnaire (RTQ; McEvoy, Mahoney, & Moulds, 2010; McEvoy, Thibodeau, & Asmundson, 2014).The RTQ was designed to assess the transdiagnostic symptom of repetitive negative thinking (i.e. rumination) that frequently underlies a range of diagnoses including depression and anxiety. In the current study we utilised a brief 10 item version of the questionnaire. Participants responded to items assessing their tendency to think negatively when feeling distressed (e.g. I think about the situation all the time), on a 5-point Likert scale. The RTQ has demonstrated reliability and validity (McEvoy et al., 2010, 2014). Internal consistency was evident in the current sample, α = .85.
Spontaneous Use of Imagery Scale (SUIS; Reisberg, Pearson, & Kosslyn, 2003). The 12 item SUIS assesses spontaneous use of imagery in daily life (e.g. When I think about visiting a relative, I almost always have a clear mental picture of him or her). Participants rate how appropriate each statement is for them on a 5-point Likert scale. Psychometric testing indicates reliability and validity of the measure when administered to university students (Nelis, Holmes, Griffith, & Raes, 2014). In this sample Cronbach’s alpha = .96.
Vividness of Visual Imagery Questionnaire-2 (VVIQ-2; Marks, 1995).The VVIQ-2 assesses how vividly people can imagine four different scenarios by responding to four prompts and rating vividness of the image on a 5 point scale. In this study only one scenario, with four prompts, was presented (watching a sun rise). The four prompts were internally consistent in this data (α = .91).
Content of NSSI-related images. Participants who self-injured were asked how often they found themselves thinking in images (mental pictures, sound images, images of sensations, tastes or smells) when they had a strong urge to self-injure (rated on a 7 point scale, 1 = not at all to 7 = all the time). Participants then provided a written description to exemplify the kind of images associated with NSSI urges.
Procedure
Participants responded to an online advertisement for undergraduate psychology students interested in participating in research for course credit. Interested students were directed to the online survey, where they were provided with an information sheet that outlined the study aims, participation requirements, voluntary nature of participation, confidentiality of data, and details of data storage. Participants completed the survey at a time and place of their choosing, and took approximately 30 min to complete all questions. At both the beginning, and at the end of the survey, all participants were provided with information about local mental health services, confidential counselling hotlines/websites and tips for reducing stress. We report how we determined our sample size, all data exclusions (if any), all manipulations and all measures in the study.
Data analysis
On average 3.34% of data were missing across the continuous variables, and were missing completely at random, Little’s MCAR χ2 (35) = 27.07, p = .83. Listwise deletion was used as the default means of dealing with missing data. After exploring descriptive statistics, and frequency of NSSI imagery, hierarchical logistic regression tested the relationship between the key variables and odds of engaging in NSSI; hierarchical linear regression tested the relationship with frequency of NSSI among participants who self-injured. Given age and gender were not related to the outcomes (both p > .05), these were not statistically controlled in analyses. All affect variables (positive affect, negative affect, psychological distress, affect intensity) were entered in Step 1, while repetitive thinking and the two imagery variables (use of imagery, vividness of imagery) were entered in Step 2. Interactions between all affect variables, rumination and imagery, the interaction between positive and negative affect, and the interactions between rumination and imagery, were entered in the final step. All predictors were standardised to reduce multicollinearity, and simple slopes interpreted at ± one standard deviation (Aiken & West, 1991).
To explore the content of imagery related to NSSI, written responses provided by participants were reviewed for emerging themes. One author conducted the initial thematic analysis; another checked the extracted themes and associated participants’ statements for accuracy. Acceptable inter-rater reliability was observed (exact agreement = 73.75% of statements; weighted κ = .69). Discrepancies were noted most often where insufficient information was provided to allow accurate categorisation (e.g. categorising “death” or “being alone” as either negative emotionality or escape).
Results
As seen in Table 1, the majority of variables were correlated in the expected direction, however neither history of NSSI or frequency of NSSI were associated with general use of imagery. Among people who self-injure, frequency of NSSI-related images was not associated with frequency of NSSI.
Table 1. Descriptive statistics and correlations between variables of interest.
| Mean | SD | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. History of NSSI | – | – | – | – | −.28*** | .23*** | .36*** | .09 | .30*** | .06 | .07 |
| 2. Freq. of NSSIa | 7.52 | 15.97 | – | .03 | −.28* | .29* | .35** | −.18 | .14 | −.04 | −.17 |
| 3. Freq. of NSSI imagerya | 4.36 | 2.73 | – | −.04 | .19* | .22* | .07 | .23* | .38*** | .13 | |
| 4. Positive affect | 31.53 | 7.67 | – | −.21*** | −.42*** | .11* | −.26*** | .14** | .04 | ||
| 5. Negative affect | 22.90 | 7.07 | – | .66*** | .33*** | .48*** | .09 | .04 | |||
| 6. Psych. distress | 24.42 | 7.46 | – | .24*** | .58*** | .13* | .08 | ||||
| 7. Affect intensity | 68.82 | 7.28 | – | .29*** | .18** | .09 | |||||
| 8. Repetitive thinking | 33.00 | 8.56 | – | .19*** | .05 | ||||||
| 9. Use of imagery | 41.87 | 7.36 | – | .31*** | |||||||
| 10. Vividness of imagery | 17.67 | 4.07 | – |
aSub-sample who self-injure only.
*p < .05; **p < .01; ***p < .001.
Predicting odds of NSSI
In the first step, the affective variables significantly differentiated participants who self-injured and those who did not, χ2(4) = 49.86, p < .001. Specifically, positive affect was associated with decreased odds of NSSI, while psychological distress increased odds of NSSI (Table 2). The second step did not significantly improve the model, χ2step (3) = 3.58, p = .31. Finally, although the 2-way interaction terms did not significantly predict odds of NSSI as a block, χ2step (13) = 18.84, p = .13, the interaction between positive and negative affect was marginally significant (p = .06). Given that moderated regression is usually under-powered, and that we adopted an independent conceptualisation of positive and negative affect specifically to explore how they work together, we opted to interpret this interaction. However results should be interpreted with caution. Depicted graphically in Figure 1, it appears there is little relationship between negative affect and NSSI at low levels of positive affect, but a high level of positive affect was related to reduced odds of NSSI when negative affect was high. Yet, while the two slopes are different from each other, neither is significantly different from zero (both p > .05). The relationship between negative affect and NSSI was also moderated by use of imagery; use of imagery was not related to NSSI in the presence of negative affect (b = .29, z = 1.27, p = .20), but less use of imagery appears protective (b = −.61, z = 2.07, p = .03; Figure 2). The final model accounted for between 20.1% (Cox & Snell R2) and 28.8% (Nagelkerke R2) of variance in NSSI.
Table 2. Regression analyses predicting odds of self-injury (left panel) and frequency of NSSI (right panel).
| Variable | Odds of NSSI | Frequency of NSSI | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | SEB | Wald | Exp(B) | p | 95% CIa | B | SEB | β | t | p | 95% CIb | |
| Step 1 | ||||||||||||
| Positive affect | −.41 | .15 | 7.72 | .66 | .006 | .50–.89 | −1.13 | 1.18 | −.10 | .96 | .34 | −3.46–1.19 |
| Negative affect | −.004 | .17 | .001 | .99 | .98 | .72–1.38 | 1.51 | 1.25 | .14 | 1.21 | .23 | −.97–3.99 |
| Psych. distress | .64 | .19 | 11.78 | 1.89 | .001 | 1.31–2.71 | 1.80 | 1.39 | .16 | 1.30 | .20 | −.94–4.54 |
| Affect intensity | .12 | .14 | .75 | 1.13 | .39 | .86–1.48 | −2.20 | 1.07 | −.19 | 2.06 | .04 | −4.32–.08 |
| Step 2 | ||||||||||||
| Repetitive thinking | .30 | .16 | 3.67 | 1.35 | .07 | .98–1.86 | .34 | 1.17 | .03 | .29 | .77 | −1.99–2.66 |
| Use of imagery | .009 | .14 | .005 | 1.01 | .95 | .78–1.32 | −.69 | 1.12 | −.06 | .62 | .54 | −2.91–1.52 |
| Vividness of imagery | .02 | .13 | .01 | 1.02 | .91 | .78–1.32 | −1.49 | 1.10 | −.13 | 1.36 | .18 | −3.66–.67 |
| Step 3c | ||||||||||||
| PA × NA | −.34 | .18 | 3.56 | .72 | .06 | .51–1.01 | −3.57 | 1.26 | −.37 | 2.84 | .005 | −6.05–1.08 |
| NA × SUIS | .51 | .20 | 6.44 | 1.67 | .002 | 1.12–2.49 | ||||||
| Final model | χ2 = 75.81, p < .001 | R = .54, R2 = .29, p = .01 | ||||||||||
a95% confidence intervals for Exp(B).
b95% confidence intervals for B.
cFor ease of presentation only significant interactions are included in the table; statistically significant results are highlighted in bold text.
PA: positive affect; NA: negative affect; K10: psychological distress; SUIS: spontaneous use of imagery: VVIQ: vividness if imagery.
Figure 1.

The relationship between negative affect and odds of NSSI is moderated by positive affect.
Figure 2.
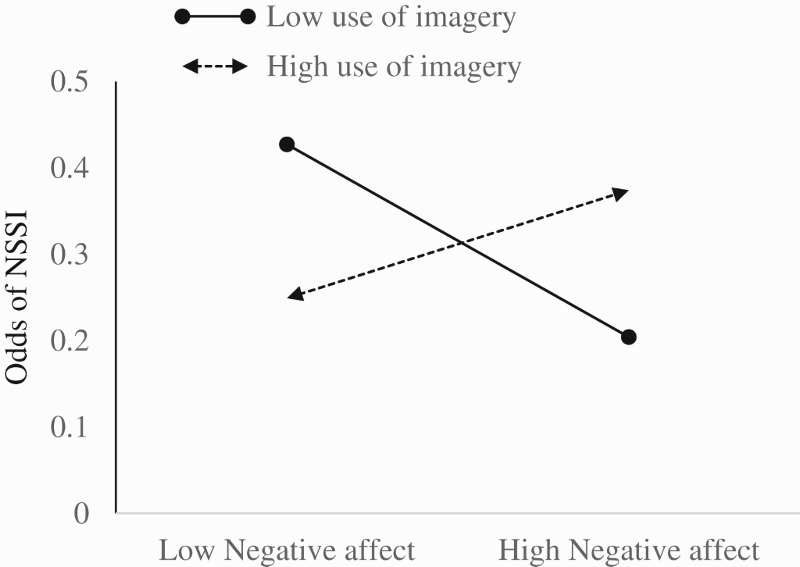
The use of imagery moderates the relationship between negative affect and odds of NSSI.
Predicting frequency of NSSI among youth who self-injure1
In the first step, the affective variables predicted frequency of NSSI, R2 = .11, F(4,122) = 3.85, p = .006, however only affect intensity accounted for unique variance in the criterion. The variables in the second step did not contribute unique variance to the regression equation, ΔR2 = .02, ΔF(3,119) = 1.06, p = .37. The final step containing the interaction terms did not predict frequency of NSSI, ΔR2 = .16, ΔF(15, 106) = 1.59, p = .09. However, examination of the coefficients revealed an interaction between negative and positive affect. Simple slopes analysis revealed a significant relationship between negative affect and frequency of NSSI at low levels of positive affect, b = .14, t = 1.87, p = .03, and an inverse relationship between negative affect and frequency of NSSI at high levels of positive affect, b = −0.28, t = −3.48, p < .001 (Figure 3).
Figure 3.

The relationship between negative affect and frequency of NSSI is moderated by positive affect.
Content of NSSI-related imagery
Only participants who self-injured were asked how often they found themselves thinking in images when they had the urge to self-injure. Of these, 93 (73.8%) reported thinking in images while the urge to self-injure was strong, with 53% thinking in images at least half the time. Frequency of NSSI was not related to how often participants experienced NSSI-related images (Table 2). The tendency to spontaneously use imagery in daily life (assessed with the SUIS) was associated with the frequency of images reported during the urge to self-injure, however vividness of images in daily life (assessed with the VVIQ) was not.
Written examples of images were provided by 82 (63.57%) participants; descriptions ranged from a single word (e.g. “blood”; “relief”) to detailed descriptions of images that were associated with the urge to self-injure:
Sometimes I pictures [sic] a dark violent scene of a volcano erupting and shooting lava into the air and molten rock burning its way through the landscape. The sky is black, its [sic] hot and there is smoke and soot around. The landscape turns to ash and there is nothing left but a charred empty space.
Four clear themes emerged from the thematic analysis: 1) images of blood; 2) images of the injury itself; 3) images related to negative emotion; 4) images related to a sense of escape.
Images of blood and of the injury itself were equally common (n = 25, 30.49%, each). Explicit images of blood were recorded (e.g. “collapsing to the ground and being found in a pool of blood”; “blood running down my arm”), while images related to the injury itself ranged from quite vague descriptions (e.g. “imagine myself doing the injury”), to detailed descriptions (e.g. “I would unintentionally visualise violent acts to my body”; “I had an image of stabbing myself through my chest and in the heart”). These descriptions also included the consequences of the injury (e.g. “Scars”; “ … what it would feel and look like”; “An image of myself after the self-injurious behaviour”).
Of the sample, 14 (17.07%) provided descriptions of images that related to negative emotionality. These included the emotional experiences preceding NSSI (e.g. “Frightening or disturbing images such as someone being in the house”; “darkness”; “a big black hole”) as well as the relief experienced after self-injuring (e.g. “feeling relaxed seeing the injury”). A number of participants reflected themes of escape in their descriptions (e.g. “The sensation of drowning as means of escape”; “me hiding safe in my bed and not at work, exposed, and unable to escape”). However, while the feeling of escape was evident in the descriptions participants provided, the ambiguity of written responses meant this was the category with the least agreement from the independent raters.
Discussion
The high prevalence and adverse consequences associated with NSSI necessitate further efforts to explain what increases the risk of self-injury, and what maintains the behaviour in people who have a history of NSSI. In this study we aimed to expand Emotional Cascade Theory to include positive as well as negative affect, and to include both verbally-based (i.e. rumination) and multisensory imagery-based cognitions. Our findings suggest that elements of Emotional Cascade Theory might usefully explain NSSI, but different factors are related to the odds of engaging in NSSI, and the frequency of the behaviour among people who self-injure. Specifically, while a lack of positive affect and psychological distress increase risk of NSSI, these are not directly related to the frequency with which someone engages in NSSI. Further, none of the potential moderators (rumination, imagery) were directly related to NSSI. Rather, both the odds of engaging in NSSI, and the frequency with which people engage in the behaviour, are best conceptualised as a complex interplay between affect and cognitions.
Affect and NSSI
It is not surprising that a lack of positive affect and heighted distress increase odds of NSSI, but it was unexpected that these are not related to frequency of NSSI. Arguably, the experience of distress and lack of a positive outlook are necessary pre-cursors to the decision to self-injure, but are not salient factors in the maintenance of behaviour. The observation that affect intensity was inversely related to frequency of NSSI was unexpected, and seems inconsistent with Emotional Cascade Theory. Research exploring the role of affect intensity in NSSI has produced equivocal results. In general, self-report studies tend to observe that people who self-injure report increased affect intensity, relative to people with no history of NSSI, but these findings are rarely held up in laboratory work (Davis et al., 2014; Gratz & Roemer, 2008). It may be that people who self-injure retrospectively explain their NSSI as a response to intense emotions, but that this intensity does not relate to how often they engage in self-injury. Conversely, the relationship between affect intensity and frequency of NSSI might plausibly be moderated by other factors such as distress tolerance and ability to regulate emotional experience. Future work investigating these possibilities is needed.
It is interesting to note that positive and negative affect interact to predict both history of NSSI and the frequency with which people engage in the behaviour, yet the relationships are quite different. Positive and negative affect were weakly correlated in this sample (−.21), providing further support for positive and negative affect being separable dimensions that are not simply polar opposites of an affective scale. Further, our findings suggest that not only do positive and negative affect work in concert as they relate to NSSI, but the way in which they relate to NSSI is dependent on the specific nature of the behaviour under investigation. In predicting odds of NSSI, positive affect appears protective, related to reduced odds of NSSI even in the presence of negative affect. Although the individual slope was not significantly different from zero (perhaps due to a lack of power), the significant interaction does confirm the effect of positive affect is different from that of negative affect. This mirrors past work highlighting that a lack of positive affect could be a risk factor for NSSI onset (Gratz et al., 2006). Enhancing positive affect has also been found to have a potent impact on well-being in mental disorders such as depression, particularly within the context of elevated negative affect (Cheng, 2006; Yamasaki & Uchida, 2016). Conversely, when predicting frequency of NSSI, people experiencing higher positive affect self-injured more often at low levels of negative affect, although this positivity was protective at high levels of negative affect. In sum, experiencing positive affect may be protective against engaging in NSSI, and reduce the frequency of NSSI when experiencing intense negative affect. However, greater positive affect was associated with more frequent NSSI at lower levels of negative affect.
These apparently discrepant results might relate to the functions of NSSI. People who self-injure to experience positive effect (e.g. a rush or high) might report positive affect as a result of their NSSI (Jenkins & Schmitz, 2012). That is, their frequent NSSI, when not experiencing intense negative affect, may give them a sense of positive affect. Rather than using NSSI to escape from negative affect, these youth might also be using NSSI to enhance positive affect. Conversely, people may interpret the relief NSSI provides as a positive emotion, and thus report more positive affect. On the other hand, people who self-injure primarily as a way to cope with intense negative affect might do so less often if they also experience frequent positive affect. That negative and positive affect interact in this way underscores the need to consider positive affect in models of emotion regulation related to NSSI. It is clear that not only is regulation of negative affect an important consideration in the initiation and maintenance of NSSI, but that this can depend on the frequency with which individuals also experience positive affect.
Imagery and NSSI
We assessed the use of mental imagery in daily life and the ability to produce vivid images to explore how non-verbal cognitions might fit within the scope of Emotional Cascade Theory. Our findings suggest that frequent use of imagery increases odds of NSSI, particularly in the context of negative affect. Although the scale used in this study does not assess impact of emotional imagery or use of NSSI-related images, the general tendency to think in images may also relate to seeing mental images of NSSI. Depending on the content of these images, this may increase the salience of NSSI as a viable emotion regulation option. Examining the content of NSSI-specific images in this sample (through written descriptions provided by participants), images which concentrate on intense emotional experiences likely work in the same way as rumination, increasing distress and developing a negative emotional cascade. In this case, risk of NSSI to break this cycle is increased. In line with recent cognitive-emotional theories of NSSI, images of the subsequent relief and escape from distress will similarly increase risk of NSSI (Hasking, Whitlock, Voon, & Rose, in press). Further, images of NSSI related to the injury itself may serve as a mental rehearsal for the behaviour, allowing someone to find the courage to deliberate harm themselves. Previous research has highlighted the particularly compelling nature of suicidal imagery (Crane, Shah, Barnhofer, & Holmes, 2012; Hales, Deeprose, Goodwin, & Holmes, 2011), and that suicidal imagery predicts intensity of suicidal ideation (Ng, Di Simplicio, McManus, Kennerley, & Holmes, 2016). Together with evidence of imagery facilitating behaviour (e.g. Libby, Schaeffer, Eibach, & Slemmer, 2007; Whiting & Dixon, 2013), this suggests that NSSI imagery may play a role in acting on the self-injury urges. Similar to repeated NSSI contributing to an acquired capability for suicidal behaviour (Joiner, 2005; Willoughby, Heffer, & Hamza, 2015), repeated imagery may facilitate the ability to self-injure.
Limitations and suggestions for future research
This is the first study, to the best of our knowledge, to explore imagery in the context of Emotional Cascade Theory. As such our findings are tentative and require replication with larger, more representative samples. Given Emotional Cascade Theory was designed to explain dysregulated behaviours in the context of borderline personality disorder (Selby & Joiner, 2009), further examination of how images relate to patterns of NSSI in clinical samples is also warranted.
Imagery-enhanced treatments have shown efficacy in anxiety disorders (McEvoy & Saulsman, 2014; McEvoy et al., 2015) and could well offer a novel approach to addressing NSSI. However before treatments can be developed we require a much more nuanced understanding of imagery in the context of NSSI. Specifically, we could ask how individuals appraise images related to NSSI. What kind of images might elevate distress and which might reduce it? Which might encourage or discourage NSSI? What kind of images arise when people experience an urge to self-injure but do not act on this urge? Answers to all these questions could inform imagery-enhanced initiatives with the aim of both preventing and intervening in NSSI. Further, use of measures which assess the impact of emotional prospective images in daily life on subsequent NSSI (e.g. the Impact of Future Events Scale; Deeprose & Holmes, 2010) would also be informative.
The aim of the current study was to assess idiosyncratic, self-generated mental imagery. However, an important consideration is that self-report assessments of imagery are generally language-based, and thus may lose important qualities of mental imagery. As knowledge accumulates about the nature of common mental imagery that encourages and discourages NSSI, future cognitive assessments of mental imagery may be able to circumvent language-based assessments. For instance, associations between NSSI, imagery and thoughts associated with engagement and disengagement from NSSI could be included in measures such as the Implicit Association Test (Greenwald, McGhee, & Schwartz, 1998) during urges to engage in NSSI, and before and after interventions.
Surprisingly, rumination was not related to NSSI in bivariate analyses, and failed to emerge as a unique predictor, or as a moderator of the affect-NSSI relationship, in the multivariate models. It is plausible that in this non-clinical sample levels of rumination were not sufficiently high to demonstrate a relationship with NSSI. Yet, mean scores on the RTQ, while lower than those observed in clinical samples, are higher than previously reported in undergraduate samples (McEvoy et al., 2014), suggesting the failure to observe an effect in this study is unlikely due to a floor effect in rumination. While other measures of rumination focus on particular forms of rumination (e.g. depressive rumination, brooding; Nolen-Hoeksema & Morrow, 1991), our measure was explicitly designed to capture tendencies to engage in rumination separately from depression or anxiety symptoms; thus it may be that this general tendency to ruminate does not adequately capture the relationship. It is also likely that although rumination intensifies affect, and subsequently increases risk of NSSI, this cycle is best captured through methodologies that allow exploration of the dynamic interplay between affect and cognitions in real time (e.g. ecological momentary assessment; Selby et al., 2013).
Naturally the cross-sectional design and the retrospective reporting of NSSI cannot answer questions about direction of effects, and longitudinal studies are warranted. Of note, retrospective reporting of NSSI-related images could be subject to memory bias, whereby people report “typical” images rather than more accurate or specific images that precede individual episodes of NSSI. Similarly, affect can be assessed with reference to different time frames (e.g. trait affect, last week, momentary affect); affect over longer or shorter periods may be differentially related to the use of rumination and imagery, and consequently outcomes such as NSSI. Momentary assessment studies, and/or real time monitoring of the thoughts and images that precede and follow NSSI, would provide a more detailed understanding of the role both affect and images play in NSSI.
Conclusion
In assessing both positive and negative affect, and the moderating role of imagery within the context of Emotional Cascade Theory, we have provided support for the importance of positive affect in NSSI. Additionally, that positive and negative affect work together in predicting both odds of NSSI and the frequency with which people engage in the behaviour suggests interesting avenues for future research in how emotional experience underpins NSSI. Likewise, these findings have implications for clinicians, parents and others working with young people who self-injure. Notably, our work suggests that imagery might be an important variable underlying NSSI, and one which could be harnessed in a therapeutic context to minimise NSSI. Further work is required to fruitfully explore these options.
Supplementary Material
Funding Statement
This study was supported, in part, by a grant awarded to Peter McEvoy, Penelope Hasking, and Clare Rees by the Research and Development Committee of the School of Psychology and Speech Pathology, Faculty of Health Sciences, Curtin University: [grant number SRAF-2014-37] and a Merit Award to Peter McEvoy from the Department of Health Western Australia: [grant number RES53597]. Martina Di Simplicio is supported by a Medical Research Council Career Development Fellowship: [grant number MC-A060-5PR50].
Note
As the distribution of residuals was not perfectly normal, data were subjected to both square root and log transformations. Regression analyses were conducted three times, with square root transform, log transform and untransformed data. Results for all three analyses were the same. Results of untransformed data are reported for ease of interpretation.
Disclosure statement
No potential conflict of interest was reported by the authors.
ORCID
Peter M. McEvoyhttp://orcid.org/0000-0003-2924-6760
References
- Aiken L. S., & West S. G. (1991). Multiple regression: Testing and interpreting interactions. Newbury Park, CA: Sage. [Google Scholar]
- Arbuthnott A. E., Lewis S. P., & Bailey H. N. (2015). Rumination and emotions in nonsuicidal self-injury and eating disorder behaviours: A preliminary test of the emotional cascade model. Journal of Clinical Psychology, 71, 62–71. doi: 10.1002/jclp.22115 [DOI] [PubMed] [Google Scholar]
- Baker T. G., & Lewis S. P. (2013). Responses to online photographs of non-suicidal self-injury: A thematic analysis. Archives of Suicide Research, 17, 223–235. doi: 10.1080/13811118.2013.805642 [DOI] [PubMed] [Google Scholar]
- Beck A. T. (1976). Cognitive therapy and the emotional disorders. New York, NY: Meridian. [Google Scholar]
- Bentley K. H., Nock M. K., & Barlow D. H. (2014). The four-function model of nonsuicidal self-injury: Implications for assessment and psychological treatment. Clinical Psychological Science, 2, 638–656. doi: 10.1177/2167702613514563 [DOI] [Google Scholar]
- Borkovec T. D., Alcaine O. M., & Behar E. (2004). Avoidance theory of worry and generalized anxiety disorder. In Heimberg R., Turk C., & Mennin D. (Eds.), Generalized anxiety disorder: Advances in research and practice (pp. 77–108). New York, NY: Guilford Press. [Google Scholar]
- Bresin K. (2014). Five indices of emotion regulation in participants with a history of non-suicidal self-injury: A daily diary study. Behavior Therapy, 45, 56–66. doi: 10.1016/j.beth.2013.09.005 [DOI] [PubMed] [Google Scholar]
- Bresin K., & Verona E. (2016). Pain, affect and rumination: An experimental test of the emotional cascade theory in two undergraduate samples. Journal of Experimental Psychopathology, 7, 205–224. doi: 10.5127/jep.047715 [DOI] [Google Scholar]
- Cheng S. T. (2006). Negative emotions make positive emotions more salient in well-being appraisal. Personality and Individual Differences, 40, 557–567. doi: 10.1016/j.paid.2005.08.002 [DOI] [Google Scholar]
- Claes L., Klonsky E. D., Muehlenkamp J., Kuppens P., & Vandereycken W. (2010). The affect-regulation function of non-suicidal self-injury in eating-disordered patients: Which affect states are regulated? Comprehensive Psychiatry, 51, 386–392. doi: 10.1016/j.comppsych.2009.09.001 [DOI] [PubMed] [Google Scholar]
- Cloos M., Weßlau C., Steil R., & Höfling V. (2017). Latent classes of dysregulated behaviors relate to negative mental images. Journal of Psychopathology and Behavioral Assessment, 39, 303–312. doi: 10.1007/s10862-016-9578-2 [DOI] [Google Scholar]
- Cohen J. N., Stange J. P., Hamilton J. L., Burke T. A., Jenkins A., Ong M., … Alloy L. B. (2015). The interaction of affective states and cognitive vulnerabilities in the prediction of non-suicidal self-injury. Cognition and Emotion, 29, 539–547. doi: 10.1080/02699931.2014.918872 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crane C., Shah D., Barnhofer T., & Holmes E. (2012). Suicidal imagery in a previously depressed community sample. Clinical Psychology & Psychotherapy, 19, 57–69. doi: 10.1002/cpp.741 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crawford J. R., & Henry J. D. (2004). The positive and negative affect schedule (PANAS): Construct validity, measurement properties and normative data in a large non-clinical sample. British Journal of Clinical Psychology, 43, 245–265. doi: 10.1348/0144665031752934 [DOI] [PubMed] [Google Scholar]
- Davis T. S., Mauss I. B., Lumian D., Troy A., Shallcross A. J., Zarolia P., & Ford B. Q. (2014). Emotional reactivity and emotion regulation among adults with a history of self-harm: Laboratory self-report and functional MRI evidence. Journal of Abnormal Psychology, 123, 499–509. doi: 10.1037/a0036962 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deeprose C., & Holmes E. (2010). An exploration of prospective imagery: The Impact of Future Events Scale. Behavioural and Cognitive Psychotherapy, 38, 201–209. doi: 10.1017/S1352465809990671 [DOI] [PubMed] [Google Scholar]
- Fox K. R., Franklin J. C., Ribeiro J. D., Kleiman E. M., Bentley K. H., & Nock M. K. (2015). Meta-analysis of risk factors for nonsuicidal self-injury. Clinical Psychology Review, 42, 156–167. doi: 10.1016/j.cpr.2015.09.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glenn C. R., & Klonsky E. D. (2010). The role of seeing blood in non-suicidal self-injury. Journal of Clinical Psychology, 66, 466–473. [DOI] [PubMed] [Google Scholar]
- Gratz K. L., & Roemer L. (2008). The relationship between emotion dysregulation and deliberate self-harm among female undergraduate students at an urban commuter university. Cognitive Behaviour Therapy, 37, 14–25. doi: 10.1080/16506070701819524 [DOI] [PubMed] [Google Scholar]
- Gratz K. L., Rosenthal M. Z., Tull M. T., Lejuez C. W., & Gunderson J. G. (2006). An experimental investigation of emotion dysregulation in borderline personality disorder. Journal of Abnormal Psychology, 115, 850–855. doi: 10.1037/0021-843X.115.4.850 [DOI] [PubMed] [Google Scholar]
- Greenwald A. G., McGhee D. E., & Schwartz J. L. (1998). Measuring individual differences in implicit cognition: The implicit association test. Journal of Personality and Social Psychology, 74, 1464–1480. doi: 10.1037/0022-3514.74.6.1464 [DOI] [PubMed] [Google Scholar]
- Hackmann A., Bennett-Levy J., & Holmes E. A. (2011). Oxford guide to imagery in cognitive therapy. Oxford: Oxford University Press. [Google Scholar]
- Hales S. A., Deeprose C., Goodwin G. M., & Holmes E. A. (2011). Cognitions in bipolar disorders versus unipolar depression: Imagining suicide. Biploar Disorder, 13, 651–661. doi: 10.1111/j.1399-5618.2011.00954.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hasking P., Whitlock J., Voon D., & Rose A. (in press). A cognitive-emotional model of NSSI: Using emotion regulation and cognitive processes to explain why people self-injure. Cognition & Emotion, doi: 10.1080/02699931.2016.1241219 [DOI] [PubMed] [Google Scholar]
- Holmes E. A., Bonsall M. B., Hales S. A., Mitchell H., Renner F., Blackwell S. E., … Di Simplicio M. (2016). Applications of time-series analysis to mood fluctuations in bipolar disorder to promote treatment innovation: A case series. Translational Psychiatry, 6, e720. doi: 10.1038/tp.2015.207 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holmes E. A., & Mathews A. (2010). Mental imagery in emotion and emotional disorders. Clinical Psychology Review, 30, 349–362. doi: 10.1016/j.cpr.2010.01.001 [DOI] [PubMed] [Google Scholar]
- Jenkins A. B., & Schmitz M. F. (2012). The roles of affect dysregulation and positive affect in non-suicidal self-injury. Archives of Suicide Research, 16, 212–225. doi: 10.1080/13811118.2012.695270 [DOI] [PubMed] [Google Scholar]
- Joiner T. E. (2005). Why people die by suicide. Cambridge, MA: Harvard University Press. [Google Scholar]
- Kessler R. C., Andrews G., Colpe L. J., Hiripi E., Mroczek D. K., Normand S. L., … Zaslavsky A. M. (2002). Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychological Medicine, 32, 959–976. doi: 10.1017/S0033291702006074 [DOI] [PubMed] [Google Scholar]
- Klonsky E. D., & Olino T. M. (2008). Identifying clinically distinct subgroups of self-injurers among young adults: A latent class analysis. Journal of Consulting and Clinical Psychology, 76, 22–27. doi: 10.1037/0022-006X.76.1.22 [DOI] [PubMed] [Google Scholar]
- Larsen R. J. (1984). Theory and measurement of affect intensity as an individual difference characteristic. Dissertation Abstracts International, 85, 2297B (University Microfilms No. 84-22112). [Google Scholar]
- Larsen R. J., & Diener E. (1987). Affect intensity as an individual difference characteristic: A review. Journal of Research in Personality, 21, 1–39. doi: 10.1016/0092-6566(87)90023-7 [DOI] [Google Scholar]
- Lewis S. P., & Baker T. (2011). The possible risks of self-injury web sites: A content analysis. Archives of Suicide Research, 15, 390–396. doi: 10.1080/13811118.2011.616154 [DOI] [PubMed] [Google Scholar]
- Lewis S. P., Heath N. L., Michal N., & Duggan J. M. (2012). Non-suicidal self-injury, youth and the internet: What mental health professionals need to know. Child and Adolescent Psychiatry and Mental Health, 6. doi: 10.1186/1753-2000-6-13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewis S. P., & Mehrabkhani S. (2016). Every scar tells a story: Insight into people’s self-injury scar experiences. Counselling Psychology Quarterly, 29, 296–310. doi: 10.1080/09515070.2015.1088431 [DOI] [Google Scholar]
- Libby L. K., Schaeffer E. M., Eibach R. P., & Slemmer J. A. (2007). Picture yourself at the polls: Visual perspective in mental imagery affects self-perception and behavior. Psychological Science, 18, 199–203. doi: 10.1111/j.1467-9280.2007.01872.x [DOI] [PubMed] [Google Scholar]
- Marks D. F. (1995). New directions for imagery research. Journal of Mental Imagery, 19, 153–167. [Google Scholar]
- McEvoy P. M., Erceg-Hurn D., Saulsman L., & Thibodeau M. (2015). Imagery enhancements increase the effectiveness of cognitive behavioural group therapy for social anxiety disorder: A benchmarking study. Behaviour Research and Therapy, 65, 42–51. doi: 10.1016/j.brat.2014.12.011 [DOI] [PubMed] [Google Scholar]
- McEvoy P., Hayes S., Hasking P., & Rees C. (2017). Acting on the urge to self-injure: Which thoughts, images, and appraisals encourage and discourage the cycle? Journal of Behavior Therapy and Experimental Psychiatry, 57, 163–171. doi: 10.1016/j.jbtep.2017.05.010 [DOI] [PubMed] [Google Scholar]
- McEvoy P. M., Mahoney A. E., & Moulds M. (2010). Are worry, rumination, and post-event processing one and the same? Development of the repetitive thinking questionnaire. Journal of Anxiety Disorders, 24, 509–519. doi: 10.1016/j.janxdis.2010.03.008 [DOI] [PubMed] [Google Scholar]
- McEvoy P. M., & Saulsman L. M. (2014). Imagery-enhanced cognitive behavioural group therapy for social anxiety disorder: A pilot study. Behaviour Research and Therapy, 55, 1–6. doi: 10.1016/j.brat.2014.01.006 [DOI] [PubMed] [Google Scholar]
- McEvoy P. M., Thibodeau M., & Asmundson G. J. G. (2014). Trait repetitive negative thinking: A brief transdiagnostic assessment. Journal of Experimental Psychopathology, 5, 382–398. doi: 10.5127/jep.037813 [DOI] [Google Scholar]
- Muehlenkamp J. J., Engel S. G., Waderson A., Crosby R. D., Wonderlich S. A., Simonrich H., & Mitchell J. E. (2009). Emotional states preceding and following acts of non-suicidal self-injury in bulimia nervosa patients. Behaviour Research and Therapy, 47, 83–87. doi: 10.1016/j.brat.2008.10.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nelis S., Holmes E. A., Griffith J. W., & Raes F. (2014). Mental imagery during daily life: Psychometric evaluation of the Spontaneous Use of Imagery Scale (SUIS). Psychologica Belgica, 54, 19–32. doi: 10.5334/pb.ag [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ng R. M. K., Di Simplicio M., McManus F., Kennerley H., & Holmes E. (2016). "Flash-forwards" and suicidal ideation: A prospective investigation of mental imagery, entrapment and defeat in a cohort from the Hong Kong Mental Morbidity Survey. Psychiatry Research, 246, 453–460. doi: 10.1016/j.psychres.2016.10.018 [DOI] [PubMed] [Google Scholar]
- Nicolai K. A., Wielgus M. D., & Mezulis A. (2016). Identifying risk for self-harm: Rumination and negative affectivity in the prospective prediction of nonsuicidal self-injury. Suicide and Life-Threatening Behavior, 46, 223–233. doi: 10.1111/sltb.12186 [DOI] [PubMed] [Google Scholar]
- Nock M. K. (2009). Why do people hurt themselves? New insights into the nature and functions of self-injury. Current Directions in Psychological Science, 18, 78–83. doi: 10.1111/j.1467-8721.2009.01613.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nock M. K., & Prinstein M. J. (2004). A functional approach to the assessment of self-mutilative behaviour. Journal of Consulting and Clinical Psychology, 72, 885–890. doi: 10.1037/0022-006X.72.5.885 [DOI] [PubMed] [Google Scholar]
- Nolen-Hoeksema S., & Morrow J. (1991). A prospective study of depression and posttraumatic stress symptoms after a natural disaster: The 1989 Loma Prieta earthquake. Journal of Personality and Social Psychology, 61, 115–121. doi: 10.1037/0022-3514.61.1.115 [DOI] [PubMed] [Google Scholar]
- Reisberg D., Pearson D. G., & Kosslyn S. M. (2003). Intuitions and introspections about imagery: The role of imagery experience in shaping an investigator’s theoretical views. Applied Cognitive Psychology, 17, 147–160. doi: 10.1002/acp.858 [DOI] [Google Scholar]
- Russell J. A., & Carroll J. M. (1999). On the bipolarity of positive and negative affect. Psychological Bulletin, 125, 3–30. doi: 10.1037/0033-2909.125.1.3 [DOI] [PubMed] [Google Scholar]
- Selby E. A., Franklin J., Carson-Wong A., & Rizvi S. L. (2013). Emotional cascades and self-injury: Investigating instability of rumination and negative emotion. Journal of Clinical Psychology, 69, 1213–1227. doi: 10.1002/jclp.21966 [DOI] [PubMed] [Google Scholar]
- Selby E. A., & Joiner T. E. (2009). Cascades of emotion: The emergence of borderline personality disorder from emotional and behavioral dysregulation. Review of General Psychology, 13, 219–229. doi: 10.1037/a0015687 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sternudd H. T. (2012). Photographs of self-injury: Production and reception in a group of self-injurers. Journal of Youth Studies, 15, 421–436. doi: 10.1080/13676261.2012.663894 [DOI] [Google Scholar]
- Swannell S., Martin G., Page A., Hasking P., & St John N. (2014). Prevalence of nonsuicidal self-injury in nonclinical samples: Systematic review, meta-analysis and meta-regression. Suicide and Life-Threatening Behavior, 44, 273–303. doi: 10.1111/sltb.12070 [DOI] [PubMed] [Google Scholar]
- Victor S. E., & Klonsky E. D. (2014). Daily emotion in non-suicidal self-injury. Journal of Clinical Psychology, 70, 364–375. doi: 10.1002/jclp.22037 [DOI] [PubMed] [Google Scholar]
- Watson D., Clark L. A., & Tellegen A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54, 1063–1070. doi: 10.1037/0022-3514.54.6.1063 [DOI] [PubMed] [Google Scholar]
- Watson D., & Tellegen A. (1999). Issues in the dimensional structure of affect – effects of descriptors, measurement error, and response formats: Comment on Russell and Carroll (1999). Psychological Bulletin, 125, 601–610. doi: 10.1037/0033-2909.125.5.601 [DOI] [Google Scholar]
- Welch S. S., Linehan M. M., Sylvers P., & Chittams J. (2008). Emotional responses to self-injury imagery among adults with borderline personality disorder. Journal of Consulting and Clinical Psychology, 76, 45–51. doi: 10.1037/0022-006X.76.1.45 [DOI] [PubMed] [Google Scholar]
- Whiting S. W., & Dixon M. R. (2013). Effects of mental imagery on gambling behavior. Journal of Gambling Studies, 29, 525–534. doi: 10.1007/s10899-012-9314-0 [DOI] [PubMed] [Google Scholar]
- Whitlock J., Muehlenkamp J., Eckenrode J., Purington A., Abrams G. B., Barriera P., & Kress V. (2013). Nonsuicidal self-injury as a gateway to suicide in young adults. Journal of Adolescent Health, 52, 486–492. doi: 10.1016/j.jadohealth.2012.09.010 [DOI] [PubMed] [Google Scholar]
- Willoughby T., Heffer T., & Hamza C. A. (2015). The link between nonsuicidal self-injury and acquired capability for suicide: A longitudinal study. Journal of Abnormal Psychology, 124, 1110–1115. doi: 10.1037/abn0000104 [DOI] [PubMed] [Google Scholar]
- Yamasaki K., & Uchida K. (2016). Effects of positive and negative affect on depression: Considering the activation dimension and balance of affect. International Journal of Psychology and Behavioral Sciences, 6, 139–147. [Google Scholar]
- Yik M. (2007). Culture, gender, and the bipolarity of momentary affect. Cognition & Emotion, 21, 664–680. doi: 10.1080/02699930600823702 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.