

Abstract
We analyzed the metacarpophalangeal pattern profile (MCPP) of 19 individuals with Brachmann-de Lange syndrome (BDLS) and calculated a mean syndrome profile. Fourteen of 19 individuals with BDLS had significant positive correlations which indicated clinical homogeneity. Discriminant analysis of individuals with BDLS compared with a sample of normal individuals produced a correct classification rate of 100% based on a function of 2 MCPP variables that may provide a useful tool for assisting in the diagnosis of BDLS. An average pattern variability index calculated for the BDLS patients was 1.9 indicating an abnormal hand pattern in this syndrome.
Keywords: metacarpophalangeal pattern profile (MCPP), pattern variability index, discriminant analysis, correlation studies, de Lange syndrome
INTRODUCTION
The Brachmann-de Lange syndrome (BDLS) is a well-recognized condition of mental retardation, microbrachycephaly, micrognathia, small nose, synophrys, long curly eyelashes and hirsutism [de Lange, 1933; Berg et al., 1970; Peeters, 1975; Opitz, 1985]. The mode of inheritance is unknown, but autosomal dominant inheritance has been suggested [Robinson et al., 1985].
Metacarpophalangeal pattern profile (MCPP) analysis is an evaluation of the hand skeleton based on a comparison of the 19 tubular bone lengths to normal bone length standards, as described by Poznanski et al. [1972] and Garn et al. [1972]. This method provides a quantitative assessment of the amount and direction of abnormality of the hand skeleton. MCPP analysis has been used to evaluate numerous syndromes [Poznanski, 1984; Butler et al., 1986].
Presently BDLS is diagnosed on purely clinical grounds. Limb, mostly hand, anomalies have been known for decades; in the absence of oligodactyly, micromelia is the most common descriptor, followed in frequency by bony defects at the elbow, limiting extension in many cases, and pronation and supination in a few. Since there probably is no discontinuity between gross limb deficiency and apparent normality in the BDLS, we undertook MCPP analysis in 19 BDLS patients to study the more subtle changes that might be present in the hand skeleton and not grossly obvious to the clinician.
MATERIALS AND METHODS
Posterior-anterior hand radiographs on 13 white individuals (6 males and 7 females) with BDLS with an average age of 11.1 years and age range of 0.1 to 32 years (Table I) and hand patterns published from 6 affected individuals [Peeters, 1975] were analyzed in this study.
Table I.
Correlations Between Individual and Group Mean MCPP, Average Z Scores and Pattern Variability Indices in Brachmann-de Lange Syndrome
| Age (years) | Sex | Average Z score | Pattern variability indexb | Correlation |
|---|---|---|---|---|
| 0.5 | F | −3.2 | 0.65 | 0.57* |
| 2.0 | F | −2.9 | 2.17 | 0.35 |
| 2.0 | F | −4.6 | 1.70 | 0.59** |
| 2.0 | F | −9.6 | 1.50 | 0.77*** |
| 2.0 | F | −9.1 | 0.80 | 0.76*** |
| 2.5 | F | −3.1 | 1.67 | 0.34 |
| 31.0 | F | −6.1 | 1.25 | -0.02 |
| 0.1 | M | −8.7 | 5.00 | 0.63** |
| 2.0 | M | −7.8 | 8.40 | 0.56* |
| 18.0 | M | −7.7 | 0.89 | 0.83** |
| 24.0 | M | −4.9 | 0.59 | 0.20 |
| 26.0 | M | −4.0 | 0.86 | 0.56* |
| 32.0 | M | −4.7 | 1.99 | -0.21 |
| 3.0 | —a | −5.6 | 1.40 | 0.87*** |
| 5.0 | — | −4.5 | 2.20 | 0.78*** |
| 9.0 | — | −5.0 | 0.70 | 0.47* |
| 11.0 | — | −5.7 | 2.50 | 0.49* |
| 14.0 | — | −5.1 | 1.00 | 0.76*** |
| 18.0 | — | −4.6 | 0.60 | 0.60** |
P < 0.05 for two-tailed test.
P < 0.01 for two-tailed test.
P < 0.001 for two-tailed test.
Patients reported by Peeters [1975], but sex not given.
Pattern variability index [ΣΖ2/Ν − (ΣΖ/Ν)2] (an index above 0.70 considered abnormal).
The metacarpophalangeal bone lengths of each patient were measured in millimeters with a vernier caliper and compared to bone length standards (appropriate for age and sex) published by Garn et al. [1972], (white Americans, age 2 years to adulthood) and Poznanski [1974], (Gefferth Hungarian sample, birth to 15 months). Through these comparisons, Z score values for the 19 bones of each patient were obtained (Z score = observed bone length minus mean bone length divided by SD). Therefore, the MCPP on a given patient is a set of 19 Z scores, which may be plotted on a graph or subjected to various statistical procedures for study and comparison with the MCPP of other patients, or groups of patients [Poznanski et al., 1972], Pattern variability index [ΣZ2/N − (ΣZ/N)2] was also calculated from the MCPP data [Garn et al., 1987], This index is a useful way of quantifying the pattern variability in hand bone measurements for a particular condition.
Correlation Studies
We derived a mean pattern profile from the 19 patients based on the average Z score for each bone [Poznanski et al., 1972; Garn et al., 1972], The pattern from each patient was compared to this group mean pattern and to each other using Pearsonian correlation coefficients.
Discriminant Analysis
A forward stepwise method of discriminant analysis [Enslein et al., 1977] was performed on the 19 Z score variables and age of individuals from 2 groups: the 19 patients with BDLS and a control group of 41 healthy control individuals whose hand radiographs were randomly obtained. The 41 normal individuals included 17 males and 24 females, with an age range of 96/12 to 18 years and a mean age of 131/12 years.
RESULTS
Of the 361 individual bone measurements from the 19 patients, all but 8 measurements were outside the normal range (+ 2 to − 2 Z scores) in the BDLS patients. All measurements were below a Z score of − 1.1. Although all bones were consistently short, the shortest bone relative to normal was the first metacarpal (average Z score of − 6.8).
The mean Z scores of the 19 patients with BDLS fell between − 2.9 and − 9.6. The mean pattern profile based on the 19 patients with BDLS was well below the normal hand pattern and showed a distinct trough at the first metacarpal and a prominent peak at the second middle interphalanx (Fig. 1).
Fig. 1.

Mean MCPP on 19 individuals with Brachmann-de Lange syndrome. Star indicates the bones that were selected in the discriminant analysis.
Next, the correlation program was used to assess similarity between the mean pattern and each of the 19 individual patterns. Fourteen of 19 individuals had significant positive correlations (Table I).
Discriminant analysis of the normal and BDLS patients resulted in a discriminant function based on 2 of the 19 MCPP variables. In the discriminant analysis, patients with BDLS were distinguished from normal individuals at an overall correct classification rate of 100% in this sample using a cut-off at a discriminant value of 0 (Fig. 2). The 2 MCPP variables in the discriminant function were the Z scores representing the first metacarpal (X1); and the fourth middle interphalanx (X13).
Fig. 2.
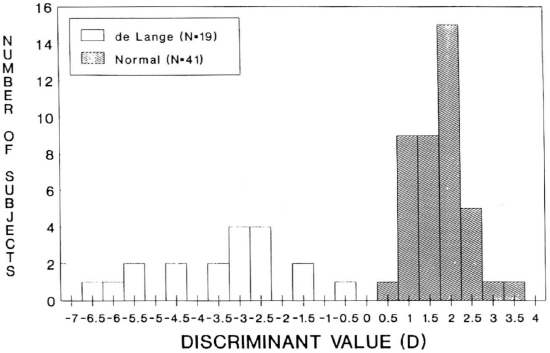
Histogram depicting normal and Brachmann-de Lange syndrome classification by discriminant analysis. D = 1.44 + 0.34 (X1) + 0.40 (X13).
Pattern variability index was calculated on each BDLS patient and the average index was 1.9 with an average Z score of − 5.6. An index above 0.70 is considered abnormal [Garn et al., 1987].
DISCUSSION
A short first metacarpal in this series agrees with previously published radiological reports by Kurlander and DeMyer [1967], Poznanski et al. [1971] and Halal and Preus [1979]. The mean hand pattern profile was well below normal and several peaks and valleys were found indicating the high pattern variability index of 1.9 which represents an abnormal pattern. The pattern variability index of 1.9 compares with 0.73 for 20 BDLS patients reported by Garn et al. [1987]. The average Z score was − 5.6(± 2.0 SD) for our 19 BDLS patients and − 5.2 for the patients reported by Garn et al. [1987]. The correlations of the BDLS individuals in our study suggest a relatively homogenous pattern with 74% of the individuals possessing a significant correlation with the Z score group mean. The correlation value of 0.47 was significant (P <0.05) between the mean hand pattern profile for our BDLS patients and the pattern reported by Peeters [1975]. Thus, a unique hand profile apparently exists for BDLS based on these measurements and after visual comparison with published profiles of other syndromes [Butler et al., 1986].
The discriminant analysis suggests effective delineation of BDLS patients with correct classification for all individuals. Additional studies with larger sample sizes are needed to test the power of the discriminant method in distinguishing patients with BDLS from normal subjects, and from patients with other conditions. In summary, the observations presented in this report suggest the potential of MCPP analysis for providing a useful tool for assisting in the diagnosis of BDLS.
ACKNOWLEDGMENTS
The authors acknowledge the use of the facilities of Computing Services, University of Kentucky, Lexington and Eastern Kentucky University, Richmond. The authors thank Margaret Lane, Sandy Cain, and Pamela Grimm for their technical assistance as well as Dr. Peg Davee and the Clover Bottom Developmental Center, Nashville, Tennessee for supplying hand x-rays.
Contributor Information
Merlin G. Butler, Division of Genetics, Departments of Pediatrics and Pathology (M.G.B.)
George A. Dahir, Department of Orthopaedics and Rehabilitation (G.A.D.)
David D. Gale, Vanderbilt University School of Medicine, Nashville, Tennessee; Eastern Kentucky University, Richmond, Kentucky (D.D.G.)
F. John Meaney, Arizona Department of Health Services, Phoenix, Arizona (F.J.M.).
REFERENCES
- Berg JM, McCreary BD, Ridler MAC, Smith GF (1970): ‘The de Lange Syndrome.” 1st Ed., New York: Pergamon Press. [Google Scholar]
- Butler MG, Meaney FJ, Kaler SG (1986): Metacarpophalangeal pattern profile analysis in clinical genetics: An applied anthropometric method. Am J Phys Anthropol 70:195–201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Lange C (1933): Sur un type nouveau de dégénération: Typus Amstelodamensis. Arch Méd Enf 36:713. [Google Scholar]
- Enslein K, Ralston A, Wilf HS (1977): “Statistical Methods for Digital Computers.” New York: John Wiley and Sons. [Google Scholar]
- Garn SM, Hertzog KP, Poznanski AK, Nagy JM (1972): Metacarpophalangeal length in the evaluation of skeletal malformation. Radiology 105:375–381. [DOI] [PubMed] [Google Scholar]
- Garn SM, Leonard WR, Poznanski AK (1987): Applications of the pattern variability index (OZ) to the quantification of dysmorphogenesis in the hand. Am J Med Genet 27:143–152. [DOI] [PubMed] [Google Scholar]
- Halal F, Preus M (1979): The hand profile in de Lange syndrome: Diagnostic criteria. Am J Med Genet 3:317–323. [DOI] [PubMed] [Google Scholar]
- Kurlander GJ, DeMyer W (1967): Roentgenology of the Brachmann-De Lange syndrome. Radiology 88:101–110. [DOI] [PubMed] [Google Scholar]
- Opitz JM (1985): The Brachmann-de Lange syndrome. Am J Med Genet 22:89–102. [DOI] [PubMed] [Google Scholar]
- Peeters FLM (1975): Radiologic manifestations of the Cornelia de Lange syndrome. Pediat Radiol 3:41–46. [DOI] [PubMed] [Google Scholar]
- Poznanski AK (1974): “The Hand in Radiological Diagnosis.” 1st Ed., Philadelphia: W.B. Saunders. [Google Scholar]
- Poznanski AK (1984): “The Hand in Radiological Diagnosis.” 2nd Ed., Philadelphia: W.B. Saunders. [Google Scholar]
- Poznanski AK, Garn SM, Holt JF (1971): The thumb in the congenital malformation syndromes. Radiology 100:115–129. [DOI] [PubMed] [Google Scholar]
- Poznanski AK, Garn SM, Nagy JM, Gall JC (1972): Metacarpophalangeal pattern profiles in the evaluation of skeletal malformations. Radiology 104:1–11. [DOI] [PubMed] [Google Scholar]
- Robinson LK, Wolfsberg E, Jones KL (1985): Brachmann-de Lange syndrome: Evidence for autosomal dominant inheritance. Am J Med Genet 22:109–115. [DOI] [PubMed] [Google Scholar]