

Abstract
The use of continuous subcutaneous insulin infusion (CSII) and continuous glucose monitoring (CGM) systems has gained wide acceptance in diabetes care. These devices have been demonstrated to be clinically valuable, improving glycemic control and reducing risks of hypoglycemia in ambulatory patients with type 1 diabetes and type 2 diabetes. Approximately 30–40% of patients with type 1 diabetes and an increasing number of insulin-requiring patients with type 2 diabetes are using pump and sensor technology. As the popularity of these devices increases, it becomes very likely that hospital health care providers will face the need to manage the inpatient care of patients under insulin pump therapy and CGM. The American Diabetes Association advocates allowing patients who are physically and mentally able to continue to use their pumps when hospitalized. Health care institutions must have clear policies and procedures to allow the patient to continue to receive CSII treatment to maximize safety and to comply with existing regulations related to self-management of medication. Randomized controlled trials are needed to determine whether CSII therapy and CGM systems in the hospital are associated with improved clinical outcomes compared with intermittent monitoring and conventional insulin treatment or with a favorable cost-benefit ratio.
Introduction
The prevalence of diabetes is steadily on the rise, such that more than 1 in every 10 adult individuals or 12.2% of the U.S. population aged 18 years or older is affected (1). Patients with diabetes have a threefold greater chance of hospitalization compared with those without diabetes (2). The annual incidence of diabetes as any listed diagnosis has more than doubled during the past two decades to a total of 7.2 million hospital discharges, accounting for a total of 43.1 million hospital days among U.S. adults affected (1,3). Current guidelines for the management of hyperglycemia recommend the use of intravenous insulin in the intensive care unit (ICU) and subcutaneous basal or basal-bolus insulin regimens in general medicine and surgery settings (4,5). Although effective in improving glycemic control and in reducing the risk of hospital complications (6,7), intensive insulin therapy results in frequent hypoglycemia, reported in 12–30% of patients (8–10). Thus, improving glycemic control while minimizing the rate of hypoglycemia is of major importance in the hospital because both hyperglycemia and hypoglycemia have been shown to be independent risk factors of poor clinical outcome and mortality (11–13).
During the past decade, diabetes technology has rapidly evolved, with new technologies being developed and improved every year. While most of the new technology development has aimed to improve diabetes care in the ambulatory setting, technology advances have also impacted the management of hospitalized patients with diabetes. Major areas of technology advances in diabetes are the use of continuous subcutaneous insulin infusion (CSII, or insulin pump) and the increasing availability of continuous glucose monitoring (CGM) systems for the management of patients with type 1 diabetes (T1D) and type 2 diabetes (T2D). These two critically important technologies have been studied in multiple randomized controlled trials in ambulatory patients, but there are few such trials in inpatients. This is in part because of the short duration of hospitalization, changes in clinical and nutritional status, and the time needed for device calibration and the warm-up period before accurate readings are obtained. In addition, among hospitalist physicians, there is lack of provider awareness and lack of health care professionals trained in the use of these devices, lack of uniform policies and guidelines for implementation in the hospital setting, and, in many hospitals, lack of expertise available for consultation on the use of insulin pumps and CGM technology.
We conducted a MEDLINE search for articles published between January 2005 and February 2018 using a combination of search terms including hospital hyperglycemia and diabetes, diabetes technology, insulin pump therapy/CSII, continuous glucose monitoring/CGM, and new therapies in inpatient diabetes care. In this article, we aim to review published evidence and discuss the application of these technological advances for the management of hospitalized patients with diabetes.
Insulin Pump Use in the Hospital
Approximately 3 million children and adults are estimated to have T1D in the U.S. (14), with incidence rates that have gradually increased during the last two decades (15,16). Similarly, the incidence of T1D in European countries has increased by 3–4% per year (17), leading to growing demands on inpatient services (17,18). Hospitalization rates in patients with T1D are about threefold higher compared with the general population (19,20). Although few studies have reported differences in hospital outcomes between patients with T1D and T2D, patients with T1D have longer hospital stays and higher rates of complications and hospital mortality compared with patients with T2D (21). Management of hospitalized patients with T1D usually differs from that of patients with T2D. Patients with T1D are often admitted for procedures that would normally be carried out by outpatient services (18,22). T1D patients must be treated with insulin therapy to prevent ketoacidosis, and they frequently have worse glycemic control and higher rates of hyperglycemia and hypoglycemia compared with patients with T2D (18,23). Frequent challenges in patients with T1D include difficulties in adjusting insulin doses during short- and long-term fasting or during nutritional support and in maintaining a consistent source of carbohydrate while modifying scheduled daily insulin therapy (18,23).
It is estimated that 400,000 patients with T1D in the U.S. are using insulin pumps (24,25). A recent report from the T1D Exchange Clinic Registry indicated that 60% of the 16,061 adult and pediatric patients with T1D in that cohort used an insulin pump (26,27). The number of pump users is expected to increase, as this technology has demonstrated significant improvements in diabetes management for adults and children with T1D by improving glycemic control, decreasing severe hypoglycemic episodes, and improving quality of life (28). As the popularity of CSII increases, hospital health care providers will face the need to manage the inpatient care of patients under insulin pump therapy.
When patients using CSII are hospitalized, a decision must be made as to whether the patient can continue on the insulin pump or not (Fig. 1). The conclusion depends on the ability of the patient to safely operate the pump and the health care provider’s familiarity with CSII (29). Inpatient health care professionals may not be familiar with insulin pump use, which may lead to medication errors, confusion among hospital staff, and potentially harmful outcomes for patients. Most insulin pump users are more knowledgeable than their hospital health care providers about diabetes management; therefore, experienced pump users may be encouraged to self-manage their diabetes during their hospitalization (30,31). Better patient satisfaction has been reported if patients can use their pump while in the hospital (31).
Figure 1.
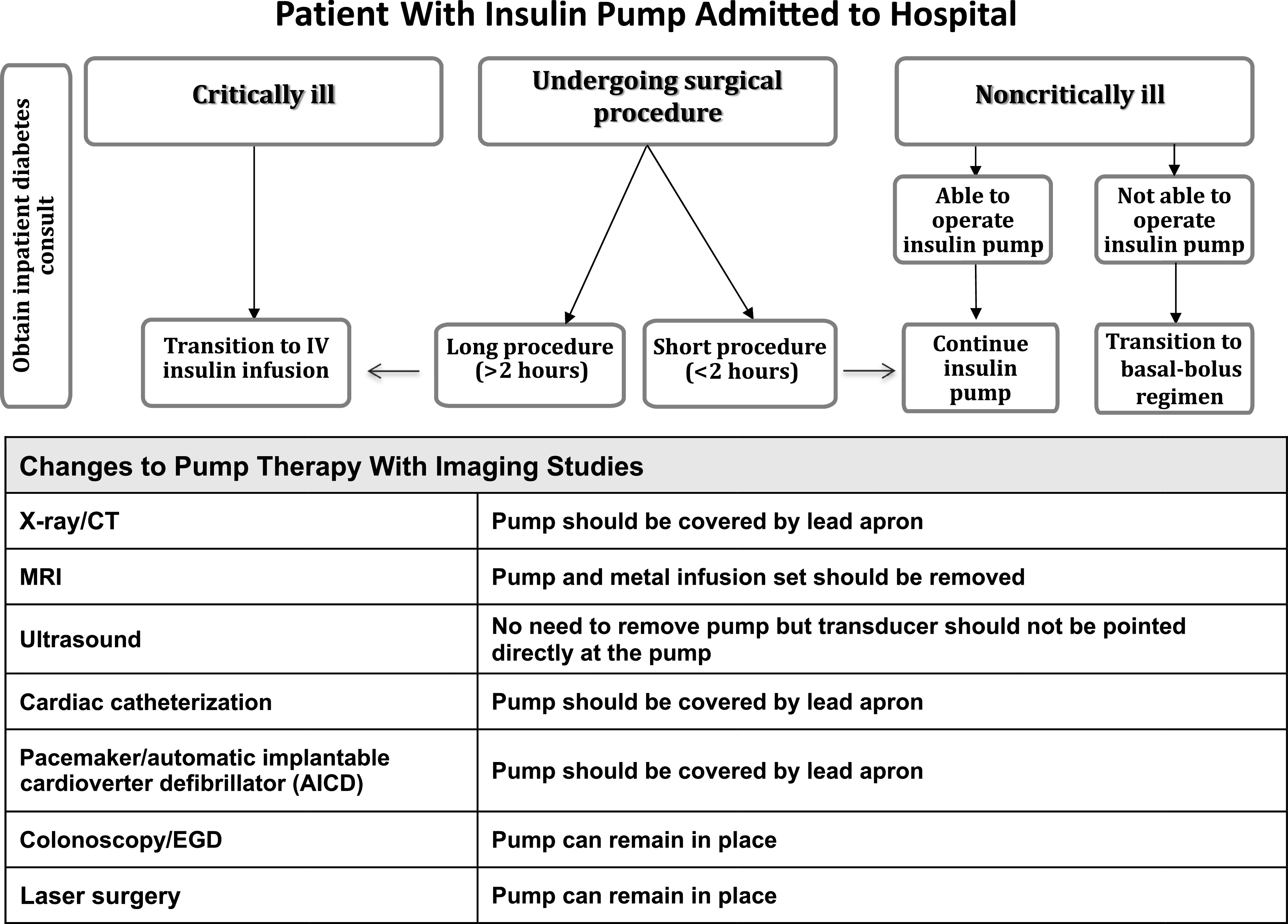
Recommendations on the course of action for hospitalized patient with T1D wearing an insulin pump (18). IV, intravenous; EGD, esophagogastroduodenoscopy.
Studies on insulin pumps in the hospital are sparse, uncontrolled, and mostly retrospective analyses. In a retrospective study of 136 patients involved in 253 hospitalizations over a 6-year period, CSII was continued for the entire duration of the hospital stay in 65% of the hospitalizations, used intermittently in 20%, and discontinued in 15%, with alternative insulin regimens given. There were no differences in the mean daily glucose levels; however, there were significantly fewer episodes of severe hyperglycemia (glucose >350 mg/dL [19.4 mmol/L]) and hypoglycemia (glucose <40 mg/dL [2.2 mmol/L]) in those who continued CSII compared with those taken off the pump (32). Similarly, a more recent study on 50 patients with 51 hospital admissions, 86% of whom had T1D, also reported no differences in mean blood glucose (BG), frequency of hyperglycemia, or hypoglycemic events among patients treated with CSII compared with those who were transitioned to a multiple daily injection (MDI) regimen (33). The authors concluded that with appropriate patient selection and usage guidelines, most patients using insulin pumps could safely have their therapy transitioned to the inpatient setting.
Bailon et al. (34) conducted a retrospective chart review in 35 admitted patients who had been receiving outpatient insulin pump therapy. The authors found that 91% had T1D. Of them, 62% were deemed candidates for continued insulin pump therapy during hospitalization. Reasons for discontinuing pump therapy at the time of admission were lack of additional pump supplies, threats of suicide or actual suicide attempts, malfunction of the pump, and altered level of consciousness. In a different study, the reasons for CSII discontinuation included patient preference, inability to safely demonstrate pump settings, and inexperience owing to recent initiation of CSII, while inability to correctly demonstrate appropriate pump settings, lack of family support, and postoperative mental status precluded restarting use of the insulin pump upon discharge (33).
The American Diabetes Association (ADA) and the American Association of Clinical Endocrinologists advocate allowing patients who are physically and mentally able to continue to use their pumps when hospitalized, having a hospital policy for CSII use, and engaging hospital personnel with expertise on pump management (35–37). They recommend that shortly after admission the inpatient diabetes team and/or the endocrinology service become promptly involved in helping with insulin adjustment and pump settings as well as in coordinating care after hospital discharge.
Current recommendations advocate the establishment of clear policies and procedures to guide patients and hospital staff in the management of diabetes with the use of insulin pumps (18) (Table 1). The hospital provider should obtain a detailed record of the type of insulin formulation and the pump settings on admission, including basal rate/rates, the carbohydrate ratio (grams of carbohydrate for 1 unit of insulin), and the correction or sensitivity factor. Clear physician’s orders with specifics on the type of diet, frequency of point-of-care glucose testing, basal rate, bolus, and correction-dose insulin settings should also be in place. In addition, the patient’s cognitive, emotional, and physical ability to manage his/her insulin pump during the hospitalization should also be considered when deciding whether to continue use of the pump while the patient is hospitalized. A signed patient agreement that specifies all the necessary tasks to be performed by the patient, consent to share information regarding pump settings with the health care staff, and the need to report any issues is also recommended.
Table 1.
Contraindications to insulin pump therapy in the hospital
| Impaired level of consciousness (except during short-term anesthesia) |
| Patient’s inability to correctly demonstrate appropriate pump settings |
| Critical illness requiring intensive care |
| Psychiatric illness that interferes with a patient’s ability to self-manage diabetes |
| Diabetic ketoacidosis and hyperosmolar hyperglycemic state |
| Refusal or unwillingness to participate in self-care |
| Lack of pump supplies |
| Lack of trained health care providers, diabetes educators, or diabetes specialist |
| Patient at risk for suicide |
| Health care decision |
The pump settings also include a target glucose level. In the outpatient setting, many patients with T1D aim for tight glucose control with a target set at 80–100 mg/dL (4.4–5.5 mmol/L), which may be too low for the hospital setting (18,38). No large randomized controlled trials have examined best glucose target levels for hospitalized patients with T1D; however, a systematic review of 19 studies (9 randomized and 10 observational) reported that in surgical noncritically ill hospitalized patients, the overall rate of infections can be significantly reduced by keeping glucose concentrations between 100 and 180 mg/dL (5.5–10 mmol/L) (6). The ADA (39) and the Endocrine Society (5) guidelines for the management of hyperglycemia in noncritically ill hospitalized patients recommended that patients with either T1D or T2D maintain goal fasting and premeal BG <140 mg/dL (7.8 mmol/L) and random glucose <180 mg/dL (10 mmol/L). Since 2017, the ADA’s Standards of Medical Care in Diabetes modified inpatients’ target glucose, recommending levels between 140 and 180 mg/dL (7.8–10 mmol/L) for most ICU as well as non-ICU medical surgery patients with diabetes (35). More stringent goals lower than 140 mg/dL (7.8 mmol/L) may be appropriate for selected patients, such as cardiac surgery patients and those with acute ischemic cardiac or neurological events, provided the targets can be achieved without significant hypoglycemia (31).
Contraindications to Insulin Pump Use in the Hospital
Contraindications to the use of insulin pumps in the hospital are shown in Table 1. If the decision is reached to discontinue insulin pump use, then the patient should be switched to a subcutaneous multidose insulin regimen (pump holiday protocol) (Table 2). The 24-h basal dose of insulin delivered by the pump should be replaced by long-acting basal insulin (glargine, detemir, or degludec). The insulin pump should be discontinued at least 2 h after the first injection of basal insulin. Mealtime insulin should be provided with subcutaneous rapid-acting insulin (aspart, lispro, or glulisine). The dose can be calculated as half of a patient’s usual total daily dose of insulin divided by three and given before each meal. Alternatively, the prandial dose can be calculated by allowing the patient to select the dose of insulin using the usual insulin-to-carbohydrate ratio. A correction dose of rapid-acting insulin should be ordered for high glucose levels based on the patient’s usual insulin sensitivity factor. For example, if the usual insulin sensitivity factor is 1 unit per 40 mg/dL (2.2 mmol/L), then for each 40 mg/dL (2.2 mmol/L) above the target range, the patient should receive 1 extra unit of rapid-acting insulin (40).
Table 2.
Transition from CSII to subcutaneous (SC) insulin regimen “pump holiday protocol”
| Stop CSII ∼2 h after SC basal insulin is given. | |
| Calculate 24-h basal dose of insulin delivered from pump setting. Total basal daily insulin can be given as once-daily or twice-daily injections. | |
| Prandial insulin can be calculated as half of a patient’s usual total daily dose of insulin divided by 3. | |
| Capillary BG should be measured before meals and bedtime. | |
| A correction-dose algorithm of rapid-acting insulin to be added to the prandial dose should be ordered for high BG levels based on the patient’s usual insulin sensitivity factor or by a sliding-scale protocol: | |
| BG before meals | Dose |
| <180 mg/dL (<10 mmol/L) | No correction |
| 181–220 mg/dL (10.1–12 mmol/L) | 1 unit |
| 221–260 mg/dL (12.1–14 mmol/L) | 2 units |
| 261–300 mg/dL (14.1–16 mmol/L) | 3 units |
| 301–340 mg/dL (16.1–18 mmol/L) | 4 units |
| 341–380 mg/dL (18.1–20 mmol/L) | 5 units |
| >380 mg/dL (>20.1 mmol/L) | 6 units, notify physician |
| Adjust basal and prandial insulin dose daily based on glucose values and nutritional intake. | |
| The pump can be restarted when the patient is able to resume responsibility or at hospital discharge. | |
Insulin Pump Use in Special Situations
Diabetic Ketoacidosis
Insulin pump failure can lead to diabetic ketoacidosis. Pump malfunction may result from blockage or leakage in the infusion set or connectors, causing an interruption of infusion flow (41). Because the subcutaneous depot of insulin is small with pump therapy (smaller than with an MDI regimen) and because it uses rapid-acting insulin with a short duration of action, any short-term interruption in the continuous flow of insulin could result in hyperglycemia and possibly diabetic ketoacidosis. In patients with diabetic ketoacidosis, the pump must be discontinued and the patient should be treated with continuous intravenous insulin administration as per hospital protocol. The patient may be transitioned back to the pump after resolution of the diabetic ketoacidosis when clinically stable and when the acid-base disorder is corrected. The intravenous insulin is continued for the first 2 h of the pump restart to allow the formation of a subcutaneous depot of insulin. Frequent BG monitoring is needed for several hours after the pump is restarted to ensure glycemic control.
Perioperative Period
Many patients undergoing ambulatory and short-term surgical procedures for up to 2–3 h could continue using their CSII device during the procedure (18,25,33,38,42). Table 3 includes a recommended insulin pump protocol for minor surgical procedures with anticipated length of surgery <2 h. This decision is to be based on the length of the procedure, postoperative recovery time, and whether exposure to an electromagnetic field (MRI, computed tomography, therapeutic radiation, or electric shock for defibrillation) is expected during or after surgery (Fig. 1). Prior to surgery, the patient’s pump settings should be reviewed and adjusted as needed by a trained professional. The patient should bring all necessary pump supplies to the hospital or outpatient surgical facility and insert a new subcutaneous infusion set outside the planned surgical area the day before surgery. Hospital policy for managing insulin pumps should be reviewed with the patient, and the patient should give written consent to abide by the policy. The presence of the insulin pump should be documented on admission and the pump inspected regularly throughout the hospital stay by nursing staff to ensure proper functioning. The infusion site should be inspected for signs of inflammation or leakage and to ensure that it is in a location away from the area where the surgery will occur. The anesthesiologist must have access to the insulin pump during surgery to allow it to be suspended or disconnected if necessary. If use of the insulin pump is to be discontinued during surgery in a patient with T1D, the patient should be managed with intravenous insulin infusion or with frequent subcutaneous insulin injections.
Table 3.
Recommended insulin pump protocol for minor surgical procedure with anticipated length of surgery <2 h
| Document insulin pump settings and current basal rate. | |
| Check BG every hour: | |
| BG <100 mg/dL (5.5 mmol/L) | Hold basal infusion rate, check BG every 30 min. |
| BG 101–140 mg/dL (5.6–7.7 mmol/L) | Decrease basal rate by 25%. |
| BG 141–180 mg/dL (7.8–10 mmol/L) | Maintain basal rate. |
| BG 181–220 mg/dL (10.1–12.2 mmol/L) | Increase basal rate by 25%. |
| BG >220 mg/dL (>12.2 mmol/L) | Increase basal rate by 25–50% and give 2–4 units as bolus insulin. |
Although no prospective randomized studies are available to prove the efficacy of CSII during the perioperative period, several retrospective studies and case reports have shown that CSII can be maintained safely. A retrospective study of 92 surgical cases found similar intraoperative glycemic control between patients on CSII continuation of basal rate with or without correctional insulin bolus and those converted to intravenous insulin (43). There was no significant difference in mean BG between continuation or conversion, with one or more intraoperative BG levels >180 mg/dL (10 mmol/L) in about 40% of patients in both groups. In a different retrospective study from a tertiary care hospital, Sobel et al. (42) reported their experience with 49 patients using insulin pump therapy who presented for 57 elective same-day surgeries. Patients treated with CSII had no episodes of intra- or postoperative hypoglycemia, and the mean postoperative glucose concentration was lower in patients with anticipated or actual surgical length ≤120 min compared with those with longer procedures (42).
Pregnancy and Delivery
Poorly controlled T1D has been associated with an increased risk of congenital birth defects, miscarriage, fetal death, and preeclampsia. Improved glycemic control and rigorous medication adjustments during gestation are associated with reduced complications. Insulin requirements follow a characteristic pattern in pregnancy, with a decrease in the first trimester and a rise in the second and third trimesters. Increases in insulin requirements of 36% to 114% from preconceptional baseline to the second and third trimesters have been reported (44,45). Recent studies have demonstrated that patients can be treated effectively with insulin pumps when compared with multiple subcutaneous insulin injections. Glycemic control and maternal or neonatal outcomes were comparable between women on insulin pump therapy and women on MDI (46–48). During labor and delivery, the maternal glucose level should be kept between 70 and 140 mg/dL (4–8 mmol/L). Intrapartum glucose levels, more than antepartum glucose levels, affect the risk of neonatal hypoglycemia, with hypoglycemia risk increasing for glucose levels <100 mg/dL (5.5 mmol/L) (49). Glucose should be measured every 1–2 h and dextrose 5% solution should be administered to prevent maternal hypoglycemia. After delivery, insulin requirement falls sharply and it is prudent to decrease the insulin dose to 25–40% of the predelivery dose to prevent hypoglycemia. This is particularly more important after cesarean section in women who may not be allowed to eat for several hours. Breast-feeding lowers insulin requirements, and the insulin dose should be decreased if necessary to prevent hypoglycemia.
Use of CSII After Hospital Discharge
Many studies and meta-analyses have shown that CSII represents one of the best available methods of physiological delivery of basal/prandial insulin in ambulatory patients with diabetes. Thus, it makes sense to continue CSII therapy while patients are in hospital and after discharge, if they can manage their pumps. Compared with MDI, CSII has been associated with improved glycemic control with lower levels of HbA1c and reduction of hypoglycemia in ambulatory patients with T1D and T2D. In addition, increasing evidence indicates that CSII is cost-effective compared with MDI for children and adults with T1D (37) and that it can improve quality of life. The American Association of Clinical Endocrinologists has published good-practice guidelines for the use of CSII. Prior to discharge, the physician or diabetes specialist should program the basal rate, which regulates the food-independent insulin requirements. This is usually done taking into consideration preadmission insulin requirements, activity levels, and overall glycemic control. Providers should reassess knowledge and the need for reeducation and adjustment of basal/prandial insulin recommendations as well as education on sick-day management and pump troubleshooting.
CGM
From the early 1970s, CGM prototypes were available for research projects aiming to develop a glucose sensor–controlled insulin infusion system. In 1977, Miles Laboratories produced the Biostator, a large bedside unit that incorporated an in-line venous cannula to measure glucose and calculated the correct insulin and dextrose infusion rate (50). This device had serious limitations in clinical practice, including its large size, the need for constant supervision, and the continuous withdrawing and discarding of venous blood to measure glucose levels ex vivo using a glucose oxidase–containing membrane. The first CGM device made available in the U.S. was the GlucoWatch Biographer (no longer in use). This device was worn like a wristwatch and provided glucose measurements every 10 min via transdermal extraction of tissue fluid by reverse iontophoresis, a process by which a device extracts glucose samples from fluids in the body by applying extremely low electric currents to intact skin (51). The first CGM system, a retrospective CGM device by MiniMed, was first approved by the U.S. Food and Drug Administration (FDA) in 1999 (50). During the past two decades, considerable technological progress has resulted in the regulatory approval of multiple continuous and semicontinuous glucose monitors, which have provided benefits to many people with diabetes.
CGM devices can be invasive (intravascular—venous and arterial), minimally invasive (subcutaneous), and noninvasive (transdermal). Glucose is measured in interstitial fluid using the glucose oxidase method through fluorescence or measured intravenously through electrochemistry, fluorescence, mid-infrared spectroscopy, or electrochemical impedance spectroscopy (52). Sampling and measurement frequencies typically range from 1 to 15 min and most commonly are every 5 min. More than 15 CGM or semi-CGM devices have been described (53). For the purpose of ambulatory monitoring, a sensor is considered continuous if it provides a value at least every 15 min or more frequently (54).
There is consensus among experts and medical societies that compared with intermittent point-of-care (POC) capillary BG testing, CGM technology offers benefits in the prevention of severe hyperglycemia and hypoglycemia, allowing insulin dosage to be adjusted in a more accurate way (53,55) as well as decreasing the nursing workload related to ICU patients (55). Technological limitations that reduce the accuracy of subcutaneous CGM sensors include the need for regular calibration because of sensor drift, measurement lag, and substance interference (acetaminophen, maltose, ascorbic acid, dopamine, mannitol, heparin, uric acid, and salicylic acid) (25,56). There is lack of evidence on the accuracy of sensors during periods of arterial hypotension, hypothermia, or hypoxia, all common events in the ICU. In addition, intravascular CGMs carry risks of thrombus formation, catheter occlusion, and catheter-related infections (56). Despite these concerns, studies performed have shown acceptable device accuracy and no safety signals in either adult or pediatric populations (Tables 4 and 5) (57–89).
Table 4.
Clinical trials of adult CGM use in the ICU
| First author, year (ref.) | Population | Sample size | No. of sites | Type of CGM | Performance measurement | Comparator |
|---|---|---|---|---|---|---|
| Goldberg, 2004 (57) | ICU | 22 | 1 | CGMS Gold | Accuracy | Capillary BG monitor |
| Corstjens, 2006 (58) | ICU | 45 | 1 | CGMS Gold | Accuracy | Arterial by blood gas analyzer |
| De Block, 2006 (59) | MICU | 50 | 1 | GlucoDay | Reliability | Arterial |
| Yamashita, 2009 (60) | ICU | 50 | 1 | STG-22 | Accuracy | Arterial by blood gas analyzer |
| Holzinger, 2009 (61) | MICU | 50 | 1 | CGMS Gold | Accuracy and reliability | Arterial by blood gas analyzer |
| Logtenberg, 2009 (62) | Cardiac surgery | 30 | 1 | Paradigm REAL-Time | Accuracy and effect on glycemia with an alarm activation | Capillary, arterial, venous blood on a BG monitor |
| Rabiee, 2009 (63) | SICU/BICU | 19 | 1 | Dexcom | Accuracy and reliability | Capillary POC and lab |
| Holzinger, 2010 (64) | ICU | 24 | 1 | Guardian | Glycemic control, mortality | CGMS Gold (blinded) |
| Jacobs, 2010 (65) | ICU | 29 | 1 | Guardian RT | Accuracy | Capillary BG monitor |
| Brunner, 2011 (66) | ICU | 174 | 1 | CGMS Gold or Guardian | Accuracy | Arterial by blood gas analyzer |
| Lorencio, 2012 (67) | ICU | 41 | 1 | Guardian | Accuracy | Arterial by blood gas analyzer |
| Kopecký, 2013 (68) | ICU, cardiac surgery | 12 | 1 | Guardian REAL-Time | Accuracy and time in various ranges | Arterial by blood gas analyzer |
| Kopecký, 2013 (68) | ICU, cardiac surgery | 12 | 1 | Guardian | Glycemic control | Computer (eMPC) algorithm alone |
| Rodríguez-Quintanilla, 2013 (69) | CCU | 16 | 1 | Guardian RT | Time to normoglycemia | Capillary and venous blood |
| Ballesteros, 2015 (70) | ICU | 18 | 1 | Soft-Sensor | Accuracy | Capillary BG monitor |
| Boom, 2014 (71) | MICU/SICU | 78 | 1 | Navigator | Accuracy | Arterial by blood gas analyzer |
| Kosiborod, 2014 (72) | Cardiac ICU | 21 | 1 | Sentrino | Accuracy and reliability | Central venous POC or lab |
| Leelarantha, 2014 (73) | Neurosurgical ICU | 24 | 1 | Navigator | Accuracy | Standard IV insulin protocol |
| De Block, 2015 (74) | ICU | 35 | 2 | GlucoDay S | Time in various ranges, accuracy | Arterial by blood gas analyzer |
| Punke, 2015 (75) | SICU | 14 | 1 | Sentrino | Accuracy | Arterial by blood gas analyzer |
| van Hooijdonk, 2015 (76) | ICU | 50 | 1 | Sentrino | Accuracy and reliability | Arterial by blood gas analyzer |
| Gottschalk, 2016 (77) | Extracorporeal cardiac life support | 25 | 1 | Sentrino | Accuracy | Arterial by blood gas analyzer |
| Umbrello, 2014 (78) | MICU | 6 | 1 | OptiScanner 5000 | Glucose control | None |
| Sechterberger, 2015 (79) | Cardiac ICU | 8 | 1 | Navigator | Accuracy | Arterial by blood gas analyzer |
| Nohra, 2016 (80) | SICU | 23 | 1 | OptiScanner 5000 | Accuracy | Yellow Springs Instrument |
| Righy Shinotsuka, 2016 (81) | ICU | 88 | 1 | OptiScanner 5000 | Accuracy | Arterial by Yellow Springs Instrument |
| Wollersheim, 2016 (82) | MICU | 20 | 1 | Sentrino | Accuracy | Arterial or venous |
| Bochicchio, 2017 (83) | ICU | 243 | 4 | OptiScanner 5000 | Venous | Yellow Springs Instrument |
| Rijkenberg, 2017 (84) | ICU | 155 | 1 | FreeStyle Navigator | Accuracy | Arterial by blood gas analyzer |
| Schierenbeck, 2017 (85) | Cardiac ICU | 26 | 1 | FreeStyle Libre | Accuracy | Arterial by blood gas analyzer |
BICU, burn intensive care unit; CGMS, continuous glucose monitoring system; eMPC, enhanced model predictive control; IV, intravenous; MICU, medical intensive care unit; SICU, surgical intensive care unit.
Table 5.
Clinical trials of CGM in non-ICU settings
| First author, year (ref.) | Population | Sample size | No. of sites | Type of CGM | Performance measurement | Comparator |
|---|---|---|---|---|---|---|
| Burt, 2013 (86) | General ward | 26 | 1 | iPro | Accuracy | Capillary BG monitoring |
| Schaupp, 2015 (87) | General ward | 84 | 1 | iPro | Accuracy | Capillary BG monitoring |
| Gómez, 2015 (88) | General ward | 38 | 1 | iPro2 | Accuracy | Capillary BG monitoring |
| Gu, 2017 (89) | General ward | 81 | 8 | Sensor-augmented pump | Accuracy | MDI with blinded CGM |
Despite close to a billion dollars spent by more than 15 different companies in developing CGM, this technology remains largely experimental in the inpatient setting, with few FDA-approved devices. In Europe, there are currently four CGM systems approved for intravenous use in hospitals: 1) GlucoClear by Edwards Lifesciences (Irvine, CA), 2) Glysure System by Glysure (Abingdon, U.K.), 3) Eirus by Maquet Getinge Group (Rastatt, Germany), and 4) OptiScanner 5000 by OptiScan (Hayward, CA); in addition, there is one CGM system approved for subcutaneous use in hospitals: Sentrino by Medtronic (Northridge, CA). Two CGM systems are FDA-approved for use in U.S. hospitals: GlucoScout (International Biomedical, Austin, TX) and recently the OptiScanner 5000 (83,90).
CGM Use in the ICU
CGM systems have been evaluated for the management of hyperglycemia in ICU patients with and without diabetes over the past 10 years (Table 4). Most of these studies included a small sample size; outcomes were mostly accuracy of glucose control, and there were few with other clinical end points. To determine whether CGM could be an effective tool to titrate intravenous insulin infusion, Holzinger et al. (64) randomized 124 patients in a medical ICU (24 with diabetes, 100 without diabetes) to undergo intravenous insulin titration based on nonblinded Guardian CGM versus arterial BG with blinded CGM (CGM System Gold) (both manufactured by Medtronic MiniMed, Northridge, CA). Arterial glucose values were checked every 1–2 h in the control group. The primary end point was percentage of time within a target glucose level of 80–110 mg/dL (4.4–6.1 mmol/L). No difference was found in percentage of time within target glucose or mean interstitial glucose levels between treatment arms. The frequency of severe hypoglycemia (<40 mg/dL [2.2 mmol/L]) was lower in the nonblinded Guardian CGM group compared with the blinded CGM group (64).
Logtenberg et al. (62) randomized 31 cardiac surgery subjects to blinded versus nonblinded Paradigm CGM (Medtronic MiniMed) starting 1 day prior to surgery. No significant difference in preoperative mean interstitial glucose was found, but postoperative mean glucose improved with nonblinded CGM compared with blinded CGM; however, there was no significant difference in frequency of or time spent in hypoglycemia. Similarly, several additional studies comparing different blinded versus nonblinded CGM in patients after cardiac surgery or with acute coronary syndrome (68,69,71,74) confirmed the accuracy and reliability of CGM technology in titrating intravenous insulin therapy; however, none of them demonstrated significant improvement in mean glucose or in the frequency of hypoglycemia in the ICU. A recent systematic review of 37 studies, both randomized controlled trials and observational studies, concluded that in terms of efficacy, the use of subcutaneous CGM systems does not seem to improve the glycemic control of critically ill patients in a clinically significant manner.
Overall, the results of ICU studies indicate that the use of CGM combined with an appropriate insulin dosing protocol has the potential to improve glucose control in the ICU; however, the results have been conflicting. Some studies, but not others, have reported improvement in mean glucose values and reduction in hypoglycemia frequency with blinded CGM (55). Larger and well-designed multicenter studies are needed to convincingly demonstrate the safety and efficacy of CGM devices in reducing length of stay and improving clinical outcome before recommending their use in the ICU. A recent panel of experts concluded that use of CGM now might not be feasible for every ICU patient (91), but there are populations of high interest who may benefit from further study of CGM owing to their high risk for glucose variability and hypoglycemia. These populations include patients receiving intravenous insulin or high-dose glucocorticoids; those undergoing cardiac surgery, transplant, or traumatic or vascular brain surgery; those with end-stage renal or liver disease or hypoglycemia unawareness; and those in neonatal ICU (53,55).
CGM Use in Non-ICU Settings
Several studies have reported on the use of CGM in non-ICU settings in patients with T2D (Table 5). Burt et al. (86) reported on 26 adult patients with diabetes (23 with T2D and 3 with T1D) who were treated with basal-bolus insulin during hospitalization using blinded CGM System Gold in medical and surgical general wards. The mean daily glucose was similar between interstitial and capillary monitoring. Ten hypoglycemic episodes (<4 mmol/L) were detected during CGM; only one was detected by finger-prick BG level monitoring. Schaupp et al. (87) recruited 84 medicine patients with T2D and applied a blinded iPro2 CGM device (Medtronic MiniMed) for up to 21 days of hospital stay or until discharge. A remarkable consistency between CGM and BG measurements was reported without differences between groups, with 99% of data points in the clinically accurate or acceptable Clarke error grid zones, and the relative numbers of correctly identified episodes of glucose <3.9 and >13.9 mmol/L detected by CGM (sensitivity) were 47.3% and 81.5%, respectively. The number of hypoglycemic episodes (3.3 to <3.9 mmol/L) during nighttime detected by CGM (compared with values from the BG measurements) was 15-fold higher, and the number of episodes >13.9 mmol/L detected by CGM during nighttime was 12.5-fold higher (94) compared with capillary POC glucose testing in general medicine patients with T2D treated with a basal-bolus insulin regimen for ≥3 days. In addition, the use of CGM, compared with POC testing, uncovered a greater number of hypoglycemic events, and 60% of the episodes were during the night. Gu et al. (89) compared the accuracy and time required to reach predefined glycemic targets with sensor-augmented pump technology (Medtronic MiniMed Paradigm 722 system), which combines CSII and real-time CGM, versus MDI with blinded CGM (Medtronic MiniMed CGM System Gold) in 81 adult patients with T2D. Glycemic targets were defined as three preprandial measurements between 80 and 130 mg/dL (4.4–7.2 mmol/L) and three 2-h postprandial measurements between 80 and 180 mg/dL (4.4–10.0 mmol/L) within the same day. The authors reported that sensor-augmented pump technology resulted in a shorter time to reach the glucose targets (3.7 ± 1.1 days vs. 6.3 ± 3.1 days for MDI) and less hypoglycemia (sensor glucose <50 mg/dL [2.8 mmol/L]: 0.04% vs. 0.32%, respectively). In another study of 38 hospitalized patients with T2D treated with a basal-bolus insulin regimen, CGM use was compared with bedside POC glucose testing (88). There were no differences in mean daily glucose or premeal, fasting, or 2-h postprandial glucose levels between the two groups. However, CGM detected a higher number of hypoglycemic events compared with capillary glucose testing. About a third of the hypoglycemic episodes were asymptomatic and more than 50% of the events occurred between dinner and breakfast, suggesting that these episodes would be missed by standard glucose testing.
Previous studies in non-ICU settings have shown that the inpatient use of CGM is more effective in identifying trends toward hypoglycemia and hyperglycemia compared with standard POC glucose testing (86,92). However, these trials used blinded CGM, and therefore interventions to prevent impending hypoglycemia were not performed (86–88,93). Another limitation is that although glucose values are captured in the CGM device, results are not transmitted to the nursing station to allow providers to detect and treat impending hypoglycemia. In addition, hypoglycemia alarms are only visible and audible at the bedside; as a result, nurses need to frequently enter the patient’s room to monitor glucose values on the CGM receiver. To overcome these limitations, a recent promising pilot study reported on the feasibility of a continuous glucose telemetry system in high hypoglycemia–risk patients in non-ICU settings (94). Elderly patients receiving high-dose insulin treatment and with multiple comorbidities were included in this study. Data collected on a Dexcom G4 CGM sensor were transmitted via Bluetooth technology from the patient’s room wirelessly to an iPad located centrally at the nursing station on the same floor. By setting the lower glucose alarms at 85 mg/dL, the glucose telemetry system allowed the nursing staff to initiate preventive actions for impending hypoglycemia (94).
Artificial Pancreas: Closed-Loop Insulin Delivery System
Recent technological advances in CSII devices, CGM systems, and insulin delivery algorithms have resulted in the development of artificial pancreas for inpatient care (95,96). An artificial pancreas, or a closed-loop system, combines a real-time glucose-sensing component, an insulin delivery device (pump), and a computer that calculates the amount of insulin needed in response to the BG concentration (95). During the past decade, a variety of closed-loop systems have been explored in various groups of critically ill patients (97,98), during the perioperative period (99), and in insulin-treated patients with T2D (100). These studies reported that the closed-loop technology is safe and effective in improving glycemic control and proportion of time spent in the target glucose concentration range, but they found no significant improvement in mean glucose concentration or in the frequency of hypoglycemic events compared with multidose insulin regimens. Despite this evidence supporting the efficacy and feasibility of closed-loop use, there are several limitations that need to be addressed to support wider adoption in the hospital setting. The need for intravascular access for intravenous closed-loop insulin systems limits their use in noncritical-care general ward settings. More importantly, no previous studies have shown that use of closed-loop systems is associated with improved clinical outcomes compared with intermittent monitoring and conventional insulin treatment and/or with favorable cost-benefit ratio.
What Lies Ahead in Diabetes Technology?
Diabetes management devices including insulin pumps and CGM have gained wide acceptance among physicians and ambulatory patients with T1D, and their use has been associated with improved glycemic control and reductions in hypoglycemia. The Endocrine Society (101), the American Association of Clinical Endocrinologists (102), and the Diabetes Technology Society (53) support the inpatient use of CSII in selected patients, such as those with appropriate insulin pump and diabetes self-management skills, with noncritical illness, without mental status changes, and with the prompt involvement of inpatient diabetes specialists. The consensus among diabetologists is to allow the patient to continue to self-manage their diabetes using the pump. If a patient is unable to manage their pump for whatever reason or a hospital lacks specialist consultation, then the pump should be removed and conventional insulin management should be initiated. CSII can be restarted once the patient has recovered.
Despite broad-based evidence supporting the use of CGM devices as a mean of facilitating glucose control in hospitalized patients and decreasing nursing workload, the technology remains largely investigational. Clinical guidelines have advised against the hospital use of CGM because of the lack of safety and efficacy outcome studies (53,101,102); however, they support continuation of outpatient CGM in the hospital under specific circumstances if proper institutional procedures and guidelines are developed (5,53). In recent years, improvement in the accuracy of CGM sensors has resulted in a reduced need for frequent calibration, or any calibration (103), which is an attractive feature in the hospital. A pragmatic evaluation of CGM proving accuracy and clinical effectiveness is needed and may facilitate more widespread adoption of this technology in the hospital setting.
Because an increasing number of people with diabetes are using insulin pumps and CGM, it is inevitable that health care professionals working in hospitals will have to care for patients using pumps and CGM devices. Technology for management of diabetes in the hospital is improving and is expected to significantly reduce the added burden and risk of diabetes for hospitalized patients. In the near term, the availability of accurate CGM systems combined with automatic insulin dosing systems using software algorithms will facilitate glycemic control and reduction of hypoglycemia and hyperglycemia in critically and noncritically ill patients with T1D and T2D (100). As artificial intelligence becomes more established, the dosing algorithms for insulin delivery in hospitalized patients will become individualized for closed-loop control of glycemia (104).
Article Information
Acknowledgments. The authors would like to thank Robert Vigersky, MD (Medtronic Diabetes, Uniformed Services University of the Health Sciences, and Diabetes Institute of Walter Reed National Military Medical Center), and Francisco Pasquel, MD (Division of Endocrinology, Emory University), for their helpful comments and Annamarie Sucher (Burlingame, CA) for her expert editorial assistance.
Funding. G.E.U. is partly supported by research grants from the U.S. Public Health Service through the National Institutes of Health National Center for Advancing Translational Sciences Clinical and Translational Science Award Program (grant UL1-TR002378) and National Center for Research Resources (grant 1P30DK111024-01).
Duality of Interest. G.E.U. has received unrestricted research support for inpatient studies (to Emory University) from Merck, Novo Nordisk, AstraZeneca, Boehringer Ingelheim, and Sanofi. G.E.U. has received honoraria for advisory board/consultant services from Sanofi and Intarcia Pharmaceuticals. D.C.K. has received honoraria for advisory board/consultant services from Ascensia, EOFlow, Intarcia, LifeCare, Novo Nordisk, Onduo, and Voluntis.
Author Contributions. G.E.U. and D.C.K. reviewed the literature and collected relevant information. G.E.U. wrote the first draft of the manuscript. D.C.K. reviewed and edited the manuscript and approved the final version.
Prior Presentation. Parts of this article were presented at the 78th Scientific Sessions of the American Diabetes Association, Orlando, FL, 23 June 2018.
Footnotes
References
- 1.Centers for Disease Control and Prevention National Diabetes Statistics Report, 2017. Atlanta, GA, Centers for Disease Control and Prevention, U.S. Department of Health and Human Services, 2017 [Google Scholar]
- 2.Donnan PT, Leese GP, Morris AD; Diabetes Audit and Research in Tayside, Scotland/Medicine Monitoring Unit Collaboration . Hospitalizations for people with type 1 and type 2 diabetes compared with the nondiabetic population of Tayside, Scotland: a retrospective cohort study of resource use. Diabetes Care 2000;23:1774–1779 [DOI] [PubMed] [Google Scholar]
- 3.American Diabetes Association Economic costs of diabetes in the U.S. in 2012 [published correction appears in Diabetes Care 2013;36:1797]. Diabetes Care 2013;36:1033–1046 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Moghissi ES, Korytkowski MT, DiNardo M, et al.; American Association of Clinical Endocrinologists; American Diabetes Association . American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Endocr Pract 2009;15:353–369 [DOI] [PubMed] [Google Scholar]
- 5.Umpierrez GE, Hellman R, Korytkowski MT, et al.; Endocrine Society . Management of hyperglycemia in hospitalized patients in non-critical care setting: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2012;97:16–38 [DOI] [PubMed] [Google Scholar]
- 6.Murad MH, Coburn JA, Coto-Yglesias F, et al. Glycemic control in non-critically ill hospitalized patients: a systematic review and meta-analysis. J Clin Endocrinol Metab 2012;97:49–58 [DOI] [PubMed] [Google Scholar]
- 7.Umpierrez GE, Smiley D, Jacobs S, et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes undergoing general surgery (RABBIT 2 surgery). Diabetes Care 2011;34:256–261 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wexler DJ, Meigs JB, Cagliero E, Nathan DM, Grant RW. Prevalence of hyper- and hypoglycemia among inpatients with diabetes: a national survey of 44 U.S. hospitals. Diabetes Care 2007;30:367–369 [DOI] [PubMed] [Google Scholar]
- 9.Umpierrez GE. Basal versus sliding-scale regular insulin in hospitalized patients with hyperglycemia during enteral nutrition therapy. Diabetes Care 2009;32:751–753 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Umpierrez GE, Smiley D, Hermayer K, et al. Randomized study comparing a basal-bolus with a basal plus correction insulin regimen for the hospital management of medical and surgical patients with type 2 diabetes: Basal Plus trial. Diabetes Care 2013;36:2169–2174 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Finfer S, Liu B, Chittock DR, et al.; NICE-SUGAR Study Investigators . Hypoglycemia and risk of death in critically ill patients. N Engl J Med 2012;367:1108–1118 [DOI] [PubMed] [Google Scholar]
- 12.Gamble JM, Eurich DT, Marrie TJ, Majumdar SR. Admission hypoglycemia and increased mortality in patients hospitalized with pneumonia. Am J Med 2010;123:556.e11–556.e16 [DOI] [PubMed] [Google Scholar]
- 13.Umpierrez GE, Isaacs SD, Bazargan N, You X, Thaler LM, Kitabchi AE. Hyperglycemia: an independent marker of in-hospital mortality in patients with undiagnosed diabetes. J Clin Endocrinol Metab 2002;87:978–982 [DOI] [PubMed] [Google Scholar]
- 14.Chiang JL, Kirkman MS, Laffel LM, Peters AL; Type 1 Diabetes Sourcebook Authors . Type 1 diabetes through the life span: a position statement of the American Diabetes Association. Diabetes Care 2014;37:2034–2054 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Maahs DM, West NA, Lawrence JM, Mayer-Davis EJ. Epidemiology of type 1 diabetes. Endocrinol Metab Clin North Am 2010;39:481–497 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.American Diabetes Association Statistics about diabetes: overall numbers, diabetes and prediabetes [Internet]. Available from http://www.diabetes.org/diabetes-basics/statistics/. Accessed 22 March 2018
- 17.Sayers A, Thayer D, Harvey JN, et al. Evidence for a persistent, major excess in all cause admissions to hospital in children with type-1 diabetes: results from a large Welsh national matched community cohort study. BMJ Open 2015;5:e005644. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mendez CE, Umpierrez GE. Management of type 1 diabetes in the hospital setting. Curr Diab Rep 2017;17:98. [DOI] [PubMed] [Google Scholar]
- 19.Icks A, Rosenbauer J, Holl RW, Grabert M, Rathmann W, Giani G; German Working Group for Pediatric Diabetology . Hospitalization among diabetic children and adolescents and the general population in Germany. Diabetes Care 2001;24:435–440 [DOI] [PubMed] [Google Scholar]
- 20.Tomlin AM, Tilyard MW, Dovey SM, Dawson AG. Hospital admissions in diabetic and non-diabetic patients: a case-control study. Diabetes Res Clin Pract 2006;73:260–267 [DOI] [PubMed] [Google Scholar]
- 21.Viens NA, Hug KT, Marchant MH, Cook C, Vail TP, Bolognesi MP. Role of diabetes type in perioperative outcomes after hip and knee arthroplasty in the United States. J Surg Orthop Adv 2012;21:253–260 [DOI] [PubMed] [Google Scholar]
- 22.Robertshaw HJ, Hall GM. Diabetes mellitus: anaesthetic management. Anaesthesia 2006;61:1187–1190 [DOI] [PubMed] [Google Scholar]
- 23.Cryer PE. Hypoglycemia in type 1 diabetes mellitus. Endocrinol Metab Clin North Am 2010;39:641–654 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Heinemann L, Fleming GA, Petrie JR, Holl RW, Bergenstal RM, Peters AL. Insulin pump risks and benefits: a clinical appraisal of pump safety standards, adverse event reporting, and research needs: a joint statement of the European Association for the Study of Diabetes and the American Diabetes Association Diabetes Technology Working Group. Diabetes Care 2015;38:716–722 [DOI] [PubMed] [Google Scholar]
- 25.Lansang MC, Modic MB, Sauvey R, et al. Approach to the adult hospitalized patient on an insulin pump. J Hosp Med 2013;8:721–727 [DOI] [PubMed] [Google Scholar]
- 26.Beck RW, Tamborlane WV, Bergenstal RM, Miller KM, DuBose SN, Hall CA; T1D Exchange Clinic Network . The T1D Exchange clinic registry. J Clin Endocrinol Metab 2012;97:4383–4389 [DOI] [PubMed] [Google Scholar]
- 27.Blackman SM, Raghinaru D, Adi S, et al. Insulin pump use in young children in the T1D Exchange clinic registry is associated with lower hemoglobin A1c levels than injection therapy. Pediatr Diabetes 2014;15:564–572 [DOI] [PubMed] [Google Scholar]
- 28.Orchard TJ, Nathan DM, Zinman B, et al.; Writing Group for the DCCT/EDIC Research Group . Association between 7 years of intensive treatment of type 1 diabetes and long-term mortality. JAMA 2015;313:45–53 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Cook CB, McNaughton DA, Braddy CM, et al. Management of inpatient hyperglycemia: assessing perceptions and barriers to care among resident physicians. Endocr Pract 2007;13:117–124 [DOI] [PubMed] [Google Scholar]
- 30.Houlden RL, Moore S. In-hospital management of adults using insulin pump therapy. Can J Diabetes 2014;38:126–133 [DOI] [PubMed] [Google Scholar]
- 31.Noschese ML, DiNardo MM, Donihi AC, et al. Patient outcomes after implementation of a protocol for inpatient insulin pump therapy. Endocr Pract 2009;15:415–424 [DOI] [PubMed] [Google Scholar]
- 32.Cook CB, Beer KA, Seifert KM, Boyle ME, Mackey PA, Castro JC. Transitioning insulin pump therapy from the outpatient to the inpatient setting: a review of 6 years’ experience with 253 cases. J Diabetes Sci Technol 2012;6:995–1002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Kannan S, Satra A, Calogeras E, Lock P, Lansang MC. Insulin pump patient characteristics and glucose control in the hospitalized setting. J Diabetes Sci Technol 2014;8:473–478 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Bailon RM, Partlow BJ, Miller-Cage V, et al. Continuous subcutaneous insulin infusion (insulin pump) therapy can be safely used in the hospital in select patients. Endocr Pract 2009;15:24–29 [DOI] [PubMed] [Google Scholar]
- 35.American Diabetes Association 14. Diabetes care in the hospital: Standards of Medical Care in Diabetes—2018. Diabetes Care 2018;41(Suppl. 1):S144–S151 [DOI] [PubMed] [Google Scholar]
- 36.Funnell MM, Brown TL, Childs BP, et al. National Standards for Diabetes Self-Management Education. Diabetes Care 2011;34(Suppl. 1):S89–S96 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Grunberger G, Bailey TS, Cohen AJ, et al.; AACE Insulin Pump Management Task Force . Statement by the American Association of Clinical Endocrinologists Consensus Panel on insulin pump management. Endocr Pract 2010;16:746–762 [DOI] [PubMed] [Google Scholar]
- 38.Yogi-Morren D, Lansang MC. Management of patients with type 1 diabetes in the hospital. Curr Diab Rep 2014;14:458. [DOI] [PubMed] [Google Scholar]
- 39.Moghissi ES, Korytkowski MT, DiNardo M, et al.; American Association of Clinical Endocrinologists; American Diabetes Association . American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Diabetes Care 2009;32:1119–1131 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Bode BW. Use of rapid-acting insulin analogues in the treatment of patients with type 1 and type 2 diabetes mellitus: insulin pump therapy versus multiple daily injections. Clin Ther 2007;29(Suppl. D):S135–S144 [DOI] [PubMed] [Google Scholar]
- 41.Klonoff DC, Freckmann G, Heinemann L. Insulin pump occlusions: for patients who have been around the (infusion) block. J Diabetes Sci Technol 2017;11:451–454 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Sobel SI, Augustine M, Donihi AC, Reider J, Forte P, Korytkowski M. Safety and efficacy of a peri-operative protocol for patients with diabetes treated with continuous subcutaneous insulin infusion who are admitted for same-day surgery. Endocr Pract 2015;21:1269–1276 [DOI] [PubMed] [Google Scholar]
- 43.Corney SM, Dukatz T, Rosenblatt S, et al. Comparison of insulin pump therapy (continuous subcutaneous insulin infusion) to alternative methods for perioperative glycemic management in patients with planned postoperative admissions. J Diabetes Sci Technol 2012;6:1003–1015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.García-Patterson A, Gich I, Amini SB, Catalano PM, de Leiva A, Corcoy R. Insulin requirements throughout pregnancy in women with type 1 diabetes mellitus: three changes of direction. Diabetologia 2010;53:446–451 [DOI] [PubMed] [Google Scholar]
- 45.Roeder HA, Moore TR, Ramos GA. Insulin pump dosing across gestation in women with well-controlled type 1 diabetes mellitus. Am J Obstet Gynecol 2012;207:324.e1–324.e5 [DOI] [PubMed] [Google Scholar]
- 46.Farrar D, Tuffnell DJ, West J, West HM. Continuous subcutaneous insulin infusion versus multiple daily injections of insulin for pregnant women with diabetes. Cochrane Database Syst Rev 2016;(6):CD005542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Bruttomesso D, Bonomo M, Costa S, et al.; Italian Group for Continuous Subcutaneous Insulin Infusion in Pregnancy . Type 1 diabetes control and pregnancy outcomes in women treated with continuous subcutaneous insulin infusion (CSII) or with insulin glargine and multiple daily injections of rapid-acting insulin analogues (glargine-MDI). Diabetes Metab 2011;37:426–431 [DOI] [PubMed] [Google Scholar]
- 48.Wender-Ozegowska E, Zawiejska A, Ozegowska K, et al. Multiple daily injections of insulin versus continuous subcutaneous insulin infusion for pregnant women with type 1 diabetes. Aust N Z J Obstet Gynaecol 2013;53:130–135 [DOI] [PubMed] [Google Scholar]
- 49.Feldman AZ, Brown FM. Management of type 1 diabetes in pregnancy. Curr Diab Rep 2016;16:76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Clarke SF, Foster JR. A history of blood glucose meters and their role in self-monitoring of diabetes mellitus. Br J Biomed Sci 2012;69:83–93 [PubMed] [Google Scholar]
- 51.Skyler JS. CGM—a technology in evolution. Diabetes Technol Ther 2009;11:63–64 [DOI] [PubMed] [Google Scholar]
- 52.Adamson TL, Eusebio FA, Cook CB, LaBelle JT. The promise of electrochemical impedance spectroscopy as novel technology for the management of patients with diabetes mellitus. Analyst (Lond) 2012;137:4179–4187 [DOI] [PubMed] [Google Scholar]
- 53.Wallia A, Umpierrez GE, Rushakoff RJ, et al.; DTS Continuous Glucose Monitoring in the Hospital Panel . Consensus statement on inpatient use of continuous glucose monitoring. J Diabetes Sci Technol 2017;11:1036–1044 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Clinical and Laboratory and Standards Institute (CLSI) Performance Metrics for Continuous Interstitial Glucose Monitoring: Approved Guideline. Wayne, PA, Clinical and Laboratory Standards Institute, 2008. (CLSI document POCT05-A) [Google Scholar]
- 55.Krinsley JS, Chase JG, Gunst J, et al. Continuous glucose monitoring in the ICU: clinical considerations and consensus. Crit Care 2017;21:197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Klonoff DC, Buckingham B, Christiansen JS, et al.; Endocrine Society . Continuous glucose monitoring: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2011;96:2968–2979 [DOI] [PubMed] [Google Scholar]
- 57.Goldberg PA, Siegel MD, Russell RR, et al. Experience with the continuous glucose monitoring system in a medical intensive care unit. Diabetes Technol Ther 2004;6:339–347 [DOI] [PubMed] [Google Scholar]
- 58.Corstjens AM, Ligtenberg JJ, van der Horst IC, et al. Accuracy and feasibility of point-of-care and continuous blood glucose analysis in critically ill ICU patients. Crit Care 2006;10:R135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.De Block C, Manuel-Y-Keenoy B, Van Gaal L, Rogiers P. Intensive insulin therapy in the intensive care unit: assessment by continuous glucose monitoring. Diabetes Care 2006;29:1750–1756 [DOI] [PubMed] [Google Scholar]
- 60.Yamashita K, Okabayashi T, Yokoyama T, et al. Accuracy and reliability of continuous blood glucose monitor in post-surgical patients. Acta Anaesthesiol Scand 2009;53:66–71 [DOI] [PubMed] [Google Scholar]
- 61.Holzinger U, Warszawska J, Kitzberger R, Herkner H, Metnitz PG, Madl C. Impact of shock requiring norepinephrine on the accuracy and reliability of subcutaneous continuous glucose monitoring. Intensive Care Med 2009;35:1383–1389 [DOI] [PubMed] [Google Scholar]
- 62.Logtenberg SJ, Kleefstra N, Snellen FT, et al. Pre- and postoperative accuracy and safety of a real-time continuous glucose monitoring system in cardiac surgical patients: a randomized pilot study. Diabetes Technol Ther 2009;11:31–37 [DOI] [PubMed] [Google Scholar]
- 63.Rabiee A, Andreasik V, Abu-Hamdah R, et al. Numerical and clinical accuracy of a continuous glucose monitoring system during intravenous insulin therapy in the surgical and burn intensive care units. J Diabetes Sci Technol 2009;3:951–959 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Holzinger U, Warszawska J, Kitzberger R, et al. Real-time continuous glucose monitoring in critically ill patients: a prospective randomized trial. Diabetes Care 2010;33:467–472 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Jacobs B, Phan K, Bertheau L, Dogbey G, Schwartz F, Shubrook J. Continuous glucose monitoring system in a rural intensive care unit: a pilot study evaluating accuracy and acceptance. J Diabetes Sci Technol 2010;4:636–644 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Brunner R, Kitzberger R, Miehsler W, Herkner H, Madl C, Holzinger U. Accuracy and reliability of a subcutaneous continuous glucose-monitoring system in critically ill patients. Crit Care Med 2011;39:659–664 [DOI] [PubMed] [Google Scholar]
- 67.Lorencio C, Leal Y, Bonet A, et al. Real-time continuous glucose monitoring in an intensive care unit: better accuracy in patients with septic shock. Diabetes Technol Ther 2012;14:568–575 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Kopecký P, Mráz M, Bláha J, et al. The use of continuous glucose monitoring combined with computer-based eMPC algorithm for tight glucose control in cardiosurgical ICU. BioMed Res Int 2013;2013:186439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Rodríguez-Quintanilla KA, Lavalle-González FJ, Mancillas-Adame LG, Zapata-Garrido AJ, Villarreal-Pérez JZ, Tamez-Pérez HE. Continuous glucose monitoring in acute coronary syndrome. Arch Cardiol Mex 2013;83:237–243 [DOI] [PubMed] [Google Scholar]
- 70.Ballesteros D, Martínez Ó, Blancas Gómez-Casero R, et al. Continuous tissue glucose monitoring correlates with measurement of intermittent capillary glucose in patients with distributive shock. Med Intensiva 2015;39:405–411 [DOI] [PubMed] [Google Scholar]
- 71.Boom DT, Sechterberger MK, Rijkenberg S, et al. Insulin treatment guided by subcutaneous continuous glucose monitoring compared to frequent point-of-care measurement in critically ill patients: a randomized controlled trial. Crit Care 2014;18:453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Kosiborod M, Gottlieb RK, Sekella JA, et al. Performance of the Medtronic Sentrino continuous glucose management (CGM) system in the cardiac intensive care unit. BMJ Open Diabetes Res Care 2014;2:e000037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Leelarathna L, English SW, Thabit H, et al. Accuracy of subcutaneous continuous glucose monitoring in critically ill adults: improved sensor performance with enhanced calibrations. Diabetes Technol Ther 2014;16:97–101 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.De Block CE, Gios J, Verheyen N, et al. Randomized evaluation of glycemic control in the medical intensive care unit using real-time continuous glucose monitoring (REGIMEN trial). Diabetes Technol Ther 2015;17:889–898 [DOI] [PubMed] [Google Scholar]
- 75.Punke MA, Decker C, Wodack K, Reuter DA, Kluge S. Continuous glucose monitoring on the ICU using a subcutaneous sensor. Med Klin Intensivmed Notf Med 2015;110:360–363 [DOI] [PubMed] [Google Scholar]
- 76.van Hooijdonk RT, Leopold JH, Winters T, et al. Point accuracy and reliability of an interstitial continuous glucose-monitoring device in critically ill patients: a prospective study. Crit Care 2015;19:34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Gottschalk A, Welp HA, Leser L, Lanckohr C, Wempe C, Ellger B. Continuous glucose monitoring in patients undergoing extracorporeal ventricular assist therapy. PLoS One 2016;11:e0148778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Umbrello M, Salice V, Spanu P, et al. Performance assessment of a glucose control protocol in septic patients with an automated intermittent plasma glucose monitoring device. Clin Nutr 2014;33:867–871 [DOI] [PubMed] [Google Scholar]
- 79.Sechterberger MK, van der Voort PH, Strasma PJ, DeVries JH. Accuracy of intra-arterial and subcutaneous continuous glucose monitoring in postoperative cardiac surgery patients in the ICU. J Diabetes Sci Technol 2015;9:663–667 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Nohra E, Buckman S, Bochicchio K, et al. Results of a near continuous glucose monitoring technology in surgical intensive care and trauma. Contemp Clin Trials 2016;50:1–4 [DOI] [PubMed] [Google Scholar]
- 81.Righy Shinotsuka C, Brasseur A, Fagnoul D, So T, Vincent JL, Preiser JC. Manual versus Automated moNitoring Accuracy of GlucosE II (MANAGE II). Crit Care 2016;20:380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Wollersheim T, Engelhardt LJ, Pachulla J, et al. Accuracy, reliability, feasibility and nurse acceptance of a subcutaneous continuous glucose management system in critically ill patients: a prospective clinical trial. Ann Intensive Care 2016;6:70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Bochicchio GV, Nasraway S, Moore L, Furnary A, Nohra E, Bochicchio K. Results of a multicenter prospective pivotal trial of the first inline continuous glucose monitor in critically ill patients. J Trauma Acute Care Surg 2017;82:1049–1054 [DOI] [PubMed] [Google Scholar]
- 84.Rijkenberg S, van Steen SC, DeVries JH, van der Voort PHJ. Accuracy and reliability of a subcutaneous continuous glucose monitoring device in critically ill patients. J Clin Monit Comput. 7 December 2017 [Epub ahead of print]. DOI: 10.1007/s10877-017-0086-z [DOI] [PubMed] [Google Scholar]
- 85.Schierenbeck F, Franco-Cereceda A, Liska J. Accuracy of 2 different continuous glucose monitoring systems in patients undergoing cardiac surgery. J Diabetes Sci Technol 2017;11:108–116 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Burt MG, Roberts GW, Aguilar-Loza NR, Stranks SN. Brief report: comparison of continuous glucose monitoring and finger-prick blood glucose levels in hospitalized patients administered basal-bolus insulin. Diabetes Technol Ther 2013;15:241–245 [DOI] [PubMed] [Google Scholar]
- 87.Schaupp L, Donsa K, Neubauer KM, et al. Taking a closer look—continuous glucose monitoring in non-critically ill hospitalized patients with type 2 diabetes mellitus under basal-bolus insulin therapy. Diabetes Technol Ther 2015;17:611–618 [DOI] [PubMed] [Google Scholar]
- 88.Gómez AM, Umpierrez GE, Muñoz OM, et al. Continuous glucose monitoring versus capillary point-of-care testing for inpatient glycemic control in type 2 diabetes patients hospitalized in the general ward and treated with a basal bolus insulin regimen. J Diabetes Sci Technol 2015;10:325–329 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Gu W, Liu Y, Chen Y, et al. Multicentre randomized controlled trial with sensor-augmented pump vs multiple daily injections in hospitalized patients with type 2 diabetes in China: time to reach target glucose. Diabetes Metab 2017;43:359–363 [DOI] [PubMed] [Google Scholar]
- 90.OptiScan Biomedical Corporation OptiScan Biomedical’s OptiScanner® 5000 receives 510(k) clearance from US Food and Drug Administration for the first inline continuous glucose monitor in the SICU [article online]. PR Newswire, 18 October 2017. Available from https://www.prnewswire.com/news-releases/optiscan-biomedicals-optiscanner-5000-receives-510k-clearance-from-us-food-and-drug-administration-for-the-first-inline-continuous-glucose-monitor-in-the-sicu-300538510.html. Accessed 17 October 2017
- 91.Wallia A, Umpierrez GE, Nasraway SA, Klonoff DC; PRIDE Investigators . Round table discussion on inpatient use of continuous glucose monitoring at the International Hospital Diabetes Meeting. J Diabetes Sci Technol 2016;10:1174–1181 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Gomez AM, Umpierrez GE. Continuous glucose monitoring in insulin-treated patients in non-ICU settings. J Diabetes Sci Technol 2014;8:930–936 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Levitt DL, Silver KD, Spanakis EK. Inpatient continuous glucose monitoring and glycemic outcomes. J Diabetes Sci Technol 2017;11:1028–1035 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Spanakis EK, Levitt DL, Siddiqui T, et al. The effect of continuous glucose monitoring in preventing inpatient hypoglycemia in general wards: the glucose telemetry system. J Diabetes Sci Technol 2018;12:20–25 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Peyser T, Dassau E, Breton M, Skyler JS. The artificial pancreas: current status and future prospects in the management of diabetes. Ann N Y Acad Sci 2014;1311:102–123 [DOI] [PubMed] [Google Scholar]
- 96.Hanazaki K, Munekage M, Kitagawa H, et al. Current topics in glycemic control by wearable artificial pancreas or bedside artificial pancreas with closed-loop system. J Artif Organs 2016;19:209–218 [DOI] [PubMed] [Google Scholar]
- 97.Mibu K, Yatabe T, Hanazaki K. Blood glucose control using an artificial pancreas reduces the workload of ICU nurses. J Artif Organs 2012;15:71–76 [DOI] [PubMed] [Google Scholar]
- 98.Okabayashi T, Shima Y, Sumiyoshi T, et al. Intensive versus intermediate glucose control in surgical intensive care unit patients. Diabetes Care 2014;37:1516–1524 [DOI] [PubMed] [Google Scholar]
- 99.Namikawa T, Munekage M, Kitagawa H, et al. Comparison between a novel and conventional artificial pancreas for perioperative glycemic control using a closed-loop system. J Artif Organs 2017;20:84–90 [DOI] [PubMed] [Google Scholar]
- 100.Thabit H, Hovorka R. Bridging technology and clinical practice: innovating inpatient hyperglycaemia management in non-critical care settings. Diabet Med 2018;35:460–471 [DOI] [PubMed] [Google Scholar]
- 101.Peters AL, Ahmann AJ, Battelino T, et al. Diabetes technology—continuous subcutaneous insulin infusion therapy and continuous glucose monitoring in adults: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2016;101:3922–3937 [DOI] [PubMed] [Google Scholar]
- 102.Handelsman Y, Bloomgarden ZT, Grunberger G, et al. American Association of Clinical Endocrinologists and American College of Endocrinology – clinical practice guidelines for developing a diabetes mellitus comprehensive care plan – 2015. Endocr Pract 2015;21(Suppl. 1):1–87 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Rodbard D. Continuous glucose monitoring: a review of recent studies demonstrating improved glycemic outcomes. Diabetes Technol Ther 2017;19:S25–S37 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.DeJournett L, DeJournett J. In silico testing of an artificial-intelligence-based artificial pancreas designed for use in the intensive care unit setting. J Diabetes Sci Technol 2016;10:1360–1371 [DOI] [PMC free article] [PubMed] [Google Scholar]