

Abstract
Objective
To describe the characteristics of spinal cord injury (SCI) individuals in Shanghai and examine their treatment and rehabilitation for traumatic and complete SCI individuals.
Design
Community-based secondary data analyses.
Setting
Shanghai, China.
Methods
We analyzed gender, age at injury, complications, disturbances of function, treatment, etiology, and severity of injury of SCI individuals that enrolled in “halfway houses”, government-supported community co-op centers. Bivariate statistical analyses were conducted to examine the factors associated with complete and traumatic SCI.
Results
We analyzed 808 SCI individuals who participated in halfway houses in Shanghai during 2009–2015. The male-to-female ratio was 2.1:1. The proportion of middle or elder age groups at injury (age 46 to 60 and age 61 or over) showed a rising trend from 1970 to 2015. The leading causes of SCIs in Shanghai were traumatic injuries (58%), followed by disease (29.5%). The proportion of traumatic injuries decreased over time, while the proportion of non-traumatic injuries rose significantly. A majority of traumatic injury individuals were aged between 16–45.
Conclusion
The middle or elder age groups at injury among SCI individuals increased continuously from 1970 to 2015. The principal causes of injury in Shanghai were traumatic injuries and disease-related injuries. Men had a higher prevalence of traumatic SCI in Shanghai. Preventive measures should focus on male and middle-aged adults. As a fast-aging society in Shanghai, more effective prevention, medical care, and rehabilitation schemes should be implemented for aging SCI individuals.
Keywords: Spinal cord injury, Epidemiology, Halfway houses, Community, China
Introduction
In a spinal cord injury (SCI), the structures and function of the spinal cord are damaged by trauma, inflammation, tumors, or other causes, resulting in impairment of motor, sensory and autonomic function below the level of injury.1,2 Since no effective treatment is available to cure SCI, patients live with the complications and bear the financial burdens for their lifelong treatment.3 The etiology of injury can be traumatic or non-traumatic, though trauma is a more frequent cause.4 The incidence of traumatic SCI varies across countries and regions, ranging from 2.1 to 195.4 individuals per million per year,5–8 with Asian countries reporting 12.1–61.6 individuals per million.9 To our knowledge, a nationwide database of SCIs has not been set up in mainland China, so existing studies in the literature have all been hospital-based,10 and most of these studies have focused on traumatic SCI.11–13 It is estimated that more than a million SCI individuals lived in China in 2012, with 10,000 to 60,000 new SCI individuals being added every year.14,15
Shanghai is one of the most developed cities in China, with a population of 24.26 million in 2014.16 An estimated population of 10,000 or more SCI patients are living in Shanghai, with 100–600 new patients each year. But little research has been done regarding these SCI patients in Shanghai. The few available reports are all based on one or a few hospitals in the city. For example, Hu et al.17 reported the incidence of SCI in Songjiang, a suburban district in Shanghai, with an incidence of 13.7 per million in the period of 1983–1991, and Pan et al.18 reported that in another district, Pudong, the incidence was 25 per million in the period of 2005–2007. Cheng et al.19 described the epidemiologic features and effects of surgical treatment of SCI patients in one Shanghai hospital. All of these studies had two limitations: First, they were hospital-based in a single district of Shanghai; second, the study period was limited.
Rehabilitation enables people with SCI to return home to their families and communities. However, owing to limited resources in China, such as rehabilitation professionals, only a small proportion of SCI individuals can receive routine rehabilitation immediately after their acute care hospitalization.20 In 2009, the China Association of Persons with Physical Disability, a government-supported national organization, started community co-op centers called “halfway houses” for SCI individuals in four provinces: Shanghai, Zhejiang, Henan, and Guangxi.21 Its main goal was to help SCI individuals to return to their communities and receive education on how to improve their daily-living capabilities from rehabilitation professionals, thus preventing the complications and aggravations of disability. In Shanghai, halfway houses had been set up in all 17 districts by the end of 2012, which makes Shanghai one of the first few cities in China to achieve city-wide coverage. Shanghai’s policy on halfway houses was adopted by the China Association of Persons with Physical Disability as the national guideline.22
This study aimed to answer three questions based on the data collected from halfway houses in Shanghai: (1) What are the socio-demographic and disease characteristics of SCI individuals from halfway houses in Shanghai, such as age, etiology of injury, and complications? (2) Which factors are associated with traumatic injury? (3) Which factors are associated with SCI individuals with complete injury? The results of this study will serve as a baseline to develop SCI prevention measures and to develop effective community-based interventions to improve the welfare of SCI patients in Shanghai
Materials and methods
Halfway houses and SCI patients
Halfway houses in Shanghai are non-residential day treatment facilities in the community. They provide persons with SCI with an opportunity to engage in activity such as workshops with healthcare professionals, receiving mutual emotional support, practicing daily-living skills and rehabilitation training methods from peer mentors, going on outings and other co-op activities. At home, they also can exchange information or ask for help via social media within the larger group of halfway house members. They can also receive suggestions and help from rehabilitation doctors or nurses who are volunteers on the spot or online and have been referred by halfway houses.
Furthermore, some individuals can also be referred by halfway houses to receive systematic health education and functional training in Shanghai Sunshine Rehabilitation Center, the largest and comprehensive public rehabilitation center in Shanghai for disabled patients (including SCI persons) after hospital discharge. To be enrolled in halfway houses, social workers visited SCI patients at their homes to introduce the idea of the halfway houses and encourage participation. SCI patients then visited the houses to be enrolled. During their enrollment process, each member filled out a paper form that recorded basic personal and injury information, which was later centrally archived in the Management Information System of the Shanghai Disabled Persons’ Federation. In 2015, there were 21 halfway houses in Shanghai, with each center having 10 to 96 members. This study analyzed the data extracted from the Management Information System of the Shanghai Disabled Persons’ Federation. We included all 808 individuals with traumatic and non-traumatic SCI who participated in halfway houses in Shanghai between 2009 and 2015.
Data and measurement
The data included the individuals’ birth date, gender, year enrolled in the halfway house, time of injury, cause of injury, severity of injury, and treatment received. Furthermore, disturbances of function were collected based on a multiple choice question: “Do you have these disturbances of function (i.e. breathing, movement, sensation, and bladder or bowel control) currently?” Complications were collected based on the following question: “Do you have this complication (i.e. bedsores, pain, urinary tract infections, and spasticity)?” with three possible answers (none; once had, but not now; have now). The causes of injury were classified as congenital, disease, traumatic, or other. Trauma may occur in the course of traffic accidents, sports, falls or tumbles, gunshot wounds, or violence and is often associated with spinal fractures and dislocations.23 Diseases that can result in SCI include inflammatory disease, tumors, chronic degenerative tuberculosis, degenerative disc disease, or lesions of the spine and iatrogenic spinal cord injury.24,25 Congenital diseases can consist of spina bifida aperta and vascular malformation in the spinal cord, etc.3 The severity of the injury is described as either complete or incomplete, according to the international standards set forth by the American Spinal Association (ASIA).26,27
The symptoms of spinal cord lesions depend on the extent of the injury or non-traumatic cause, and they can include deficits in the ability to perform basic bodily functions, such as breathing, sensation, bowel and bladder control. Deficit in sensation, or sensory loss, refers to the loss of sensations such as pain, touch or temperature. Deficits in motion, or motor loss, refer to muscle weakness and the inability to use the body. We defined urination disorders as urinary retention, urinary incontinence or both, and disorders of defecation as constipation, fecal incontinence, or both. The SCI complications included bedsores, pain, urinary tract infections, and spasticity. The main medical and rehabilitation treatments received included surgery, medicine, traditional therapy (e.g., acupuncture, moxibustion, and massage), physical therapy, rehabilitation training, assistive devices (e.g., orthosis and prosthesis) and other methods appropriate for SCI individuals.
We calculated the age at injury by birth date and the mean time from the year of injury to the enrollment year in a halfway house. The year of injury was divided into five periods: 1970–1979, 1980–1989, 1990–1999, 2000–2009 and 2010–2015. In this survey, as in previous studies,12,28 the age at injury was divided into five groups: ≤ 15, 16–30, 31–45, 46–60 and ≥ 61 years.
Statistical methods
Descriptive statistics included number of SCI individuals, frequencies and percentages of the subpopulation groups (gender, age groups at injury, complications, etiology, severity and treatment distribution), and mean of time from injury to enrolling in a halfway house in Shanghai. The means of all continuous variables were presented with standard deviations (SDs). The Pearson's chi-square test was used to evaluate the significance of differences in sex, age at injury, complications, etiology, and severity across the injury time periods. Pearson's chi-square test was conducted to examine the factors related with complete and traumatic SCI. All the statistical tests were two-sided, and a P-value less than 0.05 was considered significant. The Statistical Package for Social Sciences for Windows (SPSS for Windows 13.0) was used to perform descriptive statistics and chi-square tests.
Results
General characteristics
There were 546 male (67.6%) and 262 female (32.4%) SCI individuals (male: female = 2.1: 1). The mean time (± SD) from injury to halfway houses enrollment was 12.8 ± 10.6 years (Table 1). The proportion of men and women was almost equal before 15 years of age (Fig. 1), and after age 60 the proportion of men was only 8 percentage points greater than that of female cases. However, male SCI individuals constituted more than 2/3 of all individuals in the age groups between 16 and 60 years old. The main age groups of individuals were 46–60 years (30.3%, Table 1) and 31–45 years (29.5%). In short, male and middle-aged persons had a higher prevalence of SCI.
Table 1.
Characteristics of SCI individuals by year at injury in halfway houses of Shanghai, China.
| Variables | 1970–1979* | 1980–1989 | 1990–1999 | 2000–2009 | 2010–2015 | Total | P-value |
|---|---|---|---|---|---|---|---|
| No. individuals | 43 | 119 | 132 | 387 | 127 | 808 | |
| Years ** (mean, SD) | 36.3, 3.2 | 28.3, 3.1 | 17.9, 3.2 | 7.3, 3.4 | 1.5, 1.5 | 12.8, 10.6 | |
| Sex | 0.074 | ||||||
| male | 33 (76.7%) | 84 (70.6%) | 93 (70.5%) | 243 (62.8%) | 93 (73.2%) | 546 (67.6%) | |
| female | 10 (23.3%) | 35 (29.4%) | 39 (29.5%) | 144 (37.2%) | 34 (26.8%) | 262 (32.4%) | |
| Age at injury | < 0.001 | ||||||
| 0–15 | 5 (11.6%) | 18 (15.1%) | 15 (11.4%) | 19 (4.9%) | 6 (4.7%) | 63 (7.8%) | |
| 16–30 | 33 (76.7%) | 66 (55.5%) | 31 (23.5%) | 51 (13.2%) | 18 (14.2%) | 199 (24.6%) | |
| 31–45 | 5 (11.6%) | 33 (27.7%) | 62 (47.0%) | 116 (30.0%) | 22 (17.3%) | 238 (29.5%) | |
| 46–60 | 0 | 2 (1.7%) | 23 (17.4%) | 163 (42.1%) | 57 (44.9%) | 245 (30.3%) | |
| 61+ | 0 | 0 | 1 (0.8%) | 38 (9.8%) | 24 (18.9%) | 63 (7.8%) | |
| Complications*** | < 0.001 | ||||||
| none | 1 (2.3%) | 13 (10.9%) | 22 (16.7%) | 101 (26.1%) | 14 (11.0%) | 151 (18.7%) | |
| at least one once, but not now | 26 (60.5%) | 67 (56.3%) | 77 (58.3%) | 203 (52.5%) | 86 (67.7%) | 459 (56.8%) | |
| at least one now | 16 (37.2%) | 39 (32.8%) | 33 (25.0%) | 83 (21.4%) | 27 (21.3%) | 198 (24.5%) | |
| Etiology | < 0.001 | ||||||
| congenital | 3 (7.0%) | 10 (8.4%) | 8 (6.1%) | 9 (2.3%) | 3 (2.4%) | 33 (4.1%) | |
| disease | 6 (14.0%) | 29 (24.4%) | 29 (22.0%) | 128 (33.1%) | 46 (36.2%) | 238 (29.5%) | |
| traumatic injury | 34 (79.1%) | 79 (66.4%) | 89 (67.4%) | 207 (53.5%) | 60 (47.2%) | 469 (58.0%) | |
| other | 0 | 1 (0.8%) | 6 (4.5%) | 43 (11.1%) | 18 (14.2%) | 68 (8.4%) | |
| Severity | < 0.001 | ||||||
| incomplete | 19 (44.2%) | 52 (43.7%) | 61 (46.2%) | 238 (61.5%) | 61 (48.0%) | 431 (53.3%) | |
| complete | 24 (55.8%) | 67 (56.3%) | 71 (53.8%) | 149 (38.5%) | 66 (52.0%) | 377 (46.7%) |
*Year at injury; **time from injury to enrolling in halfway houses in Shanghai; ***includes bedsores, pain, urinary tract infections, and spasticity.
Figure 1.
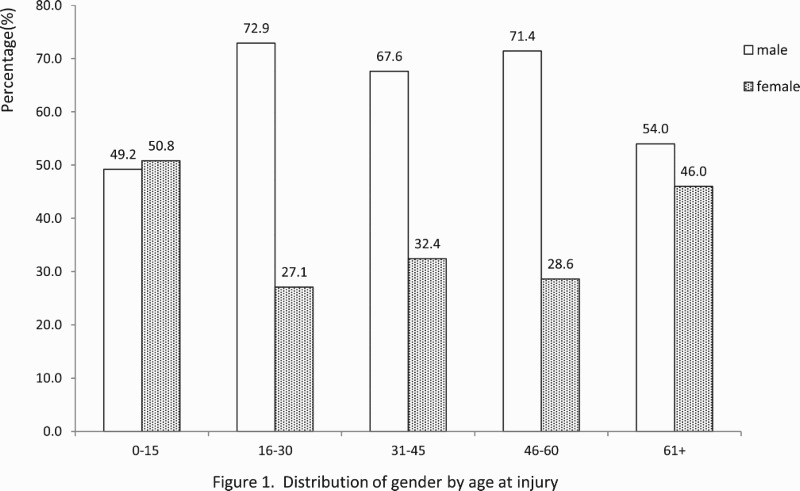
Distribution of gender by age at injury.
From the 1970s to the 2000s, the proportion of the 16–30 age group decreased from 76.7% to 13.2%; meanwhile, the proportion of the age groups over 45 years rose significantly (Table 1). The age groups of men and women showed similar trends, i.e., the proportion of 16–30 and 0–15-year-old SCI individuals at the time of injury was reduced across time (Fig. 2).
Figure 2.
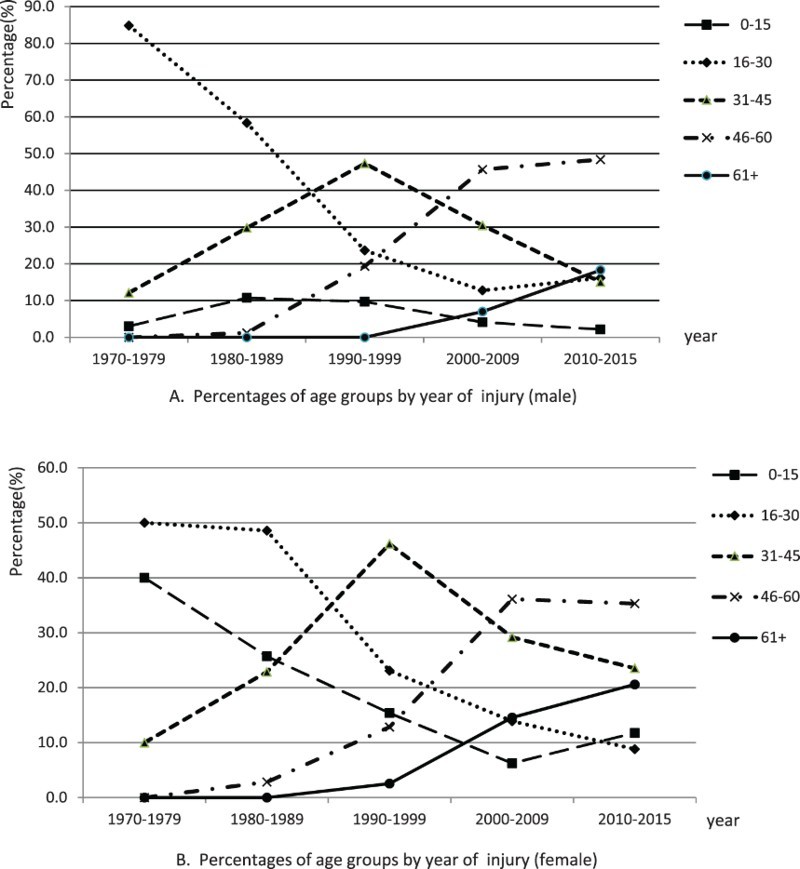
Percentages of age groups by year at injury of SCI individuals (A: male; B: female). The age at injury was divided into five groups: ≤ 15, 16–30, 31–45, 46–60 and ≥ 61 years.
Etiology of the injury
The principal cause of spinal injury was trauma, followed by disease (Table 1). From the 1970s to the 2010s, the proportion of traumatic injuries decreased by 31.9 percentage points and the proportion of disease increased by 22.2 percentage points (P < 0.001).
The principal cause of SCI in individuals younger than 16 was congenital (Fig. 3), while trauma was the leading cause of SCI among individuals between 16 and 60 years old. However, disease turned out to be the principal cause of SCI for individuals after age 60. Those age groups between 16 and 30 years old were most likely to sustain traumatic injury (Table 2), followed by the age group of 31–45 years and 45–60 years.
Figure 3.
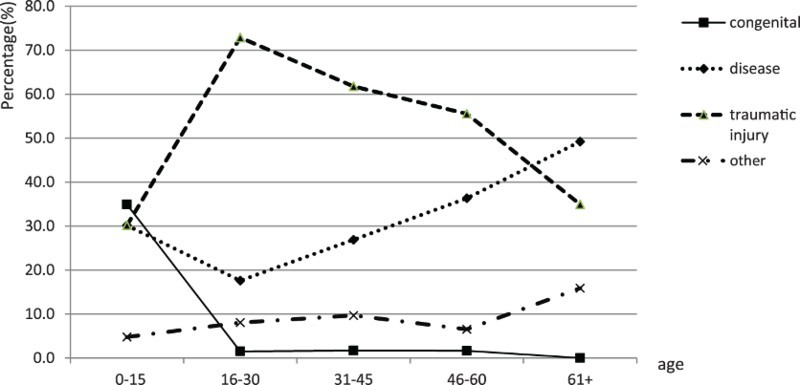
Distribution of etiology by age at injury. The etiology was classified as congenital causes, disease, traumatic causes, or other.
Table 2.
Characteristics of SCI individuals in traumatic vs. non-traumatic groups.
| Variables | Traumatic, n (%) | Non-traumatic, n (%) | P-value |
|---|---|---|---|
| Sex | 0.004 | ||
| female | 133 (50.8%) | 129 (49.2%) | |
| male | 336 (61.5%) | 210 (38.5%) | |
| Age at injury | < 0.001 | ||
| 0–15 | 19 (30.2%) | 44 (69.8%) | |
| 16–30 | 145 (72.9%) | 54 (27.1%) | |
| 31–45 | 147 (61.8%) | 91 (38.2%) | |
| 46–60 | 136 (55.5%) | 109 (44.5%) | |
| 61+ | 22 (34.9%) | 41 (65.1%) | |
| Year at injury | < 0.001 | ||
| 1970–1979 | 34 (79.1%) | 9 (20.9%) | |
| 1980–1989 | 79 (66.4%) | 40 (33.6%) | |
| 1990–1999 | 89 (67.4%) | 43 (32.6%) | |
| 2000–2009 | 207 (53.5%) | 180 (46.5%) | |
| 2010–2015 | 60 (47.2%) | 67 (52.8%) |
Severity of injury
Complete injury accounted for 46.7% of the SCI individuals (Table 1). The proportion of complete injury individuals in 2000–2009 was smaller than that of incomplete injury in 2000–2009, which was much smaller than that in other periods (Table 1, P < 0.001). Persons younger than 45 were overrepresented among the complete injury group compared to persons over age 45 (Table 3).Traumatic injuries were more likely to be complete (Table 3, P < 0.001).
Table 3.
Characteristics of SCI individuals with incomplete or complete injury.
| Variables | Incomplete, n (%) | Complete, n (%) | P-value |
|---|---|---|---|
| Sex | 0.347 | ||
| female | 146 (55.7%) | 116 (44.3%) | |
| male | 285 (52.2%) | 261 (47.8%) | |
| Age at injury | 0.015 | ||
| 0–15 | 27 (42.9%) | 36 (57.1%) | |
| 16–30 | 96 (48.2%) | 103 (51.8%) | |
| 31–45 | 121 (50.8%) | 117 (49.2%) | |
| 46–60 | 150 (61.2%) | 95 (38.8%) | |
| 61+ | 37 (58.7%) | 26 (41.3%) | |
| Etiology | < 0.001 | ||
| traumatic | 267 (56.9%) | 202 (43.1%) | |
| non-traumatic | 229 (67.9%) | 110 (32.4%) |
Treatment received
The treatment choices for SCI and its complications in different SCI patient groups are related to the etiology of the injury (Table 4). Surgery and rehabilitation training were the main choices for traumatic SCI individuals, while medicine, assistive devices, and rehabilitation training were leading options for the disease-initiated SCI individuals.
Table 4.
Medical treatment and rehabilitation received for SCI individuals by the severity of injury and etiology.*
| Variables | Total (n) | Surgery(%**) | Medicine (%) | Rehabilitation training (%) | Assistive devices (eg., orthosis, prosthesis) (%) | Physical therapy (%) | Traditional therapy (%) | Other (%) | P-value |
|---|---|---|---|---|---|---|---|---|---|
| No. individuals | 808 | 53.8 | 49.0 | 46.9 | 41.1 | 21.3 | 17.0 | 17.7 | |
| Severity | < 0.001 | ||||||||
| incomplete | 431 | 48.5 | 48.0 | 49.4 | 44.1 | 15.3 | 11.4 | 23.0 | |
| complete | 377 | 59.9 | 50.1 | 44.0 | 37.7 | 28.1 | 23.3 | 11.7 | |
| Etiology | < 0.001 | ||||||||
| congenital | 33 | 24.2 | 48.5 | 39.4 | 54.5 | 21.2 | 27.3 | 9.1 | |
| disease | 238 | 52.9 | 68.1 | 55.0 | 57.1 | 26.5 | 21.4 | 16.4 | |
| traumatic injury | 469 | 63.5 | 45.8 | 46.1 | 34.8 | 21.3 | 15.6 | 10.9 | |
| other | 68 | 4.4 | 4.4 | 27.9 | 22.1 | 2.9 | 5.9 | 73.5 |
*Patients could receive more than one type of treatment; **percentage based on cases.
Depending on the severity of the injury and the characteristics of the SCI individuals, it was expected that there would be different treatment received. The proportion of complete-injury individuals receiving surgery, traditional therapy, and physical therapy was significantly greater than that of incomplete-injury individuals, many of whom preferred rehabilitation training and assistive devices (Table 4).
Complications and disturbances of function
Among SCI individuals, 24.5% had at least one complication currently, and 56.8% had at least one complication before they enrolled in the halfway houses but reported none currently (Table 1). In this study, the disturbances of function were as follows: 44.2% of patients had observable respiratory problems; about half (47.9%) had motor loss, and only 15.3% could stand or walk for short distances; about one tenth (9.7%) had no sensory disorder, while the rest suffered partial sensory disorder (50.9%) or had loss of sensation (39.5%); and 80.6% had urination disorders, with 78.8% having disorders of defecation.
Discussion
To the best of our knowledge, this study was one of the first few community-based SCI studies in China. Although there is still a selection bias among SCI patients chosen to participate in the halfway house activities, the sample is more representative at the city level than hospital-based or district-based SCI patient samples. The results provide first-hand evidence that will be useful in designing the prevention, treatment, and rehabilitation of SCI individuals in Shanghai, as well as in other cities in China or in other developing countries.
We found more male SCI individuals than female individuals in Shanghai, especially in the patient population older than 16, possibly reflecting the different risk exposures between men and women. Similarly, our results indicated that individuals aged 31 to 60 years old were more likely to experience SCI than other age groups. Therefore, middle-aged men should be the top priority for SCI prevention efforts in Shanghai.5,7,10,12,13,29–31 But we found that the proportion of women diagnosed after 60 years of age had increased, possibly because of less family commitments; therefore, aging women are also worth special attention in the prevention of SCI.11,19
The main finding of this study is the rising age at injury in SCI individuals in Shanghai over the last four decades. This might reflect two different demographic events. First, Shanghai has become an aging society since 2000; 28.8% of the city’s residents were older than 60 at the end of 2014.32 The life expectancy of the enrolled population had increased from 73.4 years in 1978 to 82.3 years in 2014.33 Since other cities in China have also entered into an “aging society” mode, there is no doubt that the average age of SCI individuals has increased simultaneously in those locales.34 For example, the high-risk age group for SCIs had shifted from 20–39 years in 1982–198635 to 30–40 years in 200236 in Beijing. Studies from North America,37–40 Finland,41 and Brazil42 revealed the same pattern of increasing age at injury for SCI individuals. Second, the increasing age at injury could be related to changes in etiology over time. This study suggested that the main etiology of SCIs in Shanghai were traumatic injuries, which was in line with other studies.19,36,42,43 While the proportion of traumatic injuries decreased, the proportion of non-traumatic injury rose significantly from 1970 to 2015. The continuing increases in tumorigenesis, osteoporosis, and degenerative diseases44 in an aging society like China may contribute to the increase in non-traumatic SCI. In fact, non-traumatic SCI individuals were more likely to have incomplete injury and have a more favorable prognosis after active treatment.3 It has been predicted that the number of people older than age 60 in China will be 438 million by 2050,10 so the country’s health care system needs to be prepared to treat more non-traumatic SCI individuals.
Compared to the proportion of complete SCI individuals in developed countries, the rate in Shanghai was still relatively high. For example, the United States reported the proportion of complete SCI in all SCI individuals as 55.6% in 1973–2003 but decreased to 34% in recent years.45 Canada has reported that approximately two thirds of SCIs in that country were complete in the 1950s, but the proportion decreased to 45% in the 1980s46 and 35% in 1997–2001.37 This means the proportion of complete SCI individuals in Shanghai still has room to decrease. The most promising way to reduce complete SCI individuals would be to reduce traumatic injuries, since our study shows that traumatic injuries were more likely to be related to complete injuries.
Shanghai, as one of the most developed regions in China, has the resources to spend on effective programs to prevent and treat SCI individuals. This study suggests several steps for the city to improve the welfare of SCI individuals. First, it is essential to establish a surveillance system. In the future, comprehensive data must be collected and analyzed to help identify and track individual SCI patients in Shanghai.47 Second, similar to other countries and regions, traumatic injuries are still the principal cause of SCI in Shanghai, so it is recommended that exposures to traumatic risks be reduced with improved security measures, especially in high-risk industries,48 and in traffic49 and law enforcement18,50 to reduce the incidence of accidents. Last but not least, more research on halfway houses will help evaluate the effectiveness of these interventions and improve care for SCI individuals in Shanghai. This research revealed that one-fourth of those with SCIs still suffered from complications, which was similar to the result obtained in other regions in China.44 In addition, disturbances of function remained a serious problem. It is necessary to take further steps to relieve these burdens. Literature suggests that rehabilitation could improve, substitute for, and help reconstruct impaired functions. The sooner such rehabilitation is initiated, the more likely patients are to improve in their ability to manage their activities of daily living and even partially restore their ability to work, thus elevating their living quality and life quality. But before 2009, most SCI individuals could not receive any rehabilitation services after their medical discharge because of limited resources. Currently in China, the number of individuals in halfway houses has exceeded 3,000. More such houses could be established in the communities with high concentrations of SCI individuals across cities in China.51
The study has a few limitations to acknowledge. First, we conducted a census of all SCI individuals enrolled in halfway houses. However, not every SCI patient has the same probability of being enrolled in halfway houses, since some individuals may not be aware of this organization or are not interested in enrolling. This potential selection bias indicates that the study population may not be fully representative. That is to say, the data in this study only represent SCI individuals admitted in the halfway houses program; ergo the interpretation of the results may not be applicable to all SCI individuals in Shanghai. Furthermore, the size of the study population was limited. Given the national SCI prevalence of 1 in 1,370 individuals in China in 2010, there are about 10,000 SCI individuals in Shanghai. Despite this, our study sample still represents a non-trivial portion of SCI individuals in that city. Finally, information about the level of injury, cause of injury, and complications is still lacking more significant detail in the original database.
Conclusions
In summary, this article covered selected SCI individuals from halfway houses in Shanghai, among whom years of injury spanned for four decades (1970–2015). The results are important for a baseline assessment of the SCI population in Shanghai and are crucial for prevention and treatment policy improvement for SCI individuals. The government agencies of China need to implement effective policies to target high-risk groups, such as middle-aged men, for injury prevention. Additionally, more research is needed to understand the trajectory of SCI individuals’ recovery in halfway houses, such as treatment effectiveness, complications, and disturbances of function of SCI individuals. Finally, the establishment of a SCI database should be added to the agenda as soon as possible.
Acknowledgements
We express thanks to the Rehabilitation Department of the Shanghai Disabled Persons’ Federation for help with collecting data from relevant enrollment records. This work was supported by National Natural Science Foundation of China [71673052, 71203034], National Planning Office of Philosophy and Social Science of China [13AZD081], China Scholarship Council [201506105030], Shanghai Pujiang Program of Shanghai Municipal Human Resources and Social Security Bureau [17PJC003] and 111 Project [Grant Number B16031].
Disclaimer statements
Contributors None.
Declaration of interest The authors report no declarations of interest.
Ethics approval None.
References
- 1.Yang R, Guo L, Wang P, Huang L, Tang Y, Wang WH, et al. Epidemiology of spinal cord injuries and risk factors for complete injuries in Guangdong, China: A retrospective study. PLoS One 2014;9(1):e84733. doi: 10.1371/journal.pone.0084733 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Thurman DJ, Sniezek JE, Johnson D, Greenspan A, Smith SM.. Guidelines for surveillance of central nervous system injury. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention, 1995. [Google Scholar]
- 3.Hou CL, Fan ZP, Wang SB.. Guide for spinal cord injury rehabilitation: Shanghai Scientific and Technical Publishers, 2006. (in Chinese).
- 4.Ho CH, Wuermser L, Priebe MM, Chiodo AE, Scelza WM, Kirshblum SC.. Spinal Cord Injury Medicine. 1. Epidemiology and Classification. Arch. Phys. Med. Rehab. 2007;88(3):S49–54. doi: 10.1016/j.apmr.2006.12.001 [DOI] [PubMed] [Google Scholar]
- 5.Wyndaele M, Wyndaele JJ.. Incidence, prevalence and epidemiology of spinal cord injury: What learns a worldwide literature survey? Spinal Cord 2006;44(9):523–9. doi: 10.1038/sj.sc.3101893 [DOI] [PubMed] [Google Scholar]
- 6.Jazayeri SB, Beygi S, Shokraneh F, Hagen EM, Rahimi-Movaghar V.. Incidence of traumatic spinal cord injury worldwide: A systematic review. Eur. Spine J. 2015;24(5):905–18. doi: 10.1007/s00586-014-3424-6 [DOI] [PubMed] [Google Scholar]
- 7.Rahimi-Movaghar V, Sayyah MK, Akbari H, Khorramirouz R, Rasouli MR, Moradi-Lakeh M, et al. Epidemiology of traumatic spinal cord injury in developing countries: A systematic review. Neuroepidemiology 2013;41(2):65–85. doi: 10.1159/000350710 [DOI] [PubMed] [Google Scholar]
- 8.Chamberlain JD, Deriaz O, Hund-Georgiadis M, Meier S, Scheel-Sailer A, Schubert M, et al. Epidemiology and contemporary risk profile of traumatic spinal cord injury in Switzerland. Injury Epidemiology 2015;2(1):28. doi: 10.1186/s40621-015-0061-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ning GZ, Wu Q, Li YL, Feng SQ.. Epidemiology of traumatic spinal cord injury in Asia: A systematic review. J Spinal Cord Med 2012;35(4):229–39. doi: 10.1179/2045772312Y.0000000021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Liu P, Yao Y, Liu MY, Fan WL, Chao R, Wang ZG, et al. Spinal Trauma in Mainland China from 2001 to 2007. Spine 2012;37(15):1310–5. doi: 10.1097/BRS.0b013e3182474d8b [DOI] [PubMed] [Google Scholar]
- 11.Deng L, Shang H, Chang W, Wu YP, Li Bk, Guo ZP, et al. Epidemiologic analysis of 424 cases of spine and spinal cord injuries. Chinese Journal of Clinical Research 2015;28(7):858–60, 864 (in Chinese). [Google Scholar]
- 12.Wang HF, Yin ZS, Chen Y, Duan ZH, Hou S, He J.. Epidemiological features of traumatic spinal cord injury in Anhui Province, China. Spinal Cord 2013;51(1):20–2. doi: 10.1038/sc.2012.92 [DOI] [PubMed] [Google Scholar]
- 13.Wu Q, Li YL, Ning GZ, Feng SQ, Chu TC, Li Y, et al. Epidemiology of traumatic cervical spinal cord injury in Tianjin, China. Spinal Cord 2012;50(10):740–4. doi: 10.1038/sc.2012.42 [DOI] [PubMed] [Google Scholar]
- 14.China Association of Persons with Physical Disability ‘Giti hotline for spinal cord injured patients’ project construction plan [document on the Internet] 2012. [updated 2014 March 28; cited 2016 February 15]. Available from http://www.cappd.org/news/show-1268.aspx (in Chinese).
- 15.Qiu J. China Spinal Cord Injury Network: Changes from within. The Lancet Neurology 2009;8(7):606–7. doi: 10.1016/S1474-4422(09)70162-0 [DOI] [PubMed] [Google Scholar]
- 16.Shanghai Municipal Statistics Bureau Shanghai basic facts (2014) [document on the Internet] 2014 [updated 2008 January; cited 2015 December 18]. Available from http://en.shio.gov.cn/file/images/ShanghaiFacts2014En.pdf.
- 17.Hu GY, Tang HF, Tang LA.. Epidemiology investigation of spinal cord injury in SongJiang, Shanghai. Chinese Journal of Spine and Spinal Cord 1992(04):177–9 (in Chinese). [Google Scholar]
- 18.Pan J, Li X, Ceng C, Qian L, Li LJ, Tan J.. Retrospective study of acute spinal cord injury between 2005 and 2007 in Pudong New Area, Shanghai. Journal of Tongji University (medical science) 2009;30(5):131–5 (in Chinese). [Google Scholar]
- 19.Cheng LM, Zeng ZL, Yang ZY, Zhou JQ, Yuan F, Zhang SM, et al. Epidemiologic features and effects of surgical treatment of spinal injuries treated in one medical center. Chinese Journal of Orthopaedic Trauma 2008;10(3):245–8 (in Chinese). [Google Scholar]
- 20.Li J, Liu G, Zheng Y, Hao C, Zhang Y, Wei B, et al. The epidemiological survey of acute traumatic spinal cord injury (ATSCI) of 2002 in Beijing municipality. Spinal Cord 2011;49(7):777–82. doi: 10.1038/sc.2011.8 [DOI] [PubMed] [Google Scholar]
- 21.Report on "halfway houses" in Shanghai [document on the Internet] 2014. [cited 2016 March 8]. Available from http://www.spinalcord.uab.edu/show.asp?durki=116979 (in Chinese).
- 22.China Association of Persons with Physical Disability Halfway houses in China [document on the Internet] 2013 [cited 2016 February 5]. Available from http://www.cappd.org/html/special/zhongtu/ZhongTu.htm (in Chinese).
- 23.Wang CM, Chen Y, DeVivo MJ, Huang CT.. Epidemiology of extraspinal fractures associated with acute spinal cord injury. Spinal Cord 2001;39(11):589–94. doi: 10.1038/sj.sc.3101216 [DOI] [PubMed] [Google Scholar]
- 24.Chen Q, Li F, Shen K, Chen AM, Guo FJ, Luo W, et al. Epidemiological analysis of iatrogenic spinal cord injury. Neural Injury and Functional Reconstruction 2011;06(2):123–7 (in Chinese). [Google Scholar]
- 25.Kirshblum SC, Groah SL, McKinley WO, Gittler MS, Stiens SA.. Spinal cord injury medicine. 1. Etiology, classification, and acute medical management. Arch. Phys. Med. Rehab. 2002;83(3 Suppl 1):S50–57, S90–8. doi: 10.1053/apmr.2002.32156 [DOI] [PubMed] [Google Scholar]
- 26.Kirshblum SC, Burns SP, Biering-Sorensen F, Donovan W, Graves DE, Jha A, et al. International standards for neurological classification of spinal cord injury (revised 2011). J Spinal Cord Med 2011;34(6):535–46. doi: 10.1179/204577211X13207446293695 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ditunno JJ, Young W, Donovan WH, Creasey G.. The international standards booklet for neurological and functional classification of spinal cord injury. American Spinal Injury Association. Paraplegia 1994;32(2):70–80. [DOI] [PubMed] [Google Scholar]
- 28.Ning G. Z., Yu T. Q., Feng S. Q., Zhou X. H., Ban D. X., Liu Y., et al. Epidemiology of traumatic spinal cord injury in Tianjin, China. Spinal Cord. 2011;49(3):386–90. doi: 10.1038/sc.2010.130 [DOI] [PubMed] [Google Scholar]
- 29.Hao CX, Li JJ, Zhou HJ, Kang HQ, Li SQ, Liu GL, et al. Epidemiological analysis on 1264 cases of inpatient patients with spinal cord injury. Chinese Journal of Rehabilitation Theory and Practice 2007(11):1011–3 (in Chinese). [Google Scholar]
- 30.Yu TQ, Feng SQ.. Epidemiological analysis of 216 cases of hospitalized patients with traumatic spinal cord injury. Chinese Journal of Bone and Joint Damage 2010;25(7):583–5 (in Chinese). [Google Scholar]
- 31.Chiu WT, Lin HC, Lam C, Chu SF, Chiang YH, Tsai SH.. Review paper: Epidemiology of traumatic spinal cord injury: Comparisons between developed and developing countries. Asia Pac J Public Health 2010;22(1):9–18. doi: 10.1177/1010539509355470 [DOI] [PubMed] [Google Scholar]
- 32.Paper The. The proportion of Shanghai elderly population was nearly thirty percent in 2014 [document on the Internet] 2015 [updated 2015 March 30; cited 2016 March 5]. Available from http://news.163.com/15/0330/20/AM009NR200014SEH.html (in Chinese).
- 33.Shanghai Municipal Statistics Bureau Total households, population, density of registered population and life expectancy (1978∼2014) [document on the Internet] 2015 [cited 2016 January 85]. Available from http://www.stats-sh.gov.cn/tjnj/nje15.htm?d1=2015tjnje/E0201.htm.
- 34.Feng HY, Ning GZ, Feng SQ, Yu TQ, Zhou HX.. Epidemiological profile of 239 traumatic spinal cord injury cases over a period of 12 years in Tianjin, China. J Spinal Cord Med 2011;34(4):388–94. doi: 10.1179/2045772311Y.0000000017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Spinal Cord Injury Investigating Group in Beijing The Reviewing survey for spinal cord injury in Beijing. Chinese Journal of Rehabilitation. 1988(02):59–62 (in Chinese). [Google Scholar]
- 36.Li JJ, Zhou HJ, Hong Y, Ji JP, Liu GL, Su SQ, et al. Spinal cord injuries in Beijing: A municipal epidemiological survey in 2002. Chinese Journal of Rehabilitation Theory and Practice 2004(07):32–3 (in Chinese). [Google Scholar]
- 37.Pickett GE, Campos-Benitez M, Keller JL, Duggal N.. Epidemiology of traumatic spinal cord injury in Canada. Spine 2006;31(7):799–805. doi: 10.1097/01.brs.0000207258.80129.03 [DOI] [PubMed] [Google Scholar]
- 38.Lenehan B, Street J, Kwon BK, Noonan V, Zhang H, Fisher CG, et al. The epidemiology of traumatic spinal cord injury in British Columbia, Canada. Spine 2012;37(4):321–9. doi: 10.1097/BRS.0b013e31822e5ff8 [DOI] [PubMed] [Google Scholar]
- 39.Jackson AB, Dijkers M, Devivo MJ, Poczatek RB.. A demographic profile of new traumatic spinal cord injuries: Change and stability over 30 years. Arch. Phys. Med. Rehab. 2004;85(11):1740–8. doi: 10.1016/j.apmr.2004.04.035 [DOI] [PubMed] [Google Scholar]
- 40.McCammon JR, Ethans K.. Spinal cord injury in Manitoba: A provincial epidemiological study. J Spinal Cord Med 2011;34(1):6–10. doi: 10.1179/107902610X12923394765733 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Ahoniemi E, Alaranta H, Hokkinen EM, Valtonen K, Kautiainen H.. Incidence of traumatic spinal cord injuries in Finland over a 30-year period. Spinal Cord 2008;46(12):781–4. doi: 10.1038/sc.2008.53 [DOI] [PubMed] [Google Scholar]
- 42.Bellucci CH, Castro FJ, Gomes CM, Bessa JJ, Battistella LR, Souza DR, et al. Contemporary trends in the epidemiology of traumatic spinal cord injury: Changes in age and etiology. Neuroepidemiology 2015;44(2):85–90. doi: 10.1159/000371519 [DOI] [PubMed] [Google Scholar]
- 43.Selassie A, Cao Y, Saunders LL.. Epidemiology of Traumatic Spinal Cord Injury among Persons Older than 21 Years: A Population-Based Study in South Carolina, 1998–2012. Topics in Spinal Cord Injury Rehabilitation 2015;21(4):333–44. doi: 10.1310/sci2015-313 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Yu TQ, Feng SQ, Zhang XL, Deng SC, Jiang WX, Ni DK, et al. Characteristics of urban inpatients with traumatic spinal cord injuries in Tianjin, 2007. Chinese Journal of Rehabilitation Theory and Practice 2010;16(5):486–8 (in Chinese). [Google Scholar]
- 45.Model Systems Knowledge Translation Center National Spinal Cord Injury Statistical Center. Spinal cord injury (SCI) facts and figures at a glance [document on the Internet].2014 [cited 2016 January 9]. Available from https://www.nscisc.uab.edu/PublicDocuments/fact_figures_docs/Facts%202014.pdf.
- 46.Tator CH, Duncan EG, Edmonds VE, Lapczak LI, Andrews DF.. Changes in epidemiology of acute spinal cord injury from 1947 to 1981. Surgical Neurology 1993;40(3):207–15. doi: 10.1016/0090-3019(93)90069-D [DOI] [PubMed] [Google Scholar]
- 47.O'Connor PJ. Development and utilisation of the Australian spinal cord injury register. Spinal Cord 2000;38(10):597–603. doi: 10.1038/sj.sc.3101048 [DOI] [PubMed] [Google Scholar]
- 48.Ding XD. From the ‘world factory’ to the international capacity cooperation—the promotion of the position of China in global value chain. Globalization 2015(07):12–20 (in Chinese). [Google Scholar]
- 49.Lu TT, Qian YS, Zeng JW.. Comparison and study of road traffic accident in USA and China. Urban Roads Bridges & Flood 2015(10):157–60 (in Chinese). [Google Scholar]
- 50.Shin JC, Kim DH, Yu SJ, Yang HE, Yoon SY.. Epidemiologic change of patients with spinal cord injury. Annals of Rehabilitation Medicine 2013;37(1):50–6. doi: 10.5535/arm.2013.37.1.50 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Wu XG, Chen D, Zhang J.. Community-based rehabilitation and rehabilitation of ‘rehabilitation for all’. Chinese Journal of Rehabilitation Theory and Practice 2011(07):613–6 (in Chinese). [Google Scholar]