

Abstract
Dihydroartemisinin/piperaquine (DHA/PPQ) is increasingly deployed as an antimalaria drug in Africa. We report the detection in Mali of Plasmodium falciparum infections carrying plasmepsin 2 duplications (associated with piperaquine resistance) in 7/65 recurrent infections within 2 months after DHA/PPQ treatment. These findings raise concerns about the long-term efficacy of DHA/PPQ treatment in Africa.
Keywords: malaria, piperaquine, resistance, Plasmodium falciparum, plasmepsin 2, Pfpm2, dihydroartemisinin-piperaquine, DHA-PPQ, West Africa, vector-borne infections, moquitoborne diseases
Artemisinin combination therapy has been the cornerstone of malaria control in sub-Saharan Africa for the past 10 years and is typically represented by artemether/lumefantrine and artesunate/amodiaquine. Because of the notorious capacities of Plasmodium falciparum to develop drug resistance, many antimalarial programs have recently included dihydroartemisinin/piperaquine (DHA/PPQ) as a second-line antimalarial drug. This decision is sensible, considering the recent reports of substantially decreased artemether/lumefantrine cure rates in some regions, signaling a potential focus of lumefantrine resistance (1).
DHA/PPQ has shown near-perfect efficacy levels in clinical trials conducted in Africa; the combination also has been proposed as a tool for intermittent preventive approaches (2). Unfortunately, full P. falciparum resistance to DHA/PPQ treatment has been reported recently in Cambodia (3,4). These events were directly associated with increased copy number variations (CNVs) in the plasmepsin system, including the pfpm2 gene (PF3D7_1408000) coding for the food vacuole enzyme plasmepsin II, which is speculated to be a major piperaquine target.
CNV is generally considered as emerging at relatively rapid mutation rates (a rate several orders of magnitude higher compared with that of single-nucleotide polymorphisms [5]) and is able to generate substantial diversity (6). Therefore, preexisting pfpm2 duplications in Cambodia might have been rapidly selected by DHA/PPQ, aided by a less effective protective action of the artemisinin derivative (7). Such a scenario suggests that this mutation may already be present in Africa.
To investigate this possibility, we analyzed a subset of archived P. falciparum DNA samples from clinical infections, derived from a set of large, multicenter comparative artemisinin combination therapy efficacy trials conducted in West Africa by the West African Network for Antimalarial Drugs (8). These trials, performed during October 2011–February 2016 in Mali, Burkina Faso, and Guinea, had a randomized double-blind design with a 2-year follow-up for monitoring repeated treatment. Here we focus on the DHA/PPQ trial conducted at the village of Bougoula-Hameau in Mali, located ≈350 km south of the capital city of Bamako, near the border with Burkina Faso. The weekly control follow-up for each episode at Bougoula-Hameau was 63 days, and the DHA/PPQ arm involved a total of 224 patients who were >6 months of age.
We conducted a pilot study analyzing the 96 recurrent infections associated with the shortest interepisode periods, assuming that this subgroup, among whom initiation of recurrent infection ranged from 23 to 65 days posttreatment (Figure), would be the most likely to include pfpm2 duplications. The study was reviewed and approved by the Ethics Committee of the Faculty of Medicine, Pharmacy, and Odonto-Stomatology, University of Sciences, Techniques and Technology of Bamako.
Figure.
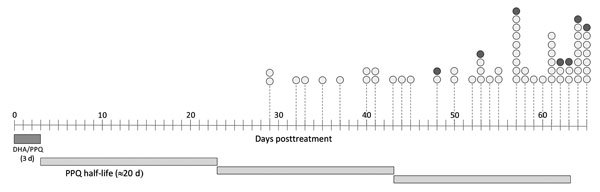
Timeline distribution of Plasmodium falciparum pfpm2 copy number status during post–DHA/PPQ treatment follow-up for artemisinin combination therapy efficacy trials conducted by the West African Network for Antimalarial Drugs, Mali, Burkina Faso, and Guinea, October 2011–February 2016. Dark gray bar highlights the period (3 d) of treatment; lighter, longer gray bars represent PPQ average half-life (≈20 d). Circles represent recurrent infections; white circles indicate 1 pfpm2 copy, and gray circles indicate 2 pfpm2 copies. DHA/PPQ, dihydroartemisinin/piperaquine; PPQ, piperaquine.
We determined copy number by using a SYBR-green–based quantitative PCR (ThermoFisher Scientific, Waltham, MA, USA) in a protocol modified from the one previously described by Witkowski et al (4). We used the P. falciparum β-tubulin gene as the internal nonduplicated standard and the 3D7 clone as a parallel 1 copy control. We ran the quantitative PCR thermal cycle at 98°C for 3 min, followed by 45 cycles at 98°C for 15 s, 63°C for 20 s, and 72°C for 20 s on a C1000 Thermal Cycler (Bio-Rad, Marnes-la-Coquette, France) with the CFX96 Real-Time System (Bio-Rad) detection system. We executed all procedures in triplicate.
The analysis was conclusive in 65 of the 96 samples. We confirm the presence of 7 infections carrying 2 copies of pfpm2, representing ≈10% of the successfully analyzed infections. We did not identify any trend of earlier recurrence associated with this group of infections (Figure), a preliminarily observation that needs to be further explored in a larger sample set.
Our results clearly show that piperaquine resistance–associated pfpm2 duplications are probably already frequent in Africa, which is of concern given the long half-life of piperaquine (>20 days). In high-transmission areas, this long period of decreasing drug exposure is likely to progressively select less sensitive, potentially pfpm2 CNV–carrying parasites. Parallel studies conducted in these areas have not detected substantial altered parasite clearance dynamics or K13 mutations associated with artemisinin-derivative therapy (9,10), indicating that these pfpm2 duplications are emerging despite the efficacy of dihydroartemisinin. Further studies are urgently needed to clarify the clinical implications of piperaquine resistance and to monitor occurrence in other areas of high malaria transmission in Africa.
Acknowledgments
We are grateful to Hamadoun Diakite, Sekou Toure, Amadou H. Togo, Sekou Koumare, and the entire WANECAM team of Bougoula-Hameau. We thank the study patients and their parents and legal guardians, the respective communities involved, and the healthcare authorities of Sikasso.
This work was supported by a Swedish Research Council Grant (no. VR-2014–3134). The WANECAM study is funded by the European and Developing Countries Clinical Trial Partnership and by the Medicines for Malaria Venture (Geneva, Switzerland) and is co-funded by the United Kingdom Medical Research Councils, the Swedish International Development Cooperation Agency, the German Ministry for Education and Research, the University Claude Bernard (Lyon, France), the University of Science, Techniques, and Technologies of Bamako (Bamako, Mali), the Centre National de Recherche et de Formation sur le Paludisme (Burkina Faso), the Institut de Recherche en Sciences de la Santé (Bobo-Dioulasso, Burkina Faso), and the Centre National de Formation et de Recherche en Santé Rurale (Guinea).
J.I. was supported by EuroInkaNet/Erasmus Mundus Program. Fundação para a Ciência e Tecnologia supports M.S. (grant no. SFRH/BD/129769/2017), M.I.V. (grant no. SFRH/BPD/76614/2011), and P.E.F. (grant no. IF/00143/2015).
Biography
Dr. Inoue is a visiting postdoctoral researcher at the University of Uppsala. Her current research interests include malaria drug resistance with an emphasis on artemisinin combination therapy.
Footnotes
Suggested citation for this article: Inoue J, Silva M, Fofana B, Sanogo K, Mårtensson A, Sagara I, et al. Plasmodium falciparum plasmepsin 2 duplications, West Africa. Emerg Infect Dis. 2018 Aug [date cited]. https://doi.org/10.3201/eid2408.180370
These authors shared first authorship on this article.
References
- 1.Plucinski MM, Talundzic E, Morton L, Dimbu PR, Macaia AP, Fortes F, et al. Efficacy of artemether-lumefantrine and dihydroartemisinin-piperaquine for treatment of uncomplicated malaria in children in Zaire and Uíge Provinces, angola. Antimicrob Agents Chemother. 2015;59:437–43. 10.1128/AAC.04181-14 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gutman J, Kovacs S, Dorsey G, Stergachis A, Ter Kuile FO. Safety, tolerability, and efficacy of repeated doses of dihydroartemisinin-piperaquine for prevention and treatment of malaria: a systematic review and meta-analysis. Lancet Infect Dis. 2017;17:184–93. 10.1016/S1473-3099(16)30378-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Amato R, Lim P, Miotto O, Amaratunga C, Dek D, Pearson RD, et al. Genetic markers associated with dihydroartemisinin-piperaquine failure in Plasmodium falciparum malaria in Cambodia: a genotype-phenotype association study. Lancet Infect Dis. 2017;17:164–73. 10.1016/S1473-3099(16)30409-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Witkowski B, Duru V, Khim N, Ross LS, Saintpierre B, Beghain J, et al. A surrogate marker of piperaquine-resistant Plasmodium falciparum malaria: a phenotype-genotype association study. Lancet Infect Dis. 2017;17:174–83. 10.1016/S1473-3099(16)30415-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Conrad DF, Hurles ME. The population genetics of structural variation. Nat Genet. 2007;39(Suppl):S30–6. 10.1038/ng2042 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Veiga MI, Ferreira PE, Malmberg M, Jörnhagen L, Björkman A, Nosten F, et al. pfmdr1 amplification is related to increased Plasmodium falciparum in vitro sensitivity to the bisquinoline piperaquine. Antimicrob Agents Chemother. 2012;56:3615–9. 10.1128/AAC.06350-11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hastings IM, Hodel EM, Kay K. Quantifying the pharmacology of antimalarial drug combination therapy. Sci Rep. 2016;6:32762. 10.1038/srep32762 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sagara I, Beavogui AH, Zongo I, Soulama I, Borghini-Fuhrer I, Fofana B, et al. ; West African Network for Clinical Trials of Antimalarial Drugs (WANECAM). Pyronaridine-artesunate or dihydroartemisinin-piperaquine versus current first-line therapies for repeated treatment of uncomplicated malaria: a randomised, multicentre, open-label, longitudinal, controlled, phase 3b/4 trial. Lancet. 2018;391:1378–90. 10.1016/S0140-6736(18)30291-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ouattara A, Kone A, Adams M, Fofana B, Maiga AW, Hampton S, et al. Polymorphisms in the K13-propeller gene in artemisinin-susceptible Plasmodium falciparum parasites from Bougoula-Hameau and Bandiagara, Mali. Am J Trop Med Hyg. 2015;92:1202–6. 10.4269/ajtmh.14-0605 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Maiga AW, Fofana B, Sagara I, Dembele D, Dara A, Traore OB, et al. No evidence of delayed parasite clearance after oral artesunate treatment of uncomplicated falciparum malaria in Mali. Am J Trop Med Hyg. 2012;87:23–8. 10.4269/ajtmh.2012.12-0058 [DOI] [PMC free article] [PubMed] [Google Scholar]