

Abstract
Background
Humans are exposed to various stimuli which lead to somatic modifications and changes in body posture, negatively affecting many of its characteristics. The purpose of this study was to assess significant alterations which occurred in selected morphological features and spinal curvatures in children and adolescents over a period of 40 years.
Material/Methods
The total of 7041 subjects, aged 4–18 years (mean age 11.3 years) were included in the study, which was designed to compare measurements performed in year 1959 (Group 1, n=3235 individuals) and in year 2003 (Group 2, n=3806 individuals). The children were examined for body height, body mass, as well as thoracic and lumbar curvatures. In 1959, the measurements were carried out using a spherodorsimeter, while in 2003, the CQ System photogrammetry was used, producing corresponding results. The Mann-Whitney U test and the Student’s t-test were used for statistical analysis.
Results
The findings showed a significant decrease in the angle of lumbar lordosis and in sacral inclination as well as an increase in body height and mass, particularly in prepubertal children. On the other hand, the angle of thoracic kyphosis and the partial angles of physiological spinal curvatures changed only to a small degree over the 40-year period.
Conclusions
This study provides evidence related to changes which occurred during the relevant period of over 40 years, namely a decrease in both the angle of lumbar lordosis and the sacral inclination angle, as well as an increase in body height and mass. These changes should be taken into consideration in selecting norms and standards applied in healthcare services, and the findings suggest it is necessary to regularly update such standards.
MeSH Keywords: Body Image, Body Weight Changes, Kyphosis, Lordosis, Population Growth, Spine
Background
The last few decades have seen significant progress in our understanding of various phenomena related to human health, including the shape of the spine. It is well established that spinal disorders are usually caused by incorrect postures adopted during daily activities. Yet, sagittal angles are frequently underestimated [1]. Their importance lies in the fact that the sagittal curvature of the spine and the pelvic inclination “work together” to enable maintenance of a stable posture and horizontal gaze. Once the sagittal alignment is abnormal, more energy is required so that the body can retain balance without external support [2].
During recent decades we have witnessed a shift towards sedentary lifestyles [3] This is largely linked with advancements in automotive and information technology (IT) industries. Low levels of physical activity [4], and growing hazards related to the natural environment can affect both body mass and height. The secular growth changes observed within populations are important because they provide markers of a given population’s general health as it changes over time [5], and they highlight inequalities in health, nutritional and social status within populations [6]. Given this, there is a lot of interest in growth trends across decades both in Poland [7] and in other countries [8,9].
In the 1950s, people in Poland were physically more active, their lifestyles were not impacted by such technological advancements as cars or computers which require sitting positions. Sedentary modes of operation have become the sign of the times at the start of the new millennium. We know that sitting causes the pelvis to rotate backward and leads to a decrease in lumbar lordosis, trunk-thigh angle, and knee angle and to an increase in muscle effort and disc pressure. Identification of changes in the shape of spinal curvatures, as well as body height and mass would provide evidence of phenotype changes occurring over time. This would also support the claim that it is necessary to update the relevant norms from time to time. Referential norms for diagnosing overweight, obesity, and underweight in children and adolescents are based on measurements performed among the white populations in 1985 [10]. It was shown in a study [11] that the choice of the norm is an important factor determining the frequency with which postural defects are identified. Studies reported by other authors suggest that the shape of the spine is affected by numerous factors, yet there are no studies assessing changes occurring in spinal curvatures over longer time periods.
It has been established that the shape of the spine in the sagittal plane is associated with stages of ontogenetic development [12], physical fitness [13], type of physical activity [14–17], body weight [18], possible overloading [19] and body positioning [20]. Changes in the shape of one section of the spine tend to entail changes in the ones adjacent to or remote from the location of the original change [21,22]. The shape of the spine plays an important role in neural regulation [23], while a reduction in spinal curvature in the sagittal plane changes loading of the spine and its mobility, causing degeneration of intervertebral disks at each level [24]. The factor of time is another variable possibly affecting the shape of the spine, and consequently body height.
Research into changes of body height and mass has been conducted over the decades in Poland [25–27] and in other countries [8,9,28], but were not designed to also focus on spinal curvatures. Such analysis will enable better understanding of how environmental changes affect the shape of the spine, as well as body mass and height.
In view of this, and given the lack of related research, a study designed to investigate this issue is justified by the evident adaptation changes occurring over time and the developments which have affected the environment since the post-war period. There are also practical aspects, such as the need to update normative values related to growth, body mass and spinal curvatures, applied in pediatric medical care. Such studies may also provide information necessary in designing guidelines for standard height of furniture, profiling of chairs, car seats, as well as other devices where body height and shape of the spine are an important matter.
The purpose of this study was to assess significant changes in spinal curvatures as well as body height and mass in Polish children and adolescents aged 4 to 18.5 years old, over a 40-year period.
Material and Methods
Study participants
The comparative analysis took into account measurements obtained from the total of 7041 Polish children and adolescents. The first group of 3235 children was examined in year 1959 (SG-1959) by Napoleon Wolański [29] and the second group of 3806 participants was assessed in year 2003 (CG-2003) by Mirosław Mrozkowiak. Both studies were carried out in various regions throughout Poland and were designed to measure identical somatic and body posture characteristics, i.e., body height, body weight, inclination angles of the lumbosacral spine (alpha), thoracolumbar spine (beta), and upper thoracic spine (gamma), as well as the angle of lumbar lordosis (LLA) and angle of thoracic kyphosis (TKA).
The study was conducted after informed consent was received from the school principals, parents, and the participants themselves. The schools were randomly selected. In 2003, they were selected only in the regions of Poland corresponding with those in which the examinations were carried out in 1959. All children in a given school were examined, provided that they and their parents expressed consent and the children met the eligibility criteria. All the persons qualified for the study were able to walk unassisted, and did not use any orthopedic aids (canes, crutches, or walkers). All the study participants were able to assume standing position for the assessment. Children with neurological disorders or motor deficits impairing their ability to maintain balance in standing position without aid and/or those using any orthopedic tools were disqualified. The eligibility criteria were as follows: absence of injuries or musculoskeletal pain in the previous 6 months; no neurological and systemic diseases. The information regarding health status, orthopedic aids as well as pain was obtained before the examinations were carried out, along with a consent for participation. All the examinations were performed during school hours, from 8 a.m. to 1 p.m.
According to the local bioethics commission in Bydgoszcz, examination of body posture using non-invasive methods, by its nature, is not a medical experiment, therefore a study of this type does not require an approval.
The study group in year 1959 (SG-1959) included 3235 children aged 4–18.5 years. Other parameters included: mean age of 11.03 years, mean body height in the girls 137.16 cm (±6.2 cm) and in the boys 140.93 cm (±5.7 cm), mean body weight of 36.69 kg (±6.4 kg) and 38.15 kg (±6.3 kg) in the girls and the boys, respectively. The comparative study in 2003 (CG-2003) comprised 3806 children aged 4–18.5 years, with mean age of 11.03 years, mean body height of 142.36 cm (±6.9 cm) in the girls and 145.22 cm (±7.1 cm) in the boys, as well as mean body weight of 38.93 kg (±6.9 kg) and 40.8 kg (±6.7 kg) in the girls and the boys, respectively. The exclusion criteria in both groups included the occurrence of neural and orthopedic diseases which affect body posture.
Objective measurement of spinal curvatures
The examinations were carried out in the free or the so-called habitual standing posture, with no shoes; lower limbs straightened to the width defined by the hips, upper limbs positioned freely alongside the torso. If during an assessment a participant deliberately straightened up, the measurement was repeated.
In 1959, the examinations were carried out following the detailed instructions specified by N. Wolański and M. Rudolf-Sokttowska in cooperation with physician M. Demel and were related to “General data and history” as well as “Health” [29,30]. The assessment focused on general health conditions and on measurements of body parts, using Martin-Saller’s method and various instruments; however, the present analyses took into account only those measurements which related to body height, body mass, and spinal curvatures. Body height was measured with a stadiometer connected to weighing scales (typical equipment used by doctors in Poland at that time). Intervals of 0.5 cm and 0.1 kg were used in recording the height and the weight, respectively. During the examination the participants were in their underwear only. The same methodological rules were applied during all examinations [29,30].
The specific elements of the standing body posture were evaluated using a type II spherodorsimeter designed by Wolański. Its components included: a frame with a vertical element carrying upper, middle and lower pin; central and median slide bar; upper, middle and lower bridge; stabilizer and the base. The ordinates were identified for the main points and intermediate points marked in the areas of the spinous process, in the standing position. In fact, these were the same points in which partial angles were later determined using the photogrammetric method. The subsequent part, necessary for acquiring the final measurements, involved mathematical operations and did not require the participants to be present.
The results of these measurements were used to calculate the inclination angle of the different sections of the trunk, by applying tangents of each angle and reading the inclination angle values from tables. As a result of these mathematical transformations the specific angles corresponded with those determined using the photogrammetric method. These angles represented the following parameters: alpha was inclination of the sacral bone; beta was thoracolumbar transition; and gamma was inclination of the upper thoracic spine (Figure 1A) [30]. Usefulness of the spherodorsimeter was validated by studies focusing on types of body posture in individuals living in Poland in the 1960s [29].
Figure 1.
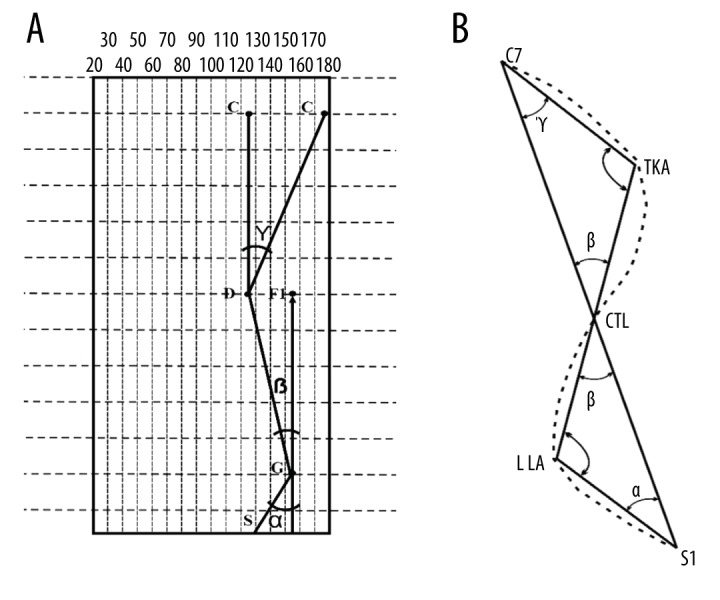
Diagram of spinal curvatures measured using (A) spherodorsimeter and (B) photogrammetry. C/C7 – spinous process of the 7th cervical vertebra; S/S1 – spinous process of the 1st sacral vertebra; (C – D – G)/(C7 – TKA – CTL) – thoracic kyphosis; D/TKA – angle of thoracic kyphosis; G/CLT – lordosis transition into kyphosis (D – G – S1)/(CTL – LLA – S1) – lumbar lordosis; LLA – angle of lumbar lordosis; α – alpha angle (sacral inclination angle); β – beta angle (inclination angle of the thoracolumbar spine); γ – gamma angle (inclination angle of the upper thoracic spine).
The 2003 examination was performed with equipment designed for computer-aided evaluation of body posture and using the projection Moiré phenomenon, now commonly employed in screening diagnostics [31,32], and facilitating accurate and reliable quantitative assessment of numerous parameters, both in sagittal and frontal plane [33]. To ensure appropriate accuracy, the examinations were conducted in conformity with generally accepted standards [15,17,18,31–36]. It was possible to obtain a 3-dimensional image by displaying lines with specific parameters on a child’s back. The lines projected onto the skin were deformed according to the surface configuration, and these deformations in the line images were then transformed into a numerical algorithm in a form of a contour map of the examined surface. This image of the surface of the back allowed for a multifaceted interpretation of body posture and enabled calculation of the following angles: alpha was sacral inclination, beta was thoracolumbar transition, and gamma was inclination of the upper thoracic spine (Figure 1B) [35,36]. These scores were compared with the results of the 1959 examination.
Despite the essential differences, these 2 methods enable assessment of specific spinal segments for their angles of inclination from vertical alignment with the use of a similar approach to spinal geometry measurement. Therefore, it seems possible to perform comparative analyses of these measurements conducted independently in different facilities. In both methods, greater partial angles meant greater inclination of the relevant spine section. The angles of lumbar lordosis (LLA) and thoracic kyphosis (TKA) were calculated according to the following formula: TKA=180 – (beta + gamma), LLA=180 – (alpha + beta), which means that the lower the value of the angle, the deeper the curvature, and the higher the value of the angle, the more reduced the curvature.
Statistical analysis
A statistical analysis of the results was carried out using Statistica 12.5. During the process, the results of the measurements performed in 2003 and in 1959 were examined for significant differences; the reverse marking of the angles in each method was taken into account. A lack of correspondence between the distribution of features and a normal distribution, identified with the Shapiro-Wilk test, was then examined using a parametric Student’s t-test and non-parametric Mann-Whitney U test. Statistical significance was assumed at P < 0.05.
Results
The mean values of the specific partial angles in the spinal curvatures, relative to age, gender, and timing of the measurement, are shown in Figures 2–4, and the mean values of LLA and TKA are presented in Figures 5 and 6.
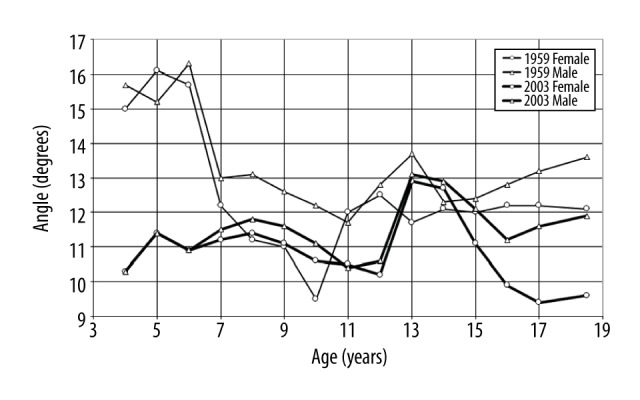
Figure 2.
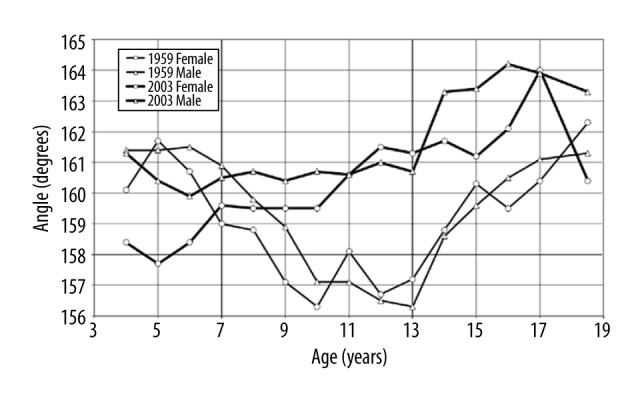
Mean inclination of sacral bone (alpha angle) relative to age, gender, and timing of measurement.
Figure 3.
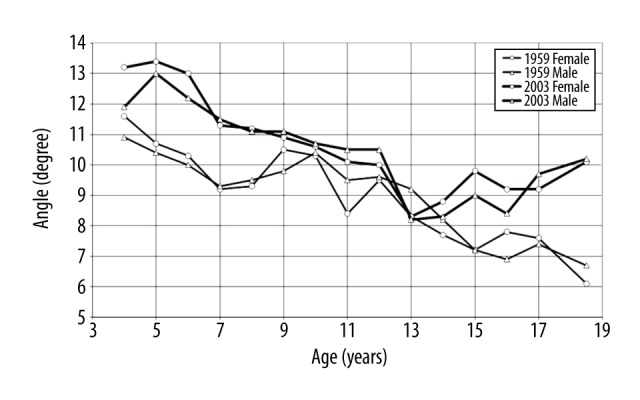
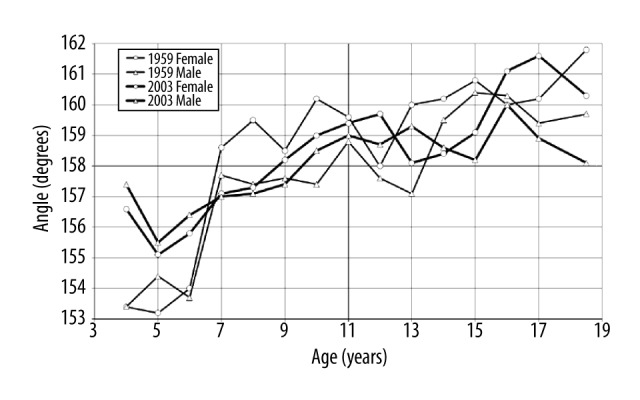
Mean inclination of thoracolumbar transition (beta angle) relative to age, gender, and timing of measurement.
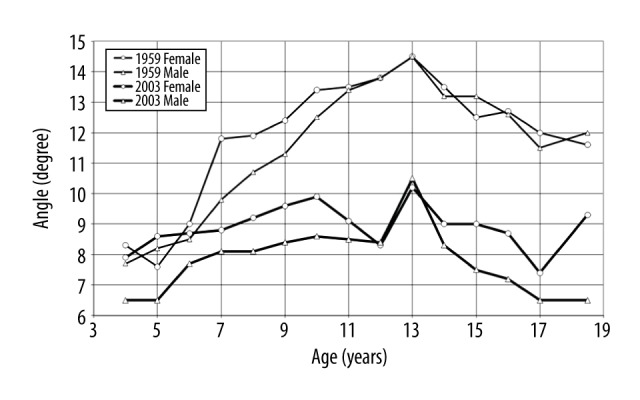
Figure 4.
Mean inclination of upper thoracic section (gamma angle) relative to age, gender, and timing of measurement.
Figure 5.
Mean angle of lumbar lordosis (LLA) relative to age, gender, and timing of measurement.
Figure 6.
Mean angle of thoracic kyphosis (TKA) relative to age, gender, and timing of measurement.
Comparative analyses of the differences between the mean measures from 1959 (SG-1959) and 2003 (CG-2003), related to partial angles of physiological curvatures of the spine, showed that generally the mean alpha and gamma angles in SG-1959 assumed greater values. This shows that the latter children, both the girls and the boys, presented with greater inclination angles of the sacral bone and the upper thoracic section than their peers from CG-2003 (Tables 1, 2).
Table 1.
Significance of the differences between the alpha, beta and gamma angles in boys in 1959 and 2003.
| Age | Alpha angle | Beta angle | Gamma angle | |||
|---|---|---|---|---|---|---|
| Mean difference between 2003 and 1959 | Mann-Whitney Z/p-value* | Mean difference between 2003 and 1959 | Mann-Whitney Z/p-value* | Mean difference between 2003 and 1959 | Mann-Whitney Z/p-value* | |
| Male | ||||||
| 4 | −1.2 | 0.0005* | 1 | 0.007* | −5.4 | 1.68 |
| 5 | −1.7 | 1.39 | 2.6 | 1.86 | −3.8 | 1.86 |
| 6 | −0.8 | 0.02 | 2.2 | 2.95 | −5.4 | 1.45 |
| 7 | −1.7 | 1.01 | 2.2 | 8.96 | −1.5 | 4.85 |
| 8 | −2.6 | 3.45 | 1.6 | 6.61 | −1.3 | 1.32 |
| 9 | −2.9 | 4.48 | 1.3 | 0.0001* | −1 | 6.26 |
| 10 | −3.9 | 1.67 | 0.3 | 0.41 | −1.1 | 6.72 |
| 11 | −4.9 | 2.28 | 1 | 0.002* | −1.3 | 1.31 |
| 12 | −5.4 | 1.51 | 0.9 | 0.009* | −2.2 | 1.31 |
| 13 | −4 | 7.21 | 1 | 0.002* | −0.6 | 1.15 |
| 14 | −4.9 | 3.88 | 0.1 | 0.76 | 0.6 | 2.09 |
| 15 | −5.7 | 9.57 | 1.8 | 1.91 | −0.3 | 3.88 |
| 16 | −5.4 | 6.89 | 1.5 | 3.14 | −1.6 | 2.37 |
| 17 | −5 | 6.81 | 2.3 | 9.88 | −1.6 | 2.53 |
| 18.5 | −5.5 | 6.95 | 3.5 | 2.03 | −1.7 | 1.4 |
Significance at p<0.05.
Table 2.
Significance of the differences between the alpha, beta and gamma angles in girls in 1959 and 2003.
| Age | Alpha angle | Beta angle | Gamma angle | |||
|---|---|---|---|---|---|---|
| Mean difference between 2003 and 1959 | Mann-Whitney Z/p-value* | Mean difference between 2003 and 1959 | Mann-Whitney Z/p-value* | Mean difference between 2003 and 1959 | Mann-Whitney Z/p-value* | |
| Female | ||||||
| 4 | −0.4 | 0.0007* | 1.6 | 0.0001* | −4.7 | 5.81 |
| 5 | 1 | 0.0004* | 2.7 | 1.27 | −4.7 | 1.01 |
| 6 | −0.3 | 0.0002* | 2.7 | 2.03 | −4.8 | 4.5 |
| 7 | −3 | 9.50 | 2.1 | 3.52 | −1 | 0.006* |
| 8 | −2.7 | 6.66 | 1.9 | 1.11 | 0.2 | 0.59 |
| 9 | −2.8 | 3.81 | 0.4 | 0.25 | 0.1 | 0.77 |
| 10 | −3.5 | 2.40 | 0.3 | 0.4 | 1.1 | 0.001* |
| 11 | −4.4 | 1.94 | 1.7 | 5.06 | −1.5 | 9.2 |
| 12 | −5.5 | 5.73 | 0.5 | 0.16 | −2.3 | 1.49 |
| 13 | −4.3 | 1.68 | 0 | 1.00 | 1.2 | 0.001* |
| 14 | −4.5 | 1.06 | 1.1 | 0.0005* | 0.6 | 0.12 |
| 15 | −3.5 | 3.42 | 2.6 | 2.01 | −0.9 | 0.02* |
| 16 | −4 | 3.78 | 1.4 | 5.84 | −2.3 | 9.93 |
| 17 | −4.6 | 1.61 | 1.6 | 2.04 | −2.8 | 5.13 |
| 18.5 | −2.3 | 3.03 | 4 | 1.51 | −2.5 | 1.69 |
Significance at p<0.05.
Statistically significant differences between the groups were observed in boys aged 4, 9, 11, and 13 (Table 1) and girls aged 4–7 and 10, 13, and 14 (Table 2). Differences in the alpha angle were observed in 4-year-old boys and 4–5-year-old girls. The mean values of sacral inclination were lower in CG-2003. The analysis of the mean beta angle values revealed significant differences in boys aged 4, 9, 11, and 13, and in 4- and 14-year-old girls. Mean values of the beta angle were higher in CG-2003. No significant differences in gamma angles were observed in boys (Table 1), however, girls aged 7, 10, and 11 years were found to differ considerably (Table 2), with higher mean values in CG-2003.
Analysis of the differences between mean LLA and TKA values showed that LLA was greater in most age groups and TKA was partly greater in some age groups in SG-1959 compared to CG-2003 (Table 3).
Table 3.
Significance of the differences between the angles of thoracic kyphosis (TKA) and lumbar lordosis (LLA) in boys and girls, in 1959 and 2003.
| Males | Females | |||||||
|---|---|---|---|---|---|---|---|---|
| Age | TKA | LLA | TKA | LLA | ||||
| Mean difference between 2003 and 1959 | Mann-Whitney Z/p-value* | Mean difference between 2003 and 1959 | Mann-Whitney Z/p-value* | Mean difference between 2003 and 1959 | Mann-Whitney Z/p-value* | Mean difference between 2003 and 1959 | Mann-Whitney Z/p-value* | |
| 4 | 4 | 0.01* | −0.1 | 0.93 | 3.2 | 0.01* | −1.7 | 0.2 |
| 5 | 1.1 | 0.37 | −1 | 0.43 | 1.9 | 0.12 | −4 | 0.004* |
| 6 | 2.7 | 0.03* | −1.6 | 0.2 | 1.8 | 0.13 | −2.3 | 0.006* |
| 7 | −0.7 | 0.52 | −0.4 | 0.72 | −1.5 | 0.16 | 0.6 | 0.60 |
| 8 | −0.3 | 0.8 | 0.9 | 0.47 | −2.2 | 0.07 | 0.7 | 0.57 |
| 9 | −0.2 | 0.86 | 1.5 | 0.19 | −0.3 | 0.80 | 2.4 | 0.04* |
| 10 | 1.1 | 0.38 | 3.6 | 0.004* | −1.2 | 0.32 | 3.2 | 0.008* |
| 11 | 0.2 | 0.85 | 3.5 | 0.001* | −0.2 | 0.87 | 2.5 | 0.04* |
| 12 | 1.1 | 0.31 | 4.5 | 0.0001* | 1.7 | 0.18 | 4.8 | 0.0002* |
| 13 | 2.2 | 0.07 | 4.4 | 0.0003* | −1.9 | 0.13 | 4.1 | 0.001* |
| 14 | −0.9 | 0.48 | 4.7 | 0.0003* | −1.8 | 0.10 | 2.9 | 0.02* |
| 15 | −2.2 | 0.08 | 3.8 | 0.0003* | −1.7 | 0.18 | 0.9 | 0.48 |
| 16 | −0.3 | 0.8 | 3.7 | 0.0003* | 1.1 | 0.39 | 2.6 | 0.04* |
| 17 | −0.5 | 0.69 | 2.8 | 0.03* | 1.4 | 0.27 | 3.6 | 0.005* |
| 18.5 | −1.6 | 0.29 | 2 | 0.19 | −1.5 | 0.36 | −1.9 | 0.25 |
Significance at p<0.05.
A lower value of the angle corresponds with a deeper curvature, and a higher value of the angle reflects a more reduced curvature.
The TKA in boys differed significantly between the groups at 4 and 6 years of age, and in girls only at 4 years of age, with higher mean values in CG-2003 representing reduced TKA in this group. A significant reduction in LLA was observed in CG-2003, compared to SG-1959; more specifically the values of the LLA in boys differed between the groups aged 10–17 years and in girls at 5–6, 9–14, and 15–17 years of age, assuming higher mean values in CG-2003, which is evidence of reduced lumbar lordosis (Table 3).
Mean values of body weight and height relative to gender, age, and timing of measurement are shown in Figures 7 and 8. The findings show greater mean values of body weight and height in all the age groups, irrespective of sex, in CG–2003.
Figure 7.
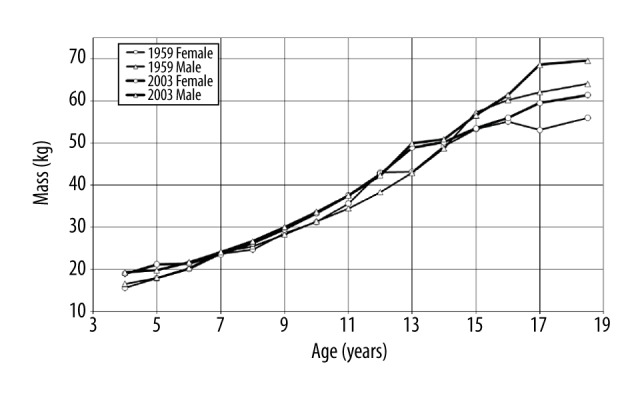
Mean values of body mass relative to age, gender, and timing of measurement.
Figure 8.
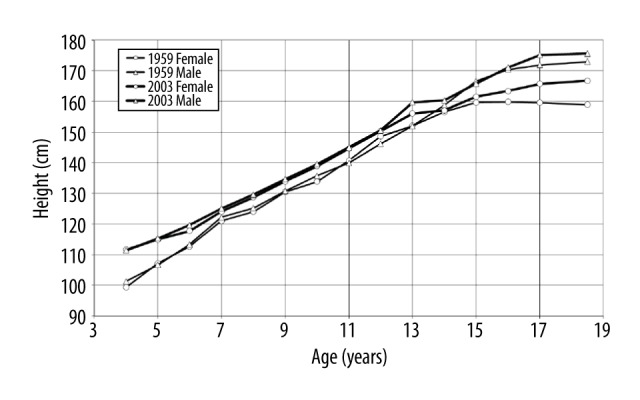
Mean values of body height relative to age, gender, and timing of measurement.
Regarding somatic characteristics, significant differences between the groups were observed in body mass in boys aged 5–6, 8–10 and 14 years, and in girls aged 5–6 and 8–11 years. The analysis of the body height measurements revealed significant differences between boys aged 7–10, 12, and 17–18 years, and girls aged 7, 9, 11, 13, and 16 years. Higher mean values of the relevant parameters were recorded in the CG-2003 measurements (Table 4).
Table 4.
Significance of the differences between the height and weight of boys and girls, in 1959 and 2003.
| Males | Females | |||||||
|---|---|---|---|---|---|---|---|---|
| Age | Mass | Height | Mass | Height | ||||
| Mean difference between 2003 and 1959 | Student’s t-test/ p-value* | Mean difference between 2003 and 1959 | Student’s t-test/ p-value* | Mean difference between 2003 and 1959 | Student’s t-test/ p-value* | Mean difference between 2003 and 1959 | Student’s t-test/ p-value* | |
| 4 | 2.8 | 2.39 | 10.1 | 1.03 | 3.4 | 4.80 | 12.4 | 1.89 |
| 5 | 1.8 | 0.0001* | 8.6 | 5.82 | 3.3 | 0.01 | 7.8 | 5.37 |
| 6 | 1.4 | 0.005* | 6.4 | 1.29 | 1.4 | 0.004 | 5.0 | 3.59 |
| 7 | 0.0 | 0.93 | 2.8 | 0.004* | −0.1 | 0.80 | 3.1 | 0.002* |
| 8 | 1.2 | 0.02 | 4.3 | 0.0001* | 1.5 | 0.004* | 4.7 | 3.54 |
| 9 | 1.7 | 0.001* | 3.9 | 0.0003* | 1.0 | 0.007* | 3.5 | 0.001* |
| 10 | 2.2 | 0.0002* | 3.8 | 0.001* | 2.1 | 0.004* | 5.1 | 9.75 |
| 11 | 3.1 | 6.66 | 5.1 | 2.32 | 2.0 | 0.001* | 3.9 | 0.001 |
| 12 | 3.9 | 2.48 | 4.3 | 0.0002* | −0.4 | 0.60 | 1.8 | 0.16 |
| 13 | 7.0 | 1.41 | 7.7 | 2.2 | 5.7 | 1.59 | 4.0 | 0.001* |
| 14 | 2.2 | 0.006* | 1.6 | 0.23 | 0.9 | 0.24 | 0.6 | 0.66 |
| 15 | −0.7 | 0.4 | −0.8 | 0.55 | 0.2 | 0.81 | 1.9 | 0.15 |
| 16 | 1.2 | 0.12 | 0.7 | 0.44 | 0.9 | 0.26 | 3.6 | 0.006* |
| 17 | 6.5 | 6.71 | 3.2 | 0.01* | 6.4 | 1.53 | 6.1 | 3.92 |
| 18.5 | 5.6 | 2.97 | 2.6 | 0.02* | 5.4 | 7.62 | 7.8 | 8.27 |
Significance at p<0.05.
Discussion
Nowadays, more and more studies focus on assessing body posture with the use of objective measuring methods [37–39], which in the 1960s was a rarity [29]. There are numerous publications reporting assessments of body posture in various populations [40,41], or discussing the relationship between environmental factors and the shape of the spine [12–20]. Yet, no research has focused on the links between the shape of the spine and time-related changes, indirectly reflecting environmental impacts. Studies investigating time-related changes in the human body provide a great deal of information about the impact of the changing environment on the body [42]. The pattern of somatic development is linked with genetic determinants as well as with environmental modifiers, such as postural habits, lifestyle, and conditions of work and leisure, therefore understanding the effects of the changing environmental impacts in somatic development of children and adolescents is of great importance. This observation provided motivation for the present study.
The present findings acquired during comparative analysis of measurements involving 2 groups of children and performed in 1959 and in 2003. The study results showed that over the years, changes occurred in front and back spinal curvatures, towards a reduction in the LLA, along with an increase in body weight and mass, particularly before pubertal growth spurt. Conversely, the present study showed that the changing living conditions did not significantly affect the shape of the thoracic spine kyphosis in Polish children and adolescents. Analysis of the specific angles, i.e., alpha angle (sacral bone inclination); beta angle (inclination angle of the thoracolumbar spine); and gamma angle (inclination angle of the upper thoracic spine) in the 2 groups showed significantly reduced inclination angle of the lumbosacral spine in the group examined in 2003, both in the boys and in the girls. The aforementioned changes showed a trend reflected by a decrease in the size of lumbar lordosis and a more vertical position of the sacral bone, compared to the participants examined in 1959. Our study also showed an increase in body mass and height in the study group examined in 2003, compared to the children examined in 1959.
The presence of significant differences in lumbar lordosis and in sacral inclination in the relevant groups can be explained by modifications in the lifestyles of post-war generations in Poland. Progress of civilization and advancements in engineering and automotive sectors contribute to changes in lifestyle, from active to sedentary [43], which is of great significance for the spine [44]. The present findings provide evidence reflecting sensitivity of lumbar lordosis and sacral inclination, as well as body height and mass to time-related changes in environmental factors.
Understanding the patterns of variation in sagittal alignment may help to discover the association between spinal shape and the development of degenerative changes in the spine. A decrease in sacral inclination over the years, identified by the present study, may explain the greater incidence of lower back pain observed nowadays in comparison to the 1960s, as reported by other researchers [45]. This is also consistent with a study by Ergun et al. [46], where decreased sacral inclination was linked to greater disc degeneration, and with other reports suggesting increased incidence of spinal pain [47].
The shape of spinal curvatures appears to be affected by such external factors as: carrying heavy school backpacks [19], sitting patterns [48], and exercise of one’s choice [14–17].
Walicka-Cupryś et al. assessed correlations between the weight of a child’s backpack, their body mass, and certain features of their body posture. The study group consisted of 109 7-year old children. The parameters of body posture were determined using the Zebris Ultrasonic System. The researchers determined that wearing a backpack heavier than 10% of one’s body weight can cause shallowing of the lumbar lordosis and a tendency towards a vertical position of the sacrum [19].
A study by Barczyk-Pawelec et al. reported higher incidence of kyphotic postures and a lower value of alpha angle (sacral inclination in relation to the vertical alignment) in table tennis players, compared to their non-player peers [17]. Muyor et al. [11] showed no relationship between tennis playing and the shape of anteroposterior spine curvatures. Grabara and Hadzik, in 2009 observed asymmetries brought about by unilateral loads as well as a progressive thoracic kyphosis and a flattened lumbar lordosis in adolescent female volleyball players [49]. Other researchers examined a group of 42 divers and found that the study group presented significantly higher values of the parameters reflecting inclination of the thoracolumbar section of the spine (P=0.0000) and length of thoracic kyphosis (P=0.000), and lower values of the length of lumbar lordosis (P=0.0163). In comparison to the controls, the study group demonstrated more pronounced curvature of thoracic kyphosis P=0.0006) and lumbar lordosis (P=0.0235) [15]. Grabara found significantly lower angular values of lumbar lordosis in young football players, compared to their untrained peers [50].
A study by Drzat-Grabiec et al. involving 91 children aged 11–13 years old, investigated changes in spine curvatures as a result of a different body posture, and found that a sedentary position greatly affects the shape of lumbar lordosis towards its reduction [48]. According to the current study, lumbar lordosis is not only reduced temporarily as a result of sitting but is also reduced permanently over several generations. Introduction of mandatory kindergarten education in Poland in the 1990s may have contributed to this situation by reducing children’s playtime and compelling them to use sedentary positions.
Reduced lordosis may lead to more frequent back pains [51]. Results of studies focusing on the impact of sedentary position on back pain do not provide explicit evidence. Some authors claim that back pain is reduced through sitting [52], while others argue that sedentary position is a cause of back pain [51]. The reduction in lumbar spine lordosis over the years, identified by the current study, may explain the higher incidence of back pain in contemporary populations [39], which corresponds with the contribution of reduced lumbar lordosis to intervertebral disk degeneration [53]. Other scientists have not found any differences in the size of lumbar spine in individuals with back pain [44], or individuals involved in specific types of motor activity [13]. Frequently observed differences in sacral inclination and lumbar lordosis angles among girls are correlated with increased incidence of postures with impaired statics between 7 and 12 years of age, these being particularly hazardous for correct body posture. This increase has been identified in studies conducted by other authors [54]. The degree of inclination in both the upper thoracic section and thoracolumbar transition correlates with scoliosis, or the so-called dowager’s hump [55,56]. The decrease in the parameters of thoracic kyphosis and inclination of the upper thoracic section over the years, identified by the present study, should be taken into account in analyses focusing on the incidence of scoliosis over the years.
Different lifestyles in 1959 and 2003 must not be overlooked as factors possibly contributing to reduced LLA. This suggests a direction of changes which should be introduced in order to decrease the incidence of back pains.
Body height and weight are among other features showing a tendency for change depending on living conditions. Acceleration in growth and body mass depends on well-being and on eating habits, which is typical of highly affluent countries [57]. The authors’ own studies have revealed a significant increase in body weight and height between generations. Considerable differences in somatic characteristics, particularly during prepubertal period, result from better nutrition and a more diversified diet, as well as limited physical activity [58,59]. In 2004 Fus and Gworys made an attempt to identify variability of the growth process and the age at which growth stops, based on selected somatic features. They compared measurements of body mass and height taken in 1988 and 2003 in a population of 9919 children and adolescents aged 9 to 23 years old, living in the Podkarpackie and Kujawsko-Pomorskie regions in Poland. It was established that essential growth in body height and in most somatometric features ended in the relevant population at the age of 16–18 years old. Body weight was the last parameter to be stabilized. An increase in the somatometric characteristics after the age of 18 years old and other related changes in body proportions were only minor [26]. The results of the study correspond to the trends identified in the current work. Another study conducted in Poland, more specifically in the city of Poznań, focused on changes in body weight and height in course of 100 years and identified periods of acceleration and stabilization in the growth of these characteristics, which supports the present findings showing increase in body height and mass over a period of 40 years [7].
In another study, Suder et al. investigated secular trends in body mass index (BMI) and waist circumference (WC) in Polish school children examined over a period of almost 50 years. The data related to body height, weight, and WC came from 4 cross-sectional surveys conducted in Poland between 1966 and 2012, involving 34 005 boys and 34 008 girls. In this study, abdominal obesity in Polish children increased significantly from 1966 to 2012, with a tendency reflecting a greater increase in the rates of children with central rather than overall obesity [27]. Based on the analysis of our findings and those reported by other authors, related to increase in body mass, it can be assumed that the number of metabolic complications in Polish children and adolescents may intensify in the future.
Furthermore, a study conducted in Russia, in the Nizhniy Novgorod region, by Kuzmichyov et al. (2014) reviewed measurements from 1946–2012, related to body length and mass in children and adolescents aged 7–17 years old, and identified quantitative and qualitative changes in these characteristics across the entire age range, which led the authors to the conclusion that children born at the start of the 21st century develop faster, on average by 2–3 years [8]. Another study conducted in Russia showed changes towards increased body height in a period of 115 years, yet during the most recent 15 years, no further changes in body weight and height were identified, which suggests stabilization in the growth of these characteristics [28]. A study by Ji et al. reported that in China positive changes had occurred in the characteristics of body mass and height in a period of 5 decades, and the authors drew a conclusion that the fact was linked with improved socioeconomic conditions [9].
These aforementioned studies suggest that secular growth trends partly depend on the region of the world and on environmental factors. During one’s physical development the spinal curvatures evolve, and the process is affected by frequently assumed body postures as well as activity in one’s daily life and these factors are likely to alter the spinal morphology.
The value of the research
This study confirms that changes in spine dimensions, such as body height and spinal curvatures, took place over a 40-year-period. These findings can be used by institutions in establishing guidelines for medical staff evaluating anthropometric characteristics of their patients, and for biomechanical computer modelling of spine growth and development. They also suggest it is necessary to constantly adapt industrial designs to changing secular trends.
Limitations of the research
Certain limitations of the study should to be taken into account. Despite the fact that the tools used in both examinations produced comparable measurements from the viewpoint of the study method, yet the different degree of engineering advancement in the design of the tools must not be overlooked.
Conclusions
The values for lumbar lordosis angle and sacral inclination decreased in girls and in boys over the 40-year study period. The values of the angle of thoracic kyphosis and partial angles of physiological spine curvatures reveal minor changes in boys and moderate changes in girls. Over a 40-year period, there was a significant change in body height and mass, particularly in prepubertal children. The results of this study demonstrating a change in the physiological spinal curvatures over 40 years should be taken into consideration, for instance by public healthcare services in developing their evaluation standards as well as in designing guidelines for standard height of furniture, profiling of chairs, car seats, as well as other devices where body height and shape of the spine are an important matter.
Acknowledgements
We would like to express our gratitude to Professor Napoleon Wolański for sharing his source materials.
Footnotes
Conflict of interests
None.
Source of support: Self financing
References
- 1.Ranavolo A, Don R, Draicchio F, et al. Modelling the spine as a deformable body: Feasibility of reconstruction using an optoelectronic system. Appl Rrgon. 2013;44(2):192–99. doi: 10.1016/j.apergo.2012.07.004. [DOI] [PubMed] [Google Scholar]
- 2.Dubousset J. Three-dimensional analysis of the scoliotic deformity. In: Weinstein SL, editor. The Pediatric Spine: Principles and practice. New York: Raven Press; 1994. [Google Scholar]
- 3.Reinders I, van Schoor NM, Deeg DJH, et al. Trends in lifestyle among three cohorts of adults aged 55–64 years in 1992/1993, 2002/2003 and 2012/2013. Eur J Public Health. 2017 doi: 10.1093/eurpub/ckx173. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 4.Saunders TJ, Gray CE, Poitras VJ, et al. Combinations of physical activity, sedentary behaviour and sleep: Relationships with health in children and youth. Med Sci Sports Exerc. 2016;48(5 Suppl 1):912. doi: 10.1139/apnm-2015-0626. [DOI] [PubMed] [Google Scholar]
- 5.Tanner JM. Growth as a measure of the nutritional and hygienic status of a population. Horm Res. 1992;38(Suppl 1):106–15. doi: 10.1159/000182580. [DOI] [PubMed] [Google Scholar]
- 6.Cole TJ. Secular trends in growth. Proc Nutr Soc. 2000;59:317–24. doi: 10.1017/s0029665100000355. [DOI] [PubMed] [Google Scholar]
- 7.Krawczynski M, Walkowiak J, Krzyzaniak A. Secular changes in body height and weight in children and adolescents in Poznan, Poland, between 1880 and 2000. Acta Paediatr. 2003;92:277–82. doi: 10.1080/08035250310009176. [DOI] [PubMed] [Google Scholar]
- 8.Kuzmichyov YG, Kaliuzhniy YA, Mikhailova SV, et al. Dynamics of indices of body length and mass in rural schoolchildren in Nizhniy Novgorod region. Morfologiia. 2015;147(3):32–36. [PubMed] [Google Scholar]
- 9.Ji Ch, Chen TJ. Secular changes in stature and body mass index for Chinese youth in sixteen major cities, 1950s–2005. Am J Hum Biol. 2008;20:530–37. doi: 10.1002/ajhb.20770. [DOI] [PubMed] [Google Scholar]
- 10.McCarthy HD, Cole TJ, Fry T, et al. Body fat reference curves for children. Int J Obes. 2006;30(4):598–602. doi: 10.1038/sj.ijo.0803232. [DOI] [PubMed] [Google Scholar]
- 11.Drzał-Grabiec J, Walicka-Cupryś K, Truszczyńska A. The influence of applied research methods on the frequency of the appearance of abnormal spinal curvatures. Advances in Rehabilitation. 2013;27(4):41–46. [Google Scholar]
- 12.Cil A, Yazici M, Uzumcugil A, et al. The evolution of sagittal segmental alignment of the spine during childhood. Spine (Phila Pa 1976) 2005;1:93–100. [PubMed] [Google Scholar]
- 13.Glista J, Pop T, Weres A, et al. Change in anthropometric parameters of the posture of students of physiotherapy after three years of professional training. Biomed Res Int. 2014;2014:719837. doi: 10.1155/2014/719837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Muyor JM, Sánchez-Sánchez E, Sanz-Rivas D, López-Miñarro PA. Sagittal spinal morphology in highly trained adolescent tennis players. J Sports Sci Med. 2013;12(3):588–93. [PMC free article] [PubMed] [Google Scholar]
- 15.Drzał-Grabiec J, Puszczałowska-Lizis E. Analysis of selected parameters of body posture in novice divers. Polish J Sport Med. 2014;30:103–11. [Google Scholar]
- 16.Muyor JM, Lopez-Minarro PA, Alacid F. Sagittal spinal curvatures and pelvic tilt in cyclists. J Sports Sci Med. 2011;10(2):355–61. [PMC free article] [PubMed] [Google Scholar]
- 17.Barczyk-Pawelec K, Bańkosz Z, Derlich M. Body postures and asymmetries in frontal and transverse planes in the trunk area in table tennis players. Biol Sport. 2012;29:129–34. [Google Scholar]
- 18.Grabara M, Pstrągowska D. [Assessment of body posture in boys and girls in the light of relative body mass index (BMI)]. Polish J Sport Med. 2008;24:231–39. [in Polish] [Google Scholar]
- 19.Walicka-Cupryś K, Skalska-Izdebska R, Rachwał M, Aleksandra T. Influence of the weight of a school backpack on spinal curvature in the sagittal plane of seven-year-old children. BioMed Res Int. 2015;2015:817913. doi: 10.1155/2015/817913. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Astfalck RG, O’Sullivan P, Straker LM, et al. Sitting postures and trunk muscle activity in adolescent with and without nonspecific chronic low back pain. Spine. 2010;35:1387–95. doi: 10.1097/BRS.0b013e3181bd3ea6. [DOI] [PubMed] [Google Scholar]
- 21.Czaprowski D, Pawłowska P, Kolwicz-Gańko A, et al. The influence of the “straighten your back” command on the sagittal spinal curvatures in children with generalized joint hypermobility. BioMed Res Int. 2017;2017:9724021. doi: 10.1155/2017/9724021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kim JH, Park JY, Yi S, et al. Anterior cervical discectomy and fusion alters whole-spine sagittal alignment. Yonsei Med J. 2015;56:1060–70. doi: 10.3349/ymj.2015.56.4.1060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Segal M. Changing views of Cajal’s neuron: The case of the dendritic spine. Prog Brain Res. 2002;136:101–7. doi: 10.1016/s0079-6123(02)36011-4. [DOI] [PubMed] [Google Scholar]
- 24.Keorochana G, Taghavi CE, Lee KB, et al. Effect of sagittal alignment on kinematic changes and degree of disc degeneration in the lumbar spine: an analysis using positional MRI. Spine. 2011;36:893–98. doi: 10.1097/BRS.0b013e3181f4d212. [DOI] [PubMed] [Google Scholar]
- 25.Suder A, Gomula A, Koziel S. Central overweight and obesity in Polish schoolchildren aged 7–18 years: Secular changes of waist circumference between 1966 and 2012. Eur J Pediatr. 2017;176(7):909–16. doi: 10.1007/s00431-017-2938-4. [DOI] [PubMed] [Google Scholar]
- 26.Fus D, Gworys B. [An attempt to determine the variability of juvenescence process and the age of puberty termination]. Scientific review of physical culture of University of Rzeszow. 2004;(1–2):23–36. [in Polish] [Google Scholar]
- 27.Suder A, Gomula A, Koziel S. Central overweight and obesity in Polish schoolchildren aged 7–18 years: Secular changes of waist circumference between 1966 and 2012. Eur J Pediatr. 2017;176(7):909–16. doi: 10.1007/s00431-017-2938-4. [DOI] [PubMed] [Google Scholar]
- 28.Matveeva NA, Emel’ianova NN, Bogomolova ES, Rodionov VA. Dynamics of physical development of Chuvash rural school children 1884–1999. Gig Sanit. 2001;(3):64–67. [PubMed] [Google Scholar]
- 29.Wolański N. [Research into development of body posture in urban children and adolescents. Surgery of Motor Systems and Polish Orthopedics]. Chirurgia narządu ruchu i ortopedia polska XXVI. 1961;2:175–91. [in Polish] [PubMed] [Google Scholar]
- 30.Wolański N. [Spherodorsimeter – proprietary device for spatial measurements of spine]. Scientific Publication of the Jagiellonian University, Zoology. 1957;10(1):241. [in Polish] [Google Scholar]
- 31.Drzał-Grabiec J, Szczepanowska-Wołowiec B. Weight-height ratios and parameters of body posture in 7–9-yearolds with particular posture types. Ortop Traumatol Rehabil. 2011;13:591–600. doi: 10.5604/15093492.971044. [DOI] [PubMed] [Google Scholar]
- 32.Grabara M. Comparison of the posture between young female handball players and non-training peers. J Back Musculoskelet Rehabil. 2014;27:85–92. doi: 10.3233/BMR-130423. [DOI] [PubMed] [Google Scholar]
- 33.Saad KR, Colombo AS, Ribeiro AP, João SAM. Reliability of photogrammetry in the evaluation of the postural aspects of individuals with structural scoliosis. J Bodyw Mov Ther. 2012;2:210–16. doi: 10.1016/j.jbmt.2011.03.005. [DOI] [PubMed] [Google Scholar]
- 34.Porto F, Gurgel JL, Russomano T, de Farinatti PT. Moiré topography: Characteristics and clinical application. Gait Posture. 2010;32(3):422–24. doi: 10.1016/j.gaitpost.2010.06.017. [DOI] [PubMed] [Google Scholar]
- 35.Mrozkowiak M, Strzecha M. [Projection moiré as a modern tool for diagnosis of body posture]. Kraków, Antropomotoryka. 2012;22(60):33–49. [in Polish] [Google Scholar]
- 36.Drzał-Grabiec J, Snela S. The influence of rural environment on body posture. Ann Agr Env Med. 2012;19(4):846–50. [PubMed] [Google Scholar]
- 37.D’Amico M, Kinel E, Roncoletta P. Normative 3D opto-electronic stereo-photogrammetric posture and spine morphology data in young healthy adult population. PLoS One. 2017;12(6):e0179619. doi: 10.1371/journal.pone.0179619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Walicka-Cupryś K, Wyszyńska J, Podgórska-Bednarz J. Concurrent validity of photogrammetric and inclinometric techniques based on assessment of anteroposterior spinal curvatures. Eur Spine J. 2017 doi: 10.1007/s00586-017-5409-8. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 39.Dolphens M, Vleeming A, Castelein R, et al. Coronal plane trunk asymmetry is associated with whole-body sagittal alignment in healthy young adolescents before pubertal peak growth. Eur Spine J. 2017 doi: 10.1007/s00586-017-5156-x. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 40.Asai Y, Tsutsui S, Oka H, et al. Sagittal spino-pelvic alignment in adults: The Wakayama Spine Study. PLoS One. 2017;12(6):e0178697. doi: 10.1371/journal.pone.0178697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Dolphens M, Cagnie B, Coorevits P, et al. Sagittal standing posture and its association with spinal pain: A school-based epidemiological study of 1196 Flemish adolescents before age at peak height velocity. Spine. 2012;37:1657–66. doi: 10.1097/BRS.0b013e3182408053. [DOI] [PubMed] [Google Scholar]
- 42.Cil A, Yazici M, Uzumcugil A, et al. The evolution of sagittal segmental alignment of the spine during childhood. Spine. 2005;30:93–100. [PubMed] [Google Scholar]
- 43.Cooper AR, Goodman A, Page AS, et al. Objectively measured physical activity and sedentary time in youth: The International children’s accelerometry database (ICAD) Int J Behav Nutr Phys Act. 2015;12:113. doi: 10.1186/s12966-015-0274-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Astfalck RG, O’Sullivan P, Straker LM, et al. Sitting postures and trunk muscle activity in adolescent with and without nonspecific chronic low back pain. Spine. 2010;35:1387–95. doi: 10.1097/BRS.0b013e3181bd3ea6. [DOI] [PubMed] [Google Scholar]
- 45.Castellini G, Gianola S, Banfi G, et al. Mechanical low back pain: Secular trend and intervention topics of randomized controlled trials. Physiother Can. 2016;68:61–63. doi: 10.3138/ptc.2014-58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Ergun T, Lakadamyal H, Sukru Sahin M. The relation between sagittal morphology of the lumbosacral spine and the degree of lumbar intervertebral disc degeneration. Acta Orthop Traumatol Turc. 2010;44:293–99. doi: 10.3944/AOTT.2010.2375. [DOI] [PubMed] [Google Scholar]
- 47.O’Sullivan PB, Smith AJ, Beales DJ, Straker LM. Association of biopsychosocial factors with degree of slump in sitting posture and self-report of back pain in adolescents: A cross-sectional study. Phys Ther. 2011;91:470–83. doi: 10.2522/ptj.20100160. [DOI] [PubMed] [Google Scholar]
- 48.Drzał-Grabiec J, Snela S, Rykała J, et al. Effects of the sitting position on the body posture of children aged 11 to 13 years. Work. 2015;51:855–62. doi: 10.3233/WOR-141901. [DOI] [PubMed] [Google Scholar]
- 49.Grabara M, Hadzik A. Postural variables in girls practicing volleyball. Biomedical Human Kinetics. 2009;1:67–71. [Google Scholar]
- 50.Grabara M. Analisis of body posture between young football players and their untrained peers. Human Movement. 2012;13(2):120–26. [Google Scholar]
- 51.Dunk NM, Callaghan JP. Lumbar spine movement patterns during prolonged sitting differentiate low back pain developers from matched asymptomatic controls. Work. 2010;35:3–14. doi: 10.3233/WOR-2010-0953. [DOI] [PubMed] [Google Scholar]
- 52.Callaghan JP, McGill SM. Low back joint loading and kinematics during standing and unsupported sitting. Ergonomics. 2001;44:280–94. doi: 10.1080/00140130118276. [DOI] [PubMed] [Google Scholar]
- 53.Oh YM, Eun JP. Clinical impact of sagittal spinopelvic parameters on disc degeneration in young adults. Medicine. 2015;94:e1833. doi: 10.1097/MD.0000000000001833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Mrozkowiak M. [Age differences in prevalence of correct body postures, incorrect body postures and scoliosis in children and adolescents from chosen regions of Poland and aged from 4 to 19 years]. Annales Universitatis Mariae Curie-Skłodowska, Sectio D: Medicina. 2007;62(Suppl 18):189–92. 5. [in Polish] [Google Scholar]
- 55.Drużbicki M, Walicka-Cupryś K, Przysada G. Evaluation of anterior-posterior spinal curvatures in children and adolescents with low-degree scoliosis. Eur J Phys Rehab Med. 2016;52(Suppl 1):780. [Google Scholar]
- 56.Grivas TB, Dangas S, Samelis P, et al. Lateral spinal profile in school-screening referrals with and without late onset idiopathic scoliosis 10 degrees-20 degrees. Stud Health Technol Inform. 2002;91:25–31. [PubMed] [Google Scholar]
- 57.Ogden CL, Flegal KM. Smoothed percentage body fat percentiles for US children and adolescents, 1999–2004. National Health Stat Report. 2011;43:1–7. [PubMed] [Google Scholar]
- 58.Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesity and trends in body mass index among U.S. children and adolescents, 1999–2010. J Am Med Assoc. 2012;307(5):483–90. doi: 10.1001/jama.2012.40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Walicka-Cupryś K, Ćwirlej A, Kużdżał A, Zawadzka D. Physical activity among adolescents in village and town areas. Young Sport Science of Ukraine. 2010;14(2):32–39. [in Polish] [Google Scholar]