

Abstract
Women of child-bearing age (especially pregnant and lactating women) are in the most nutritionally-vulnerable stages of the life cycle. The aim of this study was to assess the knowledge, attitude and practice of good nutrition among women of childbearing age in Somolu Local Government (LG), Lagos state. This study was a crosssectional descriptive survey of 244 women of childbearing age (15-49 years). Excellent knowledge and good attitude towards good nutrition was observed among 61.89% and 86.89% respectively. During pregnancy, greater than 80% took folic acid, iron supplements and increased daily consumption of fruits and vegetables while 43.59% avoided eggs, fish, meat and chocolate beverage because of taboos. Seven days prior to interview, over 90% had consumed fast foods, 56.15% and 50.01% of the respondents ate fruits and vegetables every day to ≥4 times in a day respectively. A majority of the respondents knew and had a good attitude towards good nutrition supporting studies from Kenya and Northern Nigeria. This, however, did not translate to good practice for about half of the respondents.
Key words: nutrition, women of childbearing age, Lagos
Introduction
The nutritional status of women is very significant as it is through these women and their children that the deleterious effects of malnutrition are transmitted to future generations. 1 According to the World Health Organization, many women do not get enough micronutrients in their diets during their reproductive age as well as during pregnancy. They are also unaware of how much their nutritional status impacts their pregnancy and infant outcomes.2 In Nigeria, women are usually responsible for producing and preparing food for the household, so their knowledge of good nutrition or lack of it can affect the health and nutritional status of the entire family.
Studies from Nigeria have revealed a high prevalence of both under nutrition and over nutrition, as well as nutrient deficiencies, including iron, folate, vitamin D and vitamin A.3,4 According to Nigeria Demographic and Health survey, the 11% of women of reproductive age are thin or undernourished (BMI less than 18.5kg/m2).5 17% of women are overweight (BMI of 25-29 kg/m2), and 8 percent are obese (BMI of 30 kg/m2 or above).5 Overweight or obesity is most prevalent in Lagos (44%).5 Consequently, obstetric complications such as hypertension, anemia, neural tube defects, night-blindness, low birth weight and maternal and perinatal mortality are common. In Lagos State, the maternal mortality rate is 650 deaths per 100 000 live births.6 Many of these deaths have malnutrition as the predisposing factor, either directly or indirectly. Similar studies have been conducted in Western Kenya and Northern Nigeria however few studies have been done in South Western Nigeria. It is hoped that in doing this study, it will shed more light on the knowledge, attitude and practice of good nutrition among women of childbearing age in a periurban area in Lagos State and provide a basis for developing nutrition education programs and interventions that will improve quality of life and reduce morbidity, mortality and health-care costs.
Aim of the study
To assess the level of knowledge, attitude and practice of good nutrition among women of childbearing age in Somolu Local Government.
Materials and Methods
Description of the study area
Lagos state is the smallest state in Nigeria, with an area of 356,861 hectares of which 75,755 hectares are wetlands, yet it has the highest population, which is over 5% of the nation’s estimate. As at 2006, the population of Lagos State was 17.5 million with a growth rate of 3.2%. Today, the state has over 21 million. The state is located on the south western part of Nigeria, on the narrow coastal flood plain of the Bight of Benin.7
It has 245 federal recognized wards.8 It is bounded on the north and east by Ogun State of Nigeria, on the west by the Republic of Benin and on the south by the Atlantic Ocean. There are 20 local government areas.
Somolu is one of the 20 local government areas in Lagos State with a population of about 402, 673 inhabitants of which 195, 024 are females.9 It is located at the East Senatorial District of Lagos State. It has a land area of 11.6 km.10 It is a residential suburb with problems of overcrowding, poor housing and inadequate sanitation. Most of its residents are of the Yoruba tribe.11
Study design
A cross-sectional descriptive study was conducted to assess the knowledge, attitude and practice of good nutrition among women of childbearing age in Somolu LG, Lagos. A quantitative data collection method was employed for a duration of one month.
Study population
The target population were women aged 15-49 years in Somolu Local Government of which they were selected by multistage sampling technique.
Inclusion criteria
Respondents must be residents of the Somolu Local Government, female and between the ages of 15-49 years old.
Exclusion criteria
Those who were excluded from the study were those who were not residents of Somolu Local Government, males and females not between ages 15-49 years old.
Sample size determination
The sample size was determined using Fisher’s Formula:
| n = z2p (1-p)/e2 |
where n = Minimum required sample size in population >10,000.
Z = Standard normal deviation at 95% confidence interval. Level of significance is 1.96.
P = Prevalence of women who have knowledge of good nutrition from literature reviewed12 = 0.185.
E =Acceptable margin of sampling error (0.05).
Employing a standard normal deviate of 1.96% at 95% confidence level and a maximal allowable difference from true population of 5% (0.05), the sample size was:
| n = 1.962 * 0.185 (1 – 0.185) / 0.052 = 0.57921724 / 0.0025= 232 |
The sample size gotten was then increased by 10% to account for contingencies such as non-response or recording error.
| n + 10% of n = 232 + [(10/100) * 232] = 232 + 23.2 = 255 |
Therefore, sample size (n) was equal to 255.
Sampling procedure
A multi-stage sampling technique was used to select the respondents.
Stage one: Selection of wards
A list of wards was obtained from Somolu Local Government Council. By a simple random sampling technique using the balloting method among eight wards, Ward Onipanu was selected.
Stage two: Selection of streets
A simple random sampling of streets within Somolu was done to select six streets out of thirty streets in Ward Onipanu. This was done with the intention of selecting forty-three respondents per street. (255/6 = 43)
Stage three: Selection of houses
All the houses on the selected streets was used for the study.
Stage four: Selection of households
Only one household was picked in each of the houses. If there were more than one household in the house that was selected, then simple random sampling by balloting technique was used to select one of the households.
Stage five: Selection of respondents
Only one respondent that met the inclusion criteria was interviewed in any selected household.
In a case where there were more than one eligible member in the selected household, then the respondent to be interviewed was selected by simple random technique (balloting).
Data collection tools and technique
Data collection tool
Data collection was carried out using a semi-structured interviewer-administered questionnaire. The questionnaire was in English, but was administered in Yoruba or vernacular languages for those who do not understand English.
The questionnaire consisted of four sections.
Section A determined the socio-demographic characteristics of the respondents. The occupations were categorized using an adaptation of the England and Wales classification of occupation which included professional, intermediate, skilled, unskilled and unemployed.
Section B assessed the knowledge of good nutrition among women of childbearing age. The questions assessed their knowledge on the nutritive value of common foods and adverse effects of deficient state of various nutrients.
Section C assessed the attitude to good nutrition among women of childbearing age. The questions assessed their reactions and beliefs about various diets during lactation, pregnancy and before getting pregnant.
Section D assessed the practice of nutrition among women of childbearing age. It had a total of 16 questions. It had two subsections; the first subsection assessed practice of good nutrition in women while pregnant including use of folic acid, iron therapy, alcohol and herbal concoctions in pregnancy (for those who were either pregnant or had been pregnant before) and for the second subsection, a food frequency questionnaire was used.
Pre-testing of instrument
The questionnaire was pre-tested among thirty (30) residents of Ward Fadeyi. The responses obtained during the pretesting was used to modify the questions which were not clear or seemed ambiguous.
Data collection
The data was collected on Wednesdays, Fridays, Saturdays and Sundays for a month. On the day of data collection, the respondents in each selected streets were first of all informed of the reasons and nature of the study. Participants were specifically asked not to write their names on the questionnaire and assured that any information provided would be treated with strict confidentiality. The questionnaire was then administered to the respondents. All completed questionnaire were collected and appropriately coded immediately after while the incomplete ones were put aside.
Data analysis
Data was entered and analyzed using Epi-Info 2007 statistical software. The analyzed data was presented as frequency tables and charts. Summary statistics such as frequencies, mean and inferential statistics was done. Chi-square was used to test for associations between selected variables and the level of significance was set at ≤5%.
Scoring system
The level of knowledge was scored based on a scale of 0-44. A Likert scale was used to assess level of knowledge. Strongly agree attracted 4 marks, agree attracted 3 marks, indifferent attracted 2 marks, disagree attracted 1 mark and strongly disagree attracted 0 mark for positive statements. For wrong statements, this was reversed. Using 50% as cut-off point; respondents that scored 0-10.4 were graded as very poor, those that scored 10.5-21 were graded as poor, those that scored 22-32 were graded as good and those that scored 33-44 were graded as excellent.
Attitude towards good nutrition was scored based on a scale of 5-40. A Likert scale was also used to assess attitude. Strongly agree attracted 5 marks, agree attracted 4 marks, indifferent attracted 3 marks, disagree attracted 2 marks and strongly disagree attracted 1 mark for positive statements. For wrong statements, this was reversed. Respondents that scored 5-23 were graded as having poor attitude while those that scored 24-40 were graded as having good attitude.
Ethical consideration
Ethical approval for the study was obtained from the Health Resource and Ethics committee (HREC) of the Lagos University Teaching Hospital. Permission was obtained from Somolu Local government Council. Oral informed consent was obtained from each respondent prior to participation in the study and data was kept confidential. The respondents were also informed of their right to withdraw at any point of the study without prejudice.
Results
Socio-demographic characteristics
A total of 244, out of 255 questionnaires administered to respondents, were properly filled. Thus, the response rate was 95.69%. The mean age of the respondents was 28.70±6.69 years. Less than two-thirds of the respondents (61.07%) were married.
Regarding their ethnic composition and religion and level of education, about twothirds of the respondents were of Yoruba ethnic group (65.57%) and were Christians (67.62%). Less than half (47.13%) of the respondents had post-secondary education as their highest level of education. Among the respondents that were married, more than half (62.25%) of their spouses had post-secondary education as their highest level of education.
Regarding the women’s estimated monthly income, about one-fourth (26.24%) earned an estimated monthly income of N 18,000-50,000 ($ 52-143) and about half of the respondents (51.64%) earned less than N 18,000 ($ 52) which is the minimum wage in Nigeria. Less than half of the respondents (48.77%) had skilled occupations and among those who were married, more than half of their spouse had skilled occupations (58.28%).
Knowledge, attitude and practice of good nutrition among women of childbearing age
Figure 1 shows the sources of information on good nutrition of the women. This was mostly through hospital, television, medical outreaches and internet. The others were family/friends (9.43%), school (8.20%), radio (6.67%), newspaper (5.33%), church/mosque (4.10%), and traditional birth attendants (3.28%). A majority of the respondents (87.70%) had been taught about balanced diet.
Figure 1.
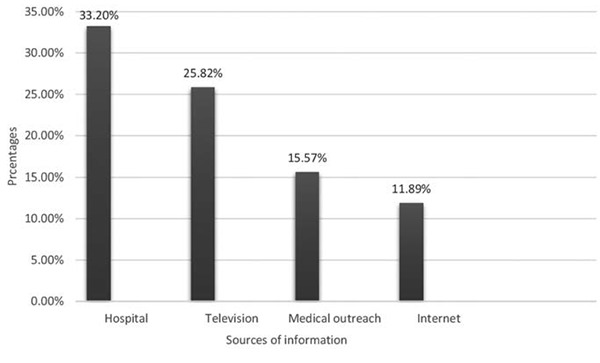
Respondents’ sources of information on nutrition.
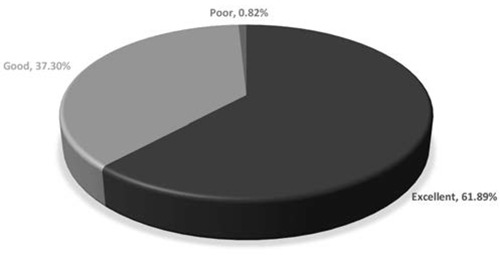
Among 244 respondents, less than twothird (61.89%) had an excellent knowledge of good nutrition (Figure 2). The mean knowledge score was 33.87±4.64 on a scale of 0-44. A majority (89.75%) knew maize is an energy-giving food, more than half of the respondents (57.59%) did not know meat, liver and dark-green vegetables were good sources of iron, (82.37%) agreed that low birth weight in babies can occur in women who do not eat well and a very high proportion of the respondents (95.08%) knew that a pregnant woman should increase fruits and vegetables intake.
Figure 2.
Overall knowledge of good nutrition among respondents.
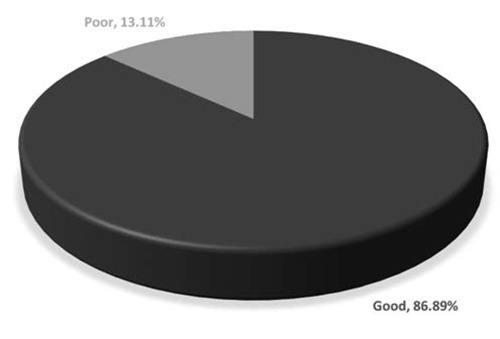
Also, majority (86.89%) had a good attitude towards good nutrition with a mean attitude score is 28.39±4.53 on a scale of 5-40 (Figure 3). About one-third of the respondents (36.59%) felt preparing their own food is time-consuming and (21.31%) of the respondents would prefer to buy food than cook their own food. Over half of the respondents (59.42%) agreed that vegetables did not have to be overcooked. Less than one-third (28.69%) felt they shouldn’t eat foods like eggs and snail when they get pregnant and a majority (84.84%) felt it was important to take folic acid and iron when they get pregnant.
Figure 3.
Overall attitude towards good nutrition among respondents.
Over 80% of the respondents took folic acid, iron and increased the amount of fruits and vegetables during pregnancy while 43.59% avoided eggs, fish, meat and chocolate beverage because of taboos, 39.10% took herbal concoctions and 16.67% took alcohol (Figure 4).
Figure 4.
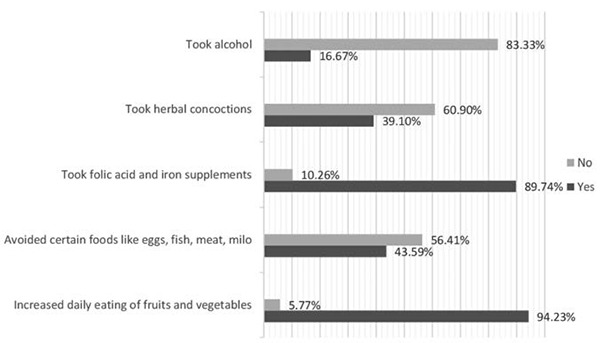
Nutritional practice while pregnant.
In the last seven days prior to the interview, 56.15% and 50.01% of the respondents ate fruits and vegetables every day to ≥4 times in a day respectively, 47.13% of the respondents ate legumes every day to ≥4 times in a day. Over 90% had consumed fast foods in the past seven days as well.
There was statistically significant association between age (P=0.0063), highest level of education (P=0.0035) and their knowledge of good nutrition. There was also statistically significant association between highest level of education of the respondents (P=0.0075) and their attitude towards good nutrition. Their knowledge was positively associated with their attitude towards good nutrition (P=0.0007).
Discussion
The study showed that hospital had the widest reach among the respondents, followed by information from television and medical outreach. This was also similar to the previous study carried out in Maiduguri, Borno State where more than half of the respondents got their knowledge from antenatal clinic but it was followed by information from home and friends.14
This is probably due to majority of the respondents being pregnant before and had probably attended antenatal clinic where nutrition education is done.
The excellent mean knowledge score of 33.87±4.64 out of a possible 44 marks among the respondents substantiated by an excellent overall and a good overall knowledge among 61.89% and 37.30% of the respondents respectively is a much better finding than the findings from a study done in Western Kenya where 46% of the respondents had a moderate overall knowledge score, followed by those with a low overall knowledge score (32.7%). More than twothirds had good attitude towards good nutrition. The mean attitude score of the respondents in this study was 28.39±4.53 out of a possible 40 marks which is similar to previous studies done in Kenya and Mazini, Swaziland where the mean attitude score is 7.39±2.2 out of a possible 10 marks and 24±2.8 out of a possible 36 marks respectively. 13,15
More than one-third of the respondents who had been pregnant before took herbal concoctions while pregnant. While administering the questionnaire, a woman said it is very good for both the mother and child as it helps the child to develop well and be strong. This is similar to findings in a previous study done in Imo State, Nigeria where 36.8% of the respondents reported herbal concoction use during pregnancy.16 This prevalence is quite high. This could be due to the cultural beliefs, easy accessibility and affordability of the herbal concoctions.
Among respondents who had been pregnant before, almost half of the respondents avoided certain foods like eggs, fish, meat and milo (a chocolate drink) while they were pregnant. This is a little lower than a similar study conducted in Borno State where 61.22% of the respondents avoided foods like eggs, fish, fruits and milo drinks while pregnant.14 This could be due to taboos regarding consumption of certain diets while pregnant in Nigeria.
Among the respondents who had been pregnant before (16.67%) took alcohol while pregnant. This is however much lower than the findings from a previous study done in Port Harcourt, Rivers State where more than half (59.28%) of the respondents took alcohol while pregnant.17
Low fruit and vegetable consumption have been reported to consistently have higher prevalence among the disadvantaged of all groups of people.18 The prevalence of low fruit and vegetable consumption tended to increase with age and decrease with income.19 Studies from mainly low- and middle-income countries showed that 78.4% of women consumed less than the minimum recommended five daily servings of fruits and vegetables.19 The daily consumption of fruits and vegetables by at least half of the respondents is higher than those in another study done in Maidiguri, Borno State where 26.53% of the respondents reported eating fruits and vegetables daily.14 The low intake of fruit and vegetables may be due to their inability to afford the food which translates to unavailability.
There is statistically significant association between socio-demographic characteristics such as age and highest level of education of the respondents and their knowledge of good nutrition. Therefore, age and highest level of education are factors that affect the knowledge of good nutrition in this study. This is comparable with studies carried out in Southeast Texas and Mazini, Swaziland in which nutritional knowledge of the women was significantly associated with the level of education, however, it was not significantly associated with age in those studies.15,20 However, in a study conducted in Belgium, age, educational level and their kind of occupation were significantly associated with their nutritional knowledge.21
There was statistically significant association between the highest level of education of the respondents and their attitude towards good nutrition. Therefore, highest level of education is a factor that affects the attitude towards good nutrition in this study. This is in contrast with a similar study done in Manzini, Swaziland in which other sociodemographic factor such as religion was found to be significantly associated with attitude towards good nutrition.15
There was statistically significant association between the knowledge of the respondents and their attitude towards good nutrition. This is in keeping with a previous study done in Manzini, Swaziland in which nutritional knowledge and attitude were significantly associated.15
Conclusions and recommendations
The results from the study show that majority of the respondents had good knowledge and attitude towards good nutrition, however this did not translate to a good dietary practice for about half of the respondents.
It is recommended that awareness of good, indigenous food cultures and dietary habits should be intensified to motivate practice. Also, community leaders and members should invest in agriculture so as to enable increased access to fresh organic agricultural products such as fruits and vegetables.
References
- 1.Cetin I, Laoreti A. From the womb to the adult. In: Vassilios F, Michele M, Antonio DV, et al., eds. The importance of maternal nutrition for health. Proceedings of the 11th International Workshop on Neonatology and Satellite Meetings. 2015 Oct 26-31,Cagliari (Italy). J Pediatr Neonat Individual Med 2015; 4:e040220. [Google Scholar]
- 2.World health Organization. Nutrition. Available from: http://www.who.int/features/factfiles/nutrition/facts/en/ [Google Scholar]
- 3.Berti C, Cetin I, Agostoni C, et al. Pregnancy and infants’ outcome: nutritional and metabolic implications. Crit Rev Food Sci Nutr 2016;56:82-91. [DOI] [PubMed] [Google Scholar]
- 4.Senbanjo IO, Olayiwola IO, Afolabi WA, Senbanjo OC. Maternal and child under-nutrition in rural and urban communities of Lagos state, Nigeria: the relationship and risk factors. BMC Res Notes 2013;6:286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.National Population Commission (NPC) and ICF International. Nigeria Demographic and Health Survey 2013. Available from: https://dhsprogram.com/pubs/pdf/FR29 3/FR293.pdf/ [Accessed 20th July 2016]. [Google Scholar]
- 6.Lindsay KL, Gibney ER, McAuliffe FM. Maternal nutrition among women from Sub-Saharan Africa, with a focus on Nigeria, and potential implications for pregnancy outcomes among immigrant populations in developed countries. J Hum Nutr Diet 2012:25;534-46. [DOI] [PubMed] [Google Scholar]
- 7.Wikipedia. List of Lagos State Local Government Areas by population. Available from: http://en.m.wikipedia.org/wiki/list-of-lagos-state-local-government-areas-by-population (Accessed 20th March, 2016). [Google Scholar]
- 8.LASIEC to INEC. Create more wards in Lagos. Available from: http://www.pmnewsnigeria.com (Accessed 15th May, 2015). [Google Scholar]
- 9.Legal notice on publication of Details of the breakdown of the National and State Provincial Totals of 2006 Census. Lagos, Nigeria: May 15, 2007. Federal Republic of Nigeria Official Gazette No 24, Vol 94, B 175–98. [Google Scholar]
- 10.Lagos State Government. The 16 LGAs of Metropolitan Lagos. Available from http://www.lagosstate.gov.ng/aboutlagos/ (Accessed March 22, 2016). [Google Scholar]
- 11.Encyclopeadia Britannica. Shomolu, Nigeria. Available from http://www.britannica.com/place/Shomolu/ (Accessed March 22, 2016). [Google Scholar]
- 12.Acheampong I, Haldeman L. Are Nutrition Knowledge, Attitudes and Beliefs Associated with Obesity among Low-Income Hispanic and African Women Caretakers? J Obesity 2013;2013:123901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Perumal N, Cole DC, Ouedraogo HZ, et al. Health and nutrition knowledge, attitudes and practices of pregnant women attending and not-attending ANC clinics in Western Kenya: a cross-sectional analysis. BMC Pregnancy Childbirth 2013;13:146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kever RT, Martins SD, Lola N, et al. Knowledge and attitude of pregnant women towards dietary practices in Yerwa Clinic, Maiduguri Metropolitan Council; Borno State. J Res erch Nurs Midwif 2015;4:12-9. [Google Scholar]
- 15.Sakhile KM, Shu-Jan JL. Nutritional Knowledge, Attitude, and Practices among Pregnant and Lactating Women Living with HIV in the Manzini Region of Swaziland. J Health Popul Nutr 2014:32:261-9. [PMC free article] [PubMed] [Google Scholar]
- 16.Chukwuma BD, Kenechi AU, Nnebue CC, et al. Socio-demographic Determinants of Herbal Medicine Use in Pregnancy Among Nigerian Women Attending Clinics in a Tertiary Hospital in Imo State, South-East, Nigeria. Am J Med Stud 2016:4;1-10. [Google Scholar]
- 17.Ordinioha B, Brisibe S. Alcohol consumption among pregnant women attending the ante-natal clinic of a tertiary hospital in South-South Nigeria. Niger J Clin Pract 2015:18;13-7. [DOI] [PubMed] [Google Scholar]
- 18.Hosseinpoor AR, Bergen N, Kunst A, et al. Socioeconomic inequalities in risk factors for non-communicable diseases in low-income and middle-income countries: results from the World Health Survey. BMC Publ Health 2012;12:912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Hall JN, Moore S, Harper SB, Lynch JW. Global variability in fruit and vegetable consumption. Am J Prev Med 2009:36;402-9 [DOI] [PubMed] [Google Scholar]
- 20.Tabassum HL, Mahbubur R, Ali MP, Abbey BB. Level of nutrition knowledge and its association with weight loss behaviors among low-income reproductive-age women. J Commun Health 2015:40;542-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.De Vriendt T, Matthys C, Verbeke W, et al. Determinants of nutrition knowledge in young and middle-aged Belgian women and the association with their dietary behaviour. J Appet 2009:52; 788-92. [DOI] [PubMed] [Google Scholar]