

Abstract
Purpose:
The present study was designed to determine the extent that horizontal inequity was realized regarding eye care utilization in a middle-aged population as well as factors affecting this equity.
Methods:
Data were obtained from a population-based study (Shahroud Eye Cohort Study) in 2009 that included 5190 participants from 40 to 64 years of age. Horizontal inequity was determined based on the following variables: (i) economic status, (ii) eye care service needs, (iii) non-need variables, and (iv) eye care utilization (visiting an ophthalmologist or optometrist). Decomposition analysis of the concentration index based on a nonlinear model and indirect standardization was used to ascertain the contribution of each factor in inequity of eye care utilization.
Results:
After adjusting for need variables, the results of our study demonstrated that horizontal inequity in eye care utilization in a middle-aged Iranian population remained positive and significant (horizontal inequity: 0.19; 95% confidence interval: 0.17–0.23) indicating that use of services was focused among participants with a better financial situation. Furthermore, decomposition analysis demonstrated that educational level and economic status had the greatest contribution (54.1% and 41.1%, respectively) in comparison to other variables.
Conclusion:
This study demonstrated that horizontal inequity exists in eye care utilization among the middle-aged Iranian population.
Keywords: Eye Care Utilization, Horizontal Inequity Index, Iran, Middle-aged Population
INTRODUCTION
The main goal of many healthcare systems is an equitable expansion of healthcare services and reducing inequalities among individuals the world over. According to the Iranian health sector evolution plan, the same holds true for Iran.[1,2,3,4,5] Furthermore, one of the items proposed by the International Agency for the Prevention of Blindness and the World Health Organization (WHO) in a document entitled “Universal eye health: a global action plan 2014–2019” for reducing avoidable blindness is equity in access to, and utilization of, eye care services.[6]
Utilization of healthcare services, especially specialized services, increases with age, which is an important issue in the aging population. This increased need is more frequently observed in countries with low and medium incomes.[7] The WHO's global action plan has been designed with the global escalation in the frequency of chronic age-related eye diseases in mind. The access to, and fair utilization of, eye care services are facets of the global action plan that are key to controlling visual impairment, including blindness.[6]
Based on the guidelines of the American Academy of Ophthalmology, it is recommended that even if no symptoms or risk factors for eye diseases exist, adults must undergo comprehensive eye examinations at least once before 40 years of age, every two to four years between the ages of 40 and 54, every one to three years between the ages of 55 and 64, and every one to two years for individuals 65 years or older.[8]
Globally, several studies have examined and described inequality in eye care utilization and its related factors.[9,10,11,12,13,14,15,16,17,18,19,20] In addition, studies around the world have shown that eye care utilization in the adult population is quite low.[21,22] People in high-income countries have more regular check-ups and eye examinations,[23,24,25] while in developing countries, a significant percentage of people never utilize eye care services.[10,13,15,16,26] On the other hand, several studies have shown that blindness is more common in poor communities[27,28,29,30] and gender is a predictor of eye disease and access to eye care.[31,32] In the literature, the concept of inequality and horizontal inequity are often considered the same. However, the two terms are different; therefore, there are two different analysis approaches. The existence of inequality based on one outcome measure of health service utilization does not mean horizontal inequity.[33,34,35] Horizontal equity in healthcare utilization is defined as equal healthcare for equal need regardless of other factors, such as socioeconomic status, race, or gender. In other words, horizontal inequity means any residual inequality in healthcare utilization after standardization based on need variables.[33,34,35] Although several studies have examined the impact of inequality on eye care utilization and eye diseases, our review of the literature showed that there are no studies of horizontal inequity in eye careutilization.
The aim of this study was to measure horizontal inequity in eye care utilization in a middle-aged Iranian population (40–64 years) using data from the first phase of the Shahroud Eye Cohort Study (ShECS) and to approximate the contribution of each variable to inequity based on the horizontal inequity index.
Achievement of the aims of the Iranian healthcare system and the global action plan of the WHO will undoubtedly be facilitated through the identification of inequity and the factors affecting it.
METHODS
This report was prepared based on data from the first phase of the ShECS that was conducted in 2009 in Shahroud, which is a northern city in Iran. A complete description of the study has been published in a previous paper.[36] In the ShECS, multi-stage cluster sampling was conducted to select 300 random clusters from nine strata. Each healthcare center was considered as one stratum, and clusters were selected proportional to the size of each stratum. From each cluster, at least 20 people aged between 40–64 years were selected to participate. After explaining the purpose of the study, participants were invited to have a thorough eye examination and all the participants signed the informed consent form after the study was explained thoroughly. Demographic characteristics, medical history, and other information were collected from participants through interviews and questionnaires.
Variable Definitions
Eye care utilization variable
The measure of eye care utilization was based on self-reported eye care visits to an optometrist or ophthalmologist during the past five years.
Need and non-need variables
”Need variables” according to O'Donnell et al.[33] include such factors as demographic characteristics, health status, and morbidity variables, including physical disabilities and chronic diseases. They indicate a higher need for services and are expected to increase utilization. In this study, the variables of age (in five categories of 40–44, 45–49, 50–54, 55–59, and 60–-64 years for descriptive analyses and as a continuous quantitative variable in the analyses for horizontal inequity and the concentration index), having chronic diseases, such as diabetes and hypertension, and eye health status (presenting visual acuity of 0.3 logMAR or worse) were used as binary variables and they were considered as need variables.[33]
In addition, “non-need variables” are factors related to need variables and, consequently, to service utilization. When measuring horizontal inequity, they are taken into account when estimating need variables to avoid bias,[33] and they are determinants of inequity. Non-need variables included gender, having basic insurance, and supplemental insurance, which were all considered in a binary fashion. They also included a variable education level (five categories of illiterate, elementary, middle school, high school, and college education), marital status, and economic status. Regarding gender, given that men and women are biologically affected differently by systemic diseases, such as diabetes, hypertension, and other chronic diseases, and it influences both the variables of eye health status and eye care service utilization, these were consequently viewed as inter-gender differences.[15,16,17,18,19,20] Also, studies have shown that the prevalence of some eye diseases, such as cataracts, is different between men and women.[37,38]
Economic Status
Since there is no reliable data for the income index in developing countries to categorize the population into different economic groups, we applied the method described by O' Donnell et al.[33] Principal component analysis (PCA) was applied to home assets (11 items) that were self-reported by the participants. In this analysis, the highest levels were associated with having a private bathroom at the residence, a microwave oven, and a dishwasher. These three variables combined represented 51.77% of the observed variance. Then, an asset index was created based on a weighting for the first PCA factor.[16,20] In other words, participants' economic scores were calculated as the sum of the weighted asset variables based on the first component and using the equation below, and the generated asset index or standard of living was used to define the economic quintiles as follows:

Where aik is the possession of K by the individual i, ᾱK is the average number of possessions of k, Sk is the standard deviation of the possessions of k, and fk is the weight of the first PCA component.[33]
Statistical Analysis
In this study, the effect of the cluster sampling was taken into account when reporting the status of the different variables and calculating horizontal inequity. We have made use of the concentration index to measure inequality related to socioeconomic status in eye care utilization. The concentration index quantifies the degree of inequity in eye care utilization based on the socioeconomic status of individuals. This index is sensitive to the population distribution across socioeconomic groups and can investigate socioeconomic aspects of inequity in eye care utilization.[39] For years, the index has been applied as a standard tool for measuring and comparing the degree of inequity in eye care utilization. The concentration index ranges from -1 to +1; a negative (positive) value shows that the variable of interest is concentrated more among people with lower (higher) economic status, and zero signifies perfect equality. Since eye care utilization in our study was a binary variable, it ranges from a lower limit of μ-1 to a higher limit of 1-μ; thus, we applied the correction for calculating the concentration index of binary variables suggested by Wagstaff et al.[33,40]
The concentration index (C) in this study was calculated using Equation 1 as follows:[33]

Where h represents the eye care utilization variable, μ is the mean or ratio of eye care utilization, and r is the individual's rank according to their economic status from the poorest to the richest.
Horizontal equity is defined as equal treatment for equal medical need regardless of such factors as socioeconomic status, gender, race, and so on. Horizontal inequity exists when individuals with equal medical need receive greater healthcare. The concentration index measures the degree of inequality in healthcare utilization using the socioeconomic status of individuals as the basis. However, due to differences in the needs of individuals for healthcare utilization among different socioeconomic groups, inequality does not indicate inequity. In other words, to measure horizontal inequity, the inequality in the use of health services should be standardized based on need variables, and then any remaining inequalities about the economic status can be interpreted as inequity. People with different economic statuses may also have different needs that result in unequal service utilization, in which case, this is not inequity. Inequity exists when people of different economic statuses have the same need, but do not use healthcare services equally. Therefore, we have made use of the horizontal inequity index to measure inequity in eye care utilization.[33,41] Horizontal inequity estimates the concentration index of need-standardized eye care utilization. The need variables in our study were specified based on gender, age, eye health status, and presence of chronic diseases, such as diabetes and hypertension. According to Wagstaff et al, horizontal inequity is measured using the difference between inequality in actual utilization of healthcare services and need-predicted utilization as follows:
HI = C–CN (2)
Where HI is horizontal inequity, C is the concentration index, and CN is the concentration index for need-predicted utilization. In the case that the result of healthcare utilization is a quantitative variable, the value of horizontal inequity calculated from Equation 2 is equivalent to the need-standardized concentration index. However, if it is a binary variable, such as in our study, the horizontal inequity value calculated by Equation 2 is not exactly equivalent to the need-standardized concentration index, with there being a slight difference. As for the concentration index, a negative (or positive) value of horizontal inequity demonstrates that horizontal inequity is concentrated among individuals with a lower (or higher) economic status.[33]
Furthermore, according to Equation 2, need-predicted eye care utilization and indirect need-standardized eye care services were determined using a non-linear probit regression model based on the following equations:[33]
Also, to quantify the contribution of each need and non-need variable involved in the observed inequity, we applied a decomposition analysis. Concentration index decomposition analysis is conducted through a regression model between the eye care utilization variable and a set of related variables (need and non-need variables). Given the non-linear nature of the outcome measure, decomposition of eye care utilization is possible if the linear approximation is added to the non-linear model. As suggested by O'Donnell et al, we used a linear approximation for the probit model, and partial effects were computed using Equation 5:[33]

In the above equation, xj is a need variable, which is used to standardize eye care utilization. Zk is a non-need variable that is not standardized, but entered into the regression model on account of its relationship with the need variables. α, β and γ are model parameters, i represents each individual, and is the model error term. The concentration index (C) for variable is obtained from Equation 6 as follows:

where μ is the mean eye care utilization (yi), Cj and Ck are concentration indices for collective need factors (Xj) and non-need variables (Zk), βjm and ykm are the partial effects for the need variable (x) and the non-need variable (Z), x̄j and Z̄k are the means of the need and non-need variables, the products of (βjm x̄j/μ)/Cj and (ykm Z̄k/μ) Ck are the contributions of the need variables (j) and non-need variables (k) related to the unadjusted concentration index, and finally, GCε is the generalized concentration index of the error term. A positive and negative contribution of each variable indicates that the variable is related to both economic status and eye care utilization. In other words, a positive (negative) contribution value for each variable indicates that it is a factor associated positively (negatively) with increased eye care utilization, and based on that variable, that it was distributed more among people with higher (lower) economic status.[33,42] All data analyses were performed using Stata version 12 (Stata Corp, College Station, TX, USA).
RESULTS
Of the 6311 invitees, 5190 people (82.2%) participated in this study. Table 1 describes the study participants based on need variables and non-need variables. Eye care utilization increases with age up to 60 years of age, and there is decreased utilization afterward.
Table 1.
Descriptive statistics of need variables and non-need variables for eye care utilization among middle-aged Iranians in 2009 (n=5190)
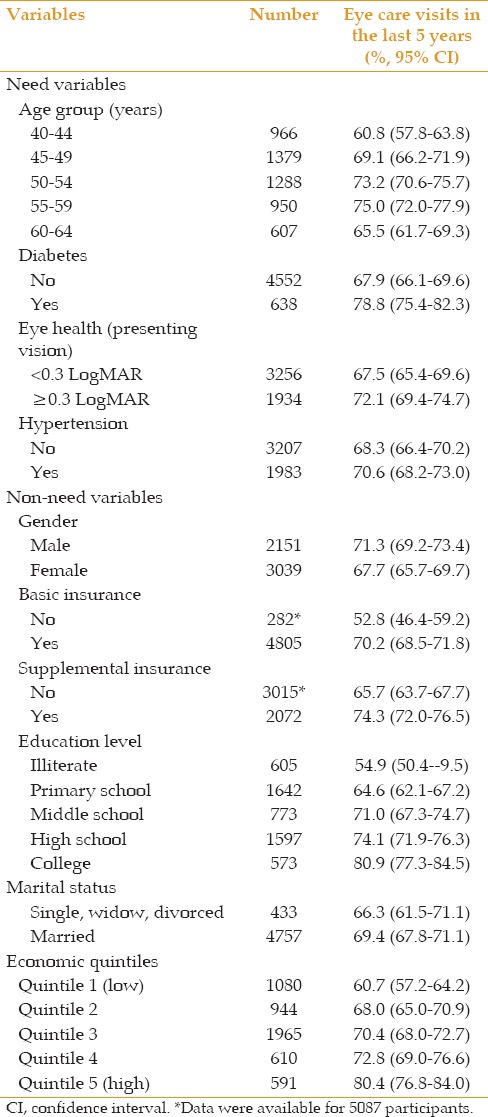
Based on non-need variables, among those who did not have basic health insurance and complementary insurance, 52.8% and 65.7% respectively, reported have eye care visits in the last five years. Eye care utilization increased by the level of education from 54.9% among illiterates to 80.9% in the group with a university education. In addition, the rate of having an eye care visit in the past five years was significantly higher among individuals with high socioeconomic status compared to those with low economic status (80.4% vs 60.7%). Table 2 shows the distribution of eye care utilization in the past five years based on actual, need-predicted utilization, and need-standardized utilization, which was derived from Equations 4 and 5.
Table 2.
Distributions of actual, need-predicted, and need-standardized eye care utilization (%) among middle-aged Iranians
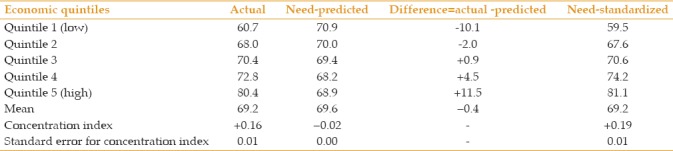
The actual and need-standardized concentration index (C = +0.16, and C = +0.19, respectively) reveal a pro-rich model. In other words, as we move from the lowest economic quintile to the highest quintile, the actual utilization rate exceeds the expected rate. For example, the utilization rate is 10.1% less than predicted in the first economic quintile, while in the highest economic quintile, the utilization rate is 11.5% more than predicted. Furthermore, when utilization was standardized based on need variables, the distribution of eye care utilization was more concentrated among the better-off, such that mean eye care utilization increased from 59.5% in the poorest quintile to 81.1% in the wealthiest economic quintile.
Table 3 presents the results of the decomposition analysis of the concentration index based on need variables, non-need variables, and Equation 6 to determine the contribution of each factor in the creation of economic inequality, and consequently, horizontal inequity. Need variables had a -13.7% contribution to a pro-poor eye care utilization pattern; in other words, a negative value for absolute contributions of the need variables indicates that these variables contribute toward reduced horizontal equity in eye care utilization in favor of the poor. Among the need variables, the variable of age with a contribution of -10.8% had the highest share in reducing horizontal equity in eye care utilization.
Table 3.
Decomposition of the concentration index in eye care utilization and the horizontal inequity index among middle-aged Iranians
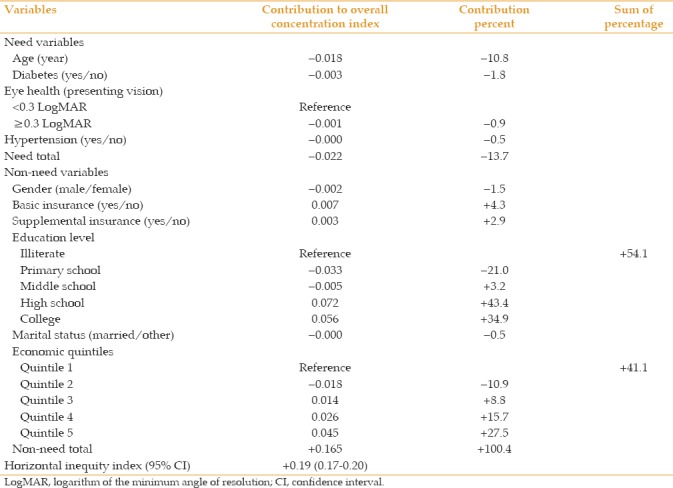
In contrast, non-need variables had a significant pro-rich contribution to eye care utilization; that is, non-need variables had a substantial contribution in increasing eye care utilization among people with higher economic status. Based on non-need variables, having a higher level of education (high school and college) and having a higher economic status had the highest share in increasing horizontal inequity in eye care utilization in comparison with other variables in this study. The total contributions of the level of education and higher economic status toward a pro-rich eye care utilization pattern were + 54.1% and + 41.1%, respectively. As presented in Table 3, we determined the horizontal inequity index (horizontal inequity = +0.19) from the difference between the concentration index for the actual utilization and the concentration index of the total need variables, and this index revealed a pro-rich pattern of eye care utilization.
Furthermore, the results indicated that eye care utilization in the higher economic quintiles was greater than the need-predicted utilization compared to the lower quintiles. In other words, the distribution of eye care utilization, including a visit to the ophthalmologist or optometrist, is concentrated among the well-off, even though the poor had a higher need than the rich.
DISCUSSION
To the best of our knowledge, this is the first study examining inequity based on the definition of horizontal equity and a decomposition analysis of inequity in eye care utilization in a middle-aged (40–64 years) population through a population-based study. This study provided new evidence concerning inequity in the utilization of specialized care, such as eye care, following the WHO's global healthcare plan and the Iranian health sector evolution plan.
Our study demonstrated that inequity existed in eye care utilization based on horizontal inequity, which is inconsistent with O'Donnell et al.'s definition of equity: that is, equal treatment for equal medical need.[33] In other words, the presence of horizontal inequity resulted in the eye care utilization of individuals in various economic classes differing from need-predicted utilization; individuals with higher economic status visited ophthalmologists or optometrists more than the predicted need in comparison to those with lower economic status. The results of our study indicate that there is pro-rich economic inequality in eye care utilization, which is in agreement with studies in Iran and other countries examining economic inequality in eye care utilization.[14,16,43,44]
Although economic inequality and inequity are often used interchangeably in the literature, their differences should be appreciated.[45] Economic inequality in healthcare utilization refers to any differences in health service utilization among economics groups, while inequity refers to avoidable differences in healthcare utilization as a result of disparity within and between groups[46] and absence of equal care for equal needs.[33]
Though the study of Emamian et al.[16] showed that inequality existed in eye care utilization, the definition of the utilization outcome of that study differed from that used in the present study. The study conducted by Emamian et al. in 2014 identified the economic inequality in using ophthalmology services based on the outcome of whether individuals ever used services provided by ophthalmologists or optometrists and analyzed data using the Oaxaca method, whereas the current study assessed horizontal inequity in the use of ophthalmic services in the past five years and then determined the contribution of various factors to the creation of this inequality using the concentration index. Moreover, Emamian et al. did not investigate the presence of inequity based on the horizontal inequity index.[16] Our findings revealed a pro-rich horizontal inequity in eye care utilization and indicated that the influential factors in inequity based on the definition of horizontal inequity were avoidable.
Our results were similar to those of other studies of the use of specialty health services.[2,3,42,47] In other studies of healthcare utilization, especially in developed countries, the unadjusted results indicate that individuals with low economic status have a higher utilization rate due to higher rates of health problems. However, our results showed no evidence of higher utilization rates among people with lower economic status. Considering age and clinical guidelines, participants were expected to have had at least one eye care visit in the past five years. However, even in the richest quintile, which had higher utilization rates than the respective expected rates according to horizontal inequality analyses, about 20% had a medical history that indicated otherwise; this is indicative of vertical inequity, which is defined as a lack of utilization compared to the standard.
Decomposing the concentration index allowed us to determine the difference between economic inequality and inequity based on estimated contributions of the need and non-need variables.[33] As presented in Table 3, the variable of age, compared to other need factors, reduced the inequality in eye care utilization in favor of people with a lower economic status by about -11%. In other words, since the mean age was higher in the lower economic quintiles compared to the higher quintiles (53 years versus 49 years), they also had a higher need for eye care utilization. Consequently, eye care utilization appeared to be higher in groups with lower socioeconomic status. In addition, the overall contribution of -13.7% for need variables shows that if utilization is determined only based on need variables, the pattern is pro-poor.
Decomposition of the concentration index for non-need variables showed that education level and economic status had the greatest share in creating a pro-rich inequity in eye care utilization in comparison with other non-need variables. In other words, the results indicated that having a higher education level (high school and college) and a higher economic status increased eye care utilization in favor of the rich. Similar results can be observed in other studies.[2,3,14,16] Higher eye care utilization among people with high school and college education, and consequently a higher economic status, can also be due to a better awareness about the importance of healthcare services, especially eye care during middle age. Recent studies report that education, as an independent variable, has a more influential role in healthcare utilization compared to economic status.[48] The same results were observed in our study, such that education level contributed 13% more than economic status to a pro-rich inequality in eye care utilization. In Iran, having a lower economic status and lower education level, as opposed to having a high level of education and economic status, often leads to decreased healthcare utilization, particularly in specialty services.[49,50,51]
The results of our study clearly show the direct role of economic status in increasing eye care utilization, such that being in the wealthiest economic quintile, compared to the lowest economic quintile, has a greater contribution toward increasing a pro-rich inequality in eye care utilization. Given that people with higher education in our study often had a higher economic status, they had the advantage of affording proper insurance coverage and obtaining supplemental insurance for better utilization of eye care services.
Considering the high rate of basic insurance coverage (94%) and the supplemental coverage of 41% in our study, and according to the decomposition of the concentration index for the expression of the contribution of various variables, the insurance coverage had a very small role in creating horizontal inequity in eye care service uptake in this population.
Despite the limitations of our study, the evidence obtained from it may aid in resolving identified obstacles in eye care utilization and the realization of the goals of the WHO's “Universal eye health: a global action plan 2014–2019,” including the reduction of avoidable blindness and inequity in healthcare utilization. The main strengths of our study are the evaluation of horizontal equity in eye care utilization using individual data from a population-based study with a large sample size, high participation rate, proper design, and quality control. Although the concentration index allows us to determine the role of different factors in creating the observed inequalities, it should be noted that decomposition analysis does not show the causal direction between economic status and eye care utilization. Since the contribution of each factor in creating the observed inequality usually depends on the product, on the elasticity estimate of a given variable with the variable of utilization in the sample mean, and on the concentration index of the variable, the analysis cannot determine a causal direction between the defined variables and eye care utilization. In addition, the decomposition method is a deterministic approach in which other variables that represent need may have had a role in creating inequity, but were not considered in our model. For example, other variables, such as physical disability, availability of eye care services, allocation of ophthalmologists and optometrists in the population, and accessibility of eye care services should have been considered in this study, but such information was not available at this stage of the study.
In conclusion, the results of our study showed that there is a significant inequality in eye care utilization between the rich and poor, which remained significant after need-standardization; this is indicative of inequity based on horizontal inequity and is attributable to non-need variables. Our findings also confirmed the direct and indirect effects of higher economic status on increasing this pro-rich eye care utilization pattern. Health policymakers should place more emphasis on education and raising public awareness about the use of eye care during middle age, especially among people with lower education and lower economic status. Furthermore, providing more available eye care services or having them covered by basic insurance for people in lower economic quintiles could be considered at the national level. Further studies should focus on the effect of socio-economic status on people's access to services as well as service-seeking behavior.
Financial Support and Sponsorship
The current study was supported by Noor Ophthalmology Research Center and Shahroud University of Medical Sciences. This study is the PhD thesis in Tehran University of Medical Sciences and Noor Ophthalmology Research Center.
Conflicts of Interest
There are no conflicts of interest.
REFERENCES
- 1.Mosquera PA, Waenerlund AK, Goicolea I, Gustafsson PE. Equitable health services for the young? A decomposition of income-related inequalities in young adults' utilization of health care in Northern Sweden. Int J Equity Health. 2017;161:20. doi: 10.1186/s12939-017-0520-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.San Sebastian M, Mosquera PA, Ng N, Gustafsson PE. Health care on equal terms? Assessing horizontal equity in health care use in Northern Sweden. Eur J Public Health. 2017 doi: 10.1093/eurpub/ckx031. [DOI] [PubMed] [Google Scholar]
- 3.Mullachery P, Silver D, Macinko J. Changes in health care inequity in Brazil between 2008 and 2013. Int J Equity Health. 2016;151:140. doi: 10.1186/s12939-016-0431-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Penning MJ, Zheng C. Income Inequities in Health Care Utilization among Adults Aged 50 and Older. Can J Aging. 2016;351:55–69. doi: 10.1017/S0714980815000562. [DOI] [PubMed] [Google Scholar]
- 5.Moradi-Lakeh M, Vosoogh-Moghaddam A. Health Sector Evolution Plan in Iran; Equity and Sustainability Concerns. Int J Health Policy Manag. 2015;410:637–640. doi: 10.15171/ijhpm.2015.160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.World Health Organization, Universal eye health: a global action plan 2014–2019. Geneva, WHO: 2013. [Last accessed on 2018 Jul 20]. Available from: http://www.who.int/blindness/actionplan/en/ [Google Scholar]
- 7.World Health Organization, World report on ageing and health 2015. Geneva, WHO: [Last accessed on 2018 Jul 15]. Available from: http://www.who.int/ageing/events/world-report-2015-launch/en/ [Google Scholar]
- 8.San Feransisco, CA: 2015. [Last accessed on 2018 Jul 20]. American Academy of Ophthalmology, Frequency of Ocular Examinations. Available from: https://www.aao.org/clinical-statement/frequency-of-ocularexaminations . [Google Scholar]
- 9.Eye-care utilization among women aged > or =40 years with eye diseases--19 states, 2006-2008. MMWR Morb Mortal Wkly Rep. 2010;59:588–591. [PubMed] [Google Scholar]
- 10.Dandona R, Dandona L, Naduvilath TJ, McCarty CA, Rao GN. Utilisation of eyecare services in an urban population in southern India: The Andhra Pradesh eye disease study. Br J Ophthalmol. 2000;841:22–27. doi: 10.1136/bjo.84.1.22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Keeffe JE, Weih LM, McCarty CA, Taylor HR. Utilisation of eye care services by urban and rural Australians. Br J Ophthalmol. 2002;861:24–27. doi: 10.1136/bjo.86.1.24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lee DJ, Lam BL, Arora S, Arheart KL, McCollister KE, Zheng DD, et al. Reported eye care utilization and health insurance status among US adults. Arch Ophthalmol. 2009;1273:303–310. doi: 10.1001/archophthalmol.2008.567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Nirmalan PK, Katz J, Robin AL, Krishnadas R, Ramakrishnan R, Thulasiraj RD, et al. Utilisation of eye care services in rural south India: The Aravind Comprehensive Eye Survey. Br J Ophthalmol. 2004;8810:1237–1241. doi: 10.1136/bjo.2004.042606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hwang J. Decomposing socioeconomic inequalities in the use of preventive eye screening services among individuals with diabetes in Korea. Int J Public Health. 2016;615:613–620. doi: 10.1007/s00038-016-0804-1. [DOI] [PubMed] [Google Scholar]
- 15.Fotouhi A, Hashemi H, Mohammad K. Eye care utilization patterns in Tehran population: A population based cross-sectional study. BMC Ophthalmol. 2006;6:4. doi: 10.1186/1471-2415-6-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Emamian MH, Zeraati H, Majdzadeh R, Shariati M, Hashemi H, Fotouhi A. Economic inequality in eye care utilization and its determinants: A Blinder-Oaxaca decomposition. Int J Health Policy Manag. 2014;36:307–313. doi: 10.15171/ijhpm.2014.100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Katibeh M, Rajavi Z, Yaseri M, Hosseini S, Hosseini S, Akbarian S, et al. Association of Socio-Economic Status and Visual Impairment: A Population-Based Study in Iran. Arch Iran Med. 2017;201:43–48. [PubMed] [Google Scholar]
- 18.Mansouri A, Emamian M, Zeraati H, Hashemi H, Fotouhi A. Economic Inequality in Presenting Vision in Shahroud, Iran: Two Decomposition Methods. In Health Policy Manag. 2017;7:59–69. doi: 10.15171/ijhpm.2017.48. DOI:10.15171/ijhpm.2017.48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Emamian MH, Zeraati H, Majdzadeh R, Shariati M, Hashemi H, Jafarzadehpur E, et al. Economic inequality in presenting near vision acuity in a middle-aged population: A Blinder-Oaxaca decomposition. Br J Ophthalmol. 2013;979:1100–1103. doi: 10.1136/bjophthalmol-2013-303249. [DOI] [PubMed] [Google Scholar]
- 20.Emamian MH, Zeraati H, Majdzadeh R, Shariati M, Hashemi H, Fotouhi A. The gap of visual impairment between economic groups in Shahroud, Iran: A Blinder-Oaxaca decomposition. Am J Epidemiol. 2011;17312:1463–1467. doi: 10.1093/aje/kwr050. [DOI] [PubMed] [Google Scholar]
- 21.Dunlop DD, Manheim LM, Sohn MW, Liu X, Chang RW. Incidence of functional limitation in older adults: The impact of gender, race, and chronic conditions. Arch Phys Med Rehabil. 2002;837:964–971. doi: 10.1053/apmr.2002.32817. [DOI] [PubMed] [Google Scholar]
- 22.Rubin GS, Bandeen-Roche K, Huang GH, Munoz B, Schein OD, Fried LP, et al. The association of multiple visual impairments with self-reported visual disability: SEE project. Invest Ophthalmol Vis Sci. 2001;421:64–72. [PubMed] [Google Scholar]
- 23.McGwin G, Khoury R, Cross J, Owsley C. Vision impairment and eye care utilization among Americans 50 and older. Curr Eye Res. 2010;356:451–458. doi: 10.3109/02713681003664931. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Jin YP, Trope GE. Eye care utilization in Canada: Disparity in the publicly funded health care system. Can J Ophthalmol. 2011;462:133–138. doi: 10.3129/i10-120. [DOI] [PubMed] [Google Scholar]
- 25.Puent BD, Klein BE, Klein R, Cruickshanks KJ, Nondahl DM. Factors related to vision care in an older adult cohort. Optom Vis Sci. 2005;827:612–616. doi: 10.1097/01.opx.0000171334.54708.89. [DOI] [PubMed] [Google Scholar]
- 26.du Toit R, Ramke J, Naduvilath T, Brian G. Awareness and use of eye care services in Fiji. Ophthalmic Epidemiol. 2006;135:309–320. doi: 10.1080/09286580600826629. [DOI] [PubMed] [Google Scholar]
- 27.Khan MD. The Duke Elder lecture: The challenge of equitable eye care in Pakistan. Eye (Lond) 2011;254:415–424. doi: 10.1038/eye.2010.186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Gilbert CE, Shah SP, Jadoon MZ, Bourne R, Dineen B, Khan MA, et al. Poverty and blindness in Pakistan: Results from the Pakistan national blindness and visual impairment survey. BMJ. 2008;3367634:29–32. doi: 10.1136/bmj.39395.500046.AE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ho VH, Schwab IR. Social economic development in the prevention of global blindness. Br J Ophthalmol. 2001;856:653–657. doi: 10.1136/bjo.85.6.653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Khanna R, Raman U, Rao GN. Blindness and poverty in India: The way forward. Clin Exp Optom. 2007;906:406–414. doi: 10.1111/j.1444-0938.2007.00199.x. [DOI] [PubMed] [Google Scholar]
- 31.Harris B, Sampson G. Gender differences in the utilisation of optometric services in Victoria. Clin Exp Optom. 2005;882:109–112. doi: 10.1111/j.1444-0938.2005.tb06676.x. [DOI] [PubMed] [Google Scholar]
- 32.Jansen E, Baltussen RM, van Doorslaer E, Ngirwamungu E, Nguyen MP, Kilima PM. An eye for inequality: How trachoma relates to poverty in Tanzania and Vietnam. Ophthalmic Epidemiol. 2007;145:278–287. doi: 10.1080/09286580701299403. [DOI] [PubMed] [Google Scholar]
- 33.O'Donnell O, van Doorslaer E, Wagstaff A. Analyzing health equity using household survey data. A guide to techniques and their implementation, The World Bank, Washington DC. 2008:69–82. [Google Scholar]
- 34.van Doorslaer E, Wagstaff A, van der Burg H, Christiansen T, De Graeve D, Duchesne I, et al. Equity in the delivery of health care in Europe and the US. J Health Econ. 2000;195:553–583. doi: 10.1016/s0167-6296(00)00050-3. [DOI] [PubMed] [Google Scholar]
- 35.Wagstaff A, van Doorslaer E, Paci P. On the measurement of horizontal inequity in the delivery of health care. J Health Econ. 1991;102:169–205. doi: 10.1016/0167-6296(91)90003-6. [DOI] [PubMed] [Google Scholar]
- 36.Fotouhi A, Hashemi H, Shariati M, Emamian MH, Yazdani K, Jafarzadehpur E, et al. Cohort profile: Shahroud Eye Cohort Study. Int J Epidemiol. 2013;42:1300–1308. doi: 10.1093/ije/dys161. [DOI] [PubMed] [Google Scholar]
- 37.Zetterberg M, Celojevic D. Gender and cataract-the role of estrogen. Curr Eye Res. 2015;402:176–190. doi: 10.3109/02713683.2014.898774. [DOI] [PubMed] [Google Scholar]
- 38.Prokofyeva E, Wegener A, Zrenner E. Cataract prevalence and prevention in Europe: A literature review. Acta Ophthalmol. 2013;91:395–405. doi: 10.1111/j.1755-3768.2012.02444.x. [DOI] [PubMed] [Google Scholar]
- 39.Wagstaff A, Paci P, van Doorslaer E. On the measurement of inequalities in health. Soc Sci Med. 1991;335:545–557. doi: 10.1016/0277-9536(91)90212-u. [DOI] [PubMed] [Google Scholar]
- 40.Wagstaff A. The bounds of the concentration index when the variable of interest is binary, with an application to immunization inequality. Health Econ. 2005;144:429–432. doi: 10.1002/hec.953. [DOI] [PubMed] [Google Scholar]
- 41.Wagstaff A, Van Doorslaer E. Measuring and testing for inequity in the delivery of health care. Journal of Human Resources. 2000:716–733. [Google Scholar]
- 42.Sozmen K, Unal B. Explaining inequalities in Health Care Utilization among Turkish adults: Findings from Health Survey 2008. Health Policy. 2016;1201:100–110. doi: 10.1016/j.healthpol.2015.10.003. [DOI] [PubMed] [Google Scholar]
- 43.Vela C, Samson E, Zunzunegui MV, Haddad S, Aubin MJ, Freeman EE. Eye care utilization by older adults in low, middle, and high income countries. BMC Ophthalmol. 2012;12:5. doi: 10.1186/1471-2415-12-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Chou CF, Barker LE, Crews JE, Primo SA, Zhang X, Elliott AF, et al. Disparities in eye care utilization among the United States adults with visual impairment: Findings from the behavioral risk factor surveillance system 2006-2009. Am J Ophthalmol. 2012;1546(Suppl):S45–52. doi: 10.1016/j.ajo.2011.09.025. e41. [DOI] [PubMed] [Google Scholar]
- 45.Asada Y, Hurley J, Norheim OF, Johri M. Unexplained health inequality-is it unfair? Int J Equity Health. 2015;14:11. doi: 10.1186/s12939-015-0138-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Final Report of the Commission on Social Determinants of Health. Geneva, WHO: 2008. World Health Organization, Closing the gap in a generation: health equity through action on the social determinants of health. [DOI] [PubMed] [Google Scholar]
- 47.Lu JF, Leung GM, Kwon S, Tin KY, Van Doorslaer E, O'Donnell O. Horizontal equity in health care utilization evidence from three high-income Asian economies. Soc Sci Med. 2007;641:199–212. doi: 10.1016/j.socscimed.2006.08.033. [DOI] [PubMed] [Google Scholar]
- 48.Habicht J, Kunst AE. Social inequalities in health care services utilisation after eight years of health care reforms: A cross-sectional study of Estonia, 1999. Soc Sci Med. 2005;604:777–787. doi: 10.1016/j.socscimed.2004.06.026. [DOI] [PubMed] [Google Scholar]
- 49.Mohammadbeigi A, Hassanzadeh J, Eshrati B, Rezaianzadeh A. Decomposition of inequity determinants of healthcare utilization, Iran. Public Health. 2013;1277:661–667. doi: 10.1016/j.puhe.2013.01.001. [DOI] [PubMed] [Google Scholar]
- 50.Ramezani Doroh V, Vahedi S, Arefnezhad M, Kavosi Z, Mohammadbeigi A. Decomposition of Health Inequality Determinants in Shiraz, South-west Iran. J Res Health Sci. 2015;153:152–158. [PubMed] [Google Scholar]
- 51.Homaie Rad E, Kavosi Z, Arefnezhad M. Economic inequalities in dental care utilizations in Iran: Evidence from an urban region. Med J Islam Repub Iran. 2016;30:383. [PMC free article] [PubMed] [Google Scholar]