

Abstract
Objectives
This review provides a broad overview of the effectiveness of interventions for subjective cognitive decline (SCD) in improving psychological well-being, metacognition and objective cognitive performance.
Methods
Databases including PubMed, Web of Science and Cochrane Systematic Reviews were searched up to August 2017 to identify randomised controlled trials evaluating interventions for SCD. Interventions were categorised as psychological, cognitive, lifestyle or pharmacological. Outcomes of interest included psychological well-being, metacognitive ability and objective cognitive performance. To assess the risk of bias, three authors independently rated study validity using criteria based on the Critical Appraisal Skills Programme. Random-effects meta-analyses were undertaken where three or more studies investigated similar interventions and reported comparable outcomes.
Results
Twenty studies met inclusion criteria and 16 had sufficient data for inclusion in the meta-analyses. Of these, only seven were rated as being high quality. Group psychological interventions significantly improved psychological well-being (g=0.40, 95% CI 0.03 to 0.76; p=0.03) but the improvement they conferred on metacognitive ability was not statistically significant (g=0.26, 95% CI −0.22 to 0.73; p=0.28). Overall, cognitive training interventions led to a small, statistically significant improvement in objective cognitive performance (g=0.13, 95% CI 0.01 to 0.25; p=0.03). However, the pooled effect sizes of studies using active control groups (g=0.02, 95% CI −0.19 to 0.22; p=0.85) or reporting global cognitive measures (g=0.06, 95% CI –0.19 to 0.31; p=0.66) were non-significant.
Conclusions
There is a lack of high-quality research in this field. Group psychological interventions improve psychological well-being and may also improve metacognition. A large, high-quality study is indicated to investigate this further. There is no evidence to suggest that cognitive interventions improve global cognitive performance and the clinical utility of small improvements in specific cognitive domains is questionable. There is a lack of research considering lifestyle interventions and poor quality evidence for pharmacological interventions.
PROSPERO registration number
CRD42017079391.
Keywords: subjective cognitive decline, metacognition, group interventions, psychologcial well-being, systematic review
Strengths and limitations of this study.
This is a comprehensive systematic review, including meta-analysis, of the effectiveness of psychological, cognitive, lifestyle and pharmacological interventions in subjective cognitive decline.
Rather than solely focussing on cognitive outcome measures, this systematic review also evaluates the effectiveness of the interventions on psychological well-being and metacognition.
The studies included in the systematic review are generally of a low quality and this makes it difficult to draw firm conclusions.
Introduction
Subjective cognitive decline (SCD) describes self-reported acquired difficulties with cognitive functioning, in the presence of normal performance on objective measures of cognition and no impairment of daily functioning.1 SCD has attracted alternative names, including subjective memory impairment and subjective memory decline (SMD). The reported prevalence of SCD is variable ranging from 18% to 55% of memory clinic attendees.2–5 However, there is no evidence-based consensus on best management for SCD and the priority of memory services is on treating patients with cognitive difficulties arising from established neurodegenerative disorders.6
The difficulty in treating patients with SCD stems from its aetiological heterogeneity. Broadly, two distinct groups of patients exist—those in whom SCD represents preclinical Alzheimer’s disease (AD) and those in whom it does not. There is accumulating evidence for the former with Mitchell’s meta-analysis7 finding that older people with SCD were twice as likely to subsequently develop dementia. Indeed, patients presenting with SCD may already have subclinical and subtle cognitive decline suggesting an early manifestation of neurodegeneration.8 Furthermore, there is a positive correlation between subjective cognitive complaints and amyloid deposition9 10 and imaging studies have found brain changes indicative of AD in some patients with SCD.11 12 However, SCD represents a heterogenous patient group and patients without preclinical AD are less likely to demonstrate these changes.
These findings have led to growing interest in SCD, especially in the context of prodromal AD, because targeted treatments at this earlier stage could have the potential to slow or even prevent progression to AD. However, this should not detract from the reality that the majority of patients with SCD do not have preclinical AD. A recent observational study found only 14% of patients with SCD progressed to mild cognitive impairment (MCI) or AD over a 6-year follow-up13while a systematic review14 highlighted that SCD symptoms frequently remit. For this non-preclinical AD group, functional psychiatric illness, personality traits, physical illness, psychosocial stress and the effects of alcohol and drug use are likely to be contributory factors.
Research into cerebrospinal fluid (CSF)15 and neuroimaging biomarkers9 10 16 suggest they hold promise for distinguishing between preclinical and non-preclinical AD in patients with SCD but they are not routinely used in clinical practice. Therefore, currently, for the vast majority of patients with SCD, it is not possible to make this important distinction in a timely manner and, often, only regular follow-up, over a number of years,13 17 will reveal the underlying aetiology.
As well as identifying preclinical neurodegenerative dementias, there is an additional aspect to treating patients with SCD that must not be overlooked and this relates to the distressing symptoms that they experience. Self-perception of cognitive difficulties can lead to anger, increased stress and fear of dementia,18 while there is growing evidence that features of anxiety and depression are common in patients with SCD.19 Therefore, patients with SCD, regardless of aetiology, would benefit from interventions that improve psychological well-being.
Given the lack of evidence-based treatments to offer patients with SCD in the clinic, alternative options need to be sought. Metacognition, an individual’s insight into their own cognitive functioning,20may be of relevance as a therapeutic target because, by definition, SCD involves an individual’s underestimation of their cognitive ability relative to objective testing. Metternich21 demonstrated that this patient group had significantly poorer metacognitive abilities than controls. As an overestimate of cognitive impairment may be related to difficulties in evaluating cognitive performance (ie, metacognitive difficulties), improving metacognitive ability may reduce the subjective cognitive impairment experienced by these patients.
Three systematic reviews evaluating interventions for SCD have been published.18 22 23 Metternich and colleagues’18 found that ‘expectancy change’, which included interventions such as cognitive restructuring or psychoeducation to change beliefs about cognition, was significantly more effective at improving metacognition than a non-active control intervention. A limitation of this systematic review was that 9 of the 14 studies included involved participants who were healthy volunteers and did not necessarily have SCD. Cavenelli22 reviewed six studies of cognitive interventions for SCD and found improvements in objective cognitive performance, often limited to the cognitive domain being trained. The most recent systematic review23 on this topic, perhaps benefitting from being the first since the conceptualisation of the term SCD,1 used a more rigorous inclusion criteria and found a small effect size for all non-pharmacological interventions (NPI).
Purpose of current review
There is no consensus on the best treatment for SCD. We acknowledge the importance, both clinically and in research, of distinguishing between preclinical and non-preclinical dementia types of SCD but are mindful that this is often difficult in the majority of cases in clinical practice. Therefore, this review is a pragmatic analysis of which treatment, if any, should be offered to patients presenting with SCD in clinical settings when CSF and neuroimaging biomarker investigations are not routinely available.
In order to establish the best current treatment evidence, we aimed to conduct a systematic review of all types of interventions (psychological, cognitive, lifestyle and pharmacological) and to evaluate their effects on psychological well-being, metacognition and objective cognitive performance. Psychological well-being was chosen as an outcome measure because psychological distress is common in SCD,18 19metacognitive ability because it may be inversely linked to subjective cognitive complaints21 especially in non-preclinical dementia SCD and objective cognitive performance as this has previously been identified as the main outcome in intervention studies in SCD23 and may reflect the subtle impairment found in this patient group.
Methods
Search strategy and selection criteria
We searched PubMed, Web of Science, Cochrane Systematic Reviews Database, PsycINFO and CIANHL in August 2017. Search terms used were: ‘memory’, ‘cognitive’ or ‘forgetfulness’ AND ‘subjective’, ‘functional’, ‘benign’, ‘self-reported’, ‘complaints’, ‘complainer’ or ‘healthy’ AND ‘training’, ‘intervention’, ‘treatment’, ‘therapy’ or ‘medicine’ (see online supplementary appendix 1 for further details on search strategy). We did not apply limits for language or date of publication. Furthermore, reference lists of included studies were manually scanned for additional relevant papers.
bmjopen-2018-021610supp001.pdf (270.3KB, pdf)
Inclusion and exclusion criteria
We included studies where participants, either all or a separately analysed subgroup, had SCD defined as being self-reported cognitive complaints, without objective evidence of deficits on cognitive testing and unaccounted for by medical or psychiatric causes.1 The intervention delivered needed to fall within the domains of psychological, cognitive, lifestyle or pharmacological. During data extraction, three authors (RB, AJB and JDH) independently assigned the study intervention to one of these domains and when there were multiple components they judged this on the most predominant activity. Outcomes of interest included psychological well-being, metacognition and objective cognitive performance. Studies with active and non-active comparator groups were included. There were no age restrictions and only randomised controlled trials (RCTs) were included. Studies including patients with MCI or dementia were excluded as were those including patients with significant psychiatric or physical comorbidities.
Assessment of trial quality
In order to assess the risk of bias, three authors (RB, AJB and JDH) independently rated study validity using criteria that were based on the Critical Appraisal Skills Programme (www.hello.nhs.uk/documents/CAT6-Randomised_Controlled_Trials.pdf) and have been used previously.24 25
Five criteria evaluating quality and bias were assessed and based on whether studies reported the following:
Randomisation of participants to treatment and control groups.
Blinding of participants and clinicians, where possible, to treatment allocation.
Use of ‘intention to treat’ analysis for incomplete outcome data.
Participant follow-up and data collection equal in all groups.
An a priori power calculation based on at least one of our outcomes of interest.
Any disagreements between raters (RB, AJB and JDH) were resolved through discussion with a fourth author (RJH). Each checklist item above scored one point; therefore, each study could score between 0 and 5 for validity. As with previous work25 studies which independently randomised participants to treatment and control groups, used intention-to-treat analysis to manage incomplete outcome data and followed up patients in the same way (points 1, 3 and 4 above) were deemed to be high quality.
Data extraction
The studies’ demographic details, participant characteristics, main findings, limitations and results in the form of means and SD for each outcome measure were independently extracted by the three authors (RB, AJB and JDH).
Statistical analysis
We compared intervention and control groups post-intervention using RevMan software. The programme uses Hedges adjusted g26 to calculate a standardised mean difference (SMD) which is adjusted for small sample bias. Meta-analyses were performed where three or more studies investigated a comparable intervention and outcome using a random effects model. Heterogeneity was quantified using the I2 statistic.
Where a study reported multiple outcome measures for one outcome domain (eg, within psychological well-being), we calculated a composite measure to provide a single quantitative measure for meta-analysis.27
For example, if a study reported two relevant outcomes, expressed as two effect sizes (y1 and y2) the overall mean effect size for the composite measure will be:
The variance of the composite effect size is calculated as follows:
where r is the correlation coefficient describing the extent to which y1 and y2 covary. In the absence of existing literature to identify a suitable correlation, we reported composite effect sizes calculated using a correlation of 0.5.
Further details of statistical methods are found in the supplementary material (see online supplementary appendix 1).
Patient and public involvement
There was no direct patient or public involvement in this review.
Results
Description of studies
Sixty-three potentially relevant articles were retrieved through our initial search. Of these, 20 studies met inclusion criteria; however, only 16 studies had sufficient outcome data to allow calculation of effect sizes for inclusion in meta-analyses (figure 1). The characteristics and validity of included studies are described in the online supplementary material (online supplementary data file 2: Table DS1).
Figure 1.

Details of search strategy. RCT, randomised control trial; SCD, subjective cognitive decline.
bmjopen-2018-021610supp002.pdf (299.2KB, pdf)
Of the 20 included studies, five were classified as psychological interventions—four as group psychological treatment28–31 and one as mindfulness training.32 Eleven studies were classified as cognitive or memory training,28 33–42 two as lifestyle35 43 and four as pharmacological44–47 interventions. Three studies31 33 46 examined two differing interventions from the same category while two studies investigated interventions from different categories.28 35
Participants were community dwelling in all of the studies although the source of recruitment varied—memory clinics in two studies,30 42 community centres in three studies28 37 38 and the remainder through more widespread advertisement.
Of the RCTs included in the meta-analyses, 12 had a non-active control28–30 33 36 39 41 43–47 while four had an active control.32 35 37 40 The studies included a range of outcomes and only five RCTs29 30 35 37 44 clearly stated their primary outcome a priori. Fifteen RCTs28 30 32 33 35–37 39–41 43–47 included in the meta-analyses included objective cognitive performance among their outcomes but only three of these used an assessment of global cognitive function.36 37 40 Ten studies28 30–34 38 39 41 43 46 47 reported metacognitive outcomes, of which three provided a global measure of metacognition.31 33 41 Seven studies28 30 32 33 36 39 44 reported psychological well-being outcomes. All of the RCTs reported outcome data within 2 weeks of the intervention ending and four studies30 39–41 collected further follow-up data up ranging from 1 to 6 months postintervention.
Quality of studies
According to criteria described in the methods section, seven studies29 30 35 41 43 44 47 included in the meta-analyses were rated as being of high quality. An a priori power calculation was only carried out in two studies30 35 while the analysis of incomplete outcome data was adequately addressed in only eight studies.29 30 35 41 43 44 47 Thirteen29–31 33, 35–37 39 41–47 out of 16 studies met criteria for adequate randomisation of participants and the same number of studies29 30 32 33 35 36 39 41–47 ensured adequate blinding of participants and researchers. Publication bias was assessed using funnel plots for each outcome of interest (see online supplementary appendix 2; figure DS1).
Group psychological interventions (four studies)
Four small studies28–31 investigated group psychological interventions. Three29–31 were assessed to be high quality. Their main focus included psychoeducation about cognitive ageing and the link between cognitive difficulties and stress or anxiety together with goal management, strategies to improve metacognition and relaxation training. One RCT31 which showed a reduction in anxiety symptoms in the intervention group compared with the control group could not be included in meta-analyses due to insufficient baseline data. The meta-analyses for the three remaining studies showed a significant improvement in psychological well-being postintervention (g=0.40, 95% CI 0.03 to 0.76, Z=2.12, p=0.03, total n=65, see figure 2).
Figure 2.

Forest plot comparing interventions (all types) versus control (all types) for patients with subjective cognitive decline. Outcome: psychological well-being (at the end of intervention). FMD, Functional memory disorder; SMART, Smartphone-based brain Anti-aging and Memory Reinforcement Training.
When meta-analysed, group psychological interventions28–30 conferred a positive effect on metacognition but this was not statistically significant (g=0.26, 95% CI −0.22 to 0.73, Z=1.07, p=0.28, total n=65, see figure 3). Interestingly, Metternich and coworkers30 found that their group-based therapy did not improve memory self-efficacy (MSE) immediately post-intervention but there was a significant improvement in MSE at 3 months follow-up (p=0.04).
Figure 3.
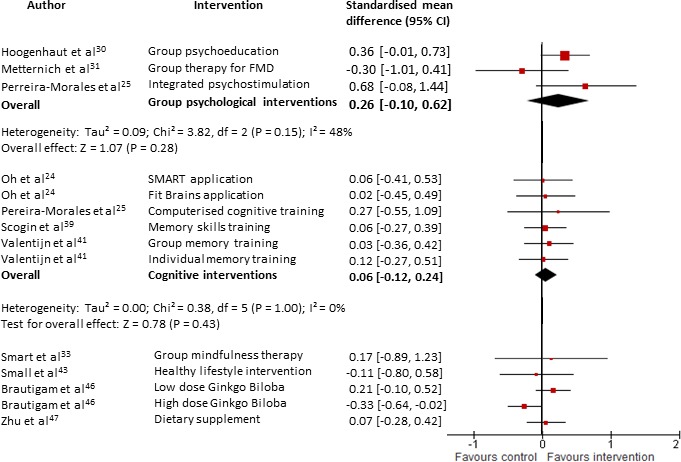
Forest plot comparing interventions (all types) versus control (all types) for patients with subjective cognitive decline. Outcome: metacognitive ability (at the end of intervention). FMD, Functional memory disorder; SMART, Smartphone- based brain Anti-aging and Memory Reinforcement Training.
Three of the studies28 29 31 measured objective cognitive performance. Hoogenhout29 did not find any significant differences in objective measures of memory (U=229, p=0.161, n=30) or executive functioning and speed (U=274, p=0.616, n=30). Similarly, there was no effect on executive function, the only cognitive domain evaluated by Van Hooren et al.31 In Pereira-Morales’ study,28 the Integrated Psychostimulation Programme, which contains cognitive training, conferred a significant improvement in a composite measure of objective cognitive performance (see figure 4).
Figure 4.
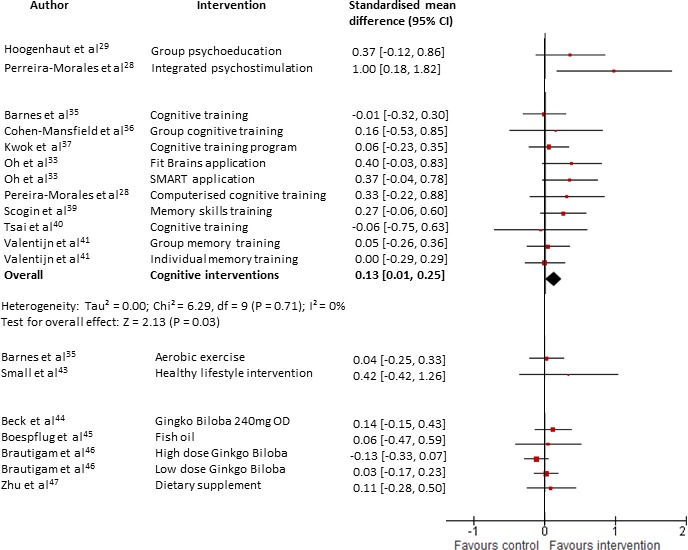
Forest plot comparing interventions (all types) versus control (all types) for patients with subjective cognitive decline. Outcome: objective cognitive performance (at the end of intervention). SMART; Smartphone-based brain Anti-aging and Memory Reinforcement Training.
Mindfulness (one study)
Smart et al32 conducted a pilot RCT (n=15) to assess the feasibility of mindfulness in SCD. The control group received psychoeducation and both groups demonstrated an improvement in MSE together with a reduction in cognitive complaints.
Lifestyle interventions (two studies)
A high-quality factorial design RCT35 showed no benefit of aerobic exercise on objective cognitive performance compared with an active control (gentle exercise that did not increase heart rate) (g=0.04, 95% CI −0.25 to 0.33, n=32, see figure 4). However, there was significant improvement in both groups.
Small’s43 small but high-quality RCT found that an intervention to promote healthy lifestyle strategies did not improve metacognition (g=−0.11, 95% CI −0.80 to 0.58, n=8, see figure 3). There was an improvement, although not reaching statistical significance, in a composite measure of verbal learning and memory and verbal fluency (g=0.42, 95% CI −0.42 to 1.26, n=8, see figure 4). The small sample size and lack of monitoring of the compliance of participants prevents any firm conclusions being drawn.
Cognitive training interventions (11 studies)
Thirteen cognitive or memory training interventions across 11 RCTs28 33–42 were evaluated. Three studies34 38 42 provided insufficient data to be included in meta-analyses. Only two studies35 41 were rated as high quality. For objective cognitive performance, significant pooled effect sizes were found (g=0.13, 95% CI 0.01 to 0.25, Z=2.13, p=0.03, total n=311, see figure 4) with no heterogeneity (I2=0%). Three studies35 37 40 had active control groups in which participants received forms of cognitive stimulation and when analysed separately, their pooled effect size was equivocal (g=0.02, 95% CI −0.19 to 0.22, Z=0.19, p=0.85, total n=132, see figure 5). Conversely, for the remaining studies which used non-active controls, the pooled effect size was significant (g=0.18, 95% CI 0.04 to 0.33, Z=2.48, p=0.01, total n=179, see figure 5).
Figure 5.

Forest plot comparing cognitive interventions versus non-active controls and active controls in separate analyses for patients with subjective cognitive decline. Outcome: objective cognitive performance (at the end of intervention).
Three studies36 37 40 used global cognitive performance outcome measures and when meta-analysed, there was no discernible improvement postintervention (g=0.06, 95% CI=–0.19 to 0.31, Z=0.45, p=0.66, total n=114, see online supplementary appendix 2: figure DS2).
Five studies28 33 36 37 39 reported psychological well-being. Each of the studies demonstrated an improvement in psychological well-being but individually none were statistically significant. However, when meta-analysed, there was a small beneficial effect on psychological well-being (g=0.25, 95% CI 0.05 to 0.46, Z=2.40, p=0.02, total n=169, see figure 2) with no heterogeneity (I2=0). Three studies33 39 42 reported metacognitive outcomes and pooled together there was no significant effect (g=0.06, 95% CI −0.12 to 0.24, Z=0.66, p=0.51, total n=165, see figure 3).
Pharmacological interventions (four studies)
Two studies investigated the effectiveness of Ginkgo biloba. Brautigam’s low-quality but relatively large trial46 included two different dosing regimens, namely high-dose and low -dose Ginkgo extract for 24 weeks. They led to conflicting results with high-dose Ginkgo causing a statistically significant worsening in metacognition while low-dose Ginkgo produced the opposite effect although statistically insignificant.
In Beck and colleagues’ trial,44 a 240 mg preparation of Ginkgo biloba was administered to the intervention group daily for 8 weeks. Both psychological well-being and objective cognitive performance improved but neither was statistically significant.
One small, low-quality trial by Boespflug et al45 found that 2.4 g fish oil daily had no effect on working memory.
Zhu and colleagues47 evaluated the effectiveness of BrainPower Advanced, a dietary supplement, taken two times per day for 12 weeks. The trial was of a poor quality with marked baseline differences in severity of cognitive complaints between groups. Analysing the primary data, there was no significant difference in metacognitive ability (g=0.07, 95% CI −0.35 to 0.31, n=47, see figure 3) or objective cognitive performance (g=0.11, 95% CI −0.28 to 0.50, n=47, see figure 4) between the groups.
Discussion
Main findings
The most obvious finding from our review is the lack of good quality evidence in this field. However, given that this is an emerging field, we attempted to be as inclusive as possible and included low-quality studies in our meta-analyses provided they did not have an inadequate or unclear rating in all five areas of bias that we assessed (see methods).
There was a statistically significant improvement in psychological well-being for interventions which incorporated psychoeducation and were delivered in group settings, although the effect size was only moderate (g=0.40).48 The studies, two of which were of high quality, are limited by small sample sizes and one of the interventions28 included cognitive training in addition to a psychological approach. Overall, however, this could be a promising intervention that can be feasibly implemented into clinical practice.
We found that cognitive interventions conferred a small but statistically significant effect (g=0.13) on cognitive outcomes which is in keeping with Smart’s earlier review.23 However, the clinical relevance of such a small improvement is easy to question. The apparent clinical utility of cognitive interventions in SCD is further undermined by our finding that meta-analysis of the three studies which used global cognitive performance outcome measures found no overall benefit. Our use of composite measures provided us with a single effect size for cognitive performance in each study but we are mindful that this merely reflects performance across the cognitive domains assessed and is not a surrogate for global cognition. Smart23 suggested that the small improvements in cognition are important because they demonstrate that cognitive enhancement and compensation is possible in this patient group. While this may be of relevance when considering the small but significant minority of persons in whom SCD represents preclinical AD, this finding has less bearing on the remaining majority who, by definition, have normal objective cognitive performance.
We found that cognitive training conferred a small but significant benefit on psychological well-being. The effects of cognitive training on psychological well-being have been poorly researched49 and there is sometimes an unproven assumption that cognitive training enhances a patient’s overall well-being by preserving cognitive function.50 This would not explain our findings given patients were evaluated within a short time frame from baseline. The larger effect on psychological well-being than on objective cognitive performance measures may reflect a significant psychogenic aetiology in many cases of SCD. However, it is important to note that the evidence is of a poor quality and this may represent a chance finding given that psychological well-being was not a primary outcome for any of the cognitive training intervention studies.
Metacognitive deficits are relevant in subjective cognitive disorders.21 Psychoeducation delivered in group settings did not lead to a significant improvement in metacognitive ability immediately after the intervention but this finding was influenced by Metternich and colleagues’30 study which found less improvement in the intervention group compared with the control (g=−0.30, 95% CI −1.01 to 0.41). However, their intervention led to a significant improvement in metacognitive ability when assessed 3 months post-treatment leading them to postulate that a period of time is needed for cognitive restructuring and the implementation of strategies into everyday life. Our findings suggest that further work is required to explore the role of group psychoeducation in improving metacognition and longer lengths of follow-up are indicated. A limitation to the literature investigating metacognitive outcomes is the broad range of subjective measures in use.
There is only limited evidence available with regards to lifestyle interventions for SCD. Exercise was evaluated in one high-quality RCT. The intervention group performed aerobic exercise while the control group performed gentle exercise designed not to increase heart rate. Both groups showed significant improvements in objective cognitive performance but there was no difference between the groups. This may suggest that exercise, regardless of intensity, could be beneficial in SCD and further RCTs with a non-active control group are indicated.
Five studies have investigated alternative medicines and medicinal supplements in SCD. Overall, the evidence for their efficacy is not encouraging. One study44 found that 240 mg daily of Ginkgo biloba for 8 weeks led to non-significant improvements in psychological well-being and cognitive performance. Brautigam and colleagues46 used two alternative doses of Ginkgo biloba and their results are conflicting. Higher doses led to significantly worse metacognition compared with control and lower doses led to statistically insignificant improvements. Fish oil45 did not improve objective cognitive performance while a dietary supplement47 did not improve either metacognition or objective cognitive performance.
In summary, psychoeducation delivered in group settings appears to be effective at improving psychological well-being, which is a relevant and important outcome, in SCD.18 19 However, individually none of the three studies demonstrated statistically significant improvements which was largely due to their small sample sizes. A large RCT is urgently needed to extrapolate our findings for this clinically practical intervention which is highly promising. Metacognition, an individual’s insight into their own cognitive functioning, is a potential area of research in SCD because deficits in this area may contribute to the condition, especially the non-preclinical dementia type. Specific interventions to improve metacognitive performance as well as to objectively quantify it are emerging20 and these may be of relevance in SCD. Cognitive interventions have a modest effect in improving objective cognitive performance and such small improvements are unlikely to be of clinical significance for the vast majority of patients with SCD who are not at risk for developing dementia. There is limited research considering lifestyle interventions in SCD and only unconvincing and poor quality evidence for pharmacological interventions in SCD.
Limitations
There is a high variability in measurement instruments used to define SCD in studies51 which limits reviews such as our own. Furthermore, SCD is a construct which includes a heterogenous group of patients that could be broadly divided into two distinct patient groups—those with and without preclinical dementia. All of the studies in our review included both groups of SCD patients together and this limits our ability to make inferences about targeted interventions for each group. Future work should investigate interventions for each group of patients separately if possible.
The poor quality of studies in this review due to a lack of clearly defined primary outcomes and small sample sizes has been highlighted previously and limits the confidence with which we can draw conclusions. Funnel plots assessing publication bias (see online supplementary appendix 2; figure DS1) appeared asymmetrical. Small sample sizes and heterogeneous interventions may be contributory factors but we are mindful that when the number of studies in the meta-analysis is small as is the case in this review, such asymmetry may arise by chance rather than reflect true publication bias.52
The interventions were heterogenous. As well as differing formats and structures of interventions which we attempted to group into broad categories, there were differences in lengths of intervention, monitoring of compliance and the motivation of participants which are more difficult to quantify. Often interventions had multiple components and we had to determine which domain was the most prominent. This may mean the most effective component of the intervention was not appropriately captured.
Similarly, the studies included in the meta-analyses contained varied control groups. In at least two32 40 of the four studies using an active control group, the control group received treatment which may have been effective in its own right thereby masking the possible effectiveness of the intervention. The other studies used non-active control groups but there is likely to have been much variability in what treatment as usual constituted.
The goal of research into interventions must be for them to be translational into clinical practice. Unfortunately, only one study30 included in the meta-analyses recruited patients from a healthcare setting while the remainder relied on convenience sampling of volunteers with subjective cognitive complaints from the community. This may limit how translatable our findings are to clinical populations.
Implications
This review demonstrates the need for higher quality studies in SCD research with a distinction made between SCD in preclinical AD and otherwise. The development of a conceptual framework for research in SCD1 should aid this. This review would support high-quality RCTs of a group psychological intervention targeting psychological well-being and metacognition in patients with SCD. Follow-up data at least 3 months postintervention should be collected. Metacognitive ability may be an important therapeutic target in SCD and interventions to directly improve this along with objective measurement tools are required.
Supplementary Material
Footnotes
Contributors: All authors made a substantial contribution to this work. RB, AJB, JDH and RJH all contributed to the conception and design of the review. RB read and screened abstracts and titles of potentially relevant studies. RB, AJB and JDH read the retained papers and were responsible for extracting data and rating their quality independently. RB drafted the paper with all the authors critically reviewing it and suggesting amendments prior to submission. All the authors had access to all the data in the study and can take responsibility for the integrity of the reported findings.
Funding: This research received no specific grant from any funding body. RB is supported by a NIHR Academic Clinical Fellowship. JH and RH are supported by the NIHR UCLH BRC.
Competing interests: None declared.
Patient consent: Not required.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data sharing statement: Details of excluded papers are available from the first author on request.
References
- 1. Jessen F, Amariglio RE, van Boxtel M, et al. . A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer’s disease. Alzheimers Dement 2014;10:844–52. 10.1016/j.jalz.2014.01.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Elfgren C, Gustafson L, Vestberg S, et al. . Subjective memory complaints, neuropsychological performance and psychiatric variables in memory clinic attendees: a 3-year follow-up study. Arch Gerontol Geriatr 2010;51:e110–e114. 10.1016/j.archger.2010.02.009 [DOI] [PubMed] [Google Scholar]
- 3. Alladi S, Arnold R, Mitchell J, et al. . Mild cognitive impairment: applicability of research criteria in a memory clinic and characterization of cognitive profile. Psychol Med 2006;36:507–15. 10.1017/S0033291705006744 [DOI] [PubMed] [Google Scholar]
- 4. Wahlund LO, Pihlstrand E, Jönhagen ME. Mild cognitive impairment: experience from a memory clinic. Acta Neurol Scand Suppl 2003;179:21–4. 10.1034/j.1600-0404.107.s179.3.x [DOI] [PubMed] [Google Scholar]
- 5. Vraamark Elberling T, Stokholm J, Høgh P, et al. . Diagnostic profile of young and middle-aged memory clinic patients. Neurology 2002;59:1259–62. 10.1212/WNL.59.8.1259 [DOI] [PubMed] [Google Scholar]
- 6. Stone J, Pal S, Blackburn D, et al. . Functional (psychogenic) cognitive disorders: a perspective from the neurology clinic. J Alzheimers Dis 2015;48(Suppl 1):S5–S17. 10.3233/JAD-150430 [DOI] [PubMed] [Google Scholar]
- 7. Mitchell AJ, Beaumont H, Ferguson D, et al. . Risk of dementia and mild cognitive impairment in older people with subjective memory complaints: meta-analysis. Acta Psychiatr Scand 2014;130:439–51. 10.1111/acps.12336 [DOI] [PubMed] [Google Scholar]
- 8. Koppara A, Wagner M, Lange C, et al. . Cognitive performance before and after the onset of subjective cognitive decline in old age. Alzheimers Dement 2015;1:194–205. 10.1016/j.dadm.2015.02.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Amariglio RE, Becker JA, Carmasin J, et al. . Subjective cognitive complaints and amyloid burden in cognitively normal older individuals. Neuropsychologia 2012;50:2880–6. 10.1016/j.neuropsychologia.2012.08.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Perrotin A, Mormino EC, Madison CM, et al. . Subjective cognition and amyloid deposition imaging: a Pittsburgh Compound B positron emission tomography study in normal elderly individuals. Arch Neurol 2012;69:223–9. 10.1001/archneurol.2011.666 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Perrotin A, de Flores R, Lamberton F, et al. . Hippocampal subfield volumetry and 3d surface mapping in subjective cognitive decline. J Alzheimers Dis 2015;48(Suppl 1):S141–S150. 10.3233/JAD-150087 [DOI] [PubMed] [Google Scholar]
- 12. Peter J, Scheef L, Abdulkadir A, et al. . Gray matter atrophy pattern in elderly with subjective memory impairment. Alzheimers Dement 2014;10:99–108. 10.1016/j.jalz.2013.05.1764 [DOI] [PubMed] [Google Scholar]
- 13. Hessen E, Eckerström M, Nordlund A, et al. . Subjective cognitive impairment is a predominantly benign condition in memory clinic patients followed for 6 years: The Gothenburg-Oslo MCI study. Dement Geriatr Cogn Dis Extra 2017;7:1–14. 10.1159/000454676 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Mendonça MD, Alves L, Bugalho P. From subjective cognitive complaints to dementia: who is at risk?: a systematic review. Am J Alzheimers Dis Other Demen 2016;31:105–14. 10.1177/1533317515592331 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Wolfsgruber S, Polcher A, Koppara A, et al. . Cerebrospinal fluid biomarkers and clinical progression in patients with subjective cognitive decline and mild cognitive impairment. J Alzheimers Dis 2017;58:939–50. 10.3233/JAD-161252 [DOI] [PubMed] [Google Scholar]
- 16. Vogel JW, Varga Doležalová M, La Joie R, et al. . Subjective cognitive decline and β-amyloid burden predict cognitive change in healthy elderly. Neurology 2017;89:2002–9. 10.1212/WNL.0000000000004627 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Eckerström M, Göthlin M, Rolstad S, et al. . Longitudinal evaluation of criteria for subjective cognitive decline and preclinical Alzheimer’s disease in a memory clinic sample. Alzheimers Dement 2017;8:96–107. 10.1016/j.dadm.2017.04.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Metternich B, Kosch D, Kriston L, et al. . The effects of nonpharmacological interventions on subjective memory complaints: a systematic review and meta-analysis. Psychother Psychosom 2010;79:6–19. 10.1159/000254901 [DOI] [PubMed] [Google Scholar]
- 19. Molinuevo JL, Rabin LA, Amariglio R, et al. . Implementation of subjective cognitive decline criteria in research studies. Alzheimers Dement 2017;13:296–311. 10.1016/j.jalz.2016.09.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Fleming SM, Dolan RJ. The neural basis of metacognitive ability. Philos Trans R Soc Lond B Biol Sci 2012;367:1338–49. 10.1098/rstb.2011.0417 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Metternich B, Schmidtke K, Hüll M. How are memory complaints in functional memory disorder related to measures of affect, metamemory and cognition? J Psychosom Res 2009;66:435–44. 10.1016/j.jpsychores.2008.07.005 [DOI] [PubMed] [Google Scholar]
- 22. Canevelli M, Adali N, Tainturier C, et al. . Cognitive interventions targeting subjective cognitive complaints. Am J Alzheimers Dis Other Demen 2013;28:560–7. 10.1177/1533317513494441 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Smart CM, Karr JE, Areshenkoff CN, et al. . Non-Pharmacologic Interventions for Older Adults with Subjective Cognitive Decline: Systematic Review, Meta-Analysis, and Preliminary Recommendations. Neuropsychol Rev 2017;27:245–57. 10.1007/s11065-017-9342-8 [DOI] [PubMed] [Google Scholar]
- 24. Cooper C, Li R, Lyketsos C, et al. . Treatment for mild cognitive impairment: systematic review. Br J Psychiatry 2013;203:255–64. 10.1192/bjp.bp.113.127811 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Rapaport P, Livingston G, Murray J, et al. . Systematic review of the effective components of psychosocial interventions delivered by care home staff to people with dementia. BMJ Open 2017;7:e014177 10.1136/bmjopen-2016-014177 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Hedges LV, Olkin I. Statistical methods for meta-analysis. New York: Academic Press, 1985. [Google Scholar]
- 27. Borenstein M, Hedges LV, Higgins JPT, et al. . Introduction to meta-analysis. Chichester: John Wiley & Sons, Ltd, 2009. [Google Scholar]
- 28. Pereira-Morales AJ, Cruz-Salinas AF, Aponte J, et al. . Efficacy of a computer-based cognitive training program in older people with subjective memory complaints: a randomized study. Int J Neurosci 2018;128:1–9. 10.1080/00207454.2017.1308930 [DOI] [PubMed] [Google Scholar]
- 29. Hoogenhout EM, de Groot RH, van der Elst W, et al. . Effects of a comprehensive educational group intervention in older women with cognitive complaints: a randomized controlled trial. Aging Ment Health 2012;16:135–44. 10.1080/13607863.2011.598846 [DOI] [PubMed] [Google Scholar]
- 30. Metternich B, Schmidtke K, Härter M, et al. . [Development and evaluation of a group therapy for functional memory and attention disorder]. Psychother Psychosom Med Psychol 2010;60:202–10. 10.1055/s-0028-1103281 [DOI] [PubMed] [Google Scholar]
- 31. van Hooren SA, Valentijn SA, Bosma H, et al. . Effect of a structured course involving goal management training in older adults: A randomised controlled trial. Patient Educ Couns 2007;65:205–13. 10.1016/j.pec.2006.07.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Smart CM, Segalowitz SJ, Mulligan BP, et al. . Mindfulness training for older adults with subjective cognitive decline: results from a pilot randomized controlled trial. J Alzheimers Dis 2016;52:757–74. 10.3233/JAD-150992 [DOI] [PubMed] [Google Scholar]
- 33. Oh SJ, Seo S, Lee JH, et al. . Effects of smartphone-based memory training for older adults with subjective memory complaints: a randomized controlled trial. Aging Ment Health 2018;22:1–9. 10.1080/13607863.2016.1274373 [DOI] [PubMed] [Google Scholar]
- 34. Andrewes DG, Kinsella G, Murphy M. Using a memory handbook to improve everyday memory in community-dwelling older adults with memory complaints. Exp Aging Res 1996;22:305–22. 10.1080/03610739608254013 [DOI] [PubMed] [Google Scholar]
- 35. Barnes DE, Santos-Modesitt W, Poelke G, et al. . The Mental Activity and eXercise (MAX) trial: a randomized controlled trial to enhance cognitive function in older adults. JAMA Intern Med 2013;173:797–804. 10.1001/jamainternmed.2013.189 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Cohen-Mansfield J, Cohen R, Buettner L, et al. . Interventions for older persons reporting memory difficulties: a randomized controlled pilot study. Int J Geriatr Psychiatry 2015;30:478–86. 10.1002/gps.4164 [DOI] [PubMed] [Google Scholar]
- 37. Kwok TC, Bai X, Li JC, Jc L, et al. . Effectiveness of cognitive training in Chinese older people with subjective cognitive complaints: a randomized placebo-controlled trial. Int J Geriatr Psychiatry 2013;28:208–15. 10.1002/gps.3812 [DOI] [PubMed] [Google Scholar]
- 38. Pike KE, Ong B, Clare L, et al. . Face-name memory training in subjective memory decline: how does office-based training translate to everyday situations? Neuropsychol Dev Cogn B Aging Neuropsychol Cogn 2017:1–29. 10.1080/13825585.2017.1366971 [DOI] [PubMed] [Google Scholar]
- 39. Scogin F, Storandt M, Lott L. Memory-skills training, memory complaints, and depression in older adults. J Gerontol 1985;40:562–8. 10.1093/geronj/40.5.562 [DOI] [PubMed] [Google Scholar]
- 40. Tsai AY, Yang MJ, Lan CF, et al. . Evaluation of effect of cognitive intervention programs for the community-dwelling elderly with subjective memory complaints. Int J Geriatr Psychiatry 2008;23:1172–4. 10.1002/gps.2050 [DOI] [PubMed] [Google Scholar]
- 41. Valentijn SA, van Hooren SA, Bosma H, et al. . The effect of two types of memory training on subjective and objective memory performance in healthy individuals aged 55 years and older: a randomized controlled trial. Patient Educ Couns 2005;57:106–14. 10.1016/j.pec.2004.05.002 [DOI] [PubMed] [Google Scholar]
- 42. Youn JH, Lee JY, Kim S, et al. . Multistrategic memory training with the metamemory concept in healthy older adults. Psychiatry Investig 2011;8:354–61. 10.4306/pi.2011.8.4.354 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Small GW, Silverman DH, Siddarth P, et al. . Effects of a 14-day healthy longevity lifestyle program on cognition and brain function. Am J Geriatr Psychiatry 2006;14:538–45. 10.1097/01.JGP.0000219279.72210.ca [DOI] [PubMed] [Google Scholar]
- 44. Beck SM, Ruge H, Schindler C, et al. . Effects of Ginkgo biloba extract EGb 761® on cognitive control functions, mental activity of the prefrontal cortex and stress reactivity in elderly adults with subjective memory impairment - a randomized double-blind placebo-controlled trial. Hum Psychopharmacol 2016;31:227–42. 10.1002/hup.2534 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Boespflug EL, McNamara RK, Eliassen JC, et al. . Fish oil supplementation increases event-related posterior cingulate activation in older adults with subjective memory impairment. J Nutr Health Aging 2016;20:161–9. 10.1007/s12603-015-0609-6 [DOI] [PubMed] [Google Scholar]
- 46. Brautigam MR, Blommaert FA, Verleye G, et al. . Treatment of age-related memory complaints with Ginkgo biloba extract: a randomized double blind placebo-controlled study. Phytomedicine 1998;5:425–34. 10.1016/S0944-7113(98)80038-X [DOI] [PubMed] [Google Scholar]
- 47. Zhu J, Shi R, Chen S, et al. . The relieving effects of brainpower advanced, a dietary supplement, in older adults with subjective memory complaints: a randomized, double-blind, placebo-controlled trial. Evid Based Complement Alternat Med 2016;2016:1–16. 10.1155/2016/7898093 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Sullivan GM, Feinn R. Using effect size-or why the p value is not enough. J Grad Med Educ 2012;4:279–82. 10.4300/JGME-D-12-00156.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Bureš V, Čech P, Mikulecká J, et al. . The effect of cognitive training on the subjective perception of well-being in older adults. PeerJ 2016;4:e2785 10.7717/peerj.2785 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Woods B, Thorgrimsen L, Spector A, et al. . Improved quality of life and cognitive stimulation therapy in dementia. Aging Ment Health 2006;10:219–26. 10.1080/13607860500431652 [DOI] [PubMed] [Google Scholar]
- 51. Rabin LA, Smart CM, Crane PK, et al. . Subjective cognitive decline in older adults: an overview of self-report measures used across 19 international research studies. J Alzheimers Dis 2015;48(Suppl 1):S63–S86. 10.3233/JAD-150154 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Higgins JP, Green S, Cochrane handbook for systematic reviews of interventions version 5.1.0. London: The Cochrane Collaboration, 2011. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2018-021610supp001.pdf (270.3KB, pdf)
bmjopen-2018-021610supp002.pdf (299.2KB, pdf)