

Abstract
Background & Aims
Eosinophilic esophagitis (EoE) is a chronic disorder in children that requires continued assessment of disease activity, involving repeated sedation, endoscopy, and biopsy analysis. We investigated whether mucosal impedance measurements can be used to monitor disease activity in pediatric patients with EoE.
Methods
We measured mucosal impedance at 3 locations in the esophagus in pediatric patients (1–18 years old; 32 with active EoE, 10 with inactive EoE, 32 with non-erosive reflux disease [NERD]) and 53 children with symptoms but normal findings from histologic analyses (controls) undergoing routine esophagogastroduodenoscopy at the Vanderbilt Pediatric Gastroenterology Clinic. Pathologists reviewed biopsies per routine protocol, determined eosinophilic density, and graded spongiosis on an ordinal visual scale. Mucosal impedance measurements were compared within patient groups. The primary outcome was correlation of mucosal impedance measurements with disease activity, based on severity of spongiosis and eosinophil counts.
Results
Mucosal impedance measurements were significantly lower in patients with active EoE at 2, 5, and 10 cm above the squamo-columnar junction (median values of 1069, 1368, and 1707, respectively) compared to patients with inactive EoE (median values of 3663, 3657, and 4494, respectively), NERD (median values of 2754, 3243, and 4387), and controls (median values of 3091, 3760, and 4509) (P<0.001 for all comparisons to patients with active EoE). We found inverse correlations between mucosal impedance measurements and eosinophil count (P<.001), and spongiosis severity (P<.001).
Conclusion
Mucosal impedance measurements may provide immediate information about mucosal inflammation in children. Patients with active EoE have significantly lower mucosal impedance values than patients with inactive EoE, NERD, or controls; mucosal impedance measurements correlate inversely with eosinophil counts and spongiosis severity. Mucosal impedance is a promising rapid and less-invasive method to monitor EoE activity in pediatric patients with EoE; it could reduce costs and risks of disease monitoring. ClincialTrials.gov no: NCT02320981
Keywords: inflammation, diagnostic, prognostic, gastroesophageal reflux disease, GERD
INTRODUCTION
Eosinophilic esophagitis (EoE) is a chronic, immune-antigen mediated esophageal disease that often begins in childhood and continues into adulthood. With an incidence of 1 per 10,000 children per year, EoE is a common condition treated by pediatric gastroenterologists.1 Symptoms vary by age and include feeding disorders, vomiting, dysphagia/food impactions.2 However, symptoms do not always correlate with disease severity and similar symptoms are found in numerous GI diseases.3 Pediatric patients appear to have a less advanced and milder form of EoE compared to adults, with up to one third having normal appearance on endoscopy.4,5 However, progression towards fibrosis and stenosis occurs with delayed diagnosis or inadequate treatment.6,7,8
Pediatric gastroenterologists, in particular, aim to promptly diagnose and aggressively treat EoE with dietary avoidance of food allergens or topical steroid treatment in order to prevent the sequelae of chronic inflammation. Assessment of disease activity and treatment success often requires repeated endoscopies with biopsies, with pediatric patients often undergoing sedated endoscopies every 2-4 months as dietary or medical therapy is adjusted.5,9 Unfortunately, while long-term consequences of repeated sedation are unclear in children, immediate pediatric anesthesia risks are well described.10,11 Due to the invasiveness and risk of monitoring modalities, and the progressive nature of this disease, there is an urgent need to develop less invasive and safer techniques for assessing esophageal inflammation in children.
EoE triggers an inflammatory cascade that compromises the epithelial barrier of the esophagus resulting in mucosal eosinophilia and spongiosis (dilated intercellular spaces [DIS] due to edema)9. If not adequately treated, it may lead to lamina propria fibrosis and esophageal strictures.7,8 Short of biopsies for histologic assessment, no method accurately assesses the mucosal effects of chronic esophageal exposure to injurious agents.
A mucosal impedance (MI) catheter was recently developed to detect changes in electrical impedance due to compromised epithelial barrier integrity and the influx of intercellular ions associated with DIS seen in esophagitis. Unlike the multichannel intraluminal impedance (MII) device, which measures impedance changes due to food and fluid transitions across the esophagus, this novel MI device is designed to measure the impedance of the surface mucosa. Prior pediatric studies attempting to differentiate mucosal changes of reflux disease with the MII device are conflicting.12,13 Compared to the MII, the MI is designed to diminish the variability of the impedance reading by decreasing the distance between impedance sensors. Adult studies validated the MI device’s ability to detect conductivity differences between endoscopically normal and inflamed esophageal mucosa.14 These studies focused on adults with gastroesophageal reflux disease (GERD) and had no histologic confirmation.14 There are no data on the utility of the MI device in the pediatric population. Based on similar but distinct histopathologic features between GERD and EoE, we hypothesized that the MI technology could detect changes in mucosal integrity in children with EoE. This takes on particular significance in children as MI validation in the pediatric EoE population could reduce costs and risks of disease monitoring.
MATERIALS AND METHODS
Patient Population and Study Design
Esophageal MI evaluation was performed prospectively in 173 pediatric patients ages 1 -18 years. Patients already scheduled for routine esophagogastroduodenoscopy (EGD) with biopsies by their primary gastroenterologist at the Vanderbilt Pediatric Gastroenterology Clinic were recruited. Exclusion criteria included: inability/unwillingness to give informed assent/consent; active comorbid conditions that would compromise the safety of prolonged anesthesia such as complex cardiac disease; presence of primary esophageal motility disorders or inflammatory bowel disease. The study was approved by the Vanderbilt Institutional Review Board (protocol #140987) and registered as a clinical trial (ClincialTrials.gov NCT02320981)
MI Catheter
Esophageal MI was measured in all patients at 2, 5 and 10 cm above the squamo-columnar junction (SCJ). These measurements were obtained via an MI catheter (Sandhill Scientific), which contains 2 electrode-sensors each 3mm in length separated by a distance of 2mm, with the distal sensor positioned 1mm from the tip of the catheter. This differs from the MII catheter, which has 7 sensors 4mm in length separated by 2cm. The electrodes connect to voltage transducer wires that run the entire length of the thin catheter and attach to the study computer. The transducer provides a maximum of 10 mA at 2 kHz. Collected data are instantaneously uploaded into the acquisition software providing immediate MI measurements (ohms). We describe an investigational use of a product or device not yet approved by the FDA for this purpose.
Diagnostic Group Definitions
Based on histologic, endoscopic and diagnostic features enumerated below, patients were classified into 4 groups: active-EoE, inactive-EoE, NERD, and controls (disease-negative group). The groups were defined as follows: Active-EoE was defined as any patient with ≥ 15 eosinophils per high power field in at least one biopsy specimen; eosinophilia needed to be limited to the esophagus; and other causes of esophageal eosinophilia were excluded. Proton pump inhibitor-responsive esophageal eosinophilia (PPI-REE) was ruled-out by lack of prior response to an 8-week course of PPI therapy. Inactive-EoE was defined as any patient with a history of active-EoE determined to be in histologic remission with <15 eosinophils per high power field in all biopsy specimens.15, 16 NERD was defined per practice guidelines as the presence of reflux symptoms, normal mucosa on endoscopy with abnormal histologic findings of esophagitis (i.e. <15 eosinophils per high power field and mild reactive epithelial changes) and/or an abnormal MII.17 Controls were symptomatic but with normal endoscopy, normal histology and, if performed, a normal MII study.
MI Measurements and Data Acquisition
Patients were assigned a de-identified number to ensure confidentiality. First, the investigator entered the coded number into the MI-measurement acquisition software (InSight; Sandhill Scientific) on the study computer. Patients underwent general anesthesia by an anesthesiologist. The endoscopist performed standard upper endoscopy, taking note of the locations of the upper esophageal sphincter and SCJ. The esophageal mucosa was examined for signs of injury, including mucosal breaks, edema, rings, exudates, furrowing, stricturing, erythema, and friability. Duodenal and gastric biopsies were obtained as indicated for routine evaluation. The MI catheter was manually guided by the endoscopist through the working channel of the endoscope until both sensors were visible through the scope camera. The endoscopist positioned the sensors directly on the esophageal mucosa at the pre-selected intervals of 2, 5 and 10 cm above the SCJ. The sensors remained in direct contact with the mucosa at each point for 5 seconds once a stable impedance reading was captured as determined by study staff. The endoscopists remained blinded to the MI measurements. After measurements were obtained, the MI catheter was removed. Esophageal biopsies were obtained at the pre-selected intervals of 2, 5, and 10 cm above the SCJ. Patients scheduled to undergo MII had this placed after the endoscopic procedure was complete. The study procedure only prolonged anesthesia-time by approximately 3 minutes.
Coded data were analyzed with BioView Analysis software (Sandhill Scientific). Pathologists blinded to MI measurements reviewed biopsies from the 3 esophageal sites assessing epithelial changes, including inflammation, spongiosis and peak eosinophil counts per high power field using a 40× magnification providing a field of view of 0.55mm. A single blinded-pathologist subsequently graded spongiosis on an ordinal visual scale (normal, mild, moderate or severe). Basic demographic information, medications, mucosal histology as well as MII results were also collected from the electronic medical record. The primary pediatric gastroenterologist determined patients’ final diagnoses based on histologic and clinical information. The mean MI measurements at each esophageal location and other de-identified patient data were entered into the Research Electronic Data Capture (REDCap) system. All authors had access to the study data and have reviewed and approved the final manuscript.
Statistical Analysis
Descriptive statistics was used to express the proportions of demographic variables by final diagnostic group, and to express the median and inter-quartile ranges of the continuous MI measurement by final diagnostic group. Kruskal-Wallis testing was used to compare continuous demographic variables against the final diagnostic group. Pearson-chi-square test was used to compare categorical variables by the final diagnostic group. Kruskal-Wallis tested differences of MI between the four diagnostic groups. Post-hoc analysis using Wilcoxon rank-sum further compared active-EoE to inactive-EoE, active-EoE to NERD and active-EoE to controls. Separate proportional-odds regression models tested associations of MI with eosinophil counts and spongiosis severity. The association depicted by the LOWESS-smoothing-regression was used to express the non-linear relationship between MI and eosinophil counts. Data on multiple covariates were collected for analysis. Multivariable linear regression models and F tests were used to analyze the proposed covariates (Active-EoE, Inactive-EoE, NERD, controls as well as age at endoscopy, and body mass index (BMI)) against the continuous MI measurement outcome. Interaction modeling was used for age and BMI. Hypothesis tests were considered significant for a p-value <0.05. Separate simple-logistic regression models were used to predict the probability of active-EoE using MI measurements at 2, 5 and 10cm above the SCJ. Receiver-operating-curve (ROC) analysis was performed to determine MI test characteristics.
RESULTS
173 patients were enrolled, including 32 active-EoE patients, 10 inactive-EoE patients, 32 NERD patients and 53 controls. 46 patients were excluded from the study or the final analysis because they either met the exclusion criteria, or they did not meet the apriori criteria set for including in the diagnostic categories. These included patients who were found to have: Crohns disease, erosive esophagitis due to ingestion, lactase deficiency, celiac disease, collagenous gastritis, H pylori-related gastritis, PPI-REE, eosinophilic disorders other than EoE, active EoE without PPI-REE being ruled out, and inactive EoE without PPI-REE being ruled out. The study population did not identify any patient with erosive reflux esophagitis (ERD) ; therefore ERD was not included in the final analysis.
Demographics
The age range of participants was 1 to 18 years (mean of 11 years). The mean ages were 10 years for active-EoE, 11 years for inactive-EoE, 9 years for NERD, and 11 years for controls (p=0.4). The mean BMI was 21 kg/m2 with a range of 12 kg/m2 to 44 kg/m2 (p=0.6). Sixty-one percent of the total study population were male, while the control group had significantly more females (p<0.001). 86% were Caucasian, 9% Black, 2% Hispanic, 2% Asian, and 1% other (p=0.162). Nausea and vomiting were the major chief complaints for active-EoE patients (22%). Dyspepsia was the major chief complaint for NERD patients (19%) and controls (38%). The majority of the inactive group was asymptomatic (60%). The majority of patients in all four groups were on PPI therapy including 84% of active-EoE, 90% of inactive-EoE, 66% of NERD and 57% of controls (p=0.024). Normal endoscopic features were noted in 22% of active-EoE, 80% of inactive-EoE, and 100% of NERD and controls. Active-EoE patients had more rings, exudates, and furrowing on endoscopy compared to the other groups (Table, Supplemental Digital Content 1). 28% of the active-EoE patients were newly diagnosed.
MI by Final Diagnostic Group
Kruskal-Wallis testing confirmed active-EoE patients had significantly lower MI measurements at 2, 5 and 10cm [median 1069 Ω; 1368 Ω; and 1707 Ω, respectively] compared to inactive-EoE [3663 Ω, 3657 Ω, and 4494 Ω], NERD [2754 Ω, 3243 Ω and 4387 Ω], and controls [3091 Ω, 3760 Ω and 4509 Ω] (p<0.001) (Table 1, Figure 1). Post-hoc analysis using three separate Wilcoxon rank-sum models per esophageal location confirmed active-EoE patients had significantly lower MI-measurements when compared individually to inactive-EoE (p<0.001), NERD (p<0.001), and controls (p<0.001).
Table 1.
MI Measurements by Final Diagnosis
| N | Active EoE N = 32 |
Inactive EoE N = 10 |
NERD N = 32 |
Control N = 53 |
P value | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 25% | Median | 75% | 25% | Median | 75% | 25% | Median | 75% | 25% | Median | 75% | |||
| 2 cm | 173 | 710 | 1069 | 1643 | 2037 | 3663 | 4471 | 1879 | 2754 | 3460 | 2005 | 3091 | 4619 | < .001 |
|
| ||||||||||||||
| 5 cm | 173 | 1018 | 1368 | 1853 | 2682 | 3657 | 3844 | 2120 | 3243 | 5241 | 2679 | 3760 | 5694 | < .001 |
|
| ||||||||||||||
| 10 cm | 173 | 1146 | 1707 | 2443 | 2396 | 4494 | 5616 | 2273 | 4387 | 5232 | 3395 | 4509 | 5960 | < .001 |
Median and 25th to 75th percentile MI values (Ω)
N is the number of non-missing values.
p-values represent results of Kruskall Wallis hypothesis testing
Figure 1.
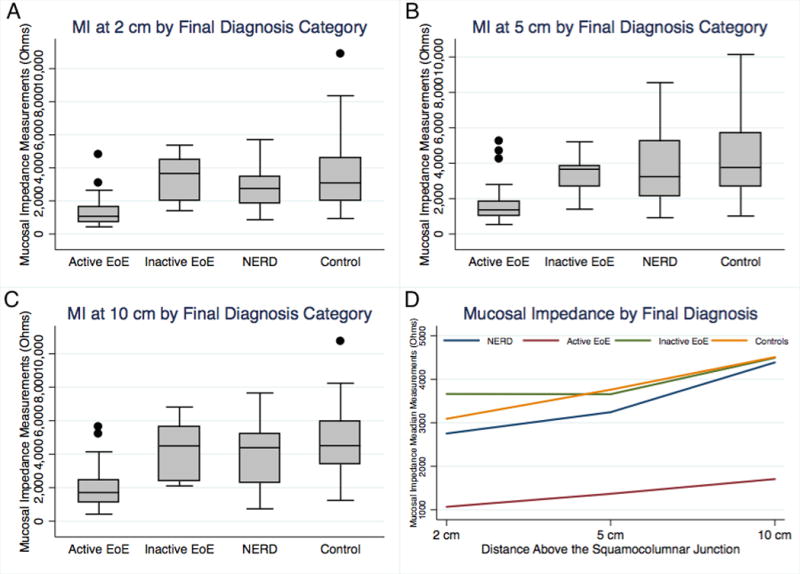
Median (IQR) MI measurements at (A) 2 cm, (B) 5 cm, and (C) 10 cm above the squamocolumnar junctions (SCJ) for the 4 study groups. (D) Median MI measurements distributed axially for each esophageal location. MI measurements were significantly lower for active-EoE compared to inactive-EoE, NERD and controls (P < .001). NERD group demonstrated non-significant lower MI pattern than inactive-EoE and controls.
Multivariable Analysis
Multivariable linear-regression analysis and F-tests with interaction modeling revealed a significant linear association of MI and active-EoE when adjusted for the final diagnostic groups (p <0.001) and BMI (p=0.014), which was significantly modified by age (p=0.042) (R2 = 0.28). However, there was insufficient evidence to show an association of MI with age (p=0.111). Residual-analysis confirmed appropriate model fit.
Disease Burden and MI
83 patients had documented eosinophilia. The mean eosinophil count was significantly higher in active-EoE (69 eosinophils) compared to inactive-EoE (2 eosinophils), NERD (1 eosinophil) and controls (none) (Table, Supplemental Digital Content 1). Proportional-odds regression determined that for every 1000 Ohm decrease in MI there was a 117% increase in the odds of higher eosinophil counts (p< 0.001). Thus, there was a statistically significant inverse correlation between MI measurements with eosinophil counts (Figure 2). Spongiosis grading was performed on 127 patients. Proportional-odds regression determined that for every 1000 Ohm decrease in MI there was an 87% increase in the odds of more severe spongiosis (p< 0.001). Thus, there was a statistically significant inverse correlation between MI measurements with spongiosis severity (Figure 3).
Figure 2.
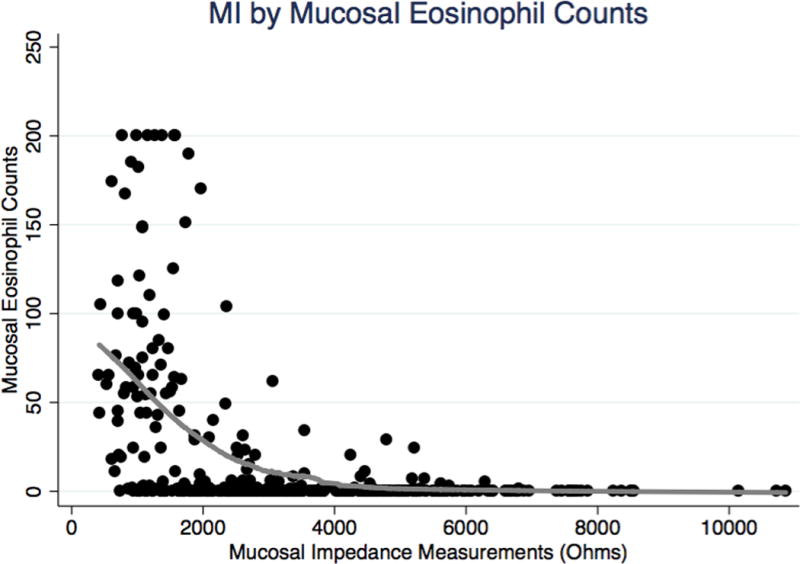
Total MI measurements by eosinophil counts. MI measurements inversely correlate with the number of eosinophils (P < .001).
Figure 3.
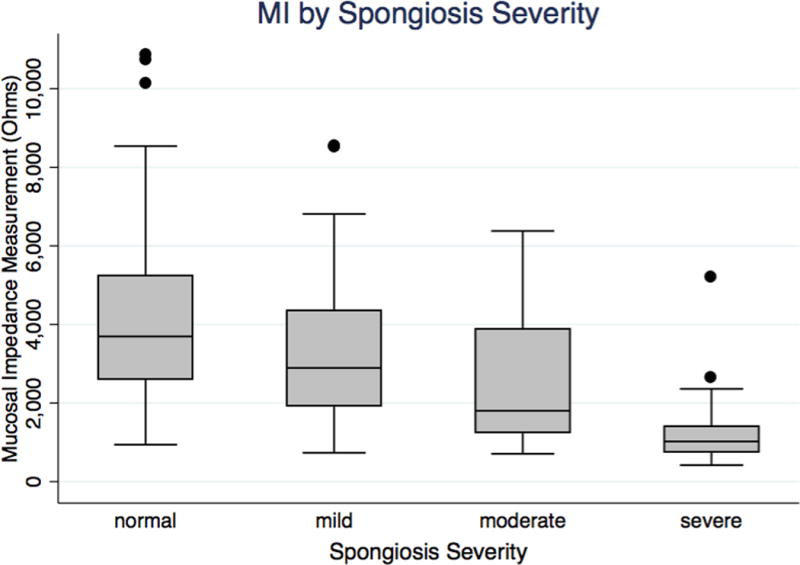
Total MI measurements by spongiosis severity grade. MI measurements inversely correlate with the severity of spongiosis (P < .001).
Predictive Probability
The MI predictive probability of active-EoE was determined using separate simple logistic regression models (Figure 4). For example, the MI values of 2213 Ohms (2cm), 2530 Ohms (5cm), 3043 Ohms (10cm) give a predictive probability of active-EoE of 75%. The MI values of 710 Ohms (2cm), 673 Ohms (5cm), 1024 Ohms (10cm) give a predictive probability of active-EoE of 95% (Figure 4).
Figure 4.
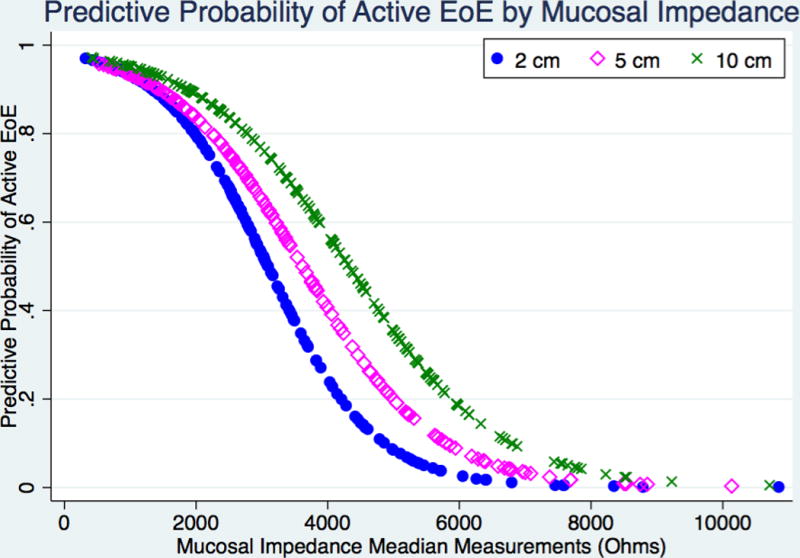
Predictive probability of active-EoE for MI measurements at 2 cm, 5 cm, and 10 cm above the squamocolumnar junction (SCJ).
Test Characteristics
ROC-analysis was performed at 2, 5, and 10 cm above the SCJ for predicting active-EoE versus inactive-EoE. Optimal MI threshold values were based on the highest combined sensitivity and specificity percentage at each esophageal location. Analysis at 2 cm above the SCJ using a cutoff point of 1410 Ohms to detect active-EoE resulted in a specificity of 100%, a sensitivity of 69%, a negative predictive value (NPV) of 50%, and a positive predictive value (PPV) of 100%. Analysis at 5 cm above the SCJ using a cutoff point of 2278 Ohms to detect active-EoE resulted in a specificity of 90%, a sensitivity of 78%, a NPV of 56%, and a PPV of 96%. Analysis at 10 cm above the SCJ using a cutoff point of 2103 Ohms to detect active-EoE resulted in a specificity of 100%, a sensitivity of 66%, a NPV of 48%, and a PPV of 100% (Table 2). Therefore, the probability of having active-EoE is very high if the MI values are below the cutoffs values of 1410 Ohms, 2278 Ohms and 2103 Ohms at 2, 5 and 10 cm above the SCJ respectively.
Table 2. ROC Analysis.
Test characteristics in predicting active EoE from inactive EoE.
| Location (above SCJ) | Threshold | Sensitivity | Specificity | PPV | NPV | ROC Area |
|---|---|---|---|---|---|---|
| 2cm | 1410 Ω | 69% | 100% | 100% | 50% | 0.90 |
| 5cm | 2278 Ω | 78% | 90% | 96% | 56% | 0.86 |
| 10cm | 2103 Ω | 66% | 100% | 100% | 48% | 0.88 |
Threshold values are based on the optimal combined sensitivity and specificity at each esophageal location for differentiating Active EoE from Inactive EoE.
SCJ: squamocolumnar junction, PPV: positive predictive value; NPV: negative predictive value; ROC: receiver operating curve
DISCUSSION
This study is the first to assess MI measurements in pediatric patients. The current gold standard for diagnosing EoE involves sedated endoscopy with at least 6 biopsies for histologic evaluation. Under existing management strategies, pediatric EoE patients may undergo sedated endoscopies every 2-4 months until adequate disease quiescence is achieved through dietary changes or medications.5,9 This is expensive, inefficient, invasive and carries risks. Moreover, endoscopic findings can be normal in 7%–33% of active EoE cases, thus supporting the need for new modalities to monitor disease activity4,5. Currently, histologic assessment is the only method to confirm disease activity, which is invasive, laborious and results are not available at the time of patient discharge.4 Given the importance of continued disease monitoring to guide management in the pediatric population and current requirements of repeated sedated endoscopy with biopsies, we sought to determine if MI measurements could be a useful tool to determine EoE activity. This study describes promising results of a new MI technology, which provides immediate evidence of active esophageal mucosal inflammation in pediatric patients consistent with those from histologic evaluations. MI measurements were significantly lower in active-EoE patients compared to inactive-EoE, NERD, and normal esophageal tissue. While unlikely to replace histologic diagnostic modalities at this time, the MI device may prove useful in providing valuable information with regards to monitoring disease activity in EoE patients as further refinements to the technology are made. Importantly, if future iterations of the MI device eliminate the need for endoscopic placement, then this device may eventually eliminate the need for obtaining biopsies and repeat endoscopies when monitoring EoE activity, potentially lowering procedural costs and risks.
In addition to the significant findings of lower impedance measurements in active EoE patients, this study showed an inverse correlation between MI measurements and disease activity measured by both eosinophil counts and spongiosis severity. These findings support the hypothesis behind the device development; inflamed tissue results in DIS with an influx of ions, thus, lowering electrical impedance.14 These correlations further support the device’s ability to delineate active EoE from inactive disease.
While the MI measurements overall had a significant inverse correlation with the eosinophil counts, the impedance measurements in a few patients with high eosinophil counts overlapped with impedance measurements of patients with no eosinophils. This may potentially be explained by an intervening air-interface surrounding the sensor, thus confounding the results. In order to address this issue, modifications in the catheter are being made to provide 360-degree esophageal mucosal contact via a balloon device.
It is important to acknowledge other potential limitations of our study. The cross-sectional study design is not devised to prove causality, although it is unlikely that patients with active EoE naturally have lower MI measurements at baseline. Ongoing prospective studies will further address this issue by analyzing MI in EoE pre and post-treatment. Although inflammation can vary within the esophagus, attempts were made to limit this bias by obtaining biopsies at the same measured esophageal location of 2, 5 and 10 cm above the SCJ. Intraluminal air/fluid contents may confound results, however, the esophagus was thoroughly suctioned before MI measurement, and visualization of the probe placement abutting the mucosal surface was confirmed. The aim of this study was to compare mucosal impedance readings to histologic findings and did not investigate the association of mucosal impedance with symptoms. However, previous studies have suggested a disconnect between EoE symptoms and the degree of histologic abnormalities.3 Ideally, the control group would have included both normal histology and normal pH-impedance testing, however, due to limitations imposed by a non-interventional study in children, only 11 patients in the control group had pH-impedance testing (all 11 had physiologic amounts of GE reflux). Similarly, the NERD group would ideally have had impedance-pH testing performed, but, for similar reasons only 8 had these studies performed (all had non-physiologic reflux). Again, these potential shortcomings are mitigated by the fact that the primary aim of our study is to compare mucosal impedance measurements to histologic changes of varying severity. Lastly, in contrast to adult studies, which noted significantly lower impedance in GERD patients, our pediatric NERD patients did not have significantly lower MI measurements. This difference is likely due to the lack of ERD seen not only in our study population, but in the pediatric population in general.18 This theory is further supported by prior pediatric MII studies noting lower baseline impedance measurements in ERD compared to NERD. However, unlike MI, the MII device did not correlate with the degree of histologic inflammation as determined by DIS supporting the MI catheter’s design to detect mucosal changes as opposed to intraluminal fluid shifts.13
In conclusion, this preliminary study suggests MI measurements may provide the ability to immediately detect inflammation in patients with active EoE during an EGD, guiding immediate therapeutic decisions. This needs to be confirmed by further, prospective studies. The natural progression of this concept is to create a minimally invasive device that does not require endoscopic placement and addresses potential confounders such as intraluminal fluid/air, an effort currently ongoing. If successful, it has the potential to significantly reduce risks and costs of repeated endoscopic and histologic evaluation.
Supplementary Material
What is known
Eosinophilic esophagitis (EoE) is a chronic, often progressive disorder in children
To monitor progression and response to dietary or medical interventions, repeated assessment of disease activity through histological examination of mucosal biopsies is often needed
At times, active or progressive disease occurs without significant clinical symptoms, emphasizing the need for continued monitoring strategies
What is new
Mucosal impedance (MI) measurements correlate with characteristic histologic changes of EoE
MI measurements provide immediate information about mucosal inflammation in children with EoE
MI measurements may serve as a surrogate for histologic examination in patients followed for EoE and provide the basis for the development of non-invasive monitoring of disease activity
Acknowledgments
Grant Support: Mary Allyson Lowry, received grant funding under the Vanderbilt Training Grant in Gastroenterology supported by the NIH grant 2T32DK007673-21 and 5T32 DK007673-22. Core Services performed through Vanderbilt University Medical Center’s Digestive Disease Research Center are supported by NIH grant P30DK058404. The REDCap database is supported by the NCATS/NIH grant UL1 TR000445.
Abbreviations
- BMI
Body Mass Index
- DIS
Dilated Intercellular Space
- EoE
Eosinophilic Esophagitis
- ERD
Erosive Reflux Disease
- EGD
Esophagogastroduodenoscopy
- GERD
Gastroesophageal Reflux Disease
- MI
Mucosal Impedance
- MII
Multichannel Intraluminal Impedance
- NERD
Non-Erosive Reflux Disease
- PPI-REE
Proton Pump Inhibitor-Responsive Esophageal Eosinophilia
- ROC
Receiver Operating Curve
- REDCap
Research Electronic Data Capture
- SCJ
Squamocolumnar Junction
Footnotes
Disclosures and Conflicts of Interest: Vanderbilt University and Sandhill Scientific Incorporated jointly hold the patent on the MI concept and device. The authors of this study have no disclosures to declare.
Author Contributions: ML: study design; patient recruitment; acquisition of data; statistical analysis; drafting of the manuscript. MV: study concept and design; editing the manuscript. HC: study design; acquisition of data; editing the manuscript. JS: statistical analysis; editing the manuscript. TH: study design; patient recruitment; acquisition of data; editing the manuscript. SA: study design; patient recruitment; acquisition of data; editing the manuscript.
References
- 1.Furuta GT, Liacouras CA, Collins MH, et al. Eosinophilic Esophagitis in Children and Adults: A Systematic Review and Consensus Recommendations for Diagnosis and Treatment. Gastroenterology. 2007;133:1342–1363. doi: 10.1053/j.gastro.2007.08.017. [DOI] [PubMed] [Google Scholar]
- 2.Noel RJ, Putnam PE, Rothenberg ME. Eosinophilic esophagitis. N Engl J Med. 2004;351:940–941. doi: 10.1056/NEJM200408263510924. [DOI] [PubMed] [Google Scholar]
- 3.Pentiuk S, Putnam PE, Collins MH, et al. Dissociation between symptoms and histological severity in pediatric eosinophilic esophagitis. J Pediatr Gastroenterol Nutr. 2009;48:152–160. doi: 10.1097/MPG.0b013e31817f0197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kim HP, Vance RB, Shaheen NJ, et al. The prevalence and diagnostic utility of endoscopic features of eosinophilic esophagitis: a meta-analysis. Clin Gastroenterol Hepatol. 2012;10:988–96.e5. doi: 10.1016/j.cgh.2012.04.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Muir AB, Merves J, Liacouras CA. Role of Endoscopy in Diagnosis and Management of Pediatric Eosinophilic Esophagitis. Gastrointestinal Endoscopy Clinics of NA. 2016;26:187–200. doi: 10.1016/j.giec.2015.08.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Schoepfer AM, Safroneeva E, Bussmann C, et al. Delay in Diagnosis of Eosinophilic Esophagitis Increases Risk for Stricture Formation in a Time-Dependent Manner. Gastroenterology. 2013;145:1230–1236.e2. doi: 10.1053/j.gastro.2013.08.015. [DOI] [PubMed] [Google Scholar]
- 7.Straumann A, Schoepfer AM. Therapeutic concepts in adult and paediatric eosinophilic oesophagitis. Nature Reviews Gastroenterology & Hepatology. 2012;9:697–704. doi: 10.1038/nrgastro.2012.182. [DOI] [PubMed] [Google Scholar]
- 8.Attwood SE. Current hurdles in the management of eosinophilic oesophagitis: The next steps. WJG. 2013;19:790. doi: 10.3748/wjg.v19.i6.790. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Furuta GT, Katzka DA. Eosinophilic Esophagitis. N Engl J Med. 2015;373:1640–1648. doi: 10.1056/NEJMra1502863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Wilder RT, Flick RP, Sprung J, et al. Early exposure to anesthesia and learning disabilities in a population-based birth cohort. Anesthesiology. 2009;110:796–804. doi: 10.1097/01.anes.0000344728.34332.5d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gleich SJ, Flick R, Hu D, et al. Neurodevelopment of children exposed to anesthesia: Design of the Mayo Anesthesia Safety in Kids (MASK) study. Contemporary Clinical Trials. 2015;41:45–54. doi: 10.1016/j.cct.2014.12.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Salvatore S, Hauser B, Devreker T, et al. Esophageal impedance and esophagitis in children: any correlation? J Pediatr Gastroenterol Nutr. 2009;49:566–570. doi: 10.1097/MPG.0b013e3181a23dac. [DOI] [PubMed] [Google Scholar]
- 13.Salvatore S, Salvatoni A, Van Berkel M, et al. Esophageal Impedance Baseline Is Age Dependent. J Pediatr Gastroenterol Nutr. 2013;57:506–513. doi: 10.1097/MPG.0b013e31829b68cd. [DOI] [PubMed] [Google Scholar]
- 14.Ates F, Yuksel ES, Higginbotham T, et al. Mucosal Impedance Discriminates GERD From Non-GERD Conditions. YGAST. 2015;148:334–343. doi: 10.1053/j.gastro.2014.10.010. [DOI] [PubMed] [Google Scholar]
- 15.Papadopoulou A, Koletzko S, Heuschkel R, et al. Management Guidelines of Eosinophilic Esophagitis in Childhood. J Pediatr GastroenterolNutr. 2014;58:107–118. doi: 10.1097/MPG.0b013e3182a80be1. [DOI] [PubMed] [Google Scholar]
- 16.Liacouras CA, Furuta GT, Hirano I, et al. Eosinophilic esophagitis: Updated consensus recommendations for children and adults. Journal of Allergy and Clinical Immunology. 2011;128:3–20.e6. doi: 10.1016/j.jaci.2011.02.040. [DOI] [PubMed] [Google Scholar]
- 17.Sherman PM, Hassall E, Fagundes-Neto U, et al. A Global, Evidence-Based Consensus on the Definition of Gastroesophageal Reflux Disease in the Pediatric Population. 2009;104:1278–1295. doi: 10.1038/ajg.2009.129. [DOI] [PubMed] [Google Scholar]
- 18.Borrelli O, Salvatore S, Mancini V, et al. Relationship between baseline impedance levels and esophageal mucosal integrity in children with erosive and non-erosive reflux disease. Neurogastroenterol Motil. 2012;24:828–e394. doi: 10.1111/j.1365-2982.2012.01947.x. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.