

Abstract
Introduction:
To compare the quality of life, areas of social, emotional, behavioural and mental problems and family functionality of gifted children and children of normal intelligence.
Methods:
The study included 49 gifted children aged 9-18 years and 56 age and gender-matched healthy children of normal intelligence. The Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL), and the Children’s Depression Rating Scale were applied to all the cases. The Quality of Life Scale for Children, the Depression Scale for Children, the Trait-State Anxiety Inventory, and the Strengths and Difficulties Questionnaire- Adolescent Form were completed by all the participants. All the parents completed the Family Evaluation Scale, the Strengths and Difficulties Questionnaire- Parents Form and the Parents Form of the Quality of Life Scale for Children.
Results:
Compared to children of normal intelligence, gifted children described themselves as more inattentive and lively, social functionality was reported to be low and they had a worse perception of their physical health status. Gifted boys were determined to have more depressive symptoms than gifted girls. The parents of boys of normal intelligence reported lower academic performance than the parents of giftedboys. This difference was not determined for girls between the cases and comparative groups.
Conclusion:
All the findings obtained in this study suggest that gifted children are at risk in respect of mental health. Therefore, to be able to become healthy adults in a biopsychosocial aspect, it is important for the future of gifted children that this status can be identified at an early age, that they can receive appropriate education, that support and counselling are provided for emotional needs and that parents and teachers are fully informed.
Keywords: Gifted children, quality of life, family functionality, depression, social-emotional-behavioural problems
INTRODUCTION
The definition of giftedness comprises of superior intelligence level, superiority in academic field and leadership skills, creativity and artistic skills (1). For the full understanding of the potentials of gifted students, the using of multiple diagnostic tools gives more reliable results (2). In Turkey, in determining of gifted students, teacher notification, aptitude tests, individual intelligence tests are used generally (3).
The different social and emotional needs arising from the asynchronousity between the cognitive and physical development of gifted children and problems that may arise from them are a subject that has been studied for years (4). It is emphasized that when compared with their peers, gifted children emotionally and socially can have different needs in comparison with their peers (5,6). There are data about gifted children’s being socially more isolated, less sensitive to thoughts of their peers, less adapted to their environment and society (7).
Reasons such as extreme and unrealistic expectations of parents and teachers, their intense concerns, discordance between the child’s ability and teaching, difficulties in peer relationships, difficulty in understanding by the social environment, suggest that behavioral and emotional problems may occur more frequently in this group (8-10).
Beside these, in the gifted group; psychological problems such as inadequacy in learning (1, 11), high test anxiety and general anxiety level (12), somatization (10), lack of self-confidence accompanied by depressive symptoms (13), attention deficit hyperactivity disorder were also found to accompany more frequently (1).
Therefore, it is important to assess gifted children in many dimensions such as academic field, self-perception, social skills, emotional and mental health (14).
Families with gifted children are reported to have higher levels of anxiety to meet the special needs of their children. These families feel themselves more inadequate and less equipped. It is reported that they are less permissive to their children and tend to use an authoritarian style. Because of these features, a gifted child is not only face difficulties in school functioning and peer relations; but also known to face difficulties in family relationships (15).
In the literature, there could not find any studies which had researched the quality of life of gifted children. In this study, it was also aimed to compare the quality of life of gifted children with those of normal intelligence. Besides; it is aimed to assess social, emotional, behavioral and family functionalities of a gifted child and to compare these functions with children with normal intelligence.
On the basis of the data in the literature; in this study, hypotheses were formed that by comparison to peers with normal intelligence, gifted child’s having exhibited anxiety and depressive mood in increased frequency; having had more problems on social, behavioral, and family functionalities, and for these reasons the quality of life of gifted children will be at a lower level.
METHOD
Sample
The study was conducted with the participation of 49 gifted and 56 normal intelligent children and adolescents. Gifted and normal intelligent children and adolescents without chronic medical disease, aged 9-18 years, haven’t had a psychiatric diagnosis of axis I according to criteria DSM-IV-TR, who voluntarily accept to participate in the study, were compared in terms of quality of life by the Pediatric Quality of Life Inventory (PedsQL); social, emotional, behavioral, psychological problem areas by the Strength and Difficulties Questionnaire (SDQ), the State-Trait Anxiety Inventory for Children (STAI-C), the Child Depression Inventory (CDI) and the Children Depression Rating Scale Revised (CDRS-R), family functioning by the Family Assesment Device (FAD).
A sample group was created by choosing gifted children (Group I) who study at Izmir Narlıdere Sıdıka Akdemir Science Art Center (INSASAC), and choosing normal intelligent children (Group II) with total intelligence points ranged 90-109 in the Wechsler Intelligence Scale for Children (WISC-R) who study at Ertugrul Gazi Primary School (EGPS). The WISC-R is first applied to children who are guided by the thought of being gifted, so that they can gain the right to education at INSASAC. Secondly, the Primary Mental Abilities (PMAs) Test is applied to children with a total intelligence score of 130 or higher in WISC-R to analyze their skill areas. Group I in the study has been made up of gifted children studying in INSASAC. Therefore, the previously applied WISC-R and PMAs were not reapplied.
In order to ensure the equivalence of compared groups, family relationships and sociodemographic factors that may affect the mental state of children have been identified. These factors are scored in sociodemographic data form as education status, number of siblings in the family, birth order, number of people living in the family, mother’s age at birth, maternal education status, maternal employment status, paternal education status, paternal employment status, cohabitation of mother and father, family income, residing, family history of medical illness, family history of mental disorder, school success, and peer relationships. It was aimed to make the groups equivalent through the criteria. However, the unmatched factors were matched to the closest criteria (number of siblings, income status, birth order, education status of mother and father, mother’s age at birth).
Tools
Schedule for Affective Disorders and Schizophrenia for School Age Children-Present and Lifetime Version-Turkish Version (K-SADS-PL-T): The K-SADS-PL-T is a semi-structured interview form which is developed by Kaufman et al. (1997) in order to determine past and present psychopathologies of children and adolescents according to DSM-III-R and DSM-IV diagnostic criteria. The K-SADS-PL-T is applied through interviews with the parents and the child himself/herself (16). Validity and reliability study for the Turkish form was done by Gökler et al (2004)(17).
Pediatric Quality of Life Inventory (PedsQL): The scale developed by Varni et al. in 1999 (18), aims to evaluate the general quality of life in the 2-18 age group. The scale consists of four sub-sections that question physical, emotional, social, and school-related functioning. Validity and reliability study for the Turkish form of the inventory, was done for 2–18 age group (19).
State-Trait Anxiety Inventory for Children (STAI-C): Turkish adaptation studies of the scale which is developed in order to determine the level of “trait and state anxiety” of the students, was done by Özusta (1993) (20).The adaptation studies of the scale demonstrate its applicability in the 9–16 age group.
Child Depression Inventory (CDI): The scale which adapted to Turkish in 1990 by Öy, is filled by the child (21).The maximum score on the twenty-seven-item scale is 54 and cut-off score is recommended as 19 (22,23).Elevation of total score points the severity of the depression level.
Strength and Difficulties Questionnaire (SDQ): For use in screening psychological problems in children and adolescents, SDQ was developed by Robert Goodman in 1997. The SDQ comprise of 25 questions, some of which question positive behavioral characteristics and some of which question negative ones. These questions were collected in five sub-headings. These headings are conduct problems, inattention and hyperactivity, emotional problems, peer problems and social behaviors (24). Scale which had adapted to Turkish was observed to be consistent and reliable (25).
Children Depression Rating Scale Revised (CDRS-R): The CDRS-R is a 17-item scale used in clinical trials to assess the severity of depression and alterations in depressive symptoms in depressed children and adolescents. Twenty-eight points and below indicate remission, and 40 points and above indicate depression. This scale was adapted to Turkish in 2012. As a result of the validity and reliability studies, the Turkish version of CDRS-R was found to have good psychometric properties (26).
Family Assesment Device (FAD): The scale was developed by Brown University and Butler Hospital in the US in 1983 (27). It was developed to evaluate whether the family fulfill their functions and to reveal the problems, it consists of 60 items. Turkish adaptation study was done by Bulut (1990) (28).
Primary Mental Abilities (PMAs) Test: The PMAs test was developed by T. G. Thurstone and L. L. Thurstone as three separate forms to be applied to 5–7, 7–11 and 11–17 age groups to identify mental ability fields. Adapting to Turkish was made in 1953 by the Ministry of National Education (29).
Sociodemographic data form: In the form of data, regarding child; date of birth, education status, school success, peer relationships, birth order, regarding parents; education levels, cohabitation status, occupational status and income levels, number of children, diagnosis of physical disease and/or mental disorder in parents/children are included.
Collection of Data
The study was found to be ethical in accordance with the decision of the Ethics Committee of Dokuz Eylul University dated 05.01.2012 and numbered 2012/01-23. On account of the decree of Ministry of National Education dated 04.04.2012 and numbered 21194, a permit has been issued in order to carry out the study in involved schools. Also obtaining permission from INSASAC and EGPS Directorates, all children were informed individually. Verbal approval was obtained from 105 students who met the participation criteria and accepted to participate. Written acknowledgment and scales which expected to be filled by the parents were sent to families of both groups and collected through their children. At this stage, verbal approvals were obtained through informing the family about the study and interviewing them by the telephone or face-to-face. The sociodemographic data form and the CDRS-R were filled in by the clinician for the students who were given an approval, and in order to exclude any psychiatric diagnosis that may be present in the children in both groups, the K-SADS-PL-T was applied in the parent-teacher interview room in their schools. By children individually, PedsQL 8–12, 13–18 age form; CDI, STAI-C, SDQ adolescent form were filled in respectively. The FAD, SDQ-parent form, PedsQL 8–12 or 13–18 age parent form were filled in by mothers and/or fathers of the students.
In order to evaluate their total intelligence score, The WISC-R psychometric intelligence test was applied to children in Group II by an experienced psychologist at Dokuz Eylul University Medical School Hospital. The WISC-R psychometric test, which was applied to the children in Group I at guidance and research center during the application to INSASAC was not reapplied to the students in the scope of the study.
Evaluation of Data
SPSS Windows 15.0 package program was used in statistical evaluation of the data obtained in study.
The mean age between group I and II was compared using t-test in independent groups, and gender distribution was compared using Pearson Chi-Square Test. T-test and two-way analysis of variance (two-way ANOVA) were used in the analysis of continuous data between the two groups. Two-way ANOVA was used to assess together the statistical significance of the differences in mean values over scale scores and the effects of the group (group I and group II) and gender (male and female) over averages of the scale scores. Statistical significance level was determined as p <0.05.
RESULTS
Group I and group II were matched in terms of gender ratios. Thus, gender distribution does not differ between group I and group II. There are 22 girls (45%), 27 boys (55%) in group I and 25 girls (45%), 31 males (55%) in group II. There was not also any significant difference between the age distributions of the groups (group I: 132.00 ± 16.26 months, group II: 131.78 ± 16.66 months, t =0.103, p =0.947, t-test in independent groups).
There was not any statistically significant difference between the group I and group II in terms of the scores which are taken in STAI-C for assessing their state and trait anxiety, CDI for assessing their depression levels, CDRS-R for assessing their depressive symptoms by the clinician (p>0.05) (Table 1). In the CDRS-R, males in group I were found to have statistically significant higher depressive scores than females in group I (2x2 ANOVA, group I *gender, F=4.797, p=0.031, Partial η2=0.045) (Figure 1). When the effect of the puberty on depressive scores in group I was examined, there was not any statistically significant difference in the mean of CDRS-R scores of boys who are in prepubertal and pubertal age range, in group I (Mann-Whitney U test, Z=-1.763, p=0.078).
Table 1.
Mean Scores of Children in Group I and Group II
| Group I Mean±SD | Group II Mean±SD | p* | |
|---|---|---|---|
| State Anxiety Score | 25.94± 5.04 | 25.25± 4.75 | 0.473 |
| Trait Anxiety Score | 27.45±6.08 | 29.34±5.75 | 0.105 |
| CDI Total Score | 4.08±3.70 | 4.45±3.62 | 0.612 |
| CDRS-R Total Score | 32.20±4.0 | 31.70±2.90 | 0.447 |
| SDQ-Emotional problems | 1.24±1.61 | 1.30±1.62 | 0.854 |
| SDQ-Behavioural problems | 1.14±1.27 | 1.03±1.11 | 0.649 |
| SDQ-Inattention/ Hyperactivity | 3.08±1.94 | 2.23±2.12 | 0.036 |
| SDQ- Peer problems | 2.08±1.68 | 2.37±1.40 | 0.333 |
| SDQ- Social Behaviour | 8.63±1.86 | 9.05±1.35 | 0.185 |
| SDQ-Total DifficultyScore | 7.36±4.86 | 6.94±4.11 | 0.632 |
| SDQ-Impact Score | 0.40±1.45 | 0.55±1.29 | 0.589 |
| PedsQL-Physical Health Total Score | 83.36±17.30 | 89.08±7.72 | 0.037 |
| PedsQL-Emotional Functioning Score | 81.22±17.42 | 85.71±13.36 | 0.139 |
| PedsQL-Social Functioning Score | 90.30±12.30 | 94.35±8.09 | 0.051 |
| PedsQL-School Functioniwng Score | 83.67±13.76 | 84.10±12.65 | 0.867 |
| PedsQL-Total Score | 84.55±11.48 | 88.28±7.47 | 0.056 |
T-test in independent groups
CDI: Child Depression Inventory, CDRS-R: Children Depression Rating Scale Revised, SDQ: Strength and Difficulties Questionnaire, PedsQL: Pediatric Quality of Life Inventory
Figure 1.
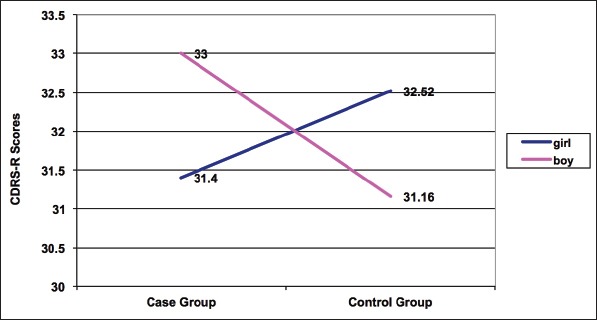
T Scores of Children Depression Rating Scale Revised (CDRS-R) in Group I and Group II According to Genders
*2 x 2 ANOVA case group*gender, F=4.797, p=0.031, Partial η2=0.045
In group I and group II, subtest scores of the SDQ child form which is applied for screening psychological problems were compared with the t-test in independent groups, and statistically significant differences were found only between the scores of inattention/hyperactivity subtest scores (p = 0.036) while there was no significant difference in other subtest scores (Table 1). A statistically significant difference was found between the genders in the peer problems subtest of SDQ child form (2×2 ANOVA gender effect; F=5.038, p=0.027, partial η2=0.048) (Table 2). Boys in both groups which participate to study, were found to have higher levels of peer relationship problems than girls at a statistically significant level, in peer problems subtest. A statistically significant interaction was found between gender and groups as a result of 2×2 ANOVA (gender × group) applied in the SDQ child form social behaviour subtest (F=4.821, p=0.004, partial η2=0.125) (Table 2). Girls in both groups which participate to study were found to have higher social behaviors than boys at a statistically significant level in SDQ child form social behaviour subtest (2×2 ANOVA gender effect; F=12.024, p=0.001, partial η2=0.106) (Table 2).
Table 2.
Mean Scores Between Genders in Peer Problems Subtest and Social Behaviour Subtest of Strength and Difficulties Questionnaire Child Form, Social Functioning Subtest of Pediatric Quality of Life Inventory Self-Assessment Form
| Mean±SD | p | |
|---|---|---|
| SDQ Child Form Peer Problems | 0.027* | |
| Boy (n=58) | 2.53 ± 1.65 | |
| Girl (n=47) | 1.87 ± 1.31 | |
| SDQ Child Form Social Behaviour | 0.001* | |
| Boy (n=58) | 8.39 ± 1.88 | |
| Girl (n=47) | 9.42 ± 0.97 | |
| PedsQL Self-Assessment Form Social Functioning | 0.020* | |
| Boy (n=58) | 90.40 ± 11.62 | |
| Girl (n=47) | 95.00 ± 8.14 |
2×2 ANOVA
GGA: Güçler Güçlükler Anketi, ÇİYKO: Çocuklar için Yaşam Kalitesi Ölçeği.
There was not any statistically significant difference between mean scores of the group I and group II, in the subtest scores of the SDQ- parental form, according to t-test results in independent groups (p >0.05) (Table 3).
Table 3.
Mean Scores of Parents of Children in Group I and Group II
| Group I Mean±SD | Group I Mean±SD | p* | |
|---|---|---|---|
| PedsQL Physical Health Total Score | 80.56±15.09 | 80.34±17.23 | 0.945 |
| PedsQL Emotional FunctioningScore | 80.83±15.72 | 81.02±14.81 | 0.951 |
| PedsQL Social Functioning Score | 89.18±12.09 | 89.72±13.10 | 0.827 |
| PedsQL School Functioning Score | 86.73±13.75 | 81.90±16.81 | 0.115 |
| PedsQL Total Score | 83.94±10.07 | 83.26±11.46 | 0.751 |
| PedsQL Psychosocial Health Total Score | 85.48±10.92 | 84.21±11.52 | 0.566 |
| SDQ Emotional problems | 1.87±1.81 | 1.41±1.60 | 0.169 |
| SDQ Behavioural problems | 1.47±1.18 | 1.10±1.35 | 0.143 |
| SDQ Inattention/Hyperactivity | 2.56±2.50 | 2.66±2.32 | 0.837 |
| SDQ Peer problems | 2.33±1.41 | 2.16±1.47 | 0.546 |
| SDQ Social behaviour | 8.66±1.58 | 8.87±1.57 | 0.504 |
| SDQ Total Difficulty Score | 8.29±4.77 | 7.32±4.33 | 0.280 |
| SDQ Impact Score | 0.22 ± 0.95 | 0.21± 0.80 | 0.931 |
| FAD Problem Solving | 1.63±0.58 | 1.60±0.49 | 0.778 |
| FAD Communication | 1.51±0.45 | 1.52±0.38 | 0.883 |
| FAD Roles | 1.70±0.39 | 1.73±0.43 | 0.702 |
| FAD Affective Responsiveness | 1.39±0.40 | 1.34±0.39 | 0.543 |
| FAD Affective Involvement | 1.69±0.30 | 1.83±0.37 | 0.035 |
| FAD Behaviour Control | 1.55±0.25 | 1.58±0.28 | 0.571 |
| FAD General Functioning | 1.42±0.43 | 1.40±0.41 | 0.740 |
T-test in independent groups
PedsQL: Pediatric Quality of Life Inventory, SDQ: Strength and Difficulties Questionnaire, FAD: Family Assesment Device
In order to evaluate the overall quality of life of Group I and Group II, PedsQL self-assessment scale was applied to children and adolescents. The average of Physical Health Total Score, a subtest of the PedsQL self-assessment scale, were found to be statistically significantly lower in Group I than Group II (p=0.037) (Table 1). It was found that gender difference did not contribute to the difference between the groups (2×2 ANOVA gender effect; F=0.395, p=0.531, partial η2=0.004).
The average of PedsQL social functioning scores was found to be in a lower level close to statistically significantly lower level in group I than group II (F=3.898, p=0.051, partial η2=0.037) (Table 1). When the effect of gender factor to social functioning subtest of PedsQL self-assessment scale was examined, boys participating in the study were seen to have statistically significantly lower PedsQL social functioning scores than girls participating in the study (2×2 ANOVA gender effect; F=5.559, p=0.020, partial η2=0.052) (Table 2). In 2×2 ANOVA, statistically significantly low school functioning subtest scores of PedsQL parental assessment scale were obtained in group II males (F=2.732, p=0.048, partial η2=0.076) (Table 4).
Table 4.
Mean Scores According to Groups and Genders in Children Depression Rating Scale Revised and School Functioning Subtest of Pediatric Quality of Life Inventory Parent Assessment Form
| Group 1 | Group 2 | TOTAL | |
|---|---|---|---|
| Children Depression Rating Scale Revised | |||
| Girl | (n=22) 31.40 ± 2.71 | (n=25) 32.52 ± 3.58 | (n=47) 32.00 ± 3.22 |
| Boy | (n=27) 33.00 ± 4.73 | (n=31) 31.16 ± 2.14 | (n=58) 32.01 ± 3.67 |
| PedsQL Parent Assessment Form School Functioning | |||
| Girl | (n=22) 87.04 ± 12.59 | (n=25) 87.20 ± 11.99 | (n=47) 87.12 ± 12.14 |
| Boy | (n=27) 86.48 ± 14.85 | (n=30) 77.50 ± 19.06 | (n=57) 81.75 ± 17.63 |
PedsQL: Pediatric Quality of Life Inventory
In “Affective Involvement” subtest of FAD, statistically significantly lower scores were obtained in group I than group II (p=0.035). There was not any significant difference between genders (2×2 ANOVA gender effect, F=0.024, p=0.877). In other FAD subtests, there was not found any statistically significant difference between groups (Table 3).
DISCUSSION
In this study, gifted children were evaluated for depressive symptomatology. The depressive symptoms identified with CDRS-R by the clinician were found to be higher in gifted boys than in gifted girls. In conclusions of this study, gifted children have defined themselves more inattentive and hyperactive than children and adolescents with normal intelligence in SDQ self-report scale. In group I and group II, when their quality of life was compared, the gifted children were found to perceive their social functionalities and physical health statuses worse. Normal intelligent boys’ having been perceived as having low school functionalities by their parents is also one of the observed results. According to own evaluations of children and adolescents, another result obtained in the study is that boys participating in the study have reported lower social functioning and higher peer relationship problems than girls. In a way that supports this finding, according to their own evaluations, girls also assessed themselves more social than boys. When family functionalities was assessed with FAD, it was determined that family members of gifted children showed more interest, care and love for each other than group II.
In the literature, there are different datas about the anxiety level of children with high intelligence level. Some of the studies reports increased frequency of anxiety in individuals with high intelligence levels (10, 12, 30–33); while the other part reports that there is not any increased frequency of anxiety (34–38). Perfectionism (39), school changes, high academic expectations (40), future-related concerns, difficulties related to family and friends were often seen to be among sources of stress that can create anxiety complaints for gifted children (38). Good intelligence and problem-solving strategies are emerging as a protective factor against anxiety (35). This study supports the argument that anxiety is not seen at a higher level in gifted children than in children with normal intelligence.
In our study, while there was not any difference in depressive complaints according to self-report and clinical interview in most of all gifted children by comparison with group II, boys of gifted children group had high depressive scores in CDRS-R. In the literature, in some of the studies, it has been reported that increased frequency of depressive complaints are seen in gifted children (32, 41, 42), but in another studies, it is emphasized that gifted children show similar depressive symptoms like their peers with normal intelligence and ability level (43–46). This situation may be related to children’s having a chance to define existing depressive symptoms more easily in a clinical interview with CDRS-R. In relation to this finding, gifted children’s being able to hide their depression is indicated in the literature. This attitude may appear as a factor that makes it difficult to understand the frequency and extent of depression in gifted children. When the reason for increased depressive symptoms in boys of gifted group was considered, boys of group I were seen to have greatest difficulty score in SDQ emotional and total difficulty scores based on both self-report and parental reports.This increase in difficulty levels may be responsible for the increased frequency of depressive symptoms.
In our study, even though gifted children are not perceived inattentive and hyperactive by their families, they perceive themselves more inattentive and hyperactive than childrens in group II perceive themselves.
Inattention and hyperactivity are separate cognitive and behavioral processes. The SDQ applied in the study does not separately evaluate inattention and hyperactivity. Therefore, it is not clear whether this group perceived themselves as inattentive or hyperactive.
Due to their fast learning capacity, gifted children’s learning lessons easily and finding the curriculum boring is known (13). Since also hyperactivity symptoms of gifted children manifest especially in school during learning in the classroom, parents may not be able to observe inattention and hyperactivity symptoms in their children. When the literature is reviewed, it is reported that Attention Deficit Hyperactivity Disorder (ADHD) coexists in gifted children (47–49), and ADHD clinical features are similar to those of children with normal and low intelligence (50, 51). However, Webb (2001) and Brazilian Council for Giftedness (CONBRASD) report that gifted children may misdiagnose with ADHD in an increasingly false positive ratio, even if they do not have ADHD (52, 53). In the literature, it has been reported that inattention and hyperactivity symptoms can be seen in gifted children due to curriculum incompatibility or high creative ability features, which in turn can lead to false positive ADHD diagnosis (51, 52). In our study, applying K-SADS-PL-T to both groups, ADHD and other axis I diagnoses were excluded. Inattention and hyperactivity complaints that gifted children have identified at increased frequency are thought to be related to giftedness. According to the results obtained from this study, when performing differential diagnosis of ADHD, it is necessary to consider giftedness. According to these results, gifted children’s perceiving themselves more problematic than group II in inattention and hyperactivity subtest of SDQ self-assestment scale suggests that they have difficulties in the classroom environment because of high skill level. On the other hand, according to the results of this study, gifted children’s attributing themselves more problems on inattention and hyperactivity than their parents is thought.
The quality of life is defined as the way in which an individual perceives their own situation within the culture and values system. This concept includes the physical health, mental health, level of independence, social relations, environmental factors and personal beliefs of the individual’s (54). The World Health Organization (1948) states that a multidimensional measure is necessary to assess health-related quality of life correctly and exactly, and this measure should at least include physical, psychological and social dimensions (55). In this study, group I perceived themselves more unhealthy than group II in terms of physical health quality of life. Gifted children mostly just focus on areas which they are capable of. Occupations which are related to outer world and are outside of their skill areas, mostly doesn’t motivate these children enough. Activities which outside of their skill areas remain at a restricted level. Assuming that out-of-school social and cultural activities are complementary to physical health, it can be supposed that the limitations in these areas lead to gifted children’s perceiving themselves physically more unhealthy. Besides, gifted children’s showing intense curiosity and interest to outer world is known (56). This intense curiosity and interest may also increase the awareness of these children to their bodies, as a result of this, normal physical difficulties which experienced may be reducing the perceived quality of life associated with physical health.
Furthermore, it is also known that gifted children can hide the depression which they are experiencing (41). In this respect, gifted children may tend to somatize their feelings, or may experience difficulty in the psychomotor field. In this study, although there were not determined any differences in the state-trait anxiety levels and depressive symptom levels of gifted children to group II, some studies in the literature reports increased somatization in gifted children (34, 57). In this respect, the tendency of the gifted children to somatize their feelings may be the source of their feeling of being unhealthy. On the other hand, gifted children’s feeling themselves physically unhealthy may be arised from the greater number of adolescents in group I than in group II and also from physiological changes in adolescence.
It is known that the ability area of academically talented gifted children only includes one field like mathematics or language and these children generally have an avarage level of ability in other fields (3). Due to the fact that this study is made up of gifted children with talent in fields other than the psychomotor field and especially with talent in academic field, though this children demonstrate a superiority in their fields, their inability of demonstrating that superiority in the psychomotor field may have led them to perceive themselves more unhealthy. Therewithal, gifted children’s being at a less developed affective and psychomotor stage in proportion to their increased cognitive development stage is entitled as internal dyssynchrony. This internal dyssynchrony may have led them to perceive themselves physically more unhealthy.
When gifted children are examined regarding peer relationships, different results are observed. While some of the studies identify prominent problems in gifted children in peer relationships (58–60), some do not identify any problem (61). Also according to results of this study, giftedness negatively affects the quality of life in social functionalities. Especially in social-functioning quality of life subtest of PedsQL; given that gifted boys’ having had the lowest social-functioning quality of life points when they evaluate themselves, it can be predicted that the quality of life of gifted boys in social functionalities is at a risk. Moreover, depressive complaints which are seen in gifted boys more often than gifted girls may have negatively affect their quality of life in social functionalities. Because depressive disorder is a psychiatric disorder that increases the risk of medical disease and causes prominent problems in academic, work and social areas and in the family. On the other hand, gifted boy’s problems in the quality of life in social functioning may have led them to have higher depressive scores in the CDRS-R.
When academic achievement and school attendance are based as indicators of school functioning, it is reported that some of gifted children are successful, but the group experiencing difficulties in the emotional, behavioral, social, and psychological area that affect school life is unsuccessful (62). In addition; school success reduces in the presence of conditions like negative familial factors, comorbid learning disabilities, and ADHD (63, 64). As a result of Matthews’ study (2006), it has been determined that about 10-20% of the group out of the education system is gifted children (65). In this study, presence of no difference in school functioning between gifted child and child with normal intelligence suggests that giftedness does not foresee a better school life. On the other hand, K-SADS-PL-T which is applied on this study, does not examine a diagnosis like learning disability which may affect school functioning, though it examine ADHD. Therefore, it could not determined that whether gifted children which involved in this study have a diagnosis of learning disability or not. Superior cognitive properties of gifted children may have hidden their learning disabilities and this situation may be the reason why they can not show better school functioning than children with normal intelligence.
In the literature, when strengths and difficulties which are seen in gifted children in social, emotional and behavioral areas are examined, while some of the studies reported that more problems were seen in gifted children in the social and emotional area (9, 66); other studies emphasize that the level of social, emotional and behavioral problems of gifted children is similar to their peers with normal intelligence and ability level (35, 67, 68). In our study, apart from inattention and hyperactivity scores, there was not find any increased complaint in gifted children in other difficulty areas of SDQ. Also, when compared to group II, there was not determined any difference in social behaviour area as a strength area.
In terms of peer relationships, popularity can become a decisive factor in peer relationships of gifted children. Studies related to this subject have reported that gifted children are popular among their peers and no peer-related problems are identified (58, 59). However, it is also reported in the literature that the qualities which enable gifted children to succeed and get ahead of others, can also lead them to be excluded from peer groups and social environments, and that these qualities may lead them to be alone in peer group (61).When the literature is reviewed on the difference between genders in peer relationships and social behaviour subtests of SDQ, it is generally seen that girls are better in peer relationships than boys. When the psychometric properties of strenghts and difficulties questionnaire are examined, it is reported that girls are more social than boys and although boys’ problems are not statistically significant, their problems in peer relationships are more prominent than girls (69). In this respect, also in our study, independently from the groups, findings that difficulties in peer relationships in girls are less than those in boys and strengths in social skills are better than those in boys, suggest that this is due to psychometric properties of SDQ.
In the quality of life scale, gifted children’s having fewer points than group II at a level close to statistically significant level in fields in which they assessed themselves, suggests that being gifted affects the quality of life negatively. Dauber and Benbow (1990) report that gifted children grow away from the normal population as their intelligence increases (70). In addition, they emphasize that their existing superiorities estrange them from the environment. Results obtained from this study support results of Dauber and Benbow (1990).
In the FAD which was given to families of groups in order to evaluate whether families fulfill their functions or not, and in order to reveal problem areas, in affective involvement subtest, group I scored statistically significant fewer points, but this difference was not observed among the genders. This finding points that family members of gifted children in group II show a sufficient level of interest, care, and love for each other. No significant difference was found with FAD in other subtests. This shows the similarity of families of group I and group II, and supports equivalence of families. The conclusion of our study is parallel to conclusions of Gubbins’ study (2002) which shows gifted childrens are encouraged and supported by their parents consistently.
In this study, due to the fact that problems emerging in social, emotional, behavioural areas and the decline in quality of life in gifted children carry a risk of arising from a psychological disorder, the exclusion of any mental disorder by the K-SADS-PL-T; group I and group II’s matching by sociocultural and sociodemographic aspects; having a heterogeneous sampling which represents gifted children in terms of various ability fields, are strengths of the study.
Small sample group and the inability of the K-SADS-PL-T to determine a diagnosis such as learning disorder which may affect school functioning, are limited aspects of the study.
All findings in this study suggest that gifted children are at risk for mental health. In terms of gifted children’s being at this risk, educational interventions and assists are needed psychologically and also those are needed so that they achieve their potential. Because of the risks which gifted children have in terms of their mental health, there is a need for longer surveillance studies which can be evaluated in more dimensions and have greater sample.
Footnotes
Ethics Committee Approval: Ethical approval was obtained from the Ethics Committee of Dokuz Eylül University (Decision No. 2012 / 01-23 dated 05.01.2012)
Informed Consent: Written informed consent form was obtained from all patients.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept - FE, BB; Design - FE, BB; Supervision - BB, SA; Resource - FE, AÖÇ, SA; Materials - FE, BB; Data Collection and/ or Processing - FE, AÖÇ; Analysis and/or Interpretation - FE, BB, SA; Literature Search - FE, AÖÇ, SA, BB; Writing - FE, SA, BB; Critical Reviews - SA, BB.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study has received no financial support.
REFERENCES
- 1.Pfeiffer SI. The gifted: clinical challenges for child psychiatry. J Am Acad Child and Adolesc Psychiatry. 2009;48:787–790. doi: 10.1097/CHI.0b013e3181aa039d. [DOI] [PubMed] [Google Scholar]
- 2.Moore AD. Gifted and talented children and youth. In: Bullock LM, editor. Exceptionalities in Children and Youth. USA: Allyn and Bacon Inc; 1992. pp. 420–448. [Google Scholar]
- 3.Metin N. Üstün Yetenekli Çocuklar. Ankara: Öz Aşama Matbaacılık; 1999. [Google Scholar]
- 4.Terrassier JC. Intellectually precocious children. Arch Pediatr. 2009;16:1603–1606. doi: 10.1016/j.arcped.2009.07.019. [DOI] [PubMed] [Google Scholar]
- 5.Delisle JR, Lewis BA. The survival guide for teachers of gifted kids. USA: Barnes and Noble Publishing; 2003. [Google Scholar]
- 6.Freeman J. The Psychology of Gifted Children: Perspectives on Development and Education. Great Britain: John Wiley and Sons; 1985. [Google Scholar]
- 7.Yun K, Chung D, Jang B, Kim JH, Jeong J. Mathematically gifted adolescents have deficiencies in social valuation and mentalization. Plos One. 2011;6:e18224. doi: 10.1371/journal.pone.0018224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Morawska A, Sanders M. An evaluation of a behavioural parenting intervention for parents of gifted children. Behav Res Ther. 2009;47:463–470. doi: 10.1016/j.brat.2009.02.008. [DOI] [PubMed] [Google Scholar]
- 9.Morawska A, Sanders MR. Patenting gifted and talented children: what are the key child behaviour and parenting issues? Aust N Z J Psychiatry. 2008;42:819–827. doi: 10.1080/00048670802277271. [DOI] [PubMed] [Google Scholar]
- 10.Vanmeerbeek M, Van OS, Boüüaert C, Burette P. Gifted children and the family physician. Presse Med. 2006;35(1 Pt 2):86–90. doi: 10.1016/s0755-4982(06)74528-6. [DOI] [PubMed] [Google Scholar]
- 11.Brody LE, Mills CJ. Gifted children with learning disabilities: a review of the issues. J Learn Disabil. 1997;30:282–296. doi: 10.1177/002221949703000304. [DOI] [PubMed] [Google Scholar]
- 12.Beer J. Depression, general anxiety, test anxiety, and rigidity of gifted junior high and high school children. Psychol Rep. 1991;69(3 Pt 2):1128–1130. doi: 10.2466/pr0.1991.69.3f.1128. [DOI] [PubMed] [Google Scholar]
- 13.Bénony H, Van Der Elst D, Chahraoui K, Bénony C, Marnier JP. Link between depression and academic self-esteem in gifted children. Encephale. 2007;33:11–20. doi: 10.1016/s0013-7006(07)91554-7. [DOI] [PubMed] [Google Scholar]
- 14.Neihart M. Services that meet social and emotional needs of gifted children. In: Purcell JH, Eckert RD, editors. Designing Services and Programs for High Ability Learners: A Guidebook for Gifted Education. California: Corwin Press; 2006. pp. 112–124. [Google Scholar]
- 15.Enç M, Çağlar D, Özsoy Y. Özel Eğitime Giriş. Ankara: Ankara Üniversitesi Eğitim Fakültesi Yayınları, No:49, Kalite Matbaası; 1975. [Google Scholar]
- 16.Kaufman J, Birmaher B, Brent D, Rao U, Flynn C, Moreci P, Williamson D, Ryan N. Schedule for affective disorders and schizophrenia for schoolage children-present and lifetime version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry. 1997;36:980–988. doi: 10.1097/00004583-199707000-00021. [DOI] [PubMed] [Google Scholar]
- 17.Gökler B, Ünal F, Pehlivantürk B, Kültür EÇ, Akdemir D, Taner Y. Okul çağıçocuklarıiçin duygulanım bozukluklarıve şizofreni görüşme çizelgesi -şimdi ve yaşam boyu şekli- Türkçe uyarlamasının geçerlik ve güvenilirliği. Çocuk ve Gençlik Ruh SağlığıDergisi. 2004;11:109–116. [Google Scholar]
- 18.Varni JW, Seid M, Rode CA. The PedsQL: measurement model for the pediatric quality of life inventory. Med Care. 1999;37:126–139. doi: 10.1097/00005650-199902000-00003. [DOI] [PubMed] [Google Scholar]
- 19.Memik NC, Ağaoğlu B, Coşkun A, Üneri OS, Karakaya I. Çocuklar için yaşam kalitesi ölçeğinin 13–18 yaşergen formunun geçerlik ve güvenirliği. Turk Psikiyatri Derg. 2007;18:353–363. [PubMed] [Google Scholar]
- 20.Özusta HŞ. Çocuklar için durumluk-sürekli kaygıenvanteri uyarlama, geçerlik ve güvenirlik çalışması. Türk Psikoloji Dergisi. 1995;10:32–44. [Google Scholar]
- 21.Öy B. Çocuklar için depresyon ölçeğinin öğrenciler ve çocuk ruh sağlığıkliniğine başvuran çocuklara uygulanması. Çocuk Psikiyatrisi Uzmanlık Tezi, Hacettepe Üniversitesi Tıp Fakültesi, Psikiyatri Anabilim Dalı, Ankara; 1990 [Google Scholar]
- 22.Kovacs M. Rating scale to assess depression in school aged children. Acta Paedopsychiatr. 1981;46:305–315. [PubMed] [Google Scholar]
- 23.Kovacs M. The Children's Depsession Inventory (CDI) Psychopharmacol Bull. 1985;21:995–998. [PubMed] [Google Scholar]
- 24.Goodman R, Meltzer H, Bailey V. The Strengths and Diffuculties Questionnarie: a pilot study on the validity of the self-report version. Int Rev Psychiatry. 2003;15:173–177. doi: 10.1080/0954026021000046137. [DOI] [PubMed] [Google Scholar]
- 25.Güvenir T, Özbek A, Baykara B, Arkar H, Şentürk B, İncekaş S. Güçler ve güçlükler anketi'nin (GGA) Türkçe uyarlamasının psikometrik özellikleri. Çocuk ve Gençlik Ruh SağlığıDergisi. 2008;15:65–74. [Google Scholar]
- 26.Alşen S, Emiroğlu N. Children Depression Rating Scale Ölçeğinin Psikometrik Özellikleri. YayınlanmamışUzmanlık Tezi, Dokuz Eylül Üniversitesi Tıp Fakültesi, Çocuk ve Ergen Ruh Sağlığıve HastalıklarıAnabilim Dalı, İzmir. 2012 [Google Scholar]
- 27.Epstein NB, Baldwin LM, Bishop DS. The McMaster Family Assessment Device. J Marital Fam Ther. 1983;9:173–180. [Google Scholar]
- 28.Bulut I. Aile Değerlendirme ölçeği (ADÖ) El Kitabı. Ankara: ÖzgüzelişMatbaası; 1990. pp. 720–727. [Google Scholar]
- 29.Milli Eğitim Bakanlığı. Temel Kabiliyetler Testi 7–11 Uyarlama ÇalışmasıEl Kitabı. Ankara: Milli Eğitim Basımevi; 2001. [Google Scholar]
- 30.Mısırlı-Taşdemir Ö. Yayınlanmamışyüksek lisans tezi. Trabzon: Karadeniz Teknik Üniversitesi, Sosyal Bilimler Enstitüsü; 2003. Üstün yetenekli çocuklarda mükemmelliyetçilik, sınav kaygısı, benlik saygısı, kontrol odağı, öz yeterlilik ve problem çözme becerileri arasındaki ilişkinin incelenmesi. [Google Scholar]
- 31.Webb J, Amend ER, Webb NE, Goerss J, Beljan P, Olenchak FR. Misdiagnosis and Dual Diagnoses of Gifted Children and Adults: ADHD, Bipolar, OCD, Asperger's, Depression and Other Disorders. 2nd ed. Scottsdale, Arizona: Great Potential Press; 2005. [Google Scholar]
- 32.Ciğerci ZC. Yayımlanmamışyüksek lisans tezi. Sakarya Üniversitesi; 2006. Üstün yetenekli olan ve olmayan ergenlerde benlik saygısı, başkalarıtarafından algılanma ve psikolojik belirtilerin karşılaştırılması. [Google Scholar]
- 33.Yoo JE, Moon SM. Counseling needs of gifted students: An analysis of intake forms at a University-Based Counseling Center. Gift Child Q. 2006;50:52–61. [Google Scholar]
- 34.Grossberg I. Relationships between IQ and emotional adjustment in gifted latency age children. Unpublished doctoral dissertation, Department of Counseling (Education), Wayne State University. 1985 [Google Scholar]
- 35.Preuss LJ, Dubow EF. A comparison between intellectually gifted and typical children in their coping responses to a school and a peer stressor. Roeper Rev. 2004;26:105–111. [Google Scholar]
- 36.Scholwinski E, Reynolds CR. Dimensions of anxiety among high IQ children. Gift Child Q. 1985;29:125–130. [Google Scholar]
- 37.Roome JR, Roomney DM. Reducing anxiety in gifted children by inducing relaxation. Roeper Rev. 1985;7:177–179. [Google Scholar]
- 38.Peterson JS, Duncan N, Canady K. A longitudinal study of negative life events, stress, and school experiences of gifted youth. Gift Child Q. 2009;53:34–49. [Google Scholar]
- 39.LoCicero KA, Ashby JS. Multidimensional perfectionism in middle school age gifted students: A comparison to peers from the general cohort. Roeper Rev. 2000;22:278–319. [Google Scholar]
- 40.Kanlı E. Üstün Zekâlıve Normal Ergenlerin Mükemmeliyetçilik, Depresyon ve KaygıDüzeyleri Arasındaki İlişkilerin İncelenmesi M. Ü. Atatürk Eğitim Fakültesi Eğitim Bilimleri Dergisi. 2011;33:103–121. [Google Scholar]
- 41.Jackson PS, Peterson J. Depressive disorder in highly gifted adolescents. Journal of Secondary Gifted Education. 2003;14:175–186. [Google Scholar]
- 42.Webb JT. Existential depression in gifted individuals 2013. Available at: http://sengifted.org/existential-depression-in-gifted-individual/
- 43.Baker JA. Depression and suicidal ideation among academically talented adolescents. In: Moon SM, Reis SM, editors. Social/Emotional Issues, Underachievement and Counseling of Gifted and Talented Students. CA: Corwin Press, A SAGE Publications Company; 2004. pp. 21–31. [Google Scholar]
- 44.Bartell NP, Reynolds WM. Depression and self-esteem in academically gifted and nongifted children: A comparison study. J Sch Psychol. 1986;24:55–61. [Google Scholar]
- 45.Neihart M. Anxiety and depression in high ability and average ability adolescents. Unpublished doctoral dissertation, University of Northern Colorado, Greeley. 1991 [Google Scholar]
- 46.Turakitwanakan W, Saiyudthong S, Srisurapanon S, Anurutwong A. The comparative study of depression between gifted children and normal children. J Med Assoc Thai. 2010;93(Suppl 2):S9–14. [PubMed] [Google Scholar]
- 47.Katusic MZ, Voigt RG, Colligan RC, Weaver AL, Homan KJ, Bar-baresi WJ. Attention-deficit hyperactivity disorder in children with high intelligence quotient: results from a population-based study. J Dev Behav Pediatr. 2011;32:103–109. doi: 10.1097/DBP.0b013e318206d700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Brown TE, Reichel PC, Quinlan DM. Executive function impairments in high IQ children and adolescents with ADHD. Open J Psychiatr. 2011;1:56–65. [Google Scholar]
- 49.Antshel KM, Faraone SV, Stallone K, Nave A, Kaufmann FA, Doyle A, Fried R, Seidman L, Biederman J. Is attention deficit hyperactivity disorder a valid diagnosis in the presence of high IQ? Results from the MGH Longitudinal Family Studies of ADHD. J Child Psychol Psychiatry. 2007;48:687–694. doi: 10.1111/j.1469-7610.2007.01735.x. [DOI] [PubMed] [Google Scholar]
- 50.Katusic MZ, Voigt RG, Colligan RC, Weaver AL, Homan KJ, Barbaresi WC. Attention-Deficit/Hyperactivity Disorder in Children With High IQ. Results from a Population-Based Study. J Dev Behav Pediatr. 2011;32:103–109. doi: 10.1097/DBP.0b013e318206d700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Antshel KM, Faraone SV, Maglione K, Doyle A, Fried R, Seidman L, Biederman J. Temporal stability of ADHD in the high-IQ population: results from the MGH Longitudinal Family Studies of ADHD. J Am Acad Child and Adolesc Psychiatry. 2008;47:817–825. doi: 10.1097/CHI.0b013e318172eecf. [DOI] [PubMed] [Google Scholar]
- 52.Webb JT. Mis-diagnosis and dual diagnosis of gifted children: Gifted and LD, ADHD, OCD, oppositional defiant disorder. In: Hafenstein N, Rainey F, editors. Perspectives in gifted education: Twice exceptional children. Denver: Ricks Center for Gifted Children, University of Denver; 2001. pp. 23–31. [Google Scholar]
- 53.ConBraSD (Brazilian Council for Giftedness) Available at: http://conbrasd.org/wp/?page_id=4188 .
- 54.Spilker B. Quality of Life and Pharmacoeconomics in Clinical Trials. 2nd ed. Philadelphia: Lippincott-Raven Publishers; 1996. [Google Scholar]
- 55.World Health Organization. Constitution of the World Health Organization basic document. Geneva, Switzerland: World Health Organization; 1948. [Google Scholar]
- 56.Winner E. The origins and ends of giftedness. Am Psychol. 2000;55:159–169. doi: 10.1037//0003-066x.55.1.159. [DOI] [PubMed] [Google Scholar]
- 57.Brody LE, Mills CJ. Gifted children with learning disabilities: a review of the issues. J Learn Disabil. 1997;30:159–169. doi: 10.1177/002221949703000304. [DOI] [PubMed] [Google Scholar]
- 58.Bell SM, Schindler WJ. Collaboration at a professional development school: Investigation of variables affecting student achievement and adjustment. Tennessee Education. 2002;31/(32):5–10. [Google Scholar]
- 59.Udvari SJ, Rubin KH. Gifted and Non-Selected Children's Perceptions of Academic Achievement, Academic Effort and Athleticism. Gift Child Q. 1996;40:211–219. [Google Scholar]
- 60.Austin AB, Draper DC. Peer relationships of the academically gifted: A review. Gift Child Q. 1981;25:129–133. [Google Scholar]
- 61.Helt CA. The role of IQ and gender in the social-emotional functioning of adolescents. Unpublished dissertation. University of Northern Colorado. 2008 [Google Scholar]
- 62.Çağlar D. Türkiye Üstün Yetenekli Çocuklar Kongresi SeçilmişMakaleler Kitabı. İstanbul:: Çocuk VakfıYayınları; 2004. Okulda Başarısız Olan Üstün ZekâlıÇocuklar. İçinde:1; pp. 409–415. [Google Scholar]
- 63.White PH, Sanbonmatsu DM, Croyle RT, Smittipatana S. Test of socially motivated underachievement:'Letting up'for others. J Exp Soc Psychol. 2002;38:162–169. [Google Scholar]
- 64.Lovett BJ, Lewandowski LJ. Gifted Students with learning disabilities: who are they? J Learn Disabil. 2006;39:515–527. doi: 10.1177/00222194060390060401. [DOI] [PubMed] [Google Scholar]
- 65.Matthews MS. Gifted students dropping out. Recent findings from a southeastern state. Roeper Review. 2006;28:216–223. [Google Scholar]
- 66.Roberts SM, Lovett SB. Examining the “F”in gifted: Academically gifted adolescents'physiological and affective responses to scholastic failure. Journal for the Education of the Gifted (JEG) 1994;17:241–259. [Google Scholar]
- 67.Oğurlu Ü. Üstün zekâlıve yeteneklilerde sosyal uyum ve arkadaşlık ilişkileri. Literatür taraması. Çukurova Üniversitesi Eğitim Fakültesi Dergisi. 2010;3:90–99. [Google Scholar]
- 68.Swanepoel RE. The psychosocial adjustment of gifted adolescents. Unpublished master thesis, University of Pretoria, South Africa. 1987 [Google Scholar]
- 69.Yalın Ş. Türkçe Güçler Güçlükler Anketi'nin Psikometrik Özellikleri. Uzmanlık tezi, Dokuz Eylül Üniversitesi Tıp Fakültesi, Çocuk ve Ergen Ruh Sağlığıve HastalıklarıAnabilim Dalı, İzmir. 2008 [Google Scholar]
- 70.Dauber SL, Benbow CP. Aspects of personality and peer relations of extremely talented adolescents. Gift Child Q. 1990;34:10–14. [Google Scholar]