

Abstract
Background:
Residency is one of the most critical periods of medical education. Residents are susceptible in high risk for mental problems which can affect the doctor–patient relationship. Emotional intelligence (EI) correlates closely with stress and mental health. Considering the important role of EI in medical education and with regard to lack of studies in this group in Iran, this study conducted to determine the relationship between EI and stress, anxiety, and depression in a sample of resident physician in our university of medical sciences.
Materials and Methods:
In this cross-sectional study, 245 residents were invited, but only100 questionnaires were analyzed, and the response rate was 41%. From this, 26 were men and 74 were women. Bar-on EI questionnaire, Depression Anxiety Stress Scales-21, for evaluating the stress, anxiety, and depression and demographic characteristics were used.
Results:
The mean score of EI in resident physician was 330.24 ± 38.5. The mean score of stress, anxiety, and depression was 17.8 ± 8.6, 10.04 ± 7.99, and 10.49 ± 8.67 respectively. There was a negative relation between mean score of anxiety (R = −0.0525), stress (R = −0.639), and depression (R = −0.644) with a mean score of EI.
Conclusion:
Higher EI appears to be good predictors of lower stress, anxiety, and depression in resident physician.
Keywords: Anxiety, depression, emotional intelligence, stress
Introduction
Medical education is a stressful period for all groups of these students. Many studies showed a high prevalence of stress, anxiety, depress,[1,2,3] suicide,[2] lower quality of life, and eventually reduction in personal and professional performance.[1,3] Residency is one of the most critical periods of medical education.[4,5,6] Need for persistent study, excessive responsibility, lack of time for resting, and pleasure activity are some of the reasons for burnout of them.[4,5,6] Many studies showed a high level of depression and emotional problem in resident physician.[5] The results of systematic review in 2015 showed 20%–40% depression and depressive symptom in a resident physician.[4] Hence, high levels of mental health of residents as well as optimal patient care are the important purpose of strategic planning for medical training systems in the world.[7,8]
Professional competence of doctors in modern medical curricula containing patient care, professionalism, System-based practices, interpersonal communication skills, medical knowledge, and emotional responsiveness.[8]
Managing emotions is fundamental for medical practice. Physician must navigate their own emotions as well as the emotions of patients and other team members.[9] One of the most predictors of therapeutic outcomes of patients is effective communication and interpersonal sensitivity during therapeutic interactions.[10]
The concept of emotional intelligence (EI) has grown rapidly in recent years and has a strong relationship with stress, mental health, and job performance.[9]
EI is an important parameter that affect all aspects of persons’ life and conceptualizes the perception, processing, regulation, and management of emotions in self and others.[8,9] EI is capable to improve by education, and the result can affect persons’ mental health and general performance.[7]
Training components of EI to improve general competencies of medical students increasingly discussed in modern medical education in the world.
Considering the important role of EI in medical education and with regard to lack of such studies in Iran and specially in resident physician, the present study has been conducted to determine the relationship between EI and anxiety, stress, and depression in sample of resident physicians of Guilan University of medical sciences in north of Iran.
Materials and Methods
This was a cross-sectional study. The study was approved by the Ethical Committee at Research center of our University of Medical Sciences in according to the Declaration of Helsinki.
Participants
All resident physicians in our university of medical sciences between 2014 and 2015 were eligible to participate in this study.
Exclusion criteria were acute mental or physical problem in recent 6 months, according to self-report of residents, in initial section.
Measurement tool
Demographic questionnaire consisted of age, sex, marital status, field and year of residency, and number of night staying in the hospital
-
Bar-on EI questionnaire: It contains ninety questions in five dimensions and 15 subsets. the five dimensions include intrapersonal relationships, interpersonal relationship, stress management, adaptability, and general mood
Every question in the questionnaire has five answer choices ranging from “I absolutely agree” to “I absolutely disagree” (the lacerate 5-grade spectrum). Reliability of the Persian version of EI questionnaire (Bar-on) was assumed 0.94 based on Cranach's alpha. The minimum and maximum scores for this questionnaire were 90 and 450
Depression Anxiety Stress Scales (DASS-21) was developed to measure depression, anxiety, and stress level.
The reliability coefficient of depression, anxiety, and stress subscales ranges from 0.81 to 0.97, and the three subscales demonstrated satisfactory discrimination ability to differentiate between physical and nonphysical problems.
The DASS manual consists of 21 questions:
Stress subscale score as normal (0–14), mild (15–18), moderate (19–25), sever (26–33), and extremely sever (34 and above)
Anxiety subscale scores as normal (0–7), mild (8–9), moderate (10–14), sever (15–19), and extremity sever (20 and above)
Depression subscale scores as normal (0–9), mild (10–13), moderate (14–20), sever (21–27), and extremely severe (28 and above). The DASS-21 was chosen for this study because it can be administered rapidly and is a good, valid, and reliable instrument. Reliability and validity of this instrument in Iran was assumed.[11]
Study design
Residents were invited by face-to-face invitation section by one of the authors who was resident of psychiatry. After explanation of the purpose of the study and the initial agreement of them, the written informed consent and the questionnaires gave them. Participation was also informed about confidentiality of data.
The questionnaire was anonymous to encourage participation and allowed up to 8 weeks to complete them. Residents who did not complete the questionnaire was reminded by second face-to-face sections, up to again 8 weeks. Data collection was closed after 16 weeks.
Statistical analysis
The collected data were analyzed using manufactured by IBM Company in Chicago, USA, 2009 software, and the final results were interpreted. Normality of variables was analyzed using the Kolmogorov–Smirnov test. Categorical variables were expressed in terms of frequency and continuous variables expressed by mean and standard deviation. To find the existence of any difference between categorical variables, one-way variance was applied. For estimation of the effect of EI in stress, anxiety, and depression of participants, we used regression model. P < 0.05 was considered as the significance level.
Results
Of the 245 residents who were invited to participate in the study, 200 residents accept to participation, but 150 residents completed the questionnaires. From these questionnaires, only 100 questionnaires were reliable and 50 questionnaires were not analyzable.
Hence, the response rate was 41%. Demographic characteristics of the residents and total score of EI of them were shown in Table 1.
Table 1.
Stress, anxiety and depression of residents
Emotional intelligence
Mean score of EI in resident physician was 330.44 ± 38.5.
Total score of EI was statistically significant for age group and married status of residents in witch age above 30 years (0.034) and married (0.023) residents had a higher score in EI. Women had higher EI than men, but the difference was not significant (P = 0.686) [Table 1].
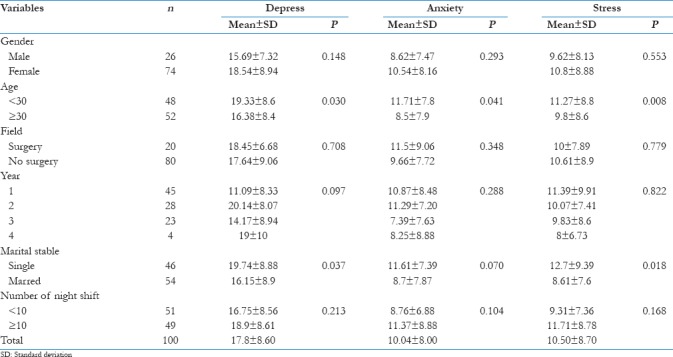
Stress, anxiety, and depression
Mean scores of stress, anxiety, and depression in resident were 17.8 ± 8.61, 10.04 ± 7.99, and 10.49 ± 8.67, respectively.
According to Table 2, stress, anxiety, and depression were significantly higher in resident physician younger than 30 years; there was also significant relation between higher scores of stress and depression in single residents. Stress, anxiety, and depression were not significantly different in male and female, surgery or nonsurgery field of work, year of residency, and residents who had a higher number of night staying in hospital.
Table 2.
Emotional intelligence of residents
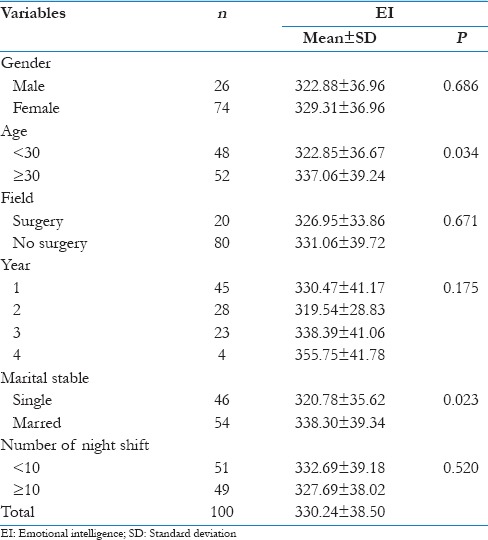
Table 3 shows a correlation between EI and stress, anxiety, and depression.
Table 3.
Correlation between emotional intelligence and stress, anxiety, and depression of residents

Regression analysis was conducted to predict stress, anxiety, and depression by the score of EI. Based on these results, higher EI appears to be good predictors of lower stress, anxiety, and depression in a resident physician.
Discussion
EI has increasingly demonstrated in all aspects of life in the recent years.[12,13] Due to its fundamental role in academic performance communication skills, therapeutic relationship, and eventually professional success, many researches have been done to incorporating that into modern medical curricula education all over the world, this study is the first to describe and investigate the EI of resident physician in Iranian postgraduate medical students.
The most important finding of this study was a negative association between EI and stress, anxiety, and depression in resident physicians.
High scores in EI associated with low scores in stress, anxiety, and depression in all age groups, gender, marital status, and field of work.
With regard to descriptive method of the present study, the results may not support the correlation of the relationships; however, given the more stable trait of EI than stress, anxiety, or mood of oneself, it might make sense to hypothesis that EI is affecting the level of stress, anxiety, and depressive mood.
In this study, the scores of anxiety (significantly) stress, and depression (not significantly) was higher in residents younger than 30 years.
Consistent with other studies, older residents were move likely to use move adoptive coping mechanisms, or they are better use problem-solving, cognitive, and emotional strategies to cope with stressful life events.[14]
The explanation may be more engagement with previous experiences that help to improve soul competencies.
Some studies reported higher EI in female; we did not find this relationship, consistent with other researchers.[9,12,13,14]
Mckinley et al. in 2014 found no difference in global EI between men and women in the specialists.[9]
They explained that individual who chose medical professions are from particular subset of general population, regardless of gender or the selection processes for medical school or kind of training may be the cause of same EI in men and women physician.[9]
There was a significant difference among marital status of resident for a mean score of stress, anxiety, and depression (SAD) and EI consistent with some other studies;[15] married residents had a lower level of SAD and high level of EI. Marriage may be a protective factor for reduced stress, anxiety, and depression or individual with better mental health earlier go to be married.
Surprisingly, residents with a surgical procedure, did not have more SAD, maybe working under supervision of their seniors is the reason of this results. Some studies discussed EI as moderator or buffer of stress.[16,17]
The best description for the relationship between EI and stress, anxiety, and depression hypothesized by the nature of EI and its components.
Individuals with high EI have better self-awareness, paying attention to emotions, recognize and understand oneself and others’ emotions, and using them to manage their relationships and provide social support. In addition, the ability of emotion regulation improves adaption coping mechanisms such as problem-solving and stress management. Good social skills help them to better resilience for everyday life reduce distress and anxiety and better satisfaction from life.[7,18,13]
Many studies confirmed the fundamental role of EI in effective communism, academic and clinical performance, job satisfaction, and client satisfaction in medical carrier,[7,8,9] but it is still a nascent field of research in medical education, especially in our country.
According to well-controlled studies, educating of life skills can improve the EI (7.18).
This fact that high EI related to better mental health and EI can improve by education showed in many studies, considering that life skills’ training could led to increase EI, and with regard to the result of the present study, it is suggested that life skills’ training as an important issue incorporates to medical curricula of resident physicians.
Limitations
The most important limitation in this study was low response rate (50%). We did not use any reward for participants and the term of intelligence may suggest some sort of to be judge. Self-rated method used for gathering data could led to information bias. Furthermore, distribution of residents in different level was not balanced; finally, the cross-sectional method used in the present study, limited result for interpretation of observed associations between measured factors. We did not differentiate dimensions of EI.
Conclusion
According to a negative relation between stress, anxiety, and depression with EI resident physician, improving EI would be a protective factor for better mental health of them.
Further study on different dimensions of EI and interventional program to improve EI is recommended.
Financial support and sponsorship
This research was conducted as a residency thesis and has been supported by our University of Medical Sciences and Grant No: 90320104.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Pereira MA, Barbosa MA. Teaching strategies for coping with stress – The perceptions of medical students. BMC Med Educ. 2013;13:50. doi: 10.1186/1472-6920-13-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Supe AN. A study of stress in medical students at seth G.S. Medical college. J Postgrad Med. 1998;44:1–6. [PubMed] [Google Scholar]
- 3.Yusoff MS. Associations of pass-fail outcomes with psychological health of first-year medical students in a Malaysian medical school. Sultan Qaboos Univ Med J. 2013;13:107–14. doi: 10.12816/0003203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mata DA, Ramos MA, Bansal N, Khan R, Guille C, Di Angelantonio E, et al. Prevalence of depression and depressive symptoms among resident physicians: A Systematic review and meta-analysis. JAMA. 2015;314:2373–83. doi: 10.1001/jama.2015.15845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.AEduc2 Ishak WW, Lederer S, Mandili C, Nikravesh R, Seligman L, Vasa M, et al. Burnout during residency training: A literature review. J Grad Med Educ. 2009;1:236–42. doi: 10.4300/JGME-D-09-00054.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Joules N, Williams D, Thompson A. Depression in resident physicians: A systematic review. Open J Depression. 2014;3:89–100. [Google Scholar]
- 7.Lolaty HA, Ghahari S, Tirgari A, Fard JH. The effect of life skills training on emotional intelligence of the medical sciences students in Iran. Indian J Psychol Med. 2012;34:350–4. doi: 10.4103/0253-7176.108217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Arora S, Ashrafian H, Davis R, Athanasiou T, Darzi A, Sevdalis N, et al. Emotional intelligence in medicine: A systematic review through the context of the ACGME competencies. Med Educ. 2010;44:749–64. doi: 10.1111/j.1365-2923.2010.03709.x. [DOI] [PubMed] [Google Scholar]
- 9.McKinley SK, Petrusa ER, Fiedeldey-Van Dijk C, Mullen JT, Smink DS, Scott-Vernaglia SE, et al. Are there gender differences in the emotional intelligence of resident physicians? J Surg Educ. 2014;71:e33–40. doi: 10.1016/j.jsurg.2014.05.003. [DOI] [PubMed] [Google Scholar]
- 10.Libbrecht N, Lievens F, Carette B, Côté S. Emotional intelligence predicts success in medical school. Emotion. 2014;14:64–73. doi: 10.1037/a0034392. [DOI] [PubMed] [Google Scholar]
- 11.Asghari A, Saed F, Dibajnia P. Psychometric properties of Depression anxiety stress scales-21 (DASS-21) in a non-clinical Iranian sample. IPA Int J Psychol. 2008;2:82–102. [Google Scholar]
- 12.Abdollahpour I, Nedjat S, Besharat MA, Hosseini B, Salimi Y. Emotional intelligence: A Comparison between medical and non-medical students. Iran J Public Health. 2016;45:214–22. [PMC free article] [PubMed] [Google Scholar]
- 13.Namdar H, Sahebihagh M, Ebrahimi H, Rahmani A. Assessing emotional intelligence and its relationship with demographic factors of nursing students. Iran J Nurs Midwifery Res. 2008;13:145–9. [Google Scholar]
- 14.Monteiro NM, Balogun SK, Oratile KN. Managing stress: The influence of gender, age and emotion regulation on coping among university students in Botswana. Int J Adolesc Youth. 2014;19:153–73. doi: 10.1080/02673843.2014.908784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Madahi ME, Javidi N, Samadzadeh M. The relationship between emotional intelligence and marital status in sample of college students. Procedia Soc Behav Sci. 2013;84:1317–20. [Google Scholar]
- 16.Pau AK, Croucher R. Emotional intelligence and perceived stress in dental undergraduates. J Dent Educ. 2003;67:1023–8. [PubMed] [Google Scholar]
- 17.Nooryan K, Gasparyan K, Sharif F, Zoladl M. Controlling anxiety in physicians and nurses working in intensive care units using emotional intelligence items as an anxiety management tool in Iran. Int J Gen Med. 2012;5:5–10. doi: 10.2147/IJGM.S25850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Radfar S, Aghaie M, Motashker A, Noohi S, Saburi A. Evaluation of emotional intelligence and its relation to the academic archievement in the students. Thrita J Med Sci. 2013;2:113–9. [Google Scholar]