

Abstract
Objective:
To assess the association between change in walking speed over a 12-month period and risk of developing radiographic knee osteoarthritis (rKOA) over a 24-month period.
Methods:
We included participants without rKOA from the Osteoarthritis Initiative. Change in walking speed was determined from a 20-meter walk assessment, calculated using walking speed at 12-month follow-up minus baseline speed and/or 24-month follow-up walking speed minus 12-month speed. Incident rKOA was defined as progressing to Kellgren-Lawrence grade ≥2 within 24 months (i.e., incidence between 12 and 36 or 24 and 48 months). Self-reported significant knee injury during the exposure period, age, body mass index (BMI), and Physical Activity Scale for the Elderly (PASE) score were adjusted for analytically.
Results:
We included 2,638 observations among 1,460 unique participants (58% female; 59±9 years, range: 45–79). The mean change in walking speed over 12 months was 0.001±0.13 m/s (range: −0.6271, 1.4968). Approximately 5% of the sample (n=122) developed rKOA over a 24-month period. After controlling for significant knee injury, age, BMI, and PASE score, we found an 8% relative increase in risk of developing rKOA for every 0.1m/s decrease in walking speed over a 12-month period (Risk Ratio=1.08; 95% CI =1.00, 1.15; P = 0.05).
Conclusion:
Evaluating change in speed over a 12-month period using a 20-meter walk test may be useful in identifying individuals at increased risk of developing rKOA over the subsequent 24-months. Identification of patients at high risk for developing rKOA would allow medical providers to implement early interventions to maximize joint health.
Keywords: Osteoarthritis, Gait, Knee
INTRODUCTION
Knee osteoarthritis is the 11th leading cause of global disability.1 There are no disease modifying interventions for knee osteoarthritis. One explanation for our failure to identify a disease modifying intervention is that we primarily test patients late in the disease process when it may be too late. Therefore, early identification of risk factors associated with the incidence and progression of knee osteoarthritis has become paramount in preventing disease onset or progression as well as associated physical disability.2,3 Clinical strategies are needed that can be easily implemented to predict the incidence of knee radiographic osteoarthritis (rKOA). Reliable and efficient clinical measures would be beneficial that identify individuals at increased risk of developing knee rKOA.
Walking speed is a readily-observable and stable objective measure of physical function. Habitual walking speed is typically a stable measure that only varies 1% per decade on average until individuals reach approximately 62 years of age.4 Individuals with symptomatic knee osteoarthritis demonstrate a rapid decrease in walking speed of as much as 2.75% per year.5 Decreased walking speed is associated with decreased confidence in knee function6 in those with knee osteoarthritis and predicts the likelihood that an individual with knee osteoarthritis will elect to undergo a knee replacement.7 In addition, slower walking speed associates with higher concentrations of serum-based markers of type-II collagen breakdown in individuals following anterior cruciate ligament reconstruction,8 who are at higher risk of developing knee rKOA.9–11
Previous authors have demonstrated that slower habitual walkers without knee rKOA demonstrated higher odds of developing rKOA at 6-year follow-up.12 However, change in walking speed may provide a more sensitive measure of future osteoarthritis risk than an assessment of gait pace at a single time point. To date no prospective studies have examined longitudinal changes in walking speed and risk of rKOA. The ability to predict an individual’s risk of developing knee rKOA by measuring a change in walking speed may provide clinicians with a cost effective measurement tool that could be employed at subsequent clinic visits. While walking speed is known to decrease in those with symptomatic knee osteoarthritis,5 it remains unknown if a decrease in walking speed among those without rKOA over one year is identifiable prior to knee rKOA development or progression.
The overall goal of our analysis was to determine whether changes in a simple 20-meter walk test, evaluated during annual clinical exams, could be used as a marker of those who will develop knee rKOA within the following two years. To accomplish this goal, we assess the association between a change in walking speed over a 12-month period among individual without osteoarthritis and the risk of developing knee rKOA over a subsequent 24-month period using data from the Osteoarthritis Initiative (OAI). We hypothesized that a decrease in walking speed over a 12-month period would be associated with an increase in knee rKOA risk over the subsequent 24 months.
PATIENTS AND METHODS
Study Design
Data used in the preparation of this article were obtained from the Osteoarthritis Initiative (OAI) database, which is available for public access at www.oai.ucsf.edu.13. Briefly, the OAI is a multi-center, longitudinal, prospective observational study of knee osteoarthritis in the United States13. Clinical staff recruited 4,796 men and women between the ages of 45 to 79 years who primarily had symptomatic knee osteoarthritis or were at increased risk for developing symptomatic knee osteoarthritis between February 2004 and May 200613. For our analyses, we used data from the OAI baseline and first four annual follow-up visits (12-month through 48-month follow-up). This study was approved by the University of North Carolina at Chapel Hill Institutional Review Board under IRB 16–1678.
Inclusion Criteria
We included OAI participants without tibiofemoral rKOA in both knees (Kellgren-Lawrence [KL] grade ≤1) and who had at least two walking speed assessments, separated by 12 months, prior to the 24-month OAI visit (Figure 1). Eligible participants also needed to have knee radiographs scored during the exposure period and at the OAI visit that occurred 24 months after the last assessment of walking speed. Participants were excluded if they demonstrated rKOA in either knee at any time during exposure assessment or if they had any knee arthroplasty in either knee, had any hip arthroplasty in either hip, had any type of prosthesis surrounding the knee, or reported using an ambulatory aid other than a single straight cane for more 50% of their time during ambulation. We excluded participants with a self-reported history or clinical suspicion of rheumatoid arthritis during our study period.
Figure 1:
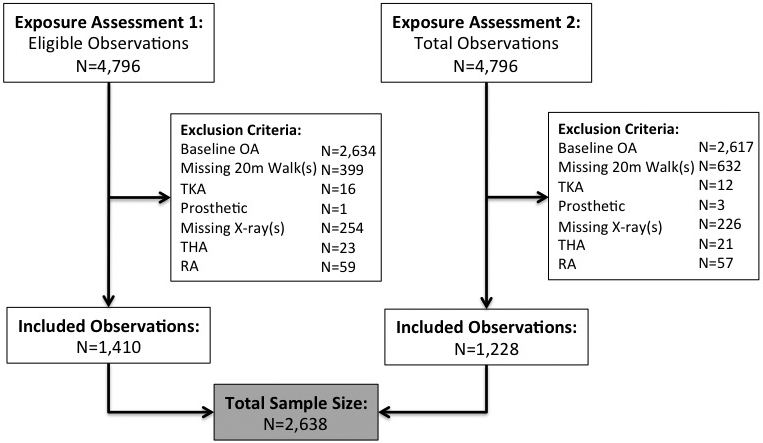
Flow diagram of study enrollment for OAI participants included in the analysis of the association between 12-month change in walking speed and 24-month risk for incident rKOA
Walking Speed
The 12-month change in walking speed was determined from the pace of a 20-meter walk assessment, using the “AllClinical” files. The 20-meter walking speed assessment has been recommended to assess physical function in individuals with r KOA.14 Participants were instructed to walk at their usual walking speed from the start to finish points of marked 20-meter distance.15 As previously reported,15,16 2 trials were collected and the mean of these trials was used for data analysis. We included two periods of exposure assessment to determine change in walking speed, resulting in two potential observations for each participant. Exposure assessment 1 was calculated from the Baseline AllClinical file (version 0.2.2) and 12-month AllClinical file (version 1.2.1). Exposure assessment 2 was calculated from the 12-month AllClinical file (version 1.2.1) and the 24-month AllClinical file (version 3.2.1). In order to maximize the number of unique assessments of walking speed change, walking speed was calculated as a continuous variable from either a) the baseline visit to the 12-month follow-up (Exposure Assessment 1: [12-month speed – baseline speed]) or b) from the 12-month follow-up to the 24-month follow-up (Exposure Assessment 2: [24-month – 12-month speed])(Figure 2). Walking speed was measured in meters per second (m/s).
Figure 2:
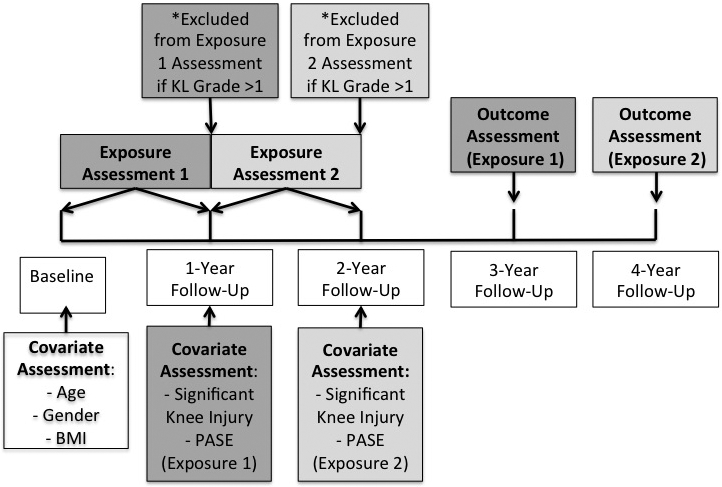
Exposure, outcome, and covariate assessment diagram for participants included in the analysis of the association between 12-month change in walking speed and 24-month risk for incident rKOA
Knee Radiographs
We assessed the incidence of rKOA over 24 months at the 36-month or 48-month OAI visits for exposure assessments 1 and 2, respectively (Figure 2). Incident tibiofemoral rKOA was determined as having a KL grade ≥ 2 in either knee 24-months following no presence of rKOA (KL ≤ 1) at any time during exposure assessment. If either or both knees developed rKOA over the 24-months following exposure assessment, that participant’s observation was considered to have incident rKOA. Central readers scored KL grades on bilateral weight-bearing, fixed-flexion posterior-anterior knee radiographs. Readers were blinded to the sequence of follow-up images. A study of image assessment in OAI found good reliability for KL grading between baseline and 36-month follow-up visit with kappa values of approximately 0.70 to 0.80.17 In addition, agreement of readings was similar for the 48-month follow-up visit radiographs.
Potential Confounders
In order to assess the association between change in walking speed and incident rKOA, we included in our initial analysis demographic information on age at baseline, gender, and body mass index (BMI) at baseline. Additionally, physical activity level was measured at the 12-month time point of the exposure assessment using the Physical Activity Scale for the Elderly (PASE)(Figure 2).18 Finally, we included information about knee pain, ankle pain, back pain, hip pain, knee injury, and history of a fall as potential confounders. Knee, ankle, and hip pain were dichotomous variables for self-reported pain, aching or stiffness for more than half the days in the past 30 days from the second walking speed assessment. Self-reported back pain in the past 30 days was also recorded during the 12-month time point of the exposure assessment. Knee injury was a dichotomous variable defined as “a serious enough knee injury to limit the ability to walk for at least two days” during the 12-month exposure assessment period. We also included self-reported history of a fall, which was defined as any fall to the floor or ground. All covariates were calculated from the Baseline AllClinical file (version 0.2.2), 12-month AllClinical file (version 1.2.1), and 24-month AllClinical file (version 3.2.1). Based on the minimally sufficient adjustment set identified from a directed acyclic graph, the following confounders were included in our analysis: knee injury, age, BMI, and PASE score.
Statistical Analysis
Descriptive statistics were calculated for all variables of interest, including counts and proportions for dichotomous variables and means and standard deviations, as well as medians and interquartile ranges (IQR), for continuous variables. Comparisons of continuous walking speed between those who developed rKOA and those who did not were performed using a two-sample t-test due to large sample size and normally distributed data. We determined a priori to assess the linear nature of the relationship prior to formal statistical analyses using functional form analysis techniques.
Results of the functional form analysis indicated a relatively linear relationship between change in walking speed and incident rKOA. Therefore, multivariable log-binomial regression was used to assess the association between continuous walking speed and incident rKOA. An adjusted risk ratio was also calculated to estimate the effect of a −0.1m/s decrease in walking speed on rKOA incidence (0.10 m/s change in walking speed has previously been reported as a the minimal clinically important difference for change in walking speed over time) while controlling for the potential confounders (knee injury, age, BMI, and PASE score) for our primary analysis.19 An interaction term was added to assess potential effect measure modification of the association between walking speed and rKOA incidence by reported knee injury. To account for the correlation within participants who were included in both exposure assessments, a generalized estimating equation analysis with robust standard errors was used. We used Statistical Analysis Software (SAS v 9.4) for all analyses with an a priori significance set at p≤0.05.
RESULTS
There were 2,638 12-month walking speed change observations among 1,460 unique participants included in this analysis. Descriptive characteristics of the included participants are listed in Table 1. Overall, average walking speed increased 0.001± 0.133 m/s (range: −0.627, 1.497 m/s) during the 12-month exposure period for observations included in our sample. The median change in walking speed was 0.001 m/s (IQR −0.075, 0.075). Walking speed decreased in 1,309 (50%) observations, and increased in 1,329 (50%) observations over the exposure period.
Table 1:
Descriptive characteristics for participants include in the analysis of the association between 12-month change in walking speed and 24-month risk for incident rOA (N=1,460 participants, 2,638 observations)
| Variable | N | Mean (SD) or n (%) | Range |
|---|---|---|---|
| Age (years) | 1460 | 59 (9) | 45, 79 |
| BMI (kg/m2) | 1460 | 27.1 (4.5) | 17.6, 45.4 |
| Gender | 1460 | ||
| Male | 618 (42%) | ||
| Female | 842 (58%) | ||
| PASEa Score | 2624 | 166 (82) | 7, 464 |
| Knee Pain | 2606 | 685 (26%) | |
| Ankle Pain | 2624 | 236 (9%) | |
| Back Pain | 2632 | 442 (17%) | |
| Hip Pain | 2626 | 624 (24%) | |
| Knee Injury | 2635 | 75 (3%) | |
| History of Fall | 1211 | 380 (31%) |
Physical Activity Scale for the Elderly (PASE) validated patient-reported outcome score for function
Approximately 5% of the sample (122 participants) developed rKOA over the 24-month period following walking speed. The average 12-month change in walking speed among those who developed rKOA was −0.012±0.119m/s compared to 0.002±0.133m/s among those who did not develop rKOA (p=0.26). The risk of developing rKOA over 24 months was 1.08 times higher (95% CI=0.94, 1.23; p=0.26) for every 0.1 m/s decrease in walking speed over a 12-month period. After controlling for significant knee injury, age, BMI, and PASE score, we found an 8% relative increase in risk of developing rKOA for every 0.1m/s decrease in walking speed over a 12-month period (RR=1.08; 95% CI=1.00 to 1.15; p=0.05)(Table 2). Among observations where no knee injury was reported (n=2,560), there was an 8% relative increase in risk of developing rKOA for every 0.1 m/s decrease in walking speed over a 12-month period (RR=1.08; 95% CI=1.00 to 1.17; p=0.05); however, among observations where an injury was reported (n=75), there was relatively no association between a change in walking speed and risk of developing rKOA over a 24-month period (RR=1.01; 95% CI=0.83 to 1.23; p=0.91).
Table 2:
Multivariable log-binomial regression results and comparison of covariates for participants who developed incident rOA over the 24-month study period compared to those who did not (N=1,460 participants, 2,638 observations)
| Variable | Incident rOA | No rOA | RR | 95%CI | ||
|---|---|---|---|---|---|---|
| N | Mean (SD) or n (%) | N | Mean (SD) or n (%) | |||
| Walking Speed | 122 | −0.0121 (0.1188) | 2516 | 0.0016 (0.1335) | 1.08 | 1.00, 1.15 |
| Age (years) | 122 | 59.3 (8.4) | 2516 | 59.0 (9.0) | 1.00 | 0.98, 1.03 |
| BMI (kg/m2) | 122 | 28.3 (4.9) | 2516 | 27.0 (4.4) | 2.03 | 1.33, 3.10 |
| PASEa Score | 122 | 162.7 (87.5) | 2501 | 166.5 (82.0) | 1.00 | 1.00, 1.00 |
| Knee Injury | 122 | 8 (6.5) | 2513 | 67 (2.7) | 1.38 | 0.76, 2.49 |
Physical Activity Scale for the Elderly (PASE) validated patient-reported outcome score for function
DISCUSSION
The results of our study support the hypothesis that individuals who decrease their walking speed over a 12-month period in the absence of knee rKOA are at increased risk for developing incident knee rKOA over the following 24-month period. Specifically, we found that for every 0.1m/s decrease in walking speed over a 12-month period with no evidence of rKOA the relative risk of developing rKOA over the subsequent 24-month period increased by 8%, when controlling for significant knee injury, age, BMI, and PASE score. We found the same relative increase in risk among participants who did not report a knee injury (RR=1.08; 95% CI=1.00 to 1.17; p=0.05); however, among participants who did report a knee injury, there was no association between walking speed change and risk of incident rKOA (RR=1.01; 95% CI=0.83 to 1.23; p=0.91).
These findings are in line with previous studies that suggested an association between habitual walking speed and incident rKOA.12,20 Purser el al.12 analyzed a community-based cohort for the effect of average habitual walking speed on the odds of developing rKOA over a 6-year period, and found a 12% decrease in odds of developing rKOA for participants with a 0.1m/s increase in habitual walking speed. Our study corroborated and added to these findings by studying a change in walking speed over time in the absence of knee rKOA, as opposed to assessing walking speed at one time point. Therefore a simple, repeated 20-meter walk test, which could be easily evaluated during annual clinical exams, could be used to indicate increased risk of developing knee rKOA within the following two years, particularly among adults without a reported knee injury. This simple indicator may help identify at-risk patients, allowing for an opportunity to intervene in order to prevent disease onset and associated disability.
Previous work has assessed the ability of walking speed to predict rKOA onset by characterizing slow walkers as those with a habitual walking speed of less than 1.00 m/s. Others have predicted a clinically meaningful improvement in function over 30 months by dichotomizing individuals into those who were and were not able to improve walking speed by 1.0m/s. In our cohort, the range of change in walking speed over 12 months was −0.627m/s to 1.497m/s, with an average change in walking speed of essentially 0m/s. The IQR for change in walking speed in our sample was −0.075m/s to 0.075m/s, suggesting that less than 25% of our sample had a change in walking speed greater than 0.1m/s in a 12-month period. Therefore, the 1.0 m/s change used previously is likely not clinically relevant since a very small proportion of people have that drastic of a change in walking speed over the course of one year. In contrast, a change of 0.10 to 0.20 m/s in habitual walking speed has been identified as a minimally clinically important difference for change in walking speed.19 Our data suggested that a decrease of 0.1 m/s over a 12-month period was associated with an 8% relative increase in risk of developing rKOA over the subsequent 24 months. A change of −1.59 seconds has been reported to be the smallest detectable difference for the 20-meter walking speed assessment,21 which would be a 0.07 m/s decrease in walking speed in individuals who initially walked at 1.00m/s. 21 Therefore, the 20-meter walking speed assessment appears to demonstrate the appropriate precision to detect a change of 0.1m/s in this patient population. The current study also improves upon previous research as evaluation of a 0.1m/s change in walking speed over a 12-month period assesses risk of developing rKOA in a shorter period of time (over 24 months) compared to a previous study that predicted rKOA onset over a 6-year follow-up.12 The ability to provide information to patients and providers about increased risk over a shorter period may motivate more immediate further evaluation or lifestyle changes necessary to mitigate the risk of rKOA.
While the mechanisms that link slower walking speeds and knee rKOA onset remain unknown, it can be hypothesized that slower walking speeds may be a biomechanical adaption to the impact of early metabolic changes at the knee.8,12 Slower walking speeds are associated with a lesser loading rate and magnitude of loading during the initial peak in the ground reaction force during the stance phase of gait.22–25 Greater impulsive loading has been found to damage articular cartilage and weaken the extracellular cartilage matrix.26 Alternatively, it is possible that decreased loading secondary to pain or inactivity may lead to deterioration and hasten the osteoarthritis disease process. Decreasing habitual walking speed may be a subconscious protective strategy aimed at minimizing the magnitude and rate of loading on knee cartilage to maximize the longevity of tissue health. Additionally, slower gait speeds may increase the duration in which the knee cartilage is loaded during the stance phase of gait.27 While slower speeds decrease the magnitude and loading rate of the first half of stance phase, these slower walking speeds increase the magnitude in which the extremity is loaded during the second half of the stance phase of gait.23–25 Thereby, slower walking speeds and increased magnitude and duration of loading in the second half of the stance phase of gait may also cause increased cartilage breakdown. Further research is needed to determine if slower walking speeds are protective of deleterious changes in joint tissue metabolism prior to rKOA onset or a contributor to these harmful changes that influence rKOA onset. Regardless of whether the change in walking speed that was appreciated in our study is an early indicator of prevalent osteoarthritis or a causal component of its development, we believe our findings are meaningful because these data may be used to develop an early clinical indicator of patients who are at risk for developing knee rKOA before structural joint changes are detected radiographically.
While our study supports the use of walking speed as a clinical indicator of incident knee rKOA, limitations must be considered when interpreting the results of this study. We only included participants who completed the longitudinal evaluations, who may be inherently different from other participants who did not participate in at least three consecutive study visits. Additionally, the results of the current study are most generalizable to a subset of the population who meet the OAI inclusion criteria, including increased risk for developing osteoarthritis; however, OAI provides a rich dataset that allows for control of potential confounders in a large study sample. In addition, this study focused on the development of tibiofemoral rKOA, and the results cannot be generalized to patients with patellofemoral rKOA. The exposure in this study was change in walking speed over a 12-month period, which was measured objectively during clinical 20-meter walk analysis at two time points and may not adequately represent the true change in walking speed over a 12-month period. Nevertheless, this is a realistic representation of screening of this simple indicator in a clinician’s office during annual visits. Overall, very little missing data (<1% for most variables) was noted in this analysis with no missing data for either exposure or outcome, but there is potential for measurement error for several of the covariates assessed using self-reported methods (i.e. history of fall, history of knee injury, knee, back, hip, or ankle pain in the last 30 days). The outcome of incident rKOA was determined based on radiographic assessment, and, as is common in such studies, it was not possible to determine the exact time of rKOA development during the 24-month follow-up period. Additionally, inclusion into the study cohort relied on KL grade <2 during the exposure period. While good reliability for KL grading between baseline and 36-month follow-up visit (kapp=0.70–0.80) was identified in a previous study17, the reliability was lower among KL grade <2. Therefore, it is possible that some individuals included in our analysis had existing osteoarthritis. It is possible that important potential confounders exist for the relationship between walking speed and incident rKOA that were not measured in OAI. Multiple previous studies15,16,28 have been published using the 20-meter walk times from the OAI, yet we are not aware of any published reliability data on this physical function outcome at the different OAI sites. While measuring 20-meter self-selected walking pace is a commonly collected clinical outcome of physical performance, a previous study has described a learning effect where individuals with rKOA walk faster in the first of three 20-meter walking trials compared to the subsequent two. Additionally, the OAI protocol29 does not indicate if standardized acceleration and deceleration space was provided to the participants, as well as verbal encouragement during the test.
In conclusion, our study found that for every 0.1m/s decrease in walking speed over a 12-month period, the relative risk of developing rKOA over the subsequent 24-months increased by 8%, when controlling for significant knee injury, age, BMI, and PASE score. For example, a patient who decreases walking speed by 0.4m/s over a one-year period has 32% greater risk of developing rKOA within the next two years compared to a patient with no change in walking speed. Evaluating a change in walking speed during serial clinical follow-ups using a 20-meter walk test may be useful in identifying which patients are at risk for developing knee rKOA over the subsequent 24-months. Early identification of these patients that are at the highest risk for developing knee OA would allow for medical providers to implement early interventions to maximize joint health.
Acknowledgments
Source of Support:
The OAI is a public-private partnership comprised of five contracts (N01-AR-2–2258; N01-AR-2–2259; N01-AR-2–2260; N01-AR-2–2261; N01-AR-2–2262) funded by the National Institutes of Health, a branch of the Department of Health and Human Services, and conducted by the OAI Study Investigators. Private funding partners include Merck Research Laboratories; Novartis Pharmaceuticals Corporation, GlaxoSmithKline; and Pfizer, Inc. Private sector funding for the OAI is managed by the Foundation for the National Institutes of Health. This manuscript was prepared using an OAI public use data set and does not necessarily reflect the opinions or views of the OAI investigators, the NIH, or the private funding partners.
University of North Carolina Injury Prevention Research Center is partially supported by an award R49/CE002479 from the National Center for Injury Prevention and Control, Centers for Disease Control and Prevention.
REFERENCES
- 1.Cross M, Smith E, Hoy D, Nolte S, Ackerman I, Fransen M, et al. The global burden of hip and knee osteoarthritis: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73:1323–1330. [DOI] [PubMed] [Google Scholar]
- 2.Chu CR, Williams AA, Coyle CH, Bowers ME. Early diagnosis to enable early treatment of pre-osteoarthritis. Arthritis Res Ther. 2012;14:212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Matzat SJ, Kogan F, Fong GW, Gold GE. Imaging strategies for assessing cartilage composition in osteoarthritis. Curr Rheumatol Rep. 2014;16:462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Middleton A, Fritz SL, Lusardi M. Walking speed: the functional vital sign. J Aging Phys Act. 2015;23:314–322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.White DK, Niu J, Zhang Y. Is symptomatic knee osteoarthritis a risk factor for a trajectory of fast decline in gait speed? Results from a longitudinal cohort study. Arthritis Care Res (Hoboken). 2013;65:187–194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Colbert CJ, Song J, Dunlop D, Chmiel JS, Hayes KW, Cahue S, et al. Knee confidence as it relates to physical function outcome in persons with or at high risk of knee osteoarthritis in the osteoarthritis initiative. Arthritis Rheum. 2012;64:1437–1446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Zeni JA Jr., Axe MJ, Snyder-Mackler L. Clinical predictors of elective total joint replacement in persons with end-stage knee osteoarthritis. BMC Musculoskelet Disord. 2010;11:86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Pietrosimone B, Blackburn JT, Harkey MS, Luc BA, Hackney AC, Dsc, et al. Walking speed as a potential indicator of cartilage breakdown following anterior cruciate ligament reconstruction. Arthritis Care Res. 2015. 2016;68:793–800 [DOI] [PubMed] [Google Scholar]
- 9.Luc B, Gribble P, Pietrosimone B. Osteoarthritis Prevalence following Anterior Cruciate Ligament Reconstruction: A Systematic Review and Numbers Needed to Treat Analysis. J Athl Train. 2014;49:806–819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ajuied A, Wong F, Smith C, Norris M, Earnshaw P, Back D, et al. Anterior cruciate ligament injury and radiologic progression of knee osteoarthritis: a systematic review and meta-analysis. Am J Sports Med. 2014;42:2242–2252. [DOI] [PubMed] [Google Scholar]
- 11.Oiestad BE, Engebretsen L, Storheim K, Risberg MA. Knee osteoarthritis after anterior cruciate ligament injury: a systematic review. Am J Sports Med. 2009;37:1434–1443. [DOI] [PubMed] [Google Scholar]
- 12.Purser JL, Golightly YM, Feng Q, Helmick CG, Renner JB, Jordan JM. Association of slower walking speed with incident knee osteoarthritis-related outcomes. Arthritis Care Res. 2012;64:1028–1035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lester G The Osteoarthritis Initiative: A NIH Public-Private Partnership. HSS J. 2012;8:62–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Altman R, Brandt K, Hochberg M, Moskowitz R, Bellamy N, Bloch DA, et al. Design and conduct of clinical trials in patients with osteoarthritis: recommendations from a task force of the Osteoarthritis Research Society. Results from a workshop. Osteoarthritis Cartilage. 1996;4:217–243. [DOI] [PubMed] [Google Scholar]
- 15.Oiestad BE, White DK, Booton R, Niu J, Zhang Y, Torner J, et al. Longitudinal Course of Physical Function in People With Symptomatic Knee Osteoarthritis: Data From the Multicenter Osteoarthritis Study and the Osteoarthritis Initiative. Arthritis Care Res. 2016;68:325–331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lee J, Chang RW, Ehrlich-Jones L, Kwoh CK, Nevitt M, Semanik PA, et al. Sedentary behavior and physical function: Objective Evidence from the Osteoarthritis Initiative. Arthritis Care Res. 2015;67:366–373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Project 15 Test-Retest Reliability of Semi-quantitative Readings from Knee Radiographs. OAI; https://oai.epi-ucsf.org/datarelease/SASDocs/kXR_SQ_Rel_BU_Descrip.pdf. [Google Scholar]
- 18.Washburn RA, Smith KW, Jette AM, Janney CA. The Physical Activity Scale for the Elderly (PASE): development and evaluation. J Clin Epidemiol. 1993;46:153–162. [DOI] [PubMed] [Google Scholar]
- 19.Bohannon RW, Glenney SS. Minimal clinically important difference for change in comfortable gait speed of adults with pathology: a systematic review. J Eval Clin Pract. 2014;20:295–300. [DOI] [PubMed] [Google Scholar]
- 20.White DK, Zhang Y, Niu J, Keysor JJ, Nevitt MC, Lewis CE, et al. Do worsening knee radiographs mean greater chances of severe functional limitation? Arthritis Care Res (Hoboken). 2010;62:1433–1439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Motyl JM, Driban JB, McAdams E, Price LL, McAlindon TE. Test-retest reliability and sensitivity of the 20-meter walk test among patients with knee osteoarthritis. BMC Musculoskelet Disord. 2013;14:166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Zeni JA Jr., Higginson JS. Differences in gait parameters between healthy subjects and persons with moderate and severe knee osteoarthritis: a result of altered walking speed? Clin Biomech (Bristol, Avon). 2009;24:372–378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Chiu MC, Wang MJ. The effect of gait speed and gender on perceived exertion, muscle activity, joint motion of lower extremity, ground reaction force and heart rate during normal walking. Gait Posture. 2007;25:385–392. [DOI] [PubMed] [Google Scholar]
- 24.Chung MJ, Wang MJ. The change of gait parameters during walking at different percentage of preferred walking speed for healthy adults aged 20–60 years. Gait Posture. 2010;31:131–135. [DOI] [PubMed] [Google Scholar]
- 25.Cook TM, Farrell KP, Carey IA, Gibbs JM, Wiger GE. Effects of restricted knee flexion and walking speed on the vertical ground reaction force during gait. J Orthop Sports Phys Ther. 1997;25:236–244. [DOI] [PubMed] [Google Scholar]
- 26.Radin EL, Martin RB, Burr DB, Caterson B, Boyd RD, Goodwin C. Effects of mechanical loading on the tissues of the rabbit knee. J Orthop Res. 1984;2:221–234. [DOI] [PubMed] [Google Scholar]
- 27.Miller RH, Edwards WB, Brandon SC, Morton AM, Deluzio KJ. Why don’t most runners get knee osteoarthritis? A case for per-unit-distance loads. Med Sci Sport Exerc. 2014;46:572–579. [DOI] [PubMed] [Google Scholar]
- 28.White DK, Neogi T, Zhang Y, Niu J, Katz PP. Association of Slow Gait Speed With Trajectories of Worsening Depressive Symptoms in Knee Osteoarthritis: An Observational Study. Arthritis Care Res. 2017;69:209–215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Manual OIO. 20-Meter Walk. Vol Version 1.0p, 3/15/062006. [Google Scholar]