

Abstract
Objective
To determine the early impacts of pediatric primary care parenting interventions on parent cognitive stimulation in low socio-economic status families and whether these impacts are sustained up to 1.5 years after program completion.
Study design
This randomized controlled trial included assignment to 1 of 2 interventions (Video Interaction Project [VIP] or Building Blocks [BB]) or to a control group. Mother–newborn dyads were enrolled postpartum in an urban public hospital. In VIP, dyads met with an interventionist on days of well-child visits; the interventionist facilitated interactions in play and shared reading through provision of learning materials and review of videotaped parent–child interactions. In BB, parents were mailed parenting pamphlets and learning materials. We compare trajectories of cognitive stimulation for parents in VIP and control from 6 to 54 months.
Results
546 families contributed data. VIP was associated with enhanced reading, parent verbal responsivity, and overall stimulation at all assessment points, with analyses demonstrating a .38 standard deviation increase in cognitive stimulation overall. Trajectory models indicated long-term persistence of VIP impacts on reading, teaching, and verbal responsivity.
Conclusions
VIP is associated with sustained enhancements in cognitive stimulation in the home 1.5 years after completion of the program and support expansion of pediatric interventions to enhance developmental trajectories of low-SES children.
Trial Registration
Keywords: prevention, poverty, child development, intervention
Differences in the early home environment related to the amount of cognitive stimulation provided by parents, such as reading, teaching, and overall verbal responsivity, explain much of the variance in child developmental outcomes(1–4). Furthermore, evidence suggests that both the quantity and quality of these interactions in the home vary markedly by socioeconomic status (SES)(5–7). Therefore, parent-child interactions are important targets for preventive interventions aiming to reduce poverty-related disparities in developmental outcomes.
The pediatric primary care platform offers unique opportunities to implement widely strategies to bolster parent-child interactions and prevent the emergence of poverty-related disparities; this is due to the near universality of access, the frequency of contact, and the potential for low cost afforded by leveraging existing resources(8). The Video Interaction Project (VIP) is a pediatric healthcare intervention, built upon the Reach out and Read (ROR) model (9,10), which is designed to capitalize on these opportunities beginning at birth. VIP provides learning materials, such as toys and books, and utilizes review and reinforcement of positive parenting behaviors in the context of videotaped parent-child interactions, led by a designated parenting coach who meets one-on-one with families at the time of well-child visits. In a pilot randomized controlled trial, VIP was found to enhance parenting, including reported reading, teaching, and verbal responsivity(11,12) and observed mother utterances(13). However, because impacts were not assessed beyond intervention conclusion, it is unknown whether VIP impacts on parenting may be sustained long-term, an important criterion for program effectiveness as highlighted by the US Department of Health and Human Service(14). A second, larger RCT called the Bellevue Project for Early Language, Literacy, and Education Success (the BELLE Project), continued follow-up of VIP families beyond intervention conclusion and is providing the opportunity to address this need. This RCT also includes a sample with greater sociodemographic diversity than the prior RCT, particularly regarding level of education and social risk, and helps to determine whether VIP impacts on parenting extend to a broader population of low-SES families. In this RCT, VIP is being evaluated alongside a lower intensity intervention called Building Blocks (BB) and a control group receiving ROR as standard of care. Early findings from this RCT reported the emergence of parenting impacts at child age 6 months related to both VIP and BB, with effects of VIP being more robust and pronounced(15). The primary goal of the current investigation is to assess whether these early VIP impacts were sustained over the intervention period as well as 1.5 years after intervention completion. We hypothesized that VIP would be associated with enhanced parenting compared with controls, with impacts sustained beyond program completion. We also investigated whether BB would continue to be associated with enhanced parenting during late infancy/toddlerhood.
METHODS
We performed a single-blind, 3-way RCT, with parent-child dyads assigned to one of two intervention strategies (VIP and BB) or to a control group receiving ROR only (as standard of care). IRB approval was obtained from New York University School of Medicine, Bellevue Hospital Center (BHC), and the New York City Health and Hospitals Corporation. Parents provided informed consent prior to participation. The trial was registered at clinicaltrials.gov (NCT00212576).
Enrollment was performed in the postpartum ward of an inner-city public hospital (BHC) serving low SES, primarily immigrant families, between November, 2005, and October, 2008. Consecutive mother-newborn dyads planning to receive pediatric primary care at our institution and meeting eligibility criteria were enrolled, designed to provide homogeneity of medical status across groups, enhance feasibility, and reduce likelihood of receipt of prior/concurrent comparable services. Eligibility criteria were: no significant medical complications (requiring extended stay or transfer to Level II/III nursery, or with potential adverse developmental consequences); full term gestation ≥37 weeks, birth weight ≥2,500gm, and singleton gestation. Feasibility criteria were: mother primary caregiver, mother able to maintain contact (working phone, intention to maintain geographic proximity), and mother’s primary language English or Spanish. Criteria for no prior or concurrent services were: mother ≥18 years (as adolescent mothers routinely receive parenting services at our institution); no participation in a prior study of VIP or BB.
Following enrollment, dyads were randomized to VIP, BB, or control using a random number generated using Microsoft Excel. Randomization group assignments were concealed from research assistants performing enrollment. Families in all groups received the same well child care, delivered by the same primary care pediatricians. Beginning at 6 months of age, all families received ROR as standard of care. VIP, BB, and Control, the three groups analyzed in this study, are described below:
Video Interaction Project
VIP, which has been previously described(16–19), takes place from birth to 3 years, with up to fifteen 25-30 minute sessions taking place primarily on the day of primary care visits. Sessions are facilitated by an interventionist, who meets one on one with families, providing an individualized, relationship-based intervention. At each session, parent-child dyads are video-recorded for approximately 5 minutes while interacting with a developmentally appropriate toy and/or book provided by the program. These recorded interactions are then reviewed together by the interventionist and the parent, while the interventionist indicates instances of positive parenting behaviors during the interaction (eg, responding to vocalizations, engaging in conversation), in effect reinforcing these behaviors and promoting self-reflection on the part of the parent. To promote generalization of positive parenting behaviors in the home, the video is given to the parent to take home, along with the learning material used in the interaction. Parents are also given pamphlets which provide suggestions for interactions in the contexts of play, shared reading, and everyday routines, and also encouraged to develop plans for interactions to promote their child’s development. VIP is estimated to cost $150–200 per child per year at scale(13).
Building Blocks
As previously described(16,19), BB utilizes mailed parenting pamphlets and learning materials to promote parenting self-efficacy and positive parent-child interactions. Each month, parents are mailed a toy or book, along with a newsletter that provides information on encouraging learning and ideas for interactions around a specific developmental goal. Parents are also asked to fill out the Ages and Stages developmental questionnaires every 4–6 months. BB has an estimated cost of $75–100 per child per year(19).
Control
As described above, control families received all standard pediatric care, including all routine anticipatory guidance, developmental surveillance. In addition, Reach out and Read was delivered to participants in all 3 groups.
Measures
As described elsewhere, we assessed baseline sociodemographic and other data characterizing the sample based on parental interview at enrollment. For parents, this included mother’s age, country of origin, education level, primary language spoken, and marital status, and family Hollingshead Four Factor Socioeconomic Status (SES) based on parental education and occupation(20). As in previous studies(17,19), mothers were considered to be at increased social risk if they had one or more of: homelessness, being a victim of violence, having involvement with child protective services, financial difficulties, food insecurity, smoking or alcohol use during pregnancy, or having a history of prior mental illness including depression. For the child, we obtained information about sex and birth order. In addition, at the 6-month assessment, we assessed maternal literacy in the mother’s preferred language using the Woodcock-Johnson III(21)/Bateria III Woodcock-Muñoz Tests of Achievement(22), Letter-Word Identification Test.
Dependent variables
We assessed parent cognitive stimulation in the context of play, shared reading, and daily routines using the StimQ2-Infant (StimQ2-I) at child age 6 months, the StimQ2-Toddler (StimQ2-T) at child ages 14 and 24 months, and the StimQ2-Preschool (StimQ2-P) at ages 36 and 54 months. The StimQ utilizes a structured interview with the child’s caregiver to assess interactions in the home(23) and has been validated, and recently re-validated for use in low SES populations in English and Spanish(24,25). The StimQ2-I, StimQ2-T and the StimQ2-P consist of 4 subscales, which are summed together for a total score (StimQ2-I range 0–42, StimQ2-T range 0–46, StimQ2-P range 0–60). ALM (Availability of Learning Materials) assesses learning materials such as toys provided by the caregiver in the home (StimQ2-I range 0–6, StimQ2-T range 0–7; StimQ2-P range 0–8). READ (Reading Activities) assesses number and diversity of books read to the child, frequency of reading activities, and associated interactions (StimQ2-I range 0–15, StimQ2-T range 0–19; StimQ2-P range 0–18). PIDA (Parental Involvement in Developmental Advancement) assesses caregiver teaching and play activities, such as naming objects, teaching the child to play with toys, and playing make believe games with the child (StimQ2-I range 0–5, StimQ2-T range 0–5; StimQ2-P range 0–15). PVR (Parental Verbal Responsivity) assesses caregiver-child verbal interactions such as talking while feeding and making sounds together (StimQ2-T range 0–16, StimQ2-T range 0–15; StimQ2-P range 0–19). A limited number of StimQ items were missing due to their inclusion after the initiation of data collection. For those items, mean imputation at the item level was utilized for calculation of the overall scales used in these analyses. To allow for analyses of trajectories of cognitive stimulation over time based on different versions of the StimQ, z-scores were calculated for StimQ subscale and total scores.
At children’s age of 54 months, parent verbal input was also assessed in the context of videotaped shared book reading interactions. For this assessment, parents were asked to share the wordless picture book, Frog, Where Are You? r(26) with their child in any way that they would at home. They were video recorded and allowed up to 10 minutes to complete the shared book reading interaction. Book reading interactions were transcribed and coded using the Codes for Human Analysis of Transcripts (CHAT)(27) system and analyzed using the Computerized Language Analysis (CLAN)(27). Collection and transcription of interactions were performed by research associates blinded to group assignment. Three measures of Parent Verbal Input were obtained including Utterances (total number of idea units verbally uttered by mother), Word Types (total number of different words used by the mother), and Word Tokens (total number of words used by the mother).
Statistical analyses
225 families were enrolled per group to provide >80% power to find .67 SD effects for VIP and BB compared with control, assuming 33% attrition. Statistical analyses were performed using Stata SE 14(28) and IBM SPSS 20(29). All statistical analyses comparing VIP and BB with Control for parenting over time were performed based on intention to treat. Due to limited resources to conduct follow-up assessments, BB was assessed only through 24 months, and thus comparisons including this group were not possible beyond that time point. At age 3 years, VIP and Control families were offered participation in a second phase of study which included random assignment to either a preschool component of the VIP intervention (or to control). Although future analyses will address impacts of this preschool component, the focus of the present investigation was limited to impacts of VIP delivered during the birth-age 3 period; therefore, assignment to the preschool intervention was adjusted for in all present analyses involving data beyond 36 months. As previously noted, differences in parent cognitive stimulation among VIP, BB, and Control groups at age 6 months have been published in a prior study(15). For the current investigation, impacts of VIP and BB on parent cognitive stimulation at ages 14, 24, 36, and 54 months were assessed using multiple regressions, in which VIP and BB were dummy coded and compared with controls. Regression analyses were adjusted for child age and sex (as the outcome variables are not normed for these factors), as well as maternal literacy/education given demonstrated moderation of the outcome variable in prior study of these interventions(12,16). Effect sizes were calculated using Cohen’s d. We also performed secondary, within group analyses at 36- and 54-months to determine the effect of VIP dose on parenting outcomes for VIP families. Consistent with prior analyses(15), we dichotomized the number of VIP visits and used regressions to compare parenting outcomes of those completing at least 5 visits with those completing 1 through 4 visits. We also performed comparisons of trajectories of parent cognitive stimulation for the VIP and Control groups over time from 6 to 54 months using multilevel modeling with age, group, and group × age included as predictors of mean Stim-Q z-scores for total StimQ and each StimQ subdimension. Based on prior analyses showing education to be a moderator of VIP impact and literacy to be a mediator of associations between education and parent-child interaction(11,12,15), we also used multilevel modeling to determine whether parenting trajectories for VIP and Control groups were affected by level of maternal literacy/education (9th grade or higher literacy; education used as proxy for any cases missing literacy) by assessing the significance of a maternal literacy/education by group interaction. Furthermore, based on evidence of increased impacts of VIP on child behavior outcomes for children in families with greater social risk in this sample(19), we explored whether trajectories of parenting were moderated by level of social risk by assessing the significance of a social risk by group interaction. Finally, to analyze parent verbal input in the context of parent-child book reading at 54 months, we performed multiple regression analyses, also based on intention to treat and adjusted for child sex, age, and maternal literacy/education, with effect sizes calculated using Cohen’s d.
RESULTS
Enrollment took place from November, 2005 through October, 2008. Of 905 eligible dyads, 675 (74.6%) were enrolled and randomized to VIP (n=225), BB (n=225) and Control (n=225) (Figure; available at www.jpeds.com). All families were allocated to group as randomized and assessed based on group assignment; however, 16 of 225 allocated to VIP attended primary care elsewhere and did not participate in any VIP visits prior to 36 months. BB families were not followed beyond 24 months.
Figure 1.
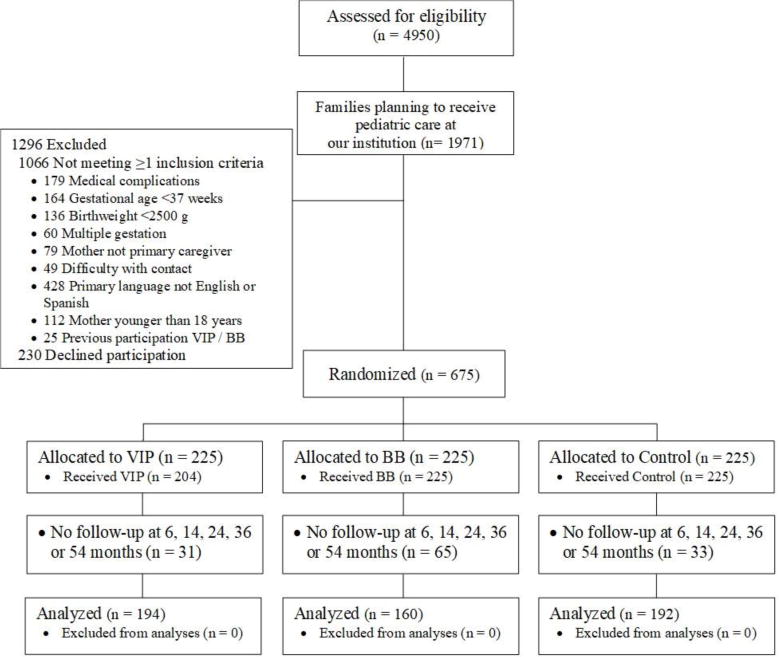
Participant enrollment and assessment
546 of 675 families (80.7%) were assessed for cognitive stimulation one or more times over the course of five time points, including 194/225 VIP families (86.2%), 160/225 (70.7%) BB families, and 192/225 controls (85.3%). A total of 1,365 observations of cognitive stimulation were recorded. Mean child age in months at each of the five assessments was: 6.9 (1.3) at 6 months, 15.5 (1.6) at 14 months, 25.7 (2.3) at 24 months, 39.1 (3.7) at 36 months, and 57.9 (4.5) at 54 months. Table I (available at www.jpeds.com) shows characteristics by group for all participants enrolled at baseline and for those participants with data collected during at least one assessment point. Groups did not differ significantly for any baseline socio-demographic characteristic or for maternal word reading assessed at the 6-month assessment. Dyads assessed during at least one assessment point did not significantly differ from those who were not assessed for maternal age, marital status, education, Hollingshead SES, level of social risk, child birth order, or child sex. However, assessed mothers were more likely to speak Spanish as primary language (P < .001), to self-identify as Latina (p <.05), and to be immigrants to the US (p <.001). Of 194 VIP families assessed at one or more assessment points, 184 (94.8%) attended at least 1 VIP visit; 130 of these families (67.0%) attended 7 or more of 15 possible visits. There were no adverse events related to participation.
Table 1.
Demographic Characteristics of Analytic Sample
| VIP (N = 194) |
BB (N = 159) |
C (N = 192) |
p† | |
|---|---|---|---|---|
| Mother <Age 21 | 10% | 13% | 10% | 0.75 |
| Hispanic | 93% | 95% | 91% | 0.28 |
| Non-High School Graduate | 61% | 51% | 60% | 0.13 |
| Born outside US | 90% | 85% | 85% | 0.25 |
| Married/partner | 83% | 87% | 84% | 0.53 |
| Spanish speaking | 81% | 77% | 79% | 0.71 |
| Low SES | 92% | 87% | 91% | 0.27 |
| Female child | 54% | 50% | 48% | 0.51 |
| First born child | 43% | 40% | 38% | 0.57 |
| Low maternal literacy (<9th grade) | 32% | 31% | 23% | 0.12 |
| High social risk | 35% | 28% | 36% | 0.94 |
p-value based on Chi-Square tests.
Primary analyses
Table 2 shows impacts of VIP and BB on parent cognitive stimulation at 14 and 24 months. At 14 months, VIP families had increased overall StimQ relative to Control with effect size (ES) based on Cohen’s d of .54, as well as increased interactions in reading, teaching and verbal responsivity, with ES ranging from .39 to .49, and a marginal increase in the availability of learning materials in the home. At 14 months, BB families engaged in significantly more teaching behaviors than control families (ES=.22). BB families also engaged in more parental verbal responsivity and overall cognitive stimulation, but these differences did not reach significance. At 24 months, VIP was also associated with enhanced reading, verbal responsivity, and overall parent cognitive stimulation when compared with controls, with ES ranging from .27–.36. BB families did not differ from Controls at this timepoint.
Table 2.
Mean (SD) Parenting Scores at Child Age 14 Months and 24 Monthsa
| 14 Months | 24 Months | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||
| VIP (n=110) |
BB (n=105) |
C (n=109) |
ESb BB vs. C |
ESb VIP vs. C |
VIP (n=161) |
BB (n=62) |
C (n=151) |
ESb BB vs. C |
ESb VIP vs. C |
|
| READ | 8.03 2.68) |
7.32 (2.71) |
7.16 (2.56) |
0.09 | .39** | 8.44 (2.68) |
8.12 (2.45) |
7.82 (2.71) |
0.15 | .27* |
| PIDA | 3.32 (1.54) |
3.00 (1.31) |
2.67 (1.45) |
.27* | .49*** | 3.51 (1.36) |
3.39 (1.35) |
3.39 (1.32) |
0.06 | 0.11 |
| PVR | 8.61 (3.26) |
7.84 (2.78) |
7.30 (3.07) |
.24t | .48*** | 8.77 (3.30) |
7.47 (2.71) |
7.81 (2.89) |
0.02 | .36** |
| ALM | 4.27 (1.78) |
3.74 (1.68) |
3.80 (1.78) |
0.08 | .22t | 5.23 (1.69) |
5.37 (1.30) |
5.19 (1.57) |
0.18 | 0.06 |
| StimQ Total |
24.20 (7.09) |
21.91 (6.35 |
20.95 (6.43) |
.22t | .54*** | 25.94 (7.28) |
24.33 (5.93) |
24.21 (6.45) |
0.11 | .30** |
p<.05,
p<.01,
p<.001,
≤.10
Analyses adjusted for child age, gender, and maternal literacy/education
Effect size based on Cohen’s d
Table 3 shows impacts of VIP on cognitive stimulation during the preschool period at 36 and 54 months. At 36 months, VIP was associated with enhanced reading, verbal responsivity, and marginally with enhanced overall cognitive stimulation when compared with controls, with ES ranging from .19–.27. Finally, at 54 months, 1.5 years after VIP intervention completion, VIP was associated with significantly enhanced reading, verbal responsivity, and greater overall cognitive stimulation, with ES ranging from .35–.38. VIP at 54 months was also associated with enhanced teaching with ES=.23, but this finding did not reach significance. Within group analyses of families in VIP indicated that greater VIP dose (at least 5 doses) was associated with greater overall cognitive stimulation in the home both at 36 months, β= .17, p <.05, and at 54 months, β= .17, p <.05.
Table 3.
| 36 Months | 54 Months | |||||
|---|---|---|---|---|---|---|
|
| ||||||
| VIP (n=153) |
C (n=149) |
ESc VIP vs. C |
VIP (n=123) |
C (n=130) |
ESc VIP vs. C |
|
| READ | 8.73 (3.11) | 8.09 (3.33) | .23* | 10.43 (4.2) | 10.00 (4.30) | .35** |
| PIDA | 6.22 (2.64) | 6.39 (2.50) | 0.03 | 9.75 (2.72) | 9.06 (2.99) | .23t |
| PVR | 5.68 (2.30) | 5.15 (2.21) | .27* | 9.20 (3.63) | 8.10 (3.77) | .36** |
| ALM | 6.13 (2.28) | 5.91 (2.30) | 0.13 | 5.99 (1.50) | 5.47 (1.69) | 0.10 |
| StimQ Total | 27.76 (8.21) | 25.55 (8.09) | .19t | 35.33 (8.82) | 32.63 (10.22) | .38** |
p<.05,
p<.01,
p<.001,
≤.10
BB not included in table due to lack of data beyond 24 months
Analyses adjusted for child age, gender, maternal literacy/education, and assignment to VIP 3–5
Effect Size based on Cohen’s d
Table 4 shows results from multilevel models of VIP impacts on trajectories of reading, teaching, parent verbal responsivity, availability of learning materials in the home, and overall cognitive stimulation as measured by the StimQ. Results of multilevel modeling yielded a main effect of group, indicating that VIP mothers engaged in more cognitive stimulation than control mothers beginning at child age 6 months and continuing through 54 months; this was true for reading, z = 3.78, p <.001, teaching, z = 2.77, p <.01, parent verbal responsivity, z = 4.80, p <.001, availability of learning materials in the home, z = 2.17, p <.05, and overall cognitive stimulation z = 4.47, p <.001. The coefficient associated with the effect of overall cognitive stimulation indicated that the cognitive stimulation engaged in by VIP mothers from 6 to 54 months was on average .38 SD greater than that engaged in by control mothers. There was a significant group by age interaction found for availability of learning materials in the home, z= −2.56, p <.05, and marginally significant for overall cognitive stimulation in the home, z=−1.96, p =.05, suggesting that the group differences on these outcomes over time remained significant, yet lessened. However, for reading, teaching, and verbal responsivity, there was no significant interaction found between group and age, suggesting that the rate of change over time was similar for both VIP and Control groups, after the initial increase experienced by VIP mothers by 6 months of age.
Table 4.
Multi-level model Results: Predictors of StimQ z-scores 6–54 months
| Unstandardized Confidence |
95% Coefficients Interval |
p | |
|---|---|---|---|
| StimQ Read | |||
| Main effects modela | |||
| VIP | 0.303 | 0.146 – 0.461 | <.001 |
| Age | 0.000 | −0.002 – 0.003 | 0.78 |
| Interaction modelb | |||
| VIP × Age | −0.0002 | −0.005 – 0.004 | 0.9 |
| Moderation modelsc | |||
| VIP × Maternal Lit/Education | 0.011 | −0.341 – 0.363 | 0.95 |
| VIP × Social Risk | 0.072 | −0.268 – 0.411 | 0.68 |
| StimQ PIDA | |||
| Main effects modela | |||
| VIP | 0.196 | 0.057 – 0.334 | 0.01 |
| Age | 0.000 | −0.003 – 0.003 | 0.84 |
| Interaction modelb | |||
| VIP × age | −0.004 | −0.010 – 0.001 | 0.11 |
| Moderation modelsc | |||
| VIP × Maternal Lit/Education | 0.192 | −0.117 – 0.501 | 0.22 |
| VIP × Social Risk | 0.069 | −0.138 – 0.275 | 0.51 |
| StimQ Parent Verbal Responsivity | |||
| Main effects modela | |||
| VIP | 0.384 | 0.227 – 0.541 | <.001 |
| Age | −0.001 | −0.004 – 0.001 | 0.35 |
| Interaction modelb | |||
| VIP × age | −0.003 | −0.008 – 0.001 | 0.14 |
| Moderation modelsc | |||
| VIP × Maternal Lit/Education | 0.05 | −0.301 – 0.401 | 0.78 |
| VIP × Social Risk | −0.04 | −0.274 – 0.195 | 0.74 |
| StimQ Availability of Learning Materials | |||
| Main effects modela | |||
| VIP | 0.174 | 0.017 – 0.331 | 0.03 |
| Age | −0.00001 | −0.003 – 0.003 | 0.99 |
| Interaction modelb | |||
| VIP × age | −0.006 | −0.010 – −0.001 | 0.01 |
| Moderation modelsc | |||
| VIP × Maternal Lit/Education | −0.111 | −0.463 – 0.241 | 0.54 |
| VIP × Social Risk | 0.045 | −0.191 – 0.280 | 0.71 |
| StimQ Total | |||
| Main effects modela | |||
| VIP | 0.375 | 0.211 – 0.540 | <.001 |
| Age | −0.0002 | −0.002 – 0.003 | 0.84 |
| Interaction modelb | |||
| VIP × age | −0.004 | −0.008 – 0.000 | 0.05 |
| Moderation modelsc | |||
| VIP × Maternal Lit/Education | 0.048 | −0.320 – 0.417 | 0.80 |
| VIP × Social Risk | 0.016 | −0.230 – 0.262 | 0.90 |
Adjusts for child gender, child age, maternal literacy/education, and 3–5 at 54 months. Coefficients for VIP represent the difference in z scores for VIP compared to control across the 6 – 54-month period.
Includes all predictors from Main effects model in addition to listed interaction terms. Coefficients represent difference in slope between 6 and 54 months for VIP compared to control.
Two separate models including all predictors from Main effects model in addition to listed interaction terms. Coefficients represent the difference in VIP impact for different levels of maternal literacy/education and social risk.
Further analyses were conducted to assess whether maternal literacy/education or level of social risk moderated positive impacts of VIP on cognitive stimulation. Subgroup analyses suggested comparable effect sizes for both literacy (low literacy ES= .33, p<.05; high literacy ES= .39, p<.001; interaction p=.80) or social risk (low risk ES= .36, p <.001; high risk ES= .36, p<.05; interaction p=.92), suggesting that associations between VIP and trajectories of parent cognitive stimulation did not vary depending on the levels of these characteristics.
Finally, we performed analyses based on observed measures of parent verbal input in the context of shared wordless picture book reading between mothers and their children at 54 months of age. Findings from these analyses of observed parent behaviors converged with findings obtained from assessment of behaviors using StimQ, demonstrating that participation in VIP was associated with increased parent language input (Table 5). In particular, VIP mothers used significantly more utterances altogether, word types (ie, number of different words), and word tokens (ie, total number of words) while sharing a wordless picture book with their children than mothers in the control condition.
Table 5.
VIP Impacts on Observed Parenting at 54 Months
| VIP (n = 119) |
C (n = 111) |
p† | ES | |
|---|---|---|---|---|
| Mother # Utterances | 148.61 (58.13) |
132.58 (57.45) |
0.04 | 0.29 |
| Mother # Word Types | 161.05 (53.96) |
147.41 (49.57) |
0.03 | 0.30 |
| Mother # Word Tokens | 534.97 (217.86) |
476.4 (209.81) |
0.03 | 0.30 |
p-value based on multiple adjusted regression adjusting for child age, child gender, maternal literacy/education
DISCUSSION
This study demonstrates that pediatric primary care parenting interventions delivered beginning in early infancy can be effective at promoting early and long-lasting changes in positive parenting behaviors with implications for enhancing development and preventing disparities often experienced by children from low-SES households. Both interventions studied, VIP and BB, had impacts on aspects of parent-child interaction critical to early development.
In line with earlier findings from a prior(11,12) and the current RCT(15), VIP and BB, which begin in early infancy, were associated with enhanced parent-child interactions at 14 months. These findings reinforce previous conclusions from prior studies that pediatricians should consider intervening with families beginning in early infancy. In addition, VIP had impacts on parenting that were larger and more robust than those of BB. Participation in VIP was associated with changes in multiple domains of parent cognitive stimulation including reading, verbal responsivity, availability of learning materials, and teaching behaviors during the infancy, toddler, and preschool periods. On the other hand, BB was primarily related to enhanced teaching behaviors and only marginally related to enhanced verbal responsivity at child age 14 months. Impacts of BB at 14 months were similar in magnitude to those reported at 6 months; however, unlike at 6 months, BB was not found to be associated with changes in availability in learning materials and reading behaviors at this age. Furthermore, no differences in parenting were associated with BB participation at child age 24 months. The reduced sample size of BB at 24 months may limit interpretability of findings at that time point. However, results could suggest that although parenting advice given through parenting pamphlets may be sufficient to increase select parenting behaviors, other intervention components utilized by VIP but not BB, such as modeling, video-prompted self-reflection, and provision of social support through a relationship with an interventionist, may be important for targeting other parenting behaviors, such as reading and other aspects of parenting responsivity more broadly. Future research delineating which intervention components are most predictive of its efficacy would be useful for dissemination of this model in primary care.
The effects of VIP on parenting were robust and experienced long-term. In cross-sectional analyses, VIP was associated with significant enhancements in overall parent cognitive stimulation, reading behaviors, and parent verbal responsivity at ages 24, 36, and 54 months. Sustained impacts of VIP were further supported by analyses of parenting trajectories using multilevel modeling. Findings demonstrated that impacts of VIP on parenting, including reading, teaching, verbal responsivity, and availability of learning materials in the home experienced by 6 months persisted through child age 54 months, 1.5 years post-intervention completion. Significant age by group interactions in multilevel models reveal diminishing impact over time for provision of learning materials in the home, but no age by group interaction was observed for other parenting measures, indicating persistence of early VIP impacts on reading, teaching, and verbal responsivity. Variability in persistence of outcomes suggest that VIP, despite distributing learning materials to families, may not meaningfully be affecting the availability of learning materials in the home per se after infancy, but rather is changing the way in which parents interact with their children with the materials that they do have; further study is needed to disentangle the effects of the intervention on these different aspects of parenting. Unlike prior analyses of VIP’s impact on socioemotional development (19), VIP’s impact on parenting was not found to vary with of social risk; this suggests that there may be some differences in the mechanisms by which these domains are affected by VIP. Additionally, current findings yielded comparable impacts on parenting regardless of maternal literacy/education, differing from prior analyses demonstrating some reduction in impacts on parent cognitive stimulation for families with very low literacy(15). Although additional study, including qualitative research, would be needed to understand why this was the case, findings suggest the possibility that cumulative exposure to VIP may have resulted in greater impacts for these families.
Demonstration of long-term VIP impacts on parenting was additionally supported in this study with evidence from observed parent verbal input, including increased number of utterances, word types, and word tokens in the context of parent-child book reading at 54 months of age. Taken together, evidence demonstrates potential of parenting interventions in pediatric primary care to lead to meaningful changes in parenting that are sustained over a year beyond program completion, meeting this aforementioned key aspect of program effectiveness as detailed by the U.S. Department of Health and Human Service(14). Ongoing study of the cohort will assess whether these ongoing impacts of VIP on parenting are also related to developmental outcomes as well as early school achievement.
Effect sizes on parent cognitive stimulation found for mothers who participated in VIP are comparable with those seen in other platforms for intervention during the infant-toddler period including home visitation and center-based programs(30–32), as well as to those seen in other programs utilizing review of videotaped interactions to promote self-reflection such as Play and Learning Strategies (33). Future consideration should be given to how videotaped interactions can also be used in primary care therapeutically to foster positive parent-child interactions for families identified to have particularly high risk in this area, as done in programs such as the Circle of Security(34). Although some effects became more modest over time, effects on parent reading and teaching and verbal responsivity were robust and long-lasting, with evidence of continued measurable differences in parenting behaviors 1.5 years after the conclusion of the VIP program. Such differences in the early home environment are likely to have cascading impacts on domains of child development important for transition to school and early academic achievement(1,5). Given the relatively lower cost associated with pediatric primary care parenting interventions(8), and the opportunity for population-wide application, findings may have important implications for public health policy.
There were three main limitations to this study. First, due to limitations in resources, we were unable to follow BB fully beyond 14 months, and at all beyond 24 months. The lower sample size of the BB group at 24 months may have left analyses underpowered to detect impacts of BB at this timepoint. Second, results at 6-36 months were based entirely on parent report, which despite being obtained from measures that are reliable and valid, can be subject to biases. However, results converged with observed measures of verbal input at 54 months in shared book reading interactions. Third, participating mothers were primarily first generation, Hispanic/Latino immigrants, and results therefore may not generalize to families with other sociodemographic characteristics.
In conclusion, this study provides evidence that pediatric primary care parenting interventions for low-SES families from birth to 3 years can result in sustained enhancements in parent-child interactions critical for early development and school readiness. Findings contribute support for the introduction of these programs in infancy, and suggest that ongoing implementation may have continued impacts prior to school entry. Given the potential for low cost and for population-level reach offered by the primary care platform, findings suggest that intervention strategies utilizing this platform may play an important role in enhancing the early home environment and thereby preventing poverty-associated disparities in readiness for school.
Acknowledgments
We thank the many individuals who contributed to this project, including Virginia Flynn, Gilbert Foley, Linda van Schaick, Jenny Arevalo, Caroline Raak, Jennifer Ledesma, Lisa White, Kristina Vlahovicova, Nina Burtchen, Angelica Alonso, Andrea Paloian, Diego Catalan Molina, Aida Custode, Yuliya Gurevich, and Maya Matalon. We would especially like to thank the parents and children who participated in this research project.
Supported by the National Institutes of Health (R01 HD047740 01-09, Supplement 3R01HD047740-08S1, R01 HD40388 01-04 [to A.M.]), the Tiger Foundation, the Marks Family Foundation, the Rhodebeck Charitable Trust, Children of Bellevue, Inc, and KiDS of NYU Foundation, Inc.
Abbreviations
- ALM
Availability of Learning Materials
- BB
Building Blocks
- PIDA
Parent Involvement in Developmental Advance
- PVR
Parent Verbal Responsivity
- READ
Reading Activities
- ROR
Reach Out and Read
- SD
standard deviation
- SES
socioeconomic status
- StimQ2-I
StimQ Infant Revised
- StimQ2-T
StimQ Toddler Revised
- StimQ2-P
StimQ Preschool Revised
- VIP
Video Interaction Project
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
The authors declare no conflicts of interest.
Reprints: No reprints requested.
Portions of this study were presented as an abstract at the 2017 Society for Research in Child Development Biennial Meeting, April 6–8, 2017, Austin, Texas; the 2015 Society for Research in Child Development Biennial Meeting, March 19–21, 2015, Philadelphia, Pennsylvania; and the Pediatric Academic Societies annual meeting, May 4–7, 2013, Washington, D.C.
References
- 1.Chazan-Cohen R, Raikes H, Brooks-Gunn J, Ayoub C, Pan BA, Kisker EE, et al. Low-Income Children’s School Readiness: Parent Contributions Over the First Five Years. Early Educ Dev. 2009;20:958–77. [Google Scholar]
- 2.Bradley RH, Caldwell BM, Rock SL, Barnard KE, Gray C, Hammond MA, et al. Home Environment and Cognitive Development in the First 3 Years of Life: A Collaborative Study Involving Six Sites and Three Ethnic Groups in North America. Dev Psychol. 1989;25:217–35. [Google Scholar]
- 3.Tamis-LeMonda CS, Bornstein MH, Baumwell L. Maternal Responsiveness and Children’s Achievement of Language Milestones. Child Dev. 2001 May;72:748–67. doi: 10.1111/1467-8624.00313. [DOI] [PubMed] [Google Scholar]
- 4.Brooks-Gunn J, Markman L. The Contribution of Parenting to Ethnic and Racial Gaps in School Readiness. Futur Child. 2005;15:139–68. doi: 10.1353/foc.2005.0001. [DOI] [PubMed] [Google Scholar]
- 5.Lugo-Gil J, Tamis-LeMonda CS. Family resources and parenting quality: Links to children’s cognitive development across the first 3 years. Child Dev. 2008;79:1065–85. doi: 10.1111/j.1467-8624.2008.01176.x. [DOI] [PubMed] [Google Scholar]
- 6.Kato P, Brooks-Gunn J, Duncan GJ. Does Neighborhood and Family Poverty Affect Mothers’ Parenting, Mental Health, and Social Support ? 2012;56:441–55. [Google Scholar]
- 7.Hart B, Risley TR. Meaningful differences in the everyday experience of young American children. Paul H Brookes Publishing; 1995. [Google Scholar]
- 8.Cates CB, Weisleder A, Mendelsohn AL. Mitigating the Effects of Family Poverty on Early Child Development through Parenting Interventions in Primary Care. Acad Pediatr. 2016;16:S112–20. doi: 10.1016/j.acap.2015.12.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.High PC, Lagasse L, Becker S, Ahlgren I, Gardner A. Literacy Promotion in Primary Care Pediatrics : Can We Make a Difference ? Pediatrics. 2000;105:927–34. [PubMed] [Google Scholar]
- 10.Klass P. Pediatrics by the Book: Pediatricians and Literacy Promotion. Pediatrics. 2002;110(5):989–95. doi: 10.1542/peds.110.5.989. Available from: http://pediatrics.aappublications.org/cgi/doi/10.1542/peds.110.5.989. [DOI] [PubMed] [Google Scholar]
- 11.Mendelsohn AL, Dreyer BP, Flynn V, Tomopoulos S, Rovira I, Tineo W, et al. Use of videotaped interactions during pediatric well-child care to promote child development: A randomized, controlled trial. J Dev Behav Pediatr. 2005;26:34–41. [PMC free article] [PubMed] [Google Scholar]
- 12.Mendelsohn AL, Valdez PT, Flynn V, Foley GM, Berkule SB, Tomopoulos S, et al. Use of videotaped interactions during pediatric well-child care: Impact at 33 months on parenting and on child development. J Dev Behav Pediatr. 2007;28:206–12. doi: 10.1097/DBP.0b013e3180324d87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Mendelsohn AL, Cates CB, Weisleder A, Berkule SB, Dreyer BP. Promotion of Early School Readiness using Pediatric Primary Care as an Innovative Platform. Zero Three. 2013;34:29–40. [Google Scholar]
- 14.Avellar S, Paulsell D, Sama-Miller E, Del Grosso P, Akers L, Kleinman R. Home visiting evidence of effectiveness review : Executive summary [Internet] Washington, DC: 2015. Available from: http://homvee.acf.hhs.gov/HomVEE_Executive_Summary_2015.pdf. [Google Scholar]
- 15.Mendelsohn AL, Huberman HS, Berkule SB, Brockmeyer CA, Morrow LM, Dreyer BP. Primary care strategies for promoting parent-child interactions and school readiness in at-risk families: The Bellevue Project for Early Language, Literacy, and Education Success. Arch Pediatr Adolesc Med. 2011;165:33–41. doi: 10.1001/archpediatrics.2010.254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mendelsohn AL, Dreyer BP, Brockmeyer CA, Berkule-Silberman SB, Huberman HS, Tomopoulos S. Randomized controlled trial of primary care pediatric parenting programs: Effect on reduced media exposure in infants, mediated through enhanced parent-child interaction. Arch Pediatr Adolesc Med. 2011;165:42–8. doi: 10.1001/archpediatrics.2010.266. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21199979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Cates CB, Weisleder A, Dreyer BP, Berkule Johnson S, Vlahovicova K, Ledesma J, et al. Leveraging Healthcare to Promote Responsive Parenting: Impacts of the Video Interaction Project on Parenting Stress. J Child Fam Stud. 2016;25:827–35. doi: 10.1007/s10826-015-0267-7. Available from: http://link.springer.com/10.1007/s10826-015-0267-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Canfield CF, Weisleder A, Cates CB, Huberman HS, Dreyer BP, Legano LA, et al. Primary Care Parenting Intervention and Its Effects on the Use of Physical Punishment Among Low-Income Parents of Toddlers. J Dev Behav Pediatr. 2015;36:586–93. doi: 10.1097/DBP.0000000000000206. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26375804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Weisleder A, Cates B, Dreyer BP, Johnson B. Promotion of Positive Parenting and Prevention of Socioemotional Disparities. Pediatrics. 2016;137 doi: 10.1542/peds.2015-3239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hollingshead AB. Four factor index of social status (Unpublished Working Paper, 1975) Yale J Sociol [Internet] 2011;8:21–52. Available from: http://elsinore.cis.yale.edu/sociology/yjs/yjs_fall_2011.pdf#page=21. [Google Scholar]
- 21.Woodcock RW, Johnson MB, Mather N. Woodcock-Johnson Tests of Achievement: Form B. Riverside Publishing Company; 1990. [Google Scholar]
- 22.Alvarado R, Ruef ML, Schrank FA. Woodcock-Munoz language survey-revised Itasca. Riverside Publ; 2005. [Google Scholar]
- 23.StimQ Cognitive Home Environment [Internet] [cited 2015 Oct 5]. Available from: http://www.med.nyu.edu/pediatrics/developmental/research/belle-project/stimq-cognitive-home-environment.
- 24.Dreyer BP, Mendelsohn AL, Tamis-LeMonda CS. Assessing the child’s cognitive home environment through parental report: Reliability and validity. Early Dev Parent. 1996;5:271–87. [Google Scholar]
- 25.Mendelsohn AL, Cates CB, Tamis-LeMonda CS, Johnson M, Berkule SB, White LJ, et al. Assessment of the cognitive home environment through parent report: Reliability and validity of StimQ (Revised) Pediatric Academic Societies; Denver, CO: 2011. [Google Scholar]
- 26.Mayer M. Frog, where are you? Dial Press; New York: 1969. [Google Scholar]
- 27.Macwhinney B. The TalkBank Project Tools for Analyzing Talk – Electronic Edition Part 2: The CLAN Programs. 2016 [Google Scholar]
- 28.StataCorp LP. College Station. TX, USA. 2015
- 29.Arbuckle JL. IBM SPSS Amos 20 [computer software] Chicago: Amos Dev Corp; 2011. [Google Scholar]
- 30.Sweet M, Appelbaum M. Is Home Visiting an Effective Strategy? A Meta-Analytic Review of Home Visiting Programs for Families With Young Children. Child Dev. 2004;75:1435–56. doi: 10.1111/j.1467-8624.2004.00750.x. [DOI] [PubMed] [Google Scholar]
- 31.Love JM, Kisker EE, Ross C, Raikes H, Constantine J, Boller K, et al. The Effectiveness of Early Head Start for 3-Year-Old Children and Their Parents: Lessons for Policy and Programs. Dev Psychol. 2005;41:885–901. doi: 10.1037/0012-1649.41.6.88. [DOI] [PubMed] [Google Scholar]
- 32.Duffee JH, Mendelsohn AL, Kuo AA, Legano LA, Earls MF, COUNCIL ON COMMUNITY PEDIATRICS et al. Early Childhood Home Visiting. Pediatrics. 2017 doi: 10.1542/peds.2017-2150. [DOI] [PubMed] [Google Scholar]
- 33.Landry SH, Smith KE, Swank PR, Zucker T, Crawford AD, Solari EF. The effects of a responsive parenting intervention on parent-child interactions during shared book reading. Dev Psychol. 2012;48:969–86. doi: 10.1037/a0026400. [DOI] [PubMed] [Google Scholar]
- 34.Marvin R, Cooper G, Hoffman K, Powell B. The Circle of Security project : Attachment-based intervention with caregiver-preschool-child dyads. Attach Hum Dev. 2002;4:107–24. doi: 10.1080/14616730252982491. [DOI] [PubMed] [Google Scholar]