

Abstract
Background
Sedentary work is hazardous. Over 80% of all US jobs are predominantly sedentary, placing full‐time office workers at increased risk for cardiovascular and metabolic morbidity and mortality. Thus, there is a critical need for effective workplace physical activity interventions. MapTrek is a mobile health platform that gamifies Fitbit use for the purpose of promoting physical activity. The purpose of this study was to test the efficacy of MapTrek for increasing daily steps and moderate‐intensity steps over 10 weeks in a sample of sedentary office workers.
Methods and Results
Participants included 146 full‐time sedentary office workers aged 21 to 65 who reported sitting at least 75% of their workday. Each participant received a Fitbit Zip to wear daily throughout the intervention. Participants were randomized to either a: (1) Fitbit‐only group or 2) Fitbit + MapTrek group. Physical activity outcomes and intervention compliance were measured with the Fitbit activity monitor. The Fitbit + MapTrek group significantly increased daily steps (+2092 steps per day) and active minutes (+11.2 min/day) compared to the Fitbit‐only arm, but, on average, participants’ steps declined during the study period.
Conclusions
MapTrek is an effective approach for increasing physical activity at a clinically meaningful level in sedentary office workers, but as with accelerometer use alone, the effect decreases over time.
Clinical Trial Registration
URL: https://www.clinicaltrials.gov. Unique identifier: NCT03109535.
Keywords: intervention, lifestyle, physical exercise
Subject Categories: Exercise, Lifestyle, Primary Prevention
Clinical Perspective
What Is New?
We demonstrated that our mobile health (mHealth) platform, combined with a wearable activity monitor, significantly increased physical activity adoption rates of sedentary office workers over a wearable activity monitor alone.
What Are the Clinical Implications?
These findings suggest that wearable activity monitors alone may not be sufficient to increase physical activity levels of sedentary adults.
Combining wearables with theory‐based mHealth technologies may be effective at increasing physical activity levels, but additional research is needed to determine whether such approaches can instill long‐term behavior changes.
Introduction
Participating in regular physical activity is effective for the primary and secondary prevention of several chronic diseases including cardiovascular disease, diabetes mellitus, cancer, obesity, hypertension, osteoporosis, and depression.1 The Federal Physical Activity Guidelines for Americans recommend that healthy adults engage in 150 minutes of moderate‐ to vigorous‐intensity physical activity each week to achieve health benefit.2 Unfortunately, studies using objective measures of physical activity (accelerometers) suggest that <25% of US adults are achieving 30 minutes of moderate‐ to vigorous‐intensity physical activity per day.3, 4 Such low levels of physical activity represent a significant public health problem as recent estimates suggest that 9% of all deaths worldwide are directly caused by physical inactivity.5
Total physical activity levels have declined among US adults over the past 50 years, and declines in work‐related physical activity are a major contributor.6 The work environment has become increasingly sedentary with the rise of labor‐saving technologies such as the desktop computer. Sedentary jobs have increased 83% since 1950; furthermore, highly sedentary service jobs now account for 43% of all US jobs.6 Employees working in office jobs spend more than 89% of their time sitting, placing them at increased risk for inactivity‐related pathologies and in need of interventions targeting hazardous sedentary work time.
In an effort to promote the health of employees, worksites and researchers have traditionally developed programs that encourage employees to exercise during times outside of their normal working hours. Such programs have suffered from high dropout rates and have been largely unsuccessful for promoting sustained behavior changes.7 These findings are not surprising given that the most common self‐reported barriers to engaging in structured exercise include lack of time, lack of motivation, inconvenience, and not finding exercise to be enjoyable.8 Thus, there is a need for low‐cost, sustainable approaches that motivate sedentary working adults to build regular physical activity into their usual routine, both at work and outside the workplace.
The rise of inexpensive, wearable activity monitors and mobile phone applications has now made it easy to both monitor daily physical activity levels and intervene for the purpose of increasing physical activity. There is evidence that just wearing activity monitors has been associated with significant increases in daily steps.9 However, recent research suggests that both activity monitors and apps are typically designed based on behavior change techniques (ie, self‐monitoring, goal setting, feedback) that are limited in their ability to engage users and promote sustained increases in physical activity.10 The development of mobile‐based programs designed to encourage more walking is a worthwhile pursuit given the demonstrated cardioprotective benefits of regular walking.11 Walking is a familiar activity most able‐bodied adults can complete throughout the day and is the most commonly reported type of physical activity among adults.12
In recent years, games have been used in a variety of settings to motivate and change health behaviors. Games not only provide performance feedback to the user but can also provide incentives for achieving goals in a context that is fun, intrinsically rewarding, and easy to understand. “Exergames,” or active video games that require physical movement while playing, have been shown to result in significant increases in energy expenditure.13 However, many exergames require expensive equipment and must be played inside the home, limiting their use in real‐world settings. Recent games have been developed that exploit motivating social factors (eg, social interactions, social comparison, peer support, competition) and have potential for promoting physical activity in real‐world settings such as the worksite.14 Social interaction features have been identified as a key influence of players’ initial and sustained interest in games15 and as a mediator for behavior change.16 Moreover, multiplayer games generally lead to greater energy expenditure than solo games, and even “virtual friends” (ie, competing against strangers) can lead to increased fitness.17
To specifically address the most commonly reported barriers to engaging in regular physical activity (time and motivation), our interdisciplinary research group created MapTrek, a low‐cost mobile phone–based walking game for the purpose of promoting physical activity in a fun and interactive format. MapTrek leverages and gamifies a widely used physical activity monitor (Fitbit) to both track users’ physical activity and motivate users to be more active on a daily basis. MapTrek places users in a series of virtual walking races that take place in any number of interesting locations around the world. MapTrek also sends users automated game messages via text message that are based on the user's Fitbit‐recorded activity.
Our overall objective was to develop a mobile game that encourages sedentary workers to walk more throughout the day and to maintain that behavior change over time. The purpose of the present study was to test the efficacy of MapTrek for increasing daily physical activity levels compared to a control group in a sample of sedentary office workers. We hypothesized that the MapTrek group would increase both daily steps and the total number of active minutes (minutes with 100+ steps) compared to a non‐MapTrek control group.
Methods
Subjects and Design
We recruited healthy adults who reported working full‐time in a primarily sedentary job. Participants were recruited via an e‐mail advertisement sent to all employees of a large university. The advertisement included a link to an online eligibility survey. Exclusion criteria included (1) age <18 or >65 years, (2) pregnancy or planned pregnancy, (3) not owning a smartphone, (4) not fluent in English, (5) any reported contraindications to engaging in physical activity, (6) not working full‐time (minimum of 35 hours per week), and (7) not working in a sedentary job (reporting sitting ≥75% of workday). Research staff contacted interested and eligible employees to schedule a baseline visit. Experimental protocols were approved by the Human Subjects Office Institutional Review Board, and voluntary written informed consent was obtained from each participant. The data that support the findings of this study are available from the corresponding author upon reasonable request.
The sample size was based on a meta‐analysis of previous pedometer‐based studies,18 which found a standard deviation of about 2000 steps per day between the average steps taken by subjects. We assumed that the within‐subject interday standard deviation would be similar, at 2000 steps per day. We assumed that within a subject, days are independent and identically distributed. In other words, the steps taken on 1 day have no impact on the steps taken on the following day and the distribution from day‐to‐day does not change. We used these assumptions to produce simulated data to conduct a power analysis. We sought to have 80% power to detect a difference between the groups of 1250 steps/day with an α of 0.05 (minimum detectable ▵0=1250). We selected the 1250 steps per day threshold as a conservative estimate based on previous research that found adding 1385 steps per day resulted in significant reductions in multiple cardiometabolic risk factors.19 Based on previous interventions, however, it seems plausible that the effect of an intervention like MapTrek will be closer to 1250 steps per day.20 For ▵0=1250, a sample size of 60 per group would have an estimated power of 0.831 (95% confidence interval [CI], 0.817–0.845). To account for the potential for dropouts, we increased our sample by 25% to 75 per arm.
A total of 784 people completed the screening survey, of which 653 were identified as eligible (Figure 1). Interested participants were contacted in the order they completed the eligibility survey and asked to attend a face‐to‐face baseline orientation visit. A total of 146 participants were found eligible. All baseline visits were conducted in September 2016. Participants were consented immediately upon arrival for their baseline visit and were provided a Fitbit Zip activity monitor to wear on the hip. Participants were then randomized (1:1 ratio) to 1 of 2 groups: (1) Fitbit‐only group (FB) or (2) Fitbit + MapTrek (MT) group. The investigators used sequentially numbered envelopes to implement the random allocation sequence. Two research assistants who enrolled all participants asked participants to select 1 of 2 sealed envelopes, giving them an equal chance (50%) of being selected for the intervention or control group. Following randomization, group responsibilities were explained.
Figure 1.
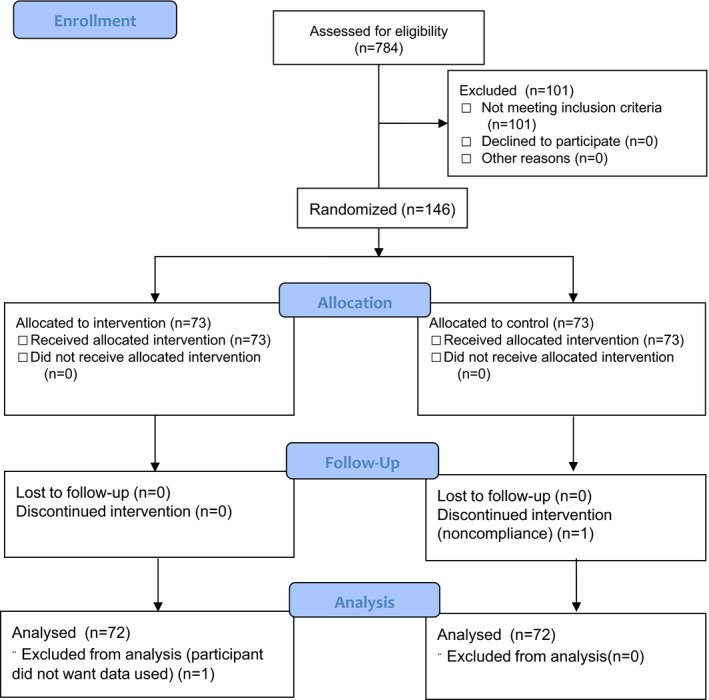
CONSORT flow diagram.
Fitbit‐Only Group
Participants randomized to the FB group were provided a Fitbit Zip activity monitor and were instructed on how to wear the monitor and how to pair and sync the activity monitor to their smartphone. Participants were free to access the Fitbit app at any time throughout the study but did not receive any reminders to do so from the research team. Participants also provided us their cell phone number and access to their Fitbit account, which allowed us to track their daily physical activity levels via our MapTrek research platform. Specifically, this platform accesses Fitbit data through Fitbit's application programming interface, and the data are then made available to our team on a minute‐by‐minute frequency. For this study, the research platform was used to analyze each user's Fitbit data and send participants text message reminders to wear their Fitbit on days following nonwear days (eg, “You didn't record any steps yesterday. Please remember to wear your Fitbit today.”) The reminder system was used to help ensure that both groups wore their monitors equally throughout the study.
Fitbit + MapTrek Group
Participants randomized to the MapTrek arm received the same Fitbit Zip and assistance setting up their Fitbit account as the FB group. MT participants were also provided access to the full MapTrek mobile health (mHealth) game. The MapTrek participant interface is a platform‐independent web app (no special installation needed). MapTrek automatically sends and receives bidirectional text messages to participants via a commercial web‐to‐short message service gateway (http://www.twilio.com/). As part of the game, users are entered into weekly virtual walking races (Sunday through Saturday), which follow a predetermined route that is displayed on Google Maps. At the beginning of each week, users received a message that a new race was about to start. Because the game leverages Google Maps, participants are able to see where they are on the route in real time via the Google Street View feature. Each participant is represented in the game by a stick figure on the map that advances along the weekly race route based on data obtained via the participant's Fitbit. Therefore, the more active the participant is in real life, the faster they move along the virtual race. The participant's position is automatically updated each time their Fitbit syncs to their phone or personal computer.
Each week, MT participants were placed into 1 of 6 leagues (≈10 people per league), which were determined based on each individual's average daily steps during the previous week. Participants were divided into sextiles to determine each individual's weekly league placement. The purpose of the activity‐based leagues was to maintain strong competition among similarly active participants and minimize discouragement.21 The competition‐based leagues were grounded in the cognitive evaluation theory, which states that intrinsic motivation is based on an individual's need for competence, achievement, and self‐determination.22 The theory also suggests that informational aspects of external events (eg, winning a race or losing a race) can both enhance (when positive) or diminish (when negative) the individual's intrinsic motivation.23 Competitiveness has also been positively associated with regular exercise.24 Therefore, individuals were place into activity‐based leagues to give each participant an equal chance of winning the weekly race, which could subsequently boost the individuals’ sense of achievement. We also hypothesized that narrowly losing a theoretically winnable race (ie, competence) might also result in increased effort from that individual during the next weekly race. To minimize any instance of discouragement from being placed in a less active league, participants were not informed of their league placement. Rather, participants were able to view only the step achievements of those participants placed into their weekly league. Each week, leagues were entered into a virtual race in a specific location in the world (eg, Appalachian Trail). The game collected real‐time step counts via Fitbit and used those data to move the user's avatar along the race path. At any point, each participant could view his or her real‐time location on the game leaderboard and route map as well as on Google Street View (Figure 2). The game also displayed each user's average number of steps taken per day, position or “place” on the trail, bonus steps achieved, and total steps accumulated each week. This constant display was developed to promote self‐monitoring of physical activity behavior, which is a construct of the social cognitive theory and has been shown to be an important predictor of physical activity adoption.25
Figure 2.
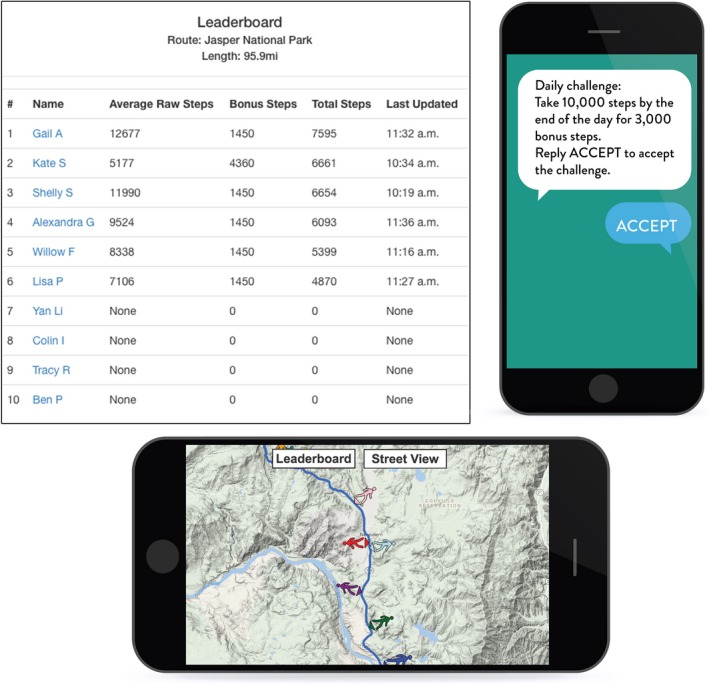
Screenshots of MapTrek leaderboard, game board, and street view.
Each morning, participants received a text message tailored to the individual's activity level and progress along the route. The daily messages informed the user of his or her place in the game, average daily steps, and a daily activity challenge (if implemented). The daily challenge messages were designed to add a fun and motivational aspect to the game, offering bonus steps if the participant chose to accept and met the challenge. Step challenges were determined by the user's typical daily physical activity behaviors. Typically, a 20% increase in steps was implemented with a minimum of 1500 steps. For example, if a participant averaged around 8000 steps per day the previous week, the daily challenge on Monday may have been to take 9600 steps. If the participant met the goal, they were rewarded with a predetermined number of bonus steps (+500 steps). However, if the participant did not meet the goal, the participant had that same amount deducted from his or her daily steps (−500 steps). This game feature was implemented based on risk‐taking theory, which suggests that people are more likely to engage in a challenge if they believe they have a realistic chance of receiving a payoff.26, 27 The individual could also choose not to accept the challenge.
Participants were also able to view and track their virtual progress along the route via Google Maps and the daily link sent via text, which is also consistent with the theoretical construct of self‐monitoring.28 Upon syncing the Fitbit to their smartphone and refreshing the MapTrek screen, participants could view their own personal updated data and progress. Participants’ raw daily step counts (sans bonus steps) were also viewable in real time by the research team via the Fitbit application programming interface.
Measures
The primary outcomes for the study were average daily steps and active minutes (minutes with ≥100 steps per minute recorded) as measured objectively for 7 consecutive days by the Fitbit Zip activity monitor. The Fitbit Zip is a small (35.6×28.9×9.6 mm) triaxial accelerometer‐based activity monitor that estimates daily steps taken at the minute‐to‐minute level. A single replaceable battery provides 4 to 6 months of use. The Fitbit Zip has been demonstrated as a valid measure of daily steps when compared to the Actigraph GT3X+ (r=0.99; intraclass correlation=0.98) in free living conditions.29 Through the Fitbit application programming interface and our custom‐built texting platform, our team was able to access each user's physical activity data on a minute‐by‐minute frequency each day they wore the monitor for the entire 10‐week intervention. Participants were instructed to wear the monitor during all waking hours (except time spent bathing or swimming) for 10 consecutive weeks. Participants’ activity monitor wear time (total daily minutes with at least 1 step recorded), steps, and active minutes were collected daily over the duration of the 10‐week intervention. Only days that had at least 1 step recorded were included in the final analysis. Additionally, only raw steps (no bonus steps) were included in the final analysis.
At baseline, each participant's height and weight were measured. Height was measured to the nearest 0.5 cm using a professional‐grade height rod (Seca 769, Hanover, MD). Weight, fat mass, and lean mass were measured to the nearest 0.1 kg using a multifrequency bioelectrical impedance analyzer (InBody 720, BioSpace Inc, Cerritos, CA), which has demonstrated excellent reliability (coefficient of variation=1.8%)30 and strong criterion validity when compared to dual‐energy x‐ray absorptiometry among obese adults (intraclass correlation=0.83 for fat mass; intraclass correlation=0.90 for fat‐free mass)31 and healthy adults (r=0.80–0.91 for body composition).30 Participants completed an online questionnaire that assessed general demographics (eg, age, sex, ethnicity, education, race, income, and marital status), and occupation category; Table 1). All measures collected at baseline were performed in a controlled laboratory by 1 of 2 staff members, who were blinded to participants’ group assignment.
Following the 10‐week intervention, MT participants were asked to also complete an additional process‐evaluation survey that asked what (if anything) they most liked about the game, what barriers (if any) prevented them from playing the game, and what improvements (if any) they would recommend for the game. Participants were asked to use a Likert scale ranging from strongly disagree to strongly agree to respond to statements regarding whether (1) the game was fun; (2) the game was easy to play; (3) the game motivated them to be more active; (4) they were able to play the game in their spare time; (5) they felt more supported to be physically active due to playing the game; (6) they would like to have continued access to the game; and (7) the game motivated them to keep wearing their Fitbit.
Statistical Analysis
Because we have clustering within subject, we used mixed‐effect models for continuous outcomes. Mixed‐effect models are commonly used to analyze longitudinal outcomes.32 Specifically, mixed‐effect models incorporate a random effect, typically an intercept, for each subject. While there is a population‐level average intercept, the subject‐specific deviations from the population intercept follow a normal distribution with a mean of 0. The only parameter that needs to be estimated in this context is the standard error for the distribution that describes the random effects. A similar result may be obtained using subject‐level fixed effects to estimate the subject‐specific mean; however, that approach would require estimation of (n‐1) coefficients compared to the 1 coefficient required using random effects.
For our compliance outcome, because it is bounded by 0 and 1, we used generalized estimating equations with a logistic link and an exchangeable correlation structure, grouped by subject.
We modeled the 3 outcomes of interest (daily step counts, daily number of active minutes, and compliance) in 3 ways: We considered the outcomes during the entire baseline period, the entire intervention period, and in a time‐varying model.
In the baseline/intervention period models, we regressed the outcome of interest on an indicator of group (MT versus FB) and a random intercept by subject using only the data from baseline or from the intervention periods. This is analogous to performing a 2‐sample t‐test but accounts for the between‐subject differences and within‐subject clustering.
The time‐varying model allowed for different levels and slopes for MT and FB during the baseline period and different levels and slopes for MT and FB during the intervention period. This was accomplished by the inclusion of the group membership variable, relative days, an indicator for whether the intervention is in effect, interactions among the group membership and days, group membership and intervention indicator and a 3‐way interaction between group membership, days and the intervention indicator. The resulting 8 effects estimated by the model describe any differences between MT and FB at baseline, the overall effect of the intervention, and the differential effect of the intervention on the MT group and the rates of decay of step counts for both MT and FB groups.
Differences and 95% CI between the intervention‐phase slopes (composite of several interaction terms) were calculated using the estimated coefficients for the fixed effects in the full model and the variance‐covariance matrix for the relevant coefficients. We estimated 95% CI for the composite coefficients by making 10 000 draws from a multivariate normal distribution centered on the point estimated with the variance‐covariance derived from the model.
All analyses were performed using R 3.3.233 and the lme4 package.34
Results
A total of 144 participants were randomized to 1 of 2 groups: FB (N=72); or MT (N=72). Final analyses were completed on all 144 participants. Baseline group characteristics are presented in Table 1. Overall, participants were middle‐aged, mostly female, mostly white, and non‐Hispanic. No significant between‐group differences were observed for baseline characteristics (Table 1). Throughout the course of the study, a total of 64 weekly MapTrek races took place, with the group sizes ranging from 5 to 13 participants (mean=10.3, standard deviation=1.3).
Table 1.
Baseline Demographic Data From Demographic Survey Analyzed Via Independent 2‐Sample t Test
| Fitbit‐Only Group (N=72) | Fitbit+MapTrek Group (N=72) | P Value | |
|---|---|---|---|
| Age, y | 40.3 (11.1) | 40.6 (11.7) | 0.88 |
| Female, % | 73.6 | 79.2 | 0.44 |
| Height, cm | 167.3 (8.3) | 169.4 (8.3) | 0.14 |
| Weight, kg | 82.5 (22.9) | 85.6 (19.6) | 0.38 |
| Body mass index | 29.5 (7.4) | 29.9 (6.6) | 0.75 |
| Body fat, % | 36.0 (10.6) | 36.2 (9.8) | 0.93 |
| Non‐Hispanic, % | 94.4 | 94.4 | 1.00 |
| White, % | 90.3 | 91.7 | 0.77 |
| College graduate, % | 84.7 | 83.3 | 0.82 |
A P value of 0.05 was considered significant.
Average daily step counts and active minutes are shown by group and days relative to the start of the intervention in Figure 3. There is a sudden increase in the number of steps taken among those in the MT group at the start of the intervention.
Figure 3.
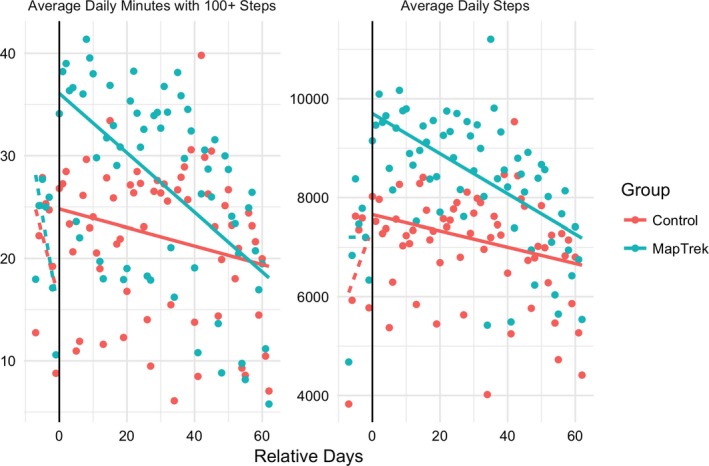
Average daily minutes with 100+ steps and average daily steps by group over the course of the intervention. Baseline is represented in data point to the left of the horizontal line marked “0,” and intervention days are to the right.
After accounting for subject‐specific differences in the mixed‐effect model, we found no difference between the groups during the 1‐week baseline in either daily total steps (MT versus FB, +562; 95% CI, −358–1452) or daily active minutes (MT versus FB, +1.1; 95% −4.1–6.1). However, after the intervention started (relative days 0–62), there was a difference between the groups. Relative to FB, MT players took an average of 1455 (95% CI, 548–2361) more steps per day. FB participants also completed an additional 5.5 active minutes (95% CI, −0.2 to 11.2), although this was not significant.
The results for the daily step counts with a time‐varying effect are shown in Table 2. While there are 8 parameters and several interactions, including a 3‐way interaction, many of the variables are 0, reducing the complexity of the equation. For instance, for those in the FB group, the MT variable is 0, and any interaction involving MT can be ignored. During the baseline period, the total number of steps taken was very similar between the groups (MT effect=−66.8; 95% CI, −1476 to 1336). However, once the intervention started, there was an immediate increase of 2183 (95% CI, 992–3344) steps per day in MT above and beyond the effect observed in the controls. After the start of the intervention, both groups exhibited regression to the mean with a decreasing number of steps taken, on average, with each day from the start of the intervention. The decay was significantly faster in MT, at a loss of 44.7 (95% CI, −51.0 to −38.0) steps per day each day since the start of the intervention compared to 24.3 steps/day (95% CI, −32.4 to −17.3).
Table 2.
Results for Model Predicting Number of Steps Taken per Day
| Parameter | Estimate | Std. Error | 95% LB | 95% UB |
|---|---|---|---|---|
| Intercept | 7123.8 | 516.9 | 6097.2 | 8145.2 |
| MapTreka | −66.8 | 718.9 | −1475.6 | 1336.2 |
| Interventionb | 324.2 | 430.8 | −529.7 | 1183.7 |
| Daysc | 150.6 | 95.3 | −36.5 | 338.9 |
| MT×Interventiond | 2182.6 | 597.4 | 991.7 | 3344.2 |
| MT×Dayse | −144.7 | 133.7 | −403.4 | 118.1 |
| Days×Interventionf | −175.4 | 95.4 | −364.3 | 12.0 |
| MT×Intervention×Daysg | 125.0 | 133.8 | −138.6 | 384.1 |
Estimates are in number of steps taken per day.
LB indicates Lower Bound; MT, MapTrek; UB, Upper Bound.
The MT indicates MapTrek variable is an indicator for intervention membership.
The Intervention variable is an indicator for the intervention period for both intervention and control subjects.
The Days variable is the number of days since the intervention period started (−7 to 62).
The MT×Intervention variable shows the effect of MapTrek after the intervention began.
The MT×Days variable gives the effect of MapTrek over time.
The Days×Intervention variable gives the effect over time after the intervention started.
The MT×Intervention×Days variable given the effect of MapTrek over time after the intervention started.
Similarly, there was an increase in active minutes among MT at the start of the intervention, Table 3. The interpretation of the model is similar for Model 1 but instead of using steps per day as the response, Model 2 is focused on the number of minutes when subjects took at least 100 steps (eg, active minutes). At baseline, the number of active minutes did not vary between the groups (MT versus FB, −2.1; 95% CI, −10.3 to 6.0). However, immediately after the start of the intervention, the active minutes per day increased by 12.8 (95% CI, 6.3–19.3) minutes in MT above and beyond the changes in FB. After the intervention started, both groups exhibited regression to the mean, with the average number of active minutes decreasing by 0.3 (95% CI, −0.33 to −0.25) minutes per day among MT and 0.1 (95% CI, −0.17 to −0.08) minutes per day among FB subjects.
Table 3.
Results for Model Predicting the Number of Active Minutes per Day
| Parameter | Estimate | Std. Error | 95% LB | 95% UB |
|---|---|---|---|---|
| Intercept | 15.0 | 3.0 | 9.0 | 20.9 |
| MapTreka | −2.1 | 4.2 | −10.3 | 6.0 |
| Interventionb | 9.4 | 2.4 | 4.6 | 14.1 |
| Daysc | −1.5 | 0.5 | −2.2 | 0.7 |
| MT×Interventiond | 12.8 | 3.4 | 6.3 | 19.3 |
| MT×Dayse | −0.7 | 0.8 | −2.2 | 0.7 |
| Days×Interventionf | 1.4 | 0.5 | 0.3 | 2.4 |
| MT×Intervention×Daysg | 0.6 | 0.8 | −0.9 | 2.0 |
Estimates are in number of minutes with ≥100 steps per day.
LB indicates Lower Bound; MT, MapTrek; UB, Upper Bound.
The MT indicates MapTrek variable is an indicator for intervention membership.
The Intervention variable is an indicator for the intervention period for both intervention and control subjects.
The Days variable is the number of days since the intervention period started (−7 to 62).
The MT×Intervention variable shows the effect of MapTrek after the intervention began.
The MT×Days variable gives the effect of MapTrek over time.
The Days×Intervention variable gives the effect over time after the intervention started.
The MT×Intervention×Days variable given the effect of MapTrek over time after the intervention started.
Compliance rates varied between the groups and over time (Figure 4. At baseline, after accounting for within‐subject clustering, there were data for 88.7% (95% CI, 84.1–93.4) of the subject days in the FB arm. Compliance was 5.0 percentage points higher in MT, although this effect was not significant (95% CI, −1.4 to 11.5). After the start of the intervention, compliance was only 64.6% (95% CI, 58.2–71.0) among those in the FB arm, and the MT arm compliance was 16.5 percentage points higher (95% CI, 7.6–25.4).
Figure 4.
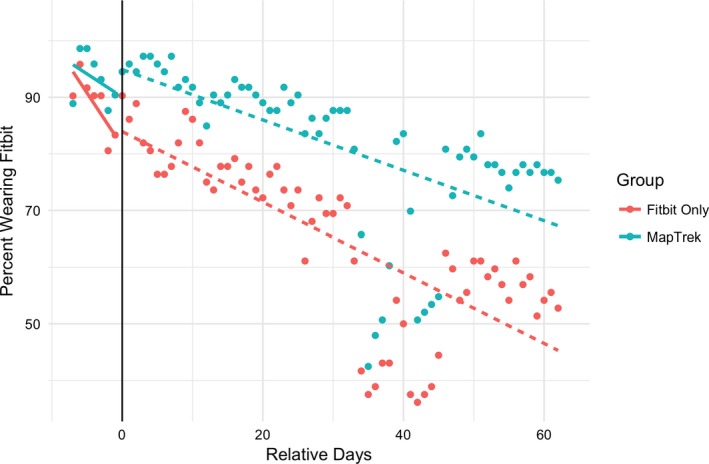
Compliance rates by group over the course of the intervention. The sudden decrease between days 35 and 45 was due to the study suspending messaging and games for a week following an error resulting in inadvertently messaging the participants repeatedly.
Compliance rates were time varying (see Figure 4 and Table 4). The odds of compliance for the MT group compared to the control group were 1.85, but these odds were not significantly different than 1 (95% CI, 0.67–5.16). However, the odds of compliance fell significantly during the preintervention period (odds ratio, 0.80; 95% CI, 0.68–0.95), and continued to fall during the intervention period.
Table 4.
Results for Generalized Estimating Equation Model Predicting the Probability of Wearing a Fitbit
| Variable | Odds Ratio | 95% LB | 95% UB |
|---|---|---|---|
| MTa | 1.85 | 0.67 | 5.16 |
| Interventionb | 1.26 | 0.67 | 2.34 |
| Daysc | 0.80 | 0.68 | 0.95 |
| MT×Daysd | 0.99 | 0.74 | 1.33 |
| MT×Interventione | 1.43 | 0.50 | 4.08 |
| Days×Interventionf | 1.21 | 1.03 | 1.44 |
| MT×Days×Interventiong | 1.01 | 0.75 | 1.34 |
LB indicates Lower Bound; MT, MapTrek; UB, Upper Bound.
The MapTrek variable is an indicator for intervention membership.
The Intervention variable is an indicator for the intervention period for both intervention and control subjects.
The Days variable is the number of days since the intervention period started (−7 to 62).
The MT×Days variable gives the effect of MapTrek over time.
The MT×Intervention variable shows the effect of MapTrek after the intervention began.
The Days×Intervention variable gives the effect over time after the intervention started.
The MT×Days×Intervention variable gives the effect of MapTrek over time after the intervention started.
A total of 72 MT participants completed the postintervention process‐evaluation survey (Figure 5. The majority of participants indicated that they enjoyed playing MapTrek; they found it easy to play; they could play it in their spare time; MapTrek made them feel more supported in physical activity; and it made them more likely to wear their Fitbit and be active.
Figure 5.
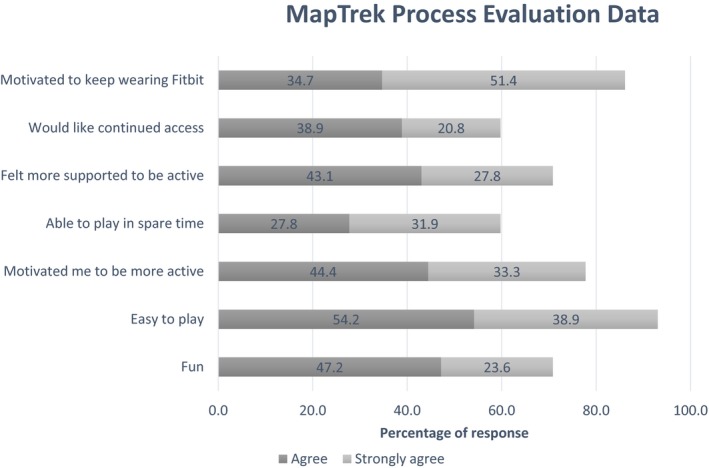
Process evaluation data summary (N=72).
Discussion
The primary findings from this study suggest that the MapTrek game was effective at dramatically increasing daily step counts initially. Immediately after the start of the intervention, MT players took an average of 2183 (95% CI, 992–3344) more steps per day than controls. An increase of 2000 steps per day is clinically meaningful as it has been associated with a 10% relative reduction in long‐term incidence of cardiovascular disease.35 Further, the MT group was walking an average of 7100 steps per day upon enrollment, which would place them in the “low active” step index before receiving the intervention.36 An increase of 2000 steps per day would place the majority of participants into the “somewhat active” step index. This is important given that the greatest physical activity–induced health benefits are realized by those who are least active.37 While this effect does not persist indefinitely, and the MT group appears to have a more rapidly decreasing step count with time, even 9 weeks after the start of the intervention, the average MapTrek player took 900 more steps per day than the average subject randomized to the FB group.
The MT group also significantly increased the number of active minutes, suggesting that MapTrek was effective for both promoting more steps but also more purposeful steps taken at a moderate intensity.38 According to the model described in Table 3, at the start of the intervention, the FB group had an average of 24.4 active minutes per day. The MT group spent an additional 12.8 (95% CI, 6.3–19.3) minutes per day active or a total of 37.2 minutes according to the model. The additional 12.8 minutes per day adds 89.6 minutes per week to the 170.8 minutes the FB subjects spent active. The MT average of 260.4 active minutes per week is 73% more than the recommended Physical Activity Guidelines for Americans.2 A 2011 study by Wen and colleagues,39 which found that achieving 92 minutes per week of moderate‐intensity aerobic activity was associated with a 14% (95% CI, 9%–19%) reduction in all‐cause mortality and an additional 3 years in life expectancy compared to controls who exercised for <1 hour per week. Additionally, for each additional 15 minutes spent above the 92 minute per week threshold, there was a further 4% (95% CI, 2.5–7.0) reduction in all‐cause mortality.39
While we were not able to identify other studies that have tested the effect of gamifying pedometer‐measured step counts, our findings can be compared with a few recent mHealth interventions that have incorporated pedometers and text messages to increase physical activity. The mActive study tested a fully automated mHealth intervention that combined the FitBug Orb wearable accelerometer with physician‐written, theory‐based smart text messages sent 3 times per day against a control group that received only the FitBug Orb.40 When participants received the text messages, they significantly increased their steps by 2534 steps per day (95% CI, 1318–3750).40 However, when the mHealth intervention did not include the text messaging, activity levels were not significantly different between the 2 groups. The authors concluded that the texting aspect of the intervention was crucial for increasing daily activity. It is notable that this intervention was only 5 weeks in duration and was performed in a sample of individuals recruited from a cardiovascular disease rehabilitation center, a population considerably different than the sedentary office workers enrolled in our study.40
The use of the Fitbit combined with our innovative platform that utilizes the Fitbit application programming interface allowed us to measure steps on a daily and minute‐by‐minute basis, which allowed for some novel examinations of trends in physical activity over the course of the intervention. For example, following the initial 2200 step per day increase in daily steps, the MapTrek group demonstrated a progressive decay of daily steps back to baseline levels over the course of the intervention. This finding suggests that more research is needed to identify improvements needed to maintain participant engagement. Data collected from the process evaluation data suggest that 8 of 48 respondents (17%) reported Fitbit battery issues were the primary barrier to playing MapTrek. Commonly recommended improvements for the game included making the game more interactive, sending more reminder text messages during the day to sync the Fitbit, sending rewarding text messages for completing a challenge, and providing a better explanation of the game rules. Each of these factors should be considered in future iterations of the MapTrek game.
The process evaluation data also suggested that participants thought the game was fun and easy to play. Importantly, participants reported that it motivated them to be more active and wear their Fitbit more. This report was verified with the Fitbit data, which indicate that MT participants were more likely than FB participants to wear their Fitbit daily. However, this raises the question of whether the increased wear time explained the observed difference in steps between the 2 groups. It is possible that more compliant participants are fundamentally different than less compliant participants and are just more active. Indeed, in an unadjusted analysis, there was a moderately strong correlation (r=0.34, 95% CI, 0.19–0.48) between average daily step counts and the percentage of days when the Fitbit was worn. However, when we accounted for percent compliance within the daily step counts analysis, the effect of MapTrek slightly decreased from 2182.6 steps per day to 2119 steps per day (95% CI, 1038.0–3368.5). Therefore, because compliance did not have a large effect on MapTrek effectiveness, we believe this provides more confidence that the MapTrek intervention was effective at increasing physical activity in this study (model not shown).
The granular‐level physical activity data collected in this study can also be used to identify unique patterns of physical activity completed over the course of a given day. We were able to examine bouts of sedentary behavior (consecutive minutes with 0 steps recorded) on a minute‐by‐minute level. The average longest sedentary bout between 8 am and 8 pm during baseline in the FB group was 139.1 (95% CI, 106.2–172.4) minutes per day in the FB arm and not different among players of MT (MT versus FB, −5.4; 95% CI, 50.8‐minute decrease to 39.7‐minute increase). However, immediately after the start of the game, there was a 26.6‐minute decrease (95% CI, 70.9‐minute decrease to 17.3‐minute increase) in the mean longest sedentary time among those randomized to MT compared to controls (data not shown). This information provides further context on how physical activity and sedentary behavior patterns differed between these 2 groups. Future studies could use these data to further enhance the efficacy of the MapTrek intervention by individualizing specific activity challenges.
Consistent with many other mobile phone–based applications used in research41 we experienced a technical barrier that could have affected the findings. During week 6 of the intervention, a bug with our platform occurred that resulted in MT participants receiving a high volume of text messages on a single day (due to the change from daylight savings to standard time). Subsequently, we stopped sending messages for 1 week and then resumed. This had a significant impact on participants’ Fitbit compliance rates during week 6 (see Figure 4). However, once the intervention resumed, compliance rates appear to have returned to prebug levels. In a sensitivity analysis considering only the data collected before the bug, the effect of MapTrek was +2071 steps per day (95% CI, 917–3216), a difference of 112 steps per day from the model using all of the data. These estimates (2071 steps per day versus 2183 steps per day) are clinically identical, and their 95% CIs both exclude 0 and include the alternative estimate. As a result, the interpretation of the data collected until the bug occurred and the entire data set are functionally identical.
Other limitations to this study include the relatively short duration and a fairly homogenous sample. Participants were mostly white, non‐Hispanic, middle‐class women; thus, the generalizability of the findings to other populations is limited.
The study also had many strengths. This study tested a novel intervention that combined gamification of a widely used physical activity monitor with automated text messages. While several improvements can be made to improve participant engagement, this approach has potential as a low‐cost and scalable approach for promoting physical activity among populations in need. This study also utilized a novel approach for measuring daily physical activity levels at a granular level. This approach allows for the exploration into how the intervention impacts daily and even hourly physical activity patterns over time. This information could be used to inform future improvements to the game for the purpose of promoting increased daily steps and to minimize bouts of sedentary behaviors.
Conclusions
These data suggest the mobile health MapTrek game yielded clinically significant increases in daily physical activity among a sample of sedentary office workers. Further research is warranted to promote sustained participant engagement and physical activity changes over time.
Sources of Funding
This study was funded in part by UI Health Ventures at the University of Iowa Hospitals and Clinics; the National Heart, Lung and Blood Institute at the National Institutes of Health, grant # K25HL122305; and the National Institute of Diabetes and Digestive and Kidney Diseases, grant # DK108019‐01A1. The study sponsors did not play a role in the study design; collection, analysis, and interpretation of data; writing the report; or the decision to submit the report for publication.
Disclosures
None.
Acknowledgments
We thank Sarah Coe and Asma Mumtaz for their contributions to the study. The research presented in this paper is that of the authors and does not reflect the official policy of the funding agency. All contributing authors have made substantial contributions to the manuscript and have provided final approval of the current version to be published and agree to its submission.
(J Am Heart Assoc. 2018;7:e007735 DOI: 10.1161/JAHA.117.007735.)
This article was handled independently by Elizabeth Jackson, MD, MPH, as a guest editor. The editors had no role in the evaluation of this manuscript or the decision about its acceptance.
References
- 1. Warburton DE, Nicol CW, Bredin SS. Health benefits of physical activity: the evidence. CMAJ. 2006;174:801–809. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Haskell WL, Lee IM, Pate RR, Powell KE, Blair SN, Franklin BA, Macera CA, Heath GW, Thompson PD, Bauman A. Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med Sci Sports Exerc. 2007;39:1423–1434. [DOI] [PubMed] [Google Scholar]
- 3. Troiano RP, Berrigan D, Dodd KW, Masse LC, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc. 2008;40:181–188. [DOI] [PubMed] [Google Scholar]
- 4. Metzger JS, Catellier DJ, Evenson KR, Treuth MS, Rosamond WD, Siega‐Riz AM. Patterns of objectively measured physical activity in the United States. Med Sci Sports Exerc. 2008;40:630–638. [DOI] [PubMed] [Google Scholar]
- 5. Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT; Lancet Physical Activity Series Working Group . Effect of physical inactivity on major non‐communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012;380:219–229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Church TS, Thomas DM, Tudor‐Locke C, Katzmarzyk PT, Earnest CP, Rodarte RQ, Martin CK, Blair SN, Bouchard C. Trends over 5 decades in U.S. occupation‐related physical activity and their associations with obesity. PLoS One. 2011;6:e19657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Conn VS, Hafdahl AR, Cooper PS, Brown LM, Lusk SL. Meta‐analysis of workplace physical activity interventions. Am J Prev Med. 2009;37:330–339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Sallis JF, Hovell MF. Determinants of exercise behavior. Exerc Sport Sci Rev. 1990;18:307–330. [PubMed] [Google Scholar]
- 9. Bravata DM, Smith‐Spangler C, Sundaram V, Gienger AL, Lin N, Lewis R, Stave CD, Olkin I, Sirard JR. Using pedometers to increase physical activity and improve health: a systematic review. JAMA. 2007;298:2296–2304. [DOI] [PubMed] [Google Scholar]
- 10. Lyons EJ, Lewis ZH, Mayrsohn BG, Rowland JL. Behavior change techniques implemented in electronic lifestyle activity monitors: a systematic content analysis. J Med Internet Res. 2014;16:e192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Murtagh EM, Murphy MH, Boone‐Heinonen J. Walking: the first steps in cardiovascular disease prevention. Curr Opin Cardiol. 2010;25:490–496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Eyler AA, Brownson RC, Bacak SJ, Housemann RA. The epidemiology of walking for physical activity in the United States. Med Sci Sports Exerc. 2003;35:1529–1536. [DOI] [PubMed] [Google Scholar]
- 13. Sween J, Wallington SF, Sheppard V, Taylor T, Llanos AA, Adams‐Campbell LL. The role of exergaming in improving physical activity: a review. J Phys Act Health. 2014;11:864–870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Zhang J, Brackbill D, Yang S, Becker J, Herbert N, Centola D. Support or competition? How online social networks increase physical activity: a randomized controlled trial. Prev Med Rep. 2016;4:453–458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Staiano AE, Abraham AA, Calvert SL. Motivating effects of cooperative exergame play for overweight and obese adolescents. J Diabetes Sci Technol. 2012;6:812–819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Lieberman DA, Chamberlin B, Medina E Jr, Franklin BA, Sanner BM, Vafiadis DK; Power of Play: Innovations in Getting Active Summit Planning Committee . The power of play: innovations in Getting Active Summit 2011: a science panel proceedings report from the American Heart Association. Circulation. 2011;123:2507–2516. [DOI] [PubMed] [Google Scholar]
- 17. Feltz DL, Irwin B, Kerr N. Two‐player partnered exergame for obesity prevention: using discrepancy in players’ abilities as a strategy to motivate physical activity. J Diabetes Sci Technol. 2012;6:820–827. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Bohannon RW. Number of pedometer‐assessed steps taken per day by adults: a descriptive meta‐analysis. Phys Ther. 2007;87:1642–1650. [DOI] [PubMed] [Google Scholar]
- 19. Carr LJ, Bartee RT, Dorozynski C, Broomfield JF, Smith ML, Smith DT. Internet‐delivered behavior change program increases physical activity and improves cardiometabolic disease risk factors in sedentary adults: results of a randomized controlled trial. Prev Med. 2008;46:431–438. [DOI] [PubMed] [Google Scholar]
- 20. Althoff T, White RW, Horvitz E. Influence of Pokémon Go on physical activity: study and implications. J Med Internet Res. 2016;18;e315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Locke EA, Latham GP. Building a practically useful theory of goal setting and task motivation: a 35‐year odyssey. Am Psychol. 2002;57:705–717. [DOI] [PubMed] [Google Scholar]
- 22. Deci EL, Ryan RM. Intrinsic Motivation and Self‐Determination. New York: Plenum Press; 1985. [Google Scholar]
- 23. Deci EL, Betley G, Kahle J, Abrams L, Porac J. When trying to win—competition and intrinsic motivation. Pers Soc Psychol Bull. 1981;7:79–83. [Google Scholar]
- 24. Frederick‐Recascino CM, Schuster‐Smith H. Competition and intrinsic motivation in physical activity: a comparison of two groups. J Sport Behav. 2003;26:240–254. [Google Scholar]
- 25. Dzewaltowski DA. Physical activity determinants: a social cognitive approach. Med Sci Sports Exerc. 1994;26:1395–1399. [PubMed] [Google Scholar]
- 26. Atkinson JW. Motivational determinants of risk‐taking behavior. Psychol Rev. 1957;64, Part 1:359–372. [DOI] [PubMed] [Google Scholar]
- 27. Martinez F, Le Floch V, Gaffie B, Villejoubert G. Reports of wins and risk taking: an investigation of the mediating effect of the illusion of control. J Gambl Stud. 2011;27:271–285. [DOI] [PubMed] [Google Scholar]
- 28. Gleeson‐Kreig JM. Self‐monitoring of physical activity: effects on self‐efficacy and behavior in people with type 2 diabetes. Diabetes Educ. 2006;32:69–77. [DOI] [PubMed] [Google Scholar]
- 29. Ferguson T, Rowlands AV, Olds T, Maher C. The validity of consumer‐level, activity monitors in healthy adults worn in free‐living conditions: a cross‐sectional study. Int J Behav Nutr Phys Act. 2015;12:42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Jensky‐Squires NE, Dieli‐Conwright CM, Rossuello A, Erceg DN, McCauley S, Schroeder ET. Validity and reliability of body composition analysers in children and adults. Br J Nutr. 2008;100:859–865. [DOI] [PubMed] [Google Scholar]
- 31. Faria SL, Faria OP, Cardeal MD, Ito MK. Validation study of multi‐frequency bioelectrical impedance with dual‐energy X‐ray absorptiometry among obese patients. Obes Surg. 2014;24:1476–1480. [DOI] [PubMed] [Google Scholar]
- 32. Breslow NE, Clayton DG. Approximate inference in generalized linear mixed models. J Am Stat Assoc. 1993;88:9–25. [Google Scholar]
- 33. R Core Team . R: a language and environment for statistical computing. 2016.
- 34. Bates D, Maechler M, Bolker B, Walker S. Fitting linear mixed‐effects models using lme4. J Stat Softw. 2015;67:1–48. [Google Scholar]
- 35. Yates T, Haffner SM, Schulte PJ, Thomas L, Huffman KM, Bales CW, Califf RM, Holman RR, McMurray JJ, Bethel MA, Tuomilehto J, Davies MJ, Kraus WE. Association between change in daily ambulatory activity and cardiovascular events in people with impaired glucose tolerance (NAVIGATOR trial): a cohort analysis. Lancet. 2014;383:1059–1066. [DOI] [PubMed] [Google Scholar]
- 36. Tudor‐Locke C, Hatano Y, Pangrazi RP, Kang M. Revisiting “how many steps are enough?” Med Sci Sports Exerc. 2008;40:S537–S543. [DOI] [PubMed] [Google Scholar]
- 37. Blair SN, Connelly JC. How much physical activity should we do? The case for moderate amounts and intensities of physical activity. Res Q Exerc Sport. 1996;67:193–205. [DOI] [PubMed] [Google Scholar]
- 38. Rowe DA, Welk GJ, Heil DP, Mahar MT, Kemble CD, Calabro MA, Camenisch K. Stride rate recommendations for moderate‐intensity walking. Med Sci Sports Exerc. 2011;43:312–318. [DOI] [PubMed] [Google Scholar]
- 39. Wen CP, Wai JP, Tsai MK, Yang YC, Cheng TY, Lee MC, Chan HT, Tsao CK, Tsai SP, Wu X. Minimum amount of physical activity for reduced mortality and extended life expectancy: a prospective cohort study. Lancet. 2011;378:1244–1253. [DOI] [PubMed] [Google Scholar]
- 40. Martin SS, Feldman DI, Blumenthal RS, Jones SR, Post WS, McKibben RA, Michos ED, Ndumele CE, Ratchford EV, Coresh J, Blaha MJ. mActive: a randomized clinical trial of an automated mHealth intervention for physical activity promotion. J Am Heart Assoc. 2015;4:e002239 DOI: 10.1161/JAHA.115.002239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Zhang J, Calabrese C, Ding J, Liu M, Zhang B. Advantages and challenges in using mobile apps for field experiments: a systematic review and a case study. Mobile Media Commun. 2017;6:1–18. [Google Scholar]