

Abstract
Background
Mucormycosis (or zygomycosis) is the term for infection caused by fungi of the order Mucorales. Mucoraceae may produce severe disease in susceptible individuals, notably patients with diabetes and leukemia. Rhinocerebral mucormycosis most commonly manifests itself in the setting of poorly controlled diabetes, especially with ketoacidosis.
Case Presentation
A 31-year-old diabetic man presented to the outpatient clinic with the following signs and symptoms: headache, periorbital pain, swelling and loss of vision in the right eye. On physical examination his right eye was red and swollen. There was periorbital cellulitis and the conjunctiva was edematous. KOH preparation of purulent discharge showed broad, ribbonlike, aseptate hyphae when examined under a fluorescence microscope. Cranial MRI showed involvement of the right orbit, thrombosis in cavernous sinus and infiltrates at ethmoid and maxillary sinuses. Mucormycosis was diagnosed based on these findings. Amphotericin B (AmBisome®; 2 mg/kg.d) was initiated after the test doses. Right orbitectomy and right partial maxillectomy were performed; the lesions in ethmoid and maxillary sinuses were removed. The duration of the liposomal amphotericin B therapy was approximately 6 months and the total dose of liposomal amphotericin B used was 32 grams. Liposomal amphotericin B therapy was stopped six months later and oral fluconazole was started.
Conclusions
Although a total surgical debridement of the lesions could not be performed, it is remarkable that regression of the disease could be achieved with medical therapy alone.
Background
Mucormycosis (or zygomycosis) is the term for infection caused by fungi of the order Mucorales [1-4]. Mucoraceae may produce severe disease in susceptible individuals, notably patients with diabetes and leukemia. Rhinocerebral mucormycosis most commonly manifests itself in the setting of poorly controlled diabetes, especially with ketoacidosis. The causative organism in most cases is Rhizopus oryzae. Progression of the disease is usually rapid, although it may become indolent if ketoacidosis resolves. Because of the rapidity with which this disease progresses, prompt and aggressive therapy is essential [5-7]. Since the introduction of combined therapy with amphotericin B and surgery, more than 80% of the patients can be expected to survive [6-8]. Administration of amphotericin B is, however, associated with adverse effects that may prevent maintenance of effective doses [9]. Because of this problem, amphotericin B has been inserted into liposomes. When the drug is administered in this form, adverse effects are less pronounced, even with administration of larger doses [10,11]. Recent work has suggested that the new antifungal triazole, fluconazole may be of benefit in treating zygomycete infection [2,3,12]. We described a case of rhinocerebral mucormycosis which was treated with surgery and a 6 month course of liposomal amphotericin B (a total of 32 gr) followed by a course of fluconazole.
Case report
In August 1998, a 31-year-old diabetic man presented to the outpatient clinic at the Department of Clinical Bacteriology and Infectious Diseases, Istanbul Faculty of Medicine, with the following signs and symptoms: headache, periorbital pain, swelling and loss of vision in the right eye. Two months prior, he had been admitted to another hospital with headache and was diagnosed as paranasal sinusitis. Despite antimicrobial therapy with ampicillin/sulbactam, his condition had worsened i.e, headache became more severe and the aforementioned signs and symptoms related with the right eye appeared. The patient had not been compliant with insulin therapy. At the time of admission, the patient was alert, and oriented. He was afebrile, and his vital signs were stable. On physical examination, his right eye was red and swollen. There was periorbital cellulitis, and the conjunctiva was edematous. There was a purulent discharge coming from the right orbit. Laboratory results were as follows; white blood cells, 9 × 103/mm3 with 86 % neutrophils, 13% lymphocytes; hemoglobin, 12.4 gr/mm3; hematocrit, 36.5 %; plasma glucose, 446 mg/dl; blood urea nitrogen, 44 mg/dl; creatinine, 0.9 mg/dl; serum sodium, 130 mEq/dl; serum potassium, 3.3 mEq/dl; aspartate transaminase, 38 U/L; alanine transaminase, 30 U/L; ESR 98 mm/h; CRP 12 mg/dl. Glycosuria and acetonuria were detected in urinalysis. Other biochemical results were normal. Gram and KOH stain were performed on the exudate obtained from the right eye. It was also inoculated onto blood agar, Mac Conkey agar, Sabouraud agar as it is routinely done. KOH preparation showed broad, ribbonlike, aseptate hyphae when examined under a fluorescence microscope. Cranial MRI showed involvement of the right orbit and optic nerve, thrombosis in cavernous sinus and infiltrates at ethmoid and maxillary sinuses (figure 1). Mucormycosis was diagnosed based on these findings.
Figure 1.
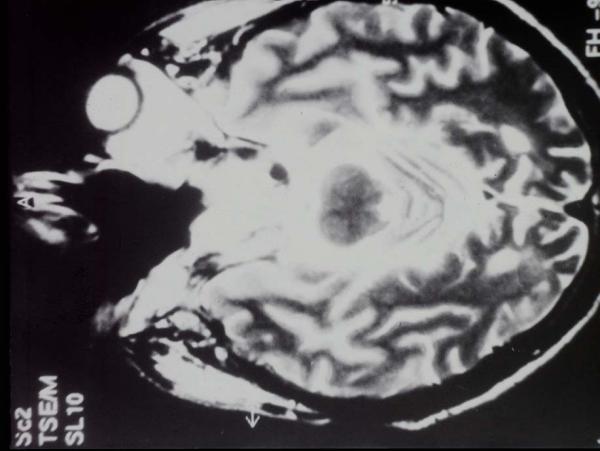
Cranial MRI (transaxial section) at the level of the ethmoid and maxillary sinuses showing contrast enhancement.
The blood glucose levels was controlled with regular insulin. Amphotericin B (1 mg/kg.d) was initiated after the test doses. Seven days later, this regimen was replaced with liposomal amphotericin B (AmBisome®; 2 mg/kg.d) due to increase of creatinine level and side effects such as fever and chills. This resulted in normalization of creatinine level and disappearence of the side effects. After one week of this regimen, the dose of liposomal amphotericin B was raised up to 4 mg/kg/day. During the course of the treatment, the patient was closely monitored for signs and symptoms of drug toxicity, and tests for acute phase reactants (CRP, ESR) were performed.
After neurosurgical and otorhinolaryngological evaluation, the patient apted to receive medical therapy alone. Three months later, the patient was reevaluated. Because there was no regression of the lesions previously noted on MRI, the patient agreed to undergo surgery. Right orbitectomy, and right partial maxillectomy were performed; the lesions in ethmoid and maxillary sinuses were removed. The specimens obtained from sinuses were intraoperatively examined under a fluorescence microscope after treating the samples with KOH or fluorescence conjugated antibody, broad, ribbonlike, and aseptate hyphae were visualized.
Following surgery, liposomal amphotericin B was continued. His blood glucose levels were easily controlled. Periorbital swelling and discharge gradually resolved. One month after the surgery, new infiltrates within ethmoid and maxillary sinuses as well as spread of infiltration to frontal sinuses and infiltration of fatty pad around left orbit were detected. A partial surgical debridment was accomplished. One month after this operation, infiltrations were still present within ethmoid and maxillary sinuses but not around left orbit. Liposomal amphotericin B therapy (4 mg/kg/day) was maintained and two months later, there was not any progression of the disease as indicated by the MRI (Figure 2). Liposomal amphotericin B therapy was stopped in March 1999 (six months later) and oral fluconazole (200 mg/d) was started based on the current medical literature [2,3,12]. Three months after fluconazole therapy was started, the lesion in the right cavernous sinus was partially resolved. Despite the decision to continue the oral fluconazole therapy, the patient refused it. A MRI performed four months after the patient discontinued the treatment did not show progression of the disease (Figure 3).
Figure 2.

Cranial MRI after surgical debridement
Figure 3.
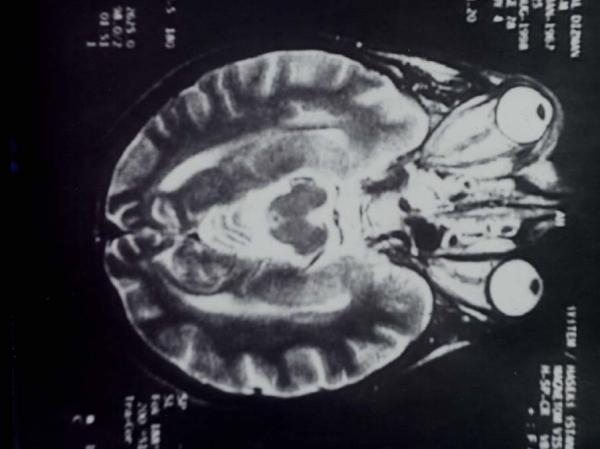
No new contrast enhancement nor progression seen after treatment with fluconazole.
Conclusions
The duration of the therapy was approximately 6 months, and the total dose of liposomal amphotericin B used was 32 grams. Although there has been previous reports on the use of Amphotericin B in various preparations such as lipid complex or colloidal dispersion, with a maximum total dose up to 73.6 grams in the treatment of invasive fungal infections [13-15], our case report is the first one in the literature where liposomal amphotericin B was administered in such a high dose (total 32 grams) over such a long period, i.e, 6 months. No adverse effect was detected during therapy. Creatinine and electrolyte levels (especially potassium) remained within normal ranges.
Although a total surgical debridement of the lesions could not be performed, it is remarkable that regression of the disease could be achieved with medical therapy alone. We could not find any recommendation in the literature on the duration of liposomal amphotericin B and use of fluconazole therapy. The optimal duration of antifungal therapy depends on the response of infection to treatment and success in resolving the underlying predisposing condition.
Competing interests
None declared.
Pre-publication history
The pre-publication history for this paper can be accessed here:
Acknowledgments
Acknowledgements
Written consent was obtained from the patient or their relative for publication of the patient's details.
Contributor Information
Atahan A Çagatay, Email: atayon@yahoo.com.
Serkan S Öncü, Email: serkanoncu@hotmail.com.
Semra S Çalangu, Email: scalangu@superonline.com.
Taner T Yildirmak, Email: taneryildirimak@hotmail.com.
Halit H Özsüt, Email: hailtozsut@superonline.com.
Haluk H Eraksoy, Email: heraksoy@superonline.com.
References
- Rinaldi MG. Zygomycosis: Infect Dis Clin North Am. 1989;3 (1):19–41. [PubMed] [Google Scholar]
- Koçak R, Tetiker T, Koçak M, et al. Fluconazole in the treatment of three cases of mucormycosis. Eur J Clin Microbiol Infect Dis. 1995;14:559–561. doi: 10.1007/BF02113443. [DOI] [PubMed] [Google Scholar]
- Selcen D, Seçmeer G, Aysun S, et al. Mucormycosis In a diabetic child and its treatment with fluconazole: A case report. Turkish J Pdr. 1995;37:165–168. [PubMed] [Google Scholar]
- Maury S, Lebianc T, Feuilhade M, Molina JM, Schaison G. Successful treatment of disseminated mucormycosis with liposomal amphotericin B and surgery in a child with leukemia. Clin Infect Dis. 1998;26:200–202. doi: 10.1086/517067. [DOI] [PubMed] [Google Scholar]
- Sugar AM. Mucormycosis. Clin Infect Dis. 1992;14 (Suppl 1):126–129. doi: 10.1093/clinids/14.supplement_1.s126. [DOI] [PubMed] [Google Scholar]
- Parfrey NA. Improved diagnosis and prognosis of mucormycosis. Medicine. 1986;65:113–123. doi: 10.1097/00005792-198603000-00004. [DOI] [PubMed] [Google Scholar]
- Lim KK, Potts MJ, Warnock DW, et al. Another case report of rhinocerebral mucormycosis treated with liposomal amphotericin B and surgery. Clin Infect Dis. 1994;18:653–654. doi: 10.1093/clinids/18.4.653. [DOI] [PubMed] [Google Scholar]
- Ericsson M, Anniko M, Gustafsson H, et al. A case of chronic progressive rhinocerebral mucormycosis treated with liposomal amphotericin B and surgery. Clin Infect Dis. 1993;16:585–586. doi: 10.1093/clind/16.4.585. [DOI] [PubMed] [Google Scholar]
- Gallis HA, Drew RH, Pickaed WW. Amphotericin B: 30 years of clinical experience. Rev Infect Dis. 1990;12:308–329. doi: 10.1093/clinids/12.2.308. [DOI] [PubMed] [Google Scholar]
- Meunier F. methods for delivery of antifungal agents. Rev Infect Dis. 1989;11 (suppl 7):1605–1612. doi: 10.1093/clinids/11.supplement_7.s1605. [DOI] [PubMed] [Google Scholar]
- Brajtburg J, Powderly WG, Kobayashi GS, Medoff G. Amphotericin B: delivery systems. Antimicrob Agents Chemother. 1990;34:381–384. doi: 10.1128/aac.34.3.381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Funada H, Miyake Y, Kanamori K, et al. Fluconazole therapy for pulmonary mucormycosis complicating acute leukemia. Jpn J Med. 1989;28(2):228–231. doi: 10.2169/internalmedicine1962.28.228. [DOI] [PubMed] [Google Scholar]
- Moses AE, Rahav G, Barenholz Y, et al. Rhinocerebral mucormycosis treated with amphotericin B colloidal dispersion in three patients. Clin Infect Dis. 1998;26:1430–1433. doi: 10.1086/516349. [DOI] [PubMed] [Google Scholar]
- Kline S, Larsen TA, Fieber L, et al. Limited toxicity of prolonged therapy with high doses of amphotericin B lipid complex. Clin Infect Dis. 1995;21:1154–1158. doi: 10.1093/clinids/21.5.1154. [DOI] [PubMed] [Google Scholar]
- Walsh TJ, Hiemenz JW, Seibel NL, et al. Amphotericin B lipid complex for invasive fungal infections: analysis of safety and efficacy in 556 cases. Clin Infect Dis. 1998;26:1383–1396. doi: 10.1086/516353. [DOI] [PubMed] [Google Scholar]