

Abstract
Papilloma associated with recurrent respiratory papillomatosis (RRP), caused by human papilloma virus (HPV) infection types 6 and 11, is the most common benign neoplasm of the larynx. The clinical features of RRP vary widely from mild to aggressive forms. RRP in children is known as juvenile-onset recurrent respiratory papillomatosis (JORRP). Its outcome may be poor or even fatal due to the high rate of recurrence and eventual spread to the entire respiratory tract. Pulmonary invasion is reported to occur in 3.3% of patients with RRP, and malignant transformation in 0.5% of patients. We report the case of a 39-year-old female patient with a diagnosis of JORRP from the age of 3 years, with extensive bilateral pulmonary involvement and malignant transformation. Analysis of the papilloma and carcinomatous tissues revealed the presence of HPV type 11, which is associated with rapid and aggressive progression. We discussed the case on the basis of a literature review on pulmonary invasion, malignant transformation, and HPV 11 aggressiveness.
Keywords: Carcinoma, Squamous Cell; Human Papillomavirus 11; Lung Neoplasms; Papillomavirus Infections; Recurrent Respiratory Papillomatosis
CASE REPORT
A 39-year-old Caucasian female had been diagnosed with juvenile-onset recurrent respiratory papillomatosis (JORRP) at the age of 3 years, and several polypoid lesions’ resections were performed at follow-up every 3 months from then on. She denied smoking and drinking alcoholics. She started presenting with shortness of breath and chest pain over the last three years, when the diagnosis of the pulmonary involvement by the papillomatosis was made with the aid of a thoracic computed tomography (CT). At her last hospitalization — 6 days before her death — she presented to the emergency room complaining of worsening of shortness of breath, chest pain and weight loss. A new CT scan was performed showing a worsening pattern of the pulmonary invasion, and a working diagnosis of bronchopneumonia. She was prescribed antibiotics, and a transbronchial biopsy was made. Her clinical status worsened with progressive respiratory failure accompanied by sepsis and death.
Autopsy Findings
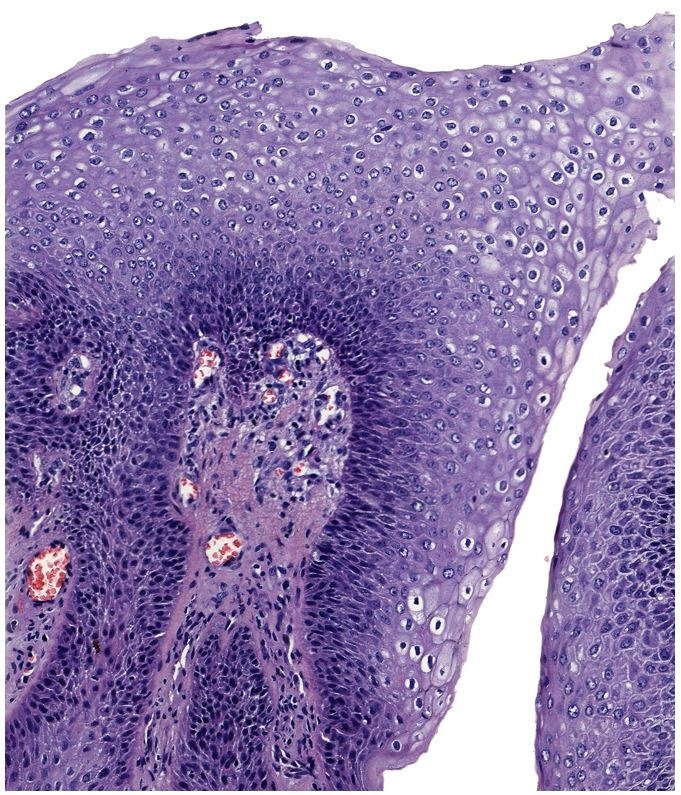
A post-mortem examination revealed multiple polypoid lesions varying from 0.5 to 1.0 cm in diameter in the larynx (Figure 1), which was consistent with extensive papillomatosis with evident koilocytotic atypia (Figure 2).
Figure 1. Gross view of the larynx with multiple polypoid projections in the larynx.
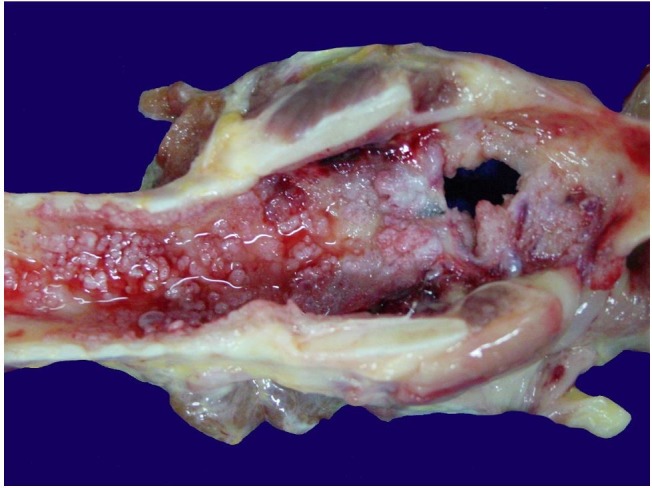
Figure 2. Photomicrography of the laryngeal papilloma with evident koilocytotic atypia (H&E, 150X).
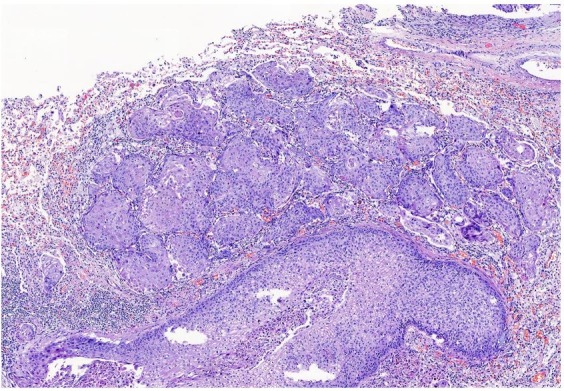
The trachea and bronchi presented hyperemia, and the pleural surfaces were firmly adhered at the posterior thoracic wall. The pulmonary parenchyma was largely replaced bilaterally by multiple confluent nodules measuring between 1.0 and 5.0 cm in diameter, some of them with necrotic and/or purulent centers (Figure 3). The histological examination confirmed the diagnosis of the last in vivo biopsy (undertaken 2 days before the patient’s death), of a well differentiated squamous cell carcinoma, diffusely infiltrating both lungs and extending to the posterior thoracic wall (Figure 4).
Figure 3. Gross view of the mediastinal organs showing lungs largely replaced bilaterally by multiple confluent and partially necrotic nodules.
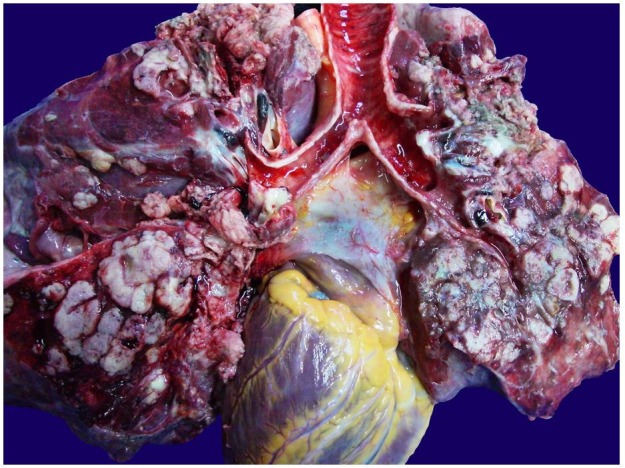
Figure 4. Photomicrography of the lung showing invasive well differentiated squamous cell carcinoma of the lung (H&E, 50X).
We tested tissue slices from the different lesions by polymerase chain reaction (PCR) followed by reverse blot hybridization with the automated human papilloma virus (HPV) genotyping using the INNO-LiPA HPV Genotyping kit (Fujirebio, USA), in an AutoBlot-3000H (MedTec Biolab Equipment, USA).1,2
We were able to detect HPV 11 in the tissue derived from both the laryngeal papilloma and the carcinomatous lung.
DISCUSSION
Despite the low incidence, papillomas associated with HPV infection types 6 and 11 are the most common benign neoplasms of the larynx, corresponding to 84% of cases. They are characterized by numerous papillomas, which are generally limited to the larynx.3,4
The course of the recurrent respiratory papillomatosis (RRP) is unpredictable, as some patients present a mild form with spontaneous recovery or cure after a single exeresis of the laryngeal papilloma, while others present an aggressive form of the disease with many recurrences requiring multiple interventions and hospitalizations.4,5 The latter situation is less common, with the incidence rate of 1.8 cases per 100,000 adults and 4.3 cases per 100,000 children. A smaller number of patients present the malignant transformation of the lesion.6
RRP is clinically divided according to the age of onset: JORRP is used to describe the disease when it primarily manifests in children around the age of 2 to 4 years, and adult-onset recurrent respiratory papillomatosis (AORRP) when it manifests mainly between the ages of 20 and 40 years.6 Although the lesion is benign in nature, RRP may present an aggressive clinical course among children and can be fatal because of its repeated recurrence and spread throughout the respiratory tract.7
It is believed that JORRP is vertically transmitted through the mother’s infected genital tract at the time of birth. Indeed, a case-control study of 3033 Danish births showed that the risk of JORRP increased 231 times when the mother had genital warts during pregnancy,8 while AORRP is related to urogenital dissemination3 and possible re-activation of a latent HPV infection acquired in childhood.9
A systematic review carried out in 2008 by Gélinas et al.10 found that 83% of cases were diagnosed before 4 years of age (median age: 2 years; range: 2 months to 19 years). In 2014, Niyibizi et al.11 analyzed 19 studies concerning the age of the initial diagnosis of JORRP, and found the mean age to be 2-9.4 years, with a median of 3-5.5 years. The results of the previous studies suggested that JORRP is not only more aggressive than AORRP, but also more prone to present a poor clinical course when diagnosed before the age of 3 years.9,12 Although our patient was diagnosed when she was 3 years old, the disease did not follow an aggressive course until her final days.
The diagnosis is usually made by direct or indirect laryngoscopy. The vocal fold is the first and predominant site of the papilloma lesions. Bronchoscopy with biopsy must be performed to assess and study the full extent of the disease. Hoarseness is the main presenting symptom and may be accompanied by stridor, which is initially inspiratory, but it then becomes biphasic. These symptoms may be followed by airway obstruction.7,13
When RRP results in respiratory distress by obstructing papilloma, a tracheotomy may be necessary. However, it has been suggested that this procedure may activate or contribute to the spread of the disease to the lower respiratory tract.7 Currently, there is no therapy that offers a cure for RRP; however, surgical excisions are frequently performed to improve the patient’s voice quality and to prevent respiratory obstruction.9 With regard to the disease’s aggressiveness, Tjon Pian Gi et al.14 showed that patients with RRP onset at an early age had a higher number of surgical interventions in the first years of the disease, which is possibly due to two causes: first, RRP is characterized by a more aggressive course at the beginning of the disease in this age group; and second, at presentation the disease is often already widespread and requires more than one intervention.
In studies carried out between 1950 and 1980 comprising 532 cases, the order of frequency of the disease’s propagation was in the true vocal cords, the oral cavity, the trachea, the bronchi, and the esophagus. In 2%–17% of RRP cases, the propagation occurred through to the distal trachea and bronchi, and less than 1% to the pulmonary parenchima,6,15-17 as observed in our case. However, Gélinas et al.10 brought together cohort studies on RRP, and of the 1666 patients with the disease 55 (3.3%) had pulmonary involvement. In addition, cross-sectional studies were evaluated in the same review, which showed an incidence of pulmonary dissemination of 2.3% (28 of 1202 patients).
Several hypotheses have been proposed to explain the development of pulmonary lesions: contiguous extension of papilloma, diffuse viral contamination, a multicentric origin of papilloma, and aerial dissemination. However, the most common reported causes of dissemination to the trachea, bronchi, and lungs are thought to occur when the tracheostomy and endoscopic resection are perfromed10,18 in which fragments of the detached lesions are carried downwards by the airflow. Fragments that lodge in the proximal respiratory bronchioles are removed by coughing and via the mucociliary transport system. Smaller fragments, which are propelled further out in the airway beyond the ciliated epithelium, may be poorly cleared, and depending on the host’s defenses and the characteristics of the papilloma, they may grow.16 Our patient did not receive a tracheostomy but did undergo several resections during her lifetime; the pulmonary involvement may be explained by the multiple resections.
Pulmonary involvement in RRP is twice as frequent among males compared with females, and is associated with a more aggressive clinical course. The median interval time between the diagnosis of RRP and the lung involvement is 8 years (range <1–45).10 The number of pulmonary lesions is directly associated with the symptoms, and when the lesions become numerous and large, or progress rapidly, the prognosis deteriorates.16,19 The difference of disease aggressiveness between juveniles and adults disappears after 10 years of follow-up; however, this does not apply to distal spread, which is more pronounced in juveniles regardless of disease duration.9 The worse prognosis is characterized by repeated polyp excisions, tracheostomy, and ultimately death due to respiratory failure or infections.4,19
Malignant transformation to squamous cell carcinoma, as found in our case study, is a rare event that, according to Gélinas et al.,10 occurs in 0.55% (9 in 1666 patients with RRP), and may be found in the larynx, the bronchi, or the lungs. Malignant transformation into squamous cell carcinoma is more frequent in older children, and the median time interval between the diagnosis of JORRP and the diagnosis of cancer is 19 years (range 4-45 years).10,20 However, in patients with RRP and pulmonary involvement, cancer developed in 16% (9 of the 55 patients), and was predominantly of the squamous cell type. These findings suggest that patients with pulmonary involvement of JORRP are more prone to develop malignant disease than those with isolated upper airway involvement.
The HPV may remain quiescent in the mucosa for a long time. The malignant transformation may occur 25 years after the onset of JORRP, probably as a consequence of the host genome’s changes induced by environmental carcinogens and by interaction with the HPV genome. Therefore, a long-term follow-up of patients with relapsed JORRP is recommended.4,21 In our case, the malignancy was diagnosed 33 years after the diagnosis of JORRP.
HPV types 6 and 11 are considered low risk for the development of pre-cancerous lesions in the genital tract; however, patients with RRP may develop bronchopulmonary carcinoma when infected by these virus types, especially when they are associated with any of the following potential cofactors: (i) radiation; (ii) immunosuppression; (iii) chemotherapy; (iv) multiple recurrences; and (v) smoking and/or alcohol addiction.4 HPV types 6 and 11 are found in more than 95% of JORRP cases; HPV 11 alone in 47% while other genotypes, namely 16, 31, 33, 35, and 39, account for less than 5%.11 Our patient had multiple recurrences as the only cofactor for developing the carcinoma.
It has been reported that patients with JORRP infected by HPV 11 experience a more rapid and aggressive disease progression than those infected by HPV 6. HPV 11 is more associated with squamous cell carcinoma, with invasion of the lungs and other sites. Patients affected by HPV-11-related papillomatosis are younger, have a longer period of disease activity, require more surgical procedures, have more laryngeal spread, and are less likely to enter remission. These data suggest that HPV 11 can play an important role in the carcinogenesis of the larynx and the respiratory tract, particularly in patients with JORRP.9,10,12,14,22,23
In the study of the final biopsy and the post-mortem examination samples of our patient, we found—by reverse hybridization and PCR—HPV 11 infected lesions. These findings are consistent with those encountered in the literature data review.
CONCLUSION
JORRP’s aggressiveness is related to three strong risk factors: (i) age at diagnosis; (ii) type 11 HPV; and (iii) multiple resections. Ultimately, JORRP can be fatal as a result of acute airway obstruction due to pulmonary spread or malignant degeneration of the papillomatous lesions.
Footnotes
How to cite: Mitsumoto GL, Del Carlo Bernardi F, Paes JF, Villa LL, Mello B, Pozzan G. Juvenile-onset recurrent respiratory papillomatosis with pulmonary involvement and carcinomatous transformation. Autops Case Report [Internet]. 2018;8(3):e2018035. http://dx.doi.org/10.4322/acr.2018.035
This manuscript is in accordance with the institutional ethics committee from Irmandade da Santa Casa de Misericordia de Sao Paulo’s requirements and was approved for publication (process number 001/2018).
Financial support: None
REFERENCES
- 1.Molijn A, Kleter B, Quint W, van Doorn L-J. Molecular diagnosis of human papillomavirus (HPV) infections. J Clin Virol. 2005;32(Suppl 1):S43-51. 10.1016/j.jcv.2004.12.004. [DOI] [PubMed] [Google Scholar]
- 2.Safaeian M, Herrero R, Hildesheim A, et al. Comparison of the SPF10-LiPA system to the Hybrid Capture 2 Assay for detection of carcinogenic human papillomavirus genotypes among 5,683 young women in Guanacaste, Costa Rica. J Clin Microbiol. 2007;45(5):1447-54. 10.1128/JCM.02580-06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Pagliuca G, Martellucci S, Degener AM, et al. Role of human papillomavirus in the pathogenesis of laryngeal dysplasia. Otolaryngol Head Neck Surg. 2014;150(6):1018-23. 10.1177/0194599814525749. [DOI] [PubMed] [Google Scholar]
- 4.Can NT, Tretiakova MS, Taxy JB. Natural history and malignant transformation in recurrent respiratory papillomatosis: human papillomavirus (HPV), dysplasia and an autopsy review. Fetal Pediatr Pathol. 2015;34(2):80-90. 10.3109/15513815.2014.968271. [DOI] [PubMed] [Google Scholar]
- 5.Aaltonen LM, Rihkanen H, Vaheri A. Human papillomavirus in larynx. Laryngoscope. 2002;112(4):700-7. 10.1097/00005537-200204000-00020. [DOI] [PubMed] [Google Scholar]
- 6.Zhang Z, Chang M, Moreta-Sainz LM. Case report: pulmonary papillomatosis in a patient presenting with cough and hemoptysis. Perm J. 2015;19(3):e125-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Derkay CS, Wiatrak B. Recurrent respiratory papillomatosis: a review. Laryngoscope. 2008;118(7):1236-47. 10.1097/MLG.0b013e31816a7135. [DOI] [PubMed] [Google Scholar]
- 8.Silverberg MJ, Thorsen P, Lindeberg H, Grant LA, Shah KV. Condyloma in pregnancy is strongly predictive of juvenile-onset recurrent respiratory papillomatosis. Obstet Gynecol. 2003;101(4):645-52. [DOI] [PubMed] [Google Scholar]
- 9.Omland T, Akre H, Lie KA, Jebsen P, Sandvik L, Brøndbo K. Risk factors for aggressive recurrent respiratory papillomatosis in adults and juveniles. PLoS One. 2014;9(11):e113584. 10.1371/journal.pone.0113584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Gélinas JF, Manoukian J, Côté A. Lung involvement in juvenile onset recurrent respiratory papillomatosis: a systematic review of the literature. Int J Pediatr Otorhinolaryngol. 2008;72(4):433-52. 10.1016/j.ijporl.2007.12.003. [DOI] [PubMed] [Google Scholar]
- 11.Niyibizi J, Rodier C, Wassef M, Trottier H. Risk factors for the development and severity of juvenile-onset recurrent respiratory papillomatosis: a systematic review. Int J Pediatr Otorhinolaryngol. 2014;78(2):186-97. 10.1016/j.ijporl.2013.11.036. [DOI] [PubMed] [Google Scholar]
- 12.Wiatrak BJ, Wiatrak DW, Broker TR, Lewis L. Recurrent respiratory papillomatosis: a longitudinal study comparing severity associated with human papilloma viral types 6 and 11 and other risk factors in a large pediatric population. Laryngoscope. 2004;114(11 Pt 2, Suppl 104):1-23. 10.1097/01.mlg.000148224.83491.0f. [DOI] [PubMed] [Google Scholar]
- 13.Fasunla AJ, Lasisi OA. Diagnostic challenges of laryngeal papillomatosis and its implications among children in developing country. Int J Pediatr Otorhinolaryngol. 2009;73(4):593-5. 10.1016/j.ijporl.2008.12.009. [DOI] [PubMed] [Google Scholar]
- 14.Tjon Pian Gi RE, San Giorgi MR, Slagter-Menkema L, et al. Clinical course of recurrent respiratory papillomatosis: comparison between aggressiveness of human papillomavirus-6 and human papillomavirus-11. Head Neck. 2015;37(11):1625-32. 10.1002/hed.23808. [DOI] [PubMed] [Google Scholar]
- 15.Frauenfelder T, Marincek B, Wildermuth S. Pulmonary spread of recurrent respiratory papillomatosis with malignant transformation: CT-findings and airflow simulation. Eur J Radiol Extra. 2005;56(1):11-6. 10.1016/j.ejrex.2005.07.004. [DOI] [Google Scholar]
- 16.Kramer SS, Wehunt WD, Stocker JT, Kashima H. Pulmonary manifestations of juvenile laryngotracheal papillomatosis. AJR Am J Roentgenol. 1985;144(4):687-94. 10.2214/ajr.144.4.687. [DOI] [PubMed] [Google Scholar]
- 17.Silver RD, Rimell FL, Adams GL, Derkay CS, Hester R. Diagnosis and management of pulmonary metastasis from recurrent respiratory papillomatosis. Otolaryngol Head Neck Surg. 2003;129(6):622-9. 10.1016/j.otohns.2003.08.018. [DOI] [PubMed] [Google Scholar]
- 18.Soldatski IL, Onufrieva EK, Steklov AM, Schepin NV. Tracheal, bronchial, and pulmonary papillomatosis in children. Laryngoscope. 2005;115(10):1848-54. 10.1097/01.mlg.0000173155.57491.2a. [DOI] [PubMed] [Google Scholar]
- 19.Harada H, Miura K, Tsutsui Y, et al. Solitary squamous cell papilloma of the lung in a 40-year-old woman with recurrent laryngeal papillomatosis. Pathol Int. 2000;50(5):431-9. 10.1046/j.1440-1827.2000.01055.x. [DOI] [PubMed] [Google Scholar]
- 20.Boudjemaa S, Leboulanger N, Daınese L, Cremoux PD, Pointe HD, Coulomb A. Metastatic squamous-cell carcinoma of the lung arising in a 12-year-old boy with juvenile recurrent respiratory papillomatosis of neonatal onset. Turk Patoloji Derg. 2014;30(2):133-6. [DOI] [PubMed] [Google Scholar]
- 21.Hočevar-Boltežar I, Žargi M, Gale N. Clinical course of laryngeal papillomatosis. Int Congr Ser. 2003;1240:769-71. 10.1016/S0531-5131(03)00742-8. [DOI] [Google Scholar]
- 22.Bergler WF, Götte K. Current advances in the basic research and clinical management of juvenile-onset recurrent respiratory papillomatosis. Eur Arch Otorhinolaryngol. 2000;257(5):263-9. 10.1007/s004050050236. [DOI] [PubMed] [Google Scholar]
- 23.Seedat RY, Thukane M, Jansen AC, Rossouw I, Goedhals D, Burt FJ. HPV types causing juvenile recurrent laryngeal papillomatosis in South Africa. Int J Pediatr Otorhinolaryngol. 2010;74(3):255-9. 10.1016/j.ijporl.2009.11.016. [DOI] [PubMed] [Google Scholar]