

INTRODUCTION
Coronary artery disease accounts for approximately one-third of all global deaths, and acute myocardial infarction (AMI) is the most severe form of coronary artery disease.1 AMI is defined as myocardial tissue necrosis due to abrupt decrease in coronary blood flow and the most common cause is atheroma-mediated thromboembolism.2 An association between bodybuilding and AMI has already been reported in the literature.3-10 However, no exact mechanism has been identified. Some postulate that strenuous isotonic exercise alone (i.e., bodybuilding) can produce plaque rupture and lead to AMI, while others blame the coexistence of high-risk attitudes towards over-the-counter medications.3-10 Bodybuilders usually abuse steroids, dietary supplements (whey protein powder, amino acid capsules) and other performance enhancers. To increase protein synthesis and induce muscle growth, strenuous isotonic exercise, the use of performance enhancers and protein supplements or a combination of both can cause myocardial infarction (MI). In this paper, we report on one of our patients with acute ST segment elevation MI who also used whey protein powder and amino acid capsules.
CASE REPORT
A 26-year-old male, newbie body builder, presented to our emergency department with substernal crushing chest pain that started after a training session of lifting, 4 hours prior to admission. He had no history of drug use for hypertension, diabetes mellitus and hyperlipidemia. Admission blood pressure was 130/70 mmHg, fasting glucose level was 97 mg/dL, low density lipoprotein level was 97 mg/dL, triglyceride level was 159 mg/dL and high density lipoprotein levels was 43 mg/dL. He had a body mass index of 25 kg/m2. He denies smoking cigarette or any recreational drugs. He denies drinking alcohol. There was no significant coronary artery disease in his family. The admission electrocardiogram showed QS ranging from V1 to V3, ST segment elevation in the lead I and AVL, and reciprocal ST segment depression in the lead II, III and the AVF (Figure 1). It was revealed that the patient has just started performing isotonic exercises for bodybuilding (2 months), and he used whey protein powder plus amino acid capsules. He used 2 gr/kg protein powder daily. It was advised the patient to use 0.8 to 2 gr/gr by the vendor. The whey protein powder contains dextrose, citric acid, soluble cheese water protein, milk protein concentrate, soya lecithin, guar gum, colorants (carmoisine), identical aroma dispersants, cacao powder, vitamins, minerals, and some amino acids (Ronic Nutrition, whey ultimate chocolate and strawberry). The amino acid capsules contain histidine, tryptophan, valine, threonine, arginine, cysteine, tyrosine, glycine, alanine, serine, isoleucine, leucine, lysine, methionine, phenylalanine, aspartic acid, proline, and glutamic acid.
Figure 1.

The admission electrocardiography showed QS from V1 to V3 and ST segment elevation in lead I and AVL and reciprocal ST segment depression in lead II, III and AVF with normal sinus rhythm.
Based on the ongoing chest pain and electrocardiography results an urgent coronary angiography (CAG) was scheduled. The CAG revealed a proximally occluded left anterior descending artery (LAD) (Figure 2A). Percutaneous coronary intervention (PCI) was performed by stenting both the LAD and the diagonal 1 (D1) coronary artery (Figure 2B-F). The patient’s admission blood samples were studied for a thrombophilia panel. The percentage of protein C, protein S, antithrombin levels, and homocysteine levels were within normal limits. Anti-nuclear antibody, HLA-B51 and anti-cardiolipin antibodies were negative. Urine toxicology was negative for over-the-counter drugs and performance enhancers. Transthoracic echocardiography revealed a reduced ejection fraction to 30% with anterior, anterolateral and anteroseptal hypokinesis. A strict recommendation was made for the patient to stop taking the whey protein powder and amino acid capsules and to stop doing the isotonic exercises.
Figure 2.
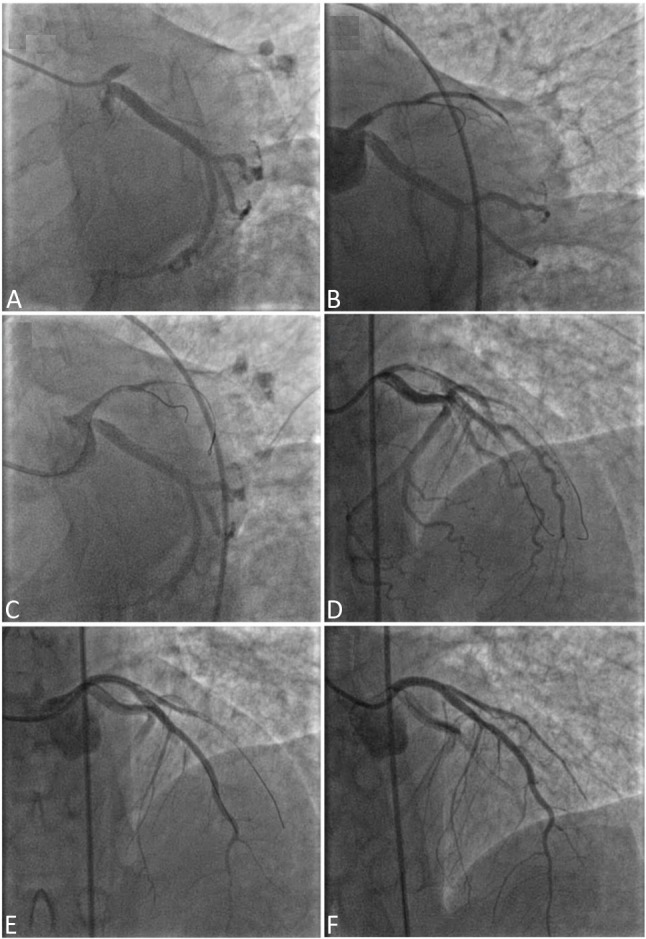
(A) Coronary angiography revealed a proximally occluded LAD; (B-E) Percutaneous coronary intervention is performed with wiring both LAD and D1; (F) The procedure was finished with a final kissing and proximal optimization of LAD (reverse crush technique) and distal TIMI-3 flow.
DISCUSSION
In this report, we present a case of acute anterior ST segment elevation MI in a 26-year-old male bodybuilder that had no conventional risk factors, drug abuse, or thrombophilia, who ingested whey protein powder and amino acid capsules.
Review of literature reveals that the first three types of MI could be seen among bodybuilders. We identified 8 case reports of bodybuilders that were complicated with MI. There is no complementary data about the frequency of MI among the bodybuilders, but it is obvious that the reported cases are far from general occurrences. One reason could be the inaction of clinicians to report, while another could be patient preference not to be socially stigmatized.
Majority of reported cases of bodybuilders complicated with AMI in the literature were associated with anabolic-androgenic steroid (AAS) usage. The ages of subjects varied from 22 years to 41 years. The duration of usage of the AAS is generally between 5 years to 10 years in cases but there is a reported case of AMI after 21 days of usage. The clinical presentation varies from sudden cardiac death to acute ST segment elevation MI. Beside the adverse effects of chronic steroid use on blood lipoprotein profile, on glucose metabolism, on liquid electrolyte balance and blood pressure, it has several significant effects on myocardium. A recently published article11 showed adverse effect of AAS on myocardium as follow: i) decreased left ventricular (LV) ejection fraction that could reverse with discontinuation, ii) decreased LV diastolic function that could not reverse with discontinuation, iii) significantly more LV hypertrophy suggesting an anabolic effect on cardiac muscle mass, iv) increased coronary atherosclerosis and strong association of cumulative lifetime AAS use with severity of atherosclerotic disease.
All the reported cases of bodybuilders that complicated with MI have an association with AAS. However, Rencuzogullari et al.10 reported a case from Turkey that showed a different association with whey protein powder. A 33-year-old bodybuilder presented with anterior ST segment elevation MI and subsequently had undergone CAG. Thrombus was found in all the three coronary arteries. History of the patient revealed usage of whey protein powder without additional AAS or performance enhancers. Speculation is that use of whey protein powder may be the associated risk factor for coronary thrombus formation without a specific pathophysiologic mechanism.
Atherosclerosis and plaque rupture may be one of the pathophysiological mechanisms of MI in our case. Intra coronary thrombus formation or embolus of thrombus could be the other mechanisms to blame. We do not have an exact response for diagnosis since we did not have a chance to see the coronary anatomy with intravascular ultrasound, but we have an impression of coronary plaque rupture complicated with thrombus formation. Intra coronary thrombus formation was the possible mechanism in the case reported by Rencuzogullari et al., because there was thrombus in all the major coronary arteries (RCA, LAD, CX) with distal TIMI-3 blood flow at the same time. Control CAG showed resolution of thrombus in all the coronaries after Gp-2b3a infusion. In our case total occlusion of LAD was present and there was no systemic embolus that makes embolism unlikely. Beside not able to explain the exact mechanism of occlusion of coronary artery in this patient, we could not explain the contribution of whey protein powder and amino acid capsules to the clinical presentation. We postulate that unidirectional nutrition with whey protein powder and amino acid capsules may have played a role in plaque formation and/or transformation from stable plaque to vulnerable plaque.
There is no adequate data about myocardial injury and MI among bodybuilders. Isotonic strenuous exercise, steroid abuse, dietary supplement (whey protein powder, amino acid capsules), and some other performance enhancer usage are the touchstones of the pathophysiology. Reports of cases and prospective studies among bodybuilders may help to clarify cause and effect of these supplements among bodybuilders’ MI.
LEARNING POINTS
1. There is lack of literature about cardiovascular disease among bodybuilders and whey protein users.
2. In the present study, we present a 26-year-old bodybuilder with anterior ST segment elevation myocardial infarction.
3. This study suggests a possible association between whey protein and coronary thrombosis, but the casual relationship has not been established yet.
REFERENCES
- 1.Chu CY, Lin TH, Lai WT. The management and prognostic factors of acute coronary syndrome: evidence from the Taiwan acute coronary syndrome full spectrum registry. Acta Cardiol Sin. 2017;33:329–338. doi: 10.6515/ACS20161205A. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lin HJ, Wang TD. Profiling the evolution of inflammatory response and exploring its prognostic significance in acute myocardial infarction: the first step to establishing anti-inflammatory strategy. Acta Cardiol Sin. 2017;33:486–488. doi: 10.6515/ACS20170731A. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wysoczanski M, Rachko M, Bergmann SR. Acute myocardial infarction in a young man using anabolic steroids. Angiology. 2008;59:376–378. doi: 10.1177/0003319707304883. [DOI] [PubMed] [Google Scholar]
- 4.Halvorsen S, Thorsby PM, Haug E. Acute myocardial infarction in a young man who had been using androgenic anabolic steroids. Tidsskr Nor Laegeforen. 2004;124:170–172. [PubMed] [Google Scholar]
- 5.Tischer KH, Heyny-von Haussen R, Mall G, et al. Coronary thrombosis and ectasia of coronary arteries after long-term use of anabolic steroids. Z Kardiol. 2003;92:326–331. doi: 10.1007/s00392-003-0915-6. [DOI] [PubMed] [Google Scholar]
- 6.Kokkonen L, Anttonen O, Penttila O, et al. Protein C deficiency and use of anabolic steroids behind the myocardial infarction in a young man. Duodecim. 2001;117:2279–2281. [PubMed] [Google Scholar]
- 7.Fineschi V, Baroldi G, Monciotti F, et al. Anabolic steroid abuse and cardiac sudden death: a pathologic study. Arch Pathol Lab Med. 2001;125:253–255. doi: 10.5858/2001-125-0253-ASAACS. [DOI] [PubMed] [Google Scholar]
- 8.Godon P, Bonnefoy E, Guerard S, et al. Myocardial infarction and anabolic steroid use. A case report. Arch Mal Coeur Vaiss. 2000;93:879–883. [PubMed] [Google Scholar]
- 9.Kennedy MC, Corrigan AB, Pilbeam ST. Myocardial infarction and cerebral haemorrhage in a young body builder taking anabolic steroids. Aust N Z J Med. 1993;23:713. doi: 10.1111/j.1445-5994.1993.tb04734.x. [DOI] [PubMed] [Google Scholar]
- 10.Rencuzogullari I, Borekci A, Karakoyun S, et al. Coronary thrombosis in three coronary arteries due to whey protein. American J Emerg Med. 2017;35:664. doi: 10.1016/j.ajem.2016.11.002. [DOI] [PubMed] [Google Scholar]
- 11.Baggish AL, Weiner RB, Kanayama G, et al. Cardiovascular toxicity of illicit anabolic-androgenic steroid use. Circulation. 2017;135:1991–2002. doi: 10.1161/CIRCULATIONAHA.116.026945. [DOI] [PMC free article] [PubMed] [Google Scholar]