

Abstract
Aim
This study investigated the effect of voluntary motor effort during a low-intensity (30% maximal voluntary contraction [MVC]) muscle exercise training program on increasing muscle strength.
Materials and Methods
Eighteen young and healthy individuals were randomly assigned to one of three groups: high mental effort (HME), low mental effort (LME), or a no-training control (CTRL) group. Training lasted for 6 weeks (15 min/day, 5 days/week). The participants’ right-elbow flexor muscle strength was measured before and after the training program.
Key findings
After training, the HME group gained 20.47 ± 8.33% (P = 0.01) strength while the LME and CTRL groups had negligible strength changes (1.89 ± 0.96% and −3.27 ± 2.61%, respectively; P > 0.05) despite muscle contraction intensity (30% MVC) sustained during training was the same for the HME and LME groups. These results suggest that the level of effort involved in resistance exercise training plays a critical role in determining the amount of strength augmentation.
Significance
The finding that high effort combined with low-level physical exercise training can significantly increase muscle strength has rehabilitation applications as many patients and frail older adults have difficulties in participating in high-intensity exercise training such as lifting heavy weights. High effort plus low-level muscle exercise might serve as a safe training regimen for effective muscle strengthening in vulnerable populations.
Keywords: elbow flexor muscles, exercise intensity, maximal voluntary contraction (MVC), mental effort training, muscle strength
Graphical abstract
1. Introduction
It is widely accepted by public and perhaps a majority in the scientific community that muscle strength is dependent on mass or size of the muscle, and muscles strengthen in response to appropriate stress or training intensity. Historically, most strength training programs have emphasized that, for maximum strength gain, training should be conducted at load intensities that are at or near the maximum level and last long enough for all motor units/muscle fibers in a muscle or muscle group to be fully activated. Many studies [1–4] have shown a load-strength relationship, with almost zero strength gain at low loads, highest strength gain at a high but still sub-maximal load, and then decreasing moderately as the load reaches the maximum. In a study near a half century ago [5], subjects trained for 12 weeks at 33% maximal voluntary contraction (MVC) level till exhaustion in each session, but they experienced no strength gain, thus confirming that higher load intensities are required for increasing muscle strength. Other earlier studies [6, 7] made similar discoveries and the observations had led to a widely accepted opinion that if the training intensity is less than 66% MVC, it would be difficult to achieve a significant muscle strength increase [1].
However, later research has reported that training-induced muscle size enlargement or hypertrophy does not match or fully explain the strength increase seen during the initial training period [8]. Thus, even though muscle hypertrophy plays an important role in long term strength increase, the augmentation shown during early weeks of training is mainly instigated by neural adaptations rather than muscular changes. More investigators [9, 10] further examined and confirmed the notion that neural adaptations can result in significant strength gain. Many recent studies [11–19] have reported that subjects who underwent training with motor imagery or mental practice, i.e. performing covert muscle contractions without noticeable muscular activities, resulted in significant strength improvement. In the study by Yue and Cole [18], one group participants performed high-intensity isometric contractions of the left hypothenar muscle (little finger abductor) for 4 weeks, five sessions per week while another group imagined producing these same, high-effort isometric contractions. They found that the group that performed high-intensity physical contractions had a 30% strength increase while the group that performed high-effort imagined contractions had a 22% increase. The strength gain in the imagery training group was attributed to alterations occurred in central motor programming and planning rather than adaptations within the muscle, as it was quiescent during training. Ranganathan et al.[12] also showed that training with mental imagery of strong muscle contractions resulted in significant strength gains in both small distal (little finger abductor) and large proximal (elbow flexor) muscles of the upper limb and that these strength additions were accompanied by an increase in movement-related cortical potentials (MRCP), triggered by multiple trials of the finger abduction and elbow flexion MVCs and considered as a measurement of descending command for the intended motor action [12, 20].
Given the fact that many motor imagery studies discovered that significant strength gain can be achieved even without muscle exercise, it appears that strength can be augmented as long as the effort involved in the intended motor action is high. The current pilot study tested this hypothesis by having two groups of participants undergo a six-week training program involving elbow flexion contractions at 30% MVC with one group engaging in high effort during each contraction while the other group low effort. It was hypothesized that the participants trained by the high effort elbow flexion task would gain a significant amount of strength but those trained by the low effort contractions would not despite the fact that both groups physically exercised at the same intensity level (30% MVC).
2. Methods
Eighteen (18 – 35 years) young and healthy volunteers were recruited and randomly assigned into three groups: high mental effort (HME, n=6); low mental effort (LME, n=6); and a no-training control (CTRL, n=6) group. A majority of the participants were college students who were active but not involved in any type of regular exercise (such as lifting weights or running regularly each week) in the past year. None of the participants had a history of neurological or musculoskeletal disorders, nor was any of them an athlete prior to the study. The training lasted for 6 weeks (15 minutes/day and 5 days/week Monday through Friday). The local Institutional Review Board approved the study and all participants gave their informed consent prior to participation.
2.1 Training Protocol
During training, participants sat comfortably in an experimental chair with their right arm attached to a force transducer device. In each trial, those in the HME group exerted elbow flexion force of the right arm to a target (30% MVC) displayed on an oscilloscope as a horizontal cursor/line. In each trial while keeping the force roughly on the target (they were told not to pay close attention to accurately match the force with the target as long as the force stayed at about the target), they urged the forearm to push upward maximally for ~15 s against the wrist cuff of the force transducer device and then rested for 15 s before performing the next trial. In the HME contraction process, participants exerted a low level of physical activity (~30% MVC) and imagined (internal imagery) at the same time that they are contracting their muscle as hard as possible. In other words, in their mind they wanted or intended to make a maximal elbow flexion in each trial; and therefore, their effort was high. A total of 30 HME trials were performed in each training session. Throughout each training session the subjects were verbally encouraged to exert their maximal effort in performing the trials.
Participants in the LME group, similar to HME, performed 30 trials (30 s each followed by a 30-s rest) in each training session. In each trial, they exerted a low-intensity, 30% MVC force to match the target displayed on the oscilloscope and at the same time watched an entertaining video (e.g., a movie) of their choice previously recorded on a tape. Because subjects did not pay much attention to the on-going muscle contraction, their mental effort for the motor task was considered to be low. In order for the participants in the LME group not to pay close attention to match the exerted force with the target and at the same time their exerted force being not lower than the target when watching the video, they were advised to exert a force that could be a slightly higher than the target level to create a positive margin between the exerted force and target that would allow fluctuations of the force (due to lack of attention) above or near the target. The CTRL group participated in all measurement sessions, but did not undergo any training.
2.2 Force Measurement
Elbow flexion force was measured by a force sensor (JR3 Universal Force-Moment Sensor System, Woodland, CA) with subjects seated, their right hand placed in a wrist cuff, forearm in a neutral position with an elbow joint angle of ~100°, and upper arm slightly abducted (around 15°) on the side of the torso [12]. The elbow was supported at hip height and the shoulders and torso were kept in position using restraints. Three trials (4–5 s per trial) were performed in each measurement session and the highest force among the trials was analyzed [18]. For each trial, participants were verbally encouraged to exert maximal force/strength. Strength measurements were made before training and after the 6-week training period. The strength measurement conditions (arm and body positions), and joint angles were carefully measured each time and maintained as consistently as possible over the sessions. In addition, the verbal instruction and encouragement for maximal force production were similar for all measurement sessions. The same force transducer system was used to measure the force during the HME and LME training. The force data were digitized at 100 samples per second using a data acquisition system (1401 Plus, Cambridge Electronic Design, Ltd., Cambridge, UK).
2.3 Statistical analysis
Due to pilot nature of the study, statistical analysis was performed using one-tail, paired t-test (within group) to compare the post-training strength measurement with the pre-training measurement within each group. Between-group values, including pre-training (baseline) strength, post-training strength, and percent increase were analyzed using one-way analysis of variance (ANOVA). The level of significance was set at 0.05 for all statistical analyses. Results are given as mean ± SE.
3. Results
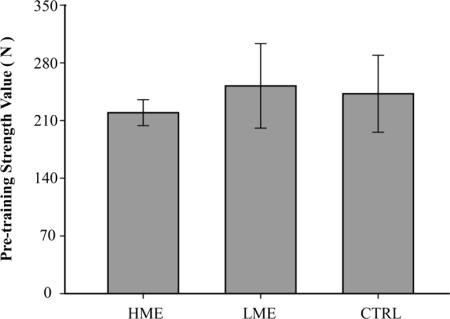
There was no significant difference in the pre-training strength values between groups (F(2,15) = 0.166, P = 0.849) (Fig. 1). Training intensity (elbow flexion force sustained during training) randomly sampled during the 6 week period was slightly higher (but not statistically significant, F(1,10) = 1.536, P = 0.244) for the LME than HME groups (Fig. 2). Periodic (~twice a week) surface EMG recordings did not show a significant difference in the biceps brachii (BB) and brachioradialis (BR) muscle activity level during training between the HME and LME groups, suggesting that likely the agonist-antagonist co-contraction level was also similar between the two groups (this is because if one group had a higher level of co-contraction or higher antagonist muscle activity, then to maintain the same force the BB and/or BR activation level should also be higher). Within-group comparisons revealed that the strength increased significantly after training in the HME group (t(5) = 2.405, P = 0.03) but the change was not significant in the LME group (t(5) = −1.086, P = 0.16). The elbow flexion strength of the CTRL group decreased six weeks after the baseline strength test but the change was not significant (t(5) = 1.801, P = 0.07). Groups comparisons in percent (%) strength change (post-training vs. pre-training) indicated that the increase was significantly greater in HME (20.47 ± 8.33%) than LME (1.89 ± 0.96%) and CTRL (−3.27 ± 2.61%) groups (F(2,15) = 6.065, P = 0.01). Fig. 3 shows strength changes (relative to each group’s baseline) in the three groups.
Fig. 1.
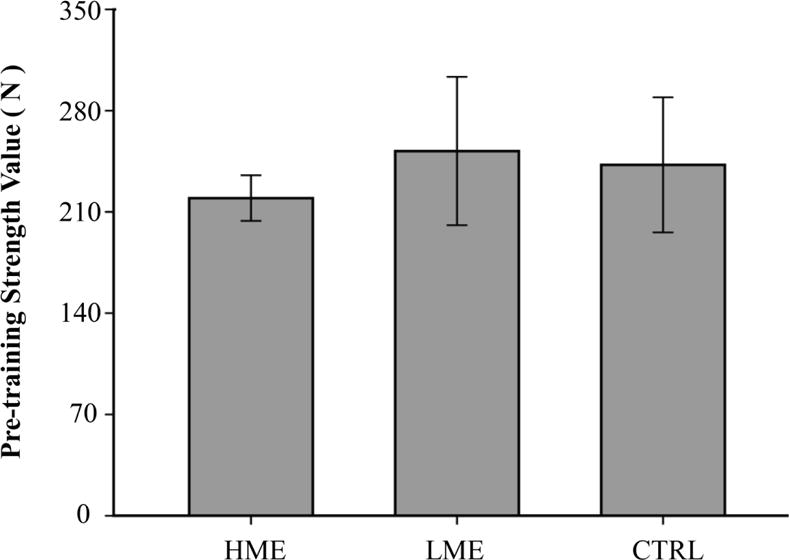
Pre-training (baseline) strength measurement. There was no significant difference in pre-training strength among the three groups (P=0.85).
Fig. 2.
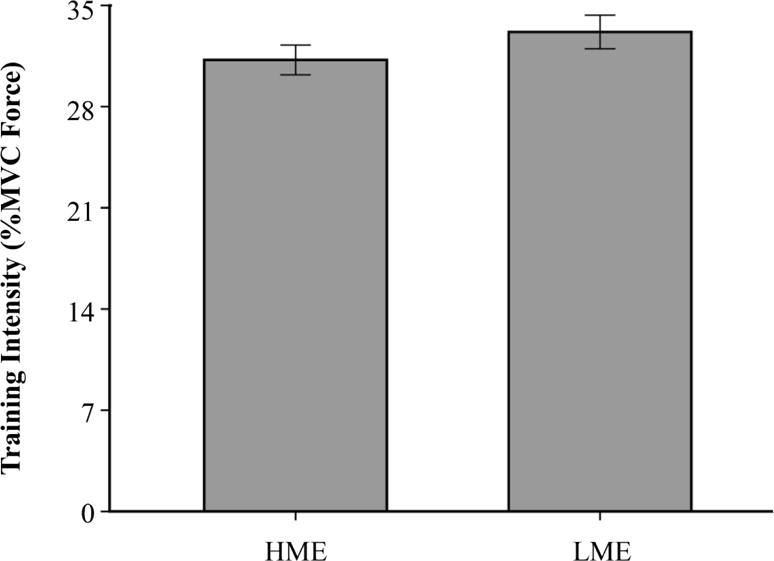
Muscle exercise intensity (percent elbow flexion force) during high mental effort (HME) and low mental effort (LME) training. The muscle training intensity during the 6-week period was similar (~30% MVC) between the LME and HME groups (P = 0.24).
Fig. 3.
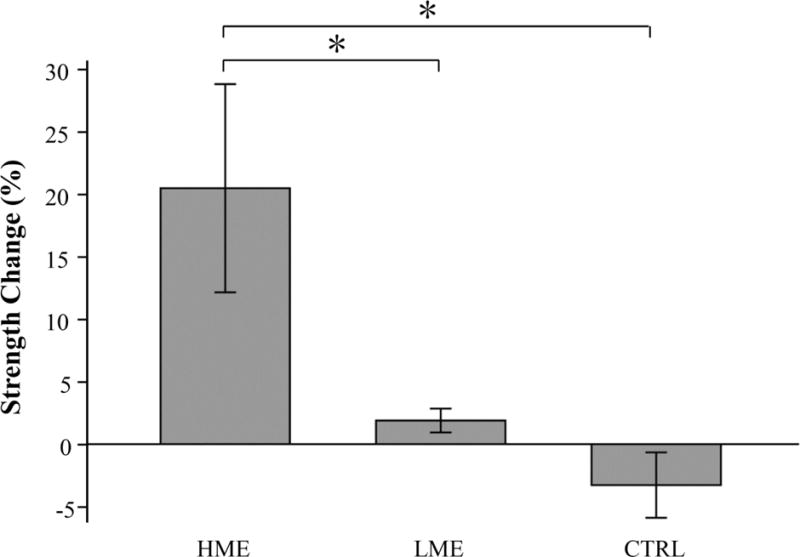
Percent elbow flexion strength changes in high mental effort (HME), low mental effort (LME) and no-training control (CTRL) groups following a 6-week training program. Only the HME group had a significant strength gain (20.47%) after training (P<0.05). The strength change in the LME and CTRL groups was not significant.
4. Discussion
The major finding of this pilot study was that participants in the HME group had a significant strength increase but those in the LME group did not despite the fact that subjects in both groups trained their muscles (elbow flexors) at a similar activation intensity (~30% MVC). Since the only difference in the training programs for the two groups was the level of effort involved during the low-intensity physical exercise, it is reasonably to suggest that human muscle strength gain following a relatively short training program (e.g., 6 weeks in this study) depends primarily on the level of effort involved in the training, not muscle exercise intensity per se. The data suggest that the level of effort involved in generating a relatively low-level motor activity during training plays a critical role in determining strength gains. This explains repeated observations in recent years that human upper and lower limb muscles can be significantly strengthened even without noticeable muscle exercise as long as a strong intent or effort is involved in the envisioned muscle action during training. The application of this finding to medical rehabilitation is obvious as many frail patients and elderly persons are afraid of or feel difficult in engaging in high-intensity physical training such as weightlifting, yet these individuals are capable to carry out strong-willed mental exercises alone or combined with low- to moderate-level muscle contractions to strengthen their muscles [21]. Weakness is considered as a primary factor contributing to physical disability in aging [22–23] and other conditions [24–25]; yet, individuals with prominent muscle weakness are ones mostly challenged by conventional strength training. The finding of the current study points to a beneficial and cost-effective muscle strengthening therapy for populations enduring significant weakness.
4.1 Why high effort training can but low effort training cannot augment strength?
High mental effort training without muscle activation is essentially the same as internal or kinesthetic motor imagery (KMI) training. In KMI (also known as first-person imagery), a person imagines or mentally creates the feeling of performing the exercise from first-person perspective or within the body [17]. For instance, motor imagery training aimed at increasing strength using KMI emphasizes that the participant generates a similar feeling as he/she felt during a physical, strong muscle contraction [12, 15, 19]. Indeed, performing KMI generates obvious physiological responses such as increased heart rate, blood pressure and respiration rate [12]. An increase in movement-related cortical potential (MRCP) directly associated with and triggered by multiple maximal voluntary contractions (MVC) following KMI training suggests that intensified descending command is a consequence of the high effort training [12, 17]. Augmented EMG signal during MVC following high effort training is an indication of improved motor unit recruitment and/or motor unit activation level [18, 26] as a result of elevated MRCP. Thus, the significant strength gain seen in the HME group cannot be a result of covert or low-level muscle activation (psychoneuromuscular theory) or non-specific motivational effects [19], since the LME group during training also had similar or even slightly higher amount of muscle activities, but did not experience significant strength gains.
Explanations for the LME group not having a significant strength gain following six weeks exercise training at ~30% MVC level include, but not limited to (i) the effort was too low to induce meaningful adaptations in the brain to change the descending command for maximal force production, especially the subjects’ attention was directed to watching their favorite entertaining programs; (ii) the muscle exercise intensity was not high enough to inflict a significant increase in muscle mass; and (iii) the training was not able to significantly change muscle coordination such as reducing antagonist muscle activation or altering activation patterns among the synergists and antagonists during post-training strength measurement. It has often been reported that low intensity muscle exercise training (assuming the associated effort is also low) does not result in significant strength improvement [1] and our results are in agreement with this view.
The control of the low-intensity training task could be accomplished by lower-order motor centers located in the sub-cortical motor areas without significant participation by the cortical fields especially higher-order cortices such as secondary and association motor control cortices. This view is supported by our observation that the participants were able to sustain the force at roughly 30% MVC level without paying close attention (they were watching video programs) and people’s experience of walking while doing another activity such as a telephone conversation or reading a text message. On the other hand, the HME task involves internal imagery or strong intent to move that activates higher order cortical areas that strengthen or enhance the neural circuitry that controls the descending pathway projecting to and driving the trained muscle. Many functional imaging studies [27–29] have shown cortical motor-control network activation during various motor imagery tasks. Together, the findings suggest that the level of mental effort does play a crucial role in determining short-term strength gains for both conventional strength training as well as KMI training with or without combined low-intensity muscle exercise. It is worth noting that high intensity muscle contractions such as MVC always require high effort; that is the reason that conventional high-intensity strength training almost always leads to strength improvements even before muscular adaptions occur [30].
4.2 Why high effort training should combine with low-intensity muscle exercise?
A unique aspect of our HME training was the simultaneous performance of high-effort and low-intensity exercise. Many studies have reported that combining imagery and physical contractions result in the highest strength gain compared to physical contraction or mental imagery alone. However, the training protocols followed in these studies require some trials with physical contraction alone and remaining trials with mental contractions alone, but never a simultaneous physical and mental contraction together. In our study, the subjects exerted low levels of physical contraction (30% MVC) and imagined (internal imagery) at the same time that they are contracting their muscle as hard as possible. Similar to observations from other studies, this combination of mental and physical contraction is more effective than either one alone. One of the important implications of this finding is in clinical rehabilitation, where patients who can exert only low levels of force can combine high levels of mental effort to improve or at least maintain their muscle strength. In addition, maintaining low to moderate level physical exercise during high effort training may add extra benefit such as vascular and metabolic function gains within the exercised muscles.
4.3 Is effort training combined with low-intensity exercise better than effort training alone?
No direct comparisons have been made between the two types of effort training (with and without light exercise) aiming at improving muscle strength. However, the results made by the current study and Yao et al. [17] are worth for comparative evaluation. Both the studies examined healthy and young participants with six individuals in each group who underwent a six week high effort training program (one session each day M-F each week) for elbow flexion strength improvement. The only difference between the two training programs was that in Yao et al. [17] no physical activities were combined with the high effort training. The strength increase observed by Yao et al. [17] was 10.8% but that by the current study was 20.47%, an almost 10% difference, or the amount of strength gain was almost doubled in the combined protocol vs. high effort alone protocol (with no exercise performed). These preliminary observations suggest that a strength training regime combining strong effort with a low level of muscle activation can yield better training outcome (greater strength increase) than a similar effort training program but without added physical exercise, albeit both training regimes can yield significant strength gains. Perhaps by allowing a certain level of motor output to flow out the descending pathway to the target muscle, the motor control network at various levels may be more efficiently or effectively trained in a process in which the control system does not need to completely shut down the descending pathway while at the same time attempting to generate a strong muscle activation command.
4.4 Limitations and future direction
The small group sample size limits us from making strong conclusions, although a significant difference in strength gain was seen between the HME and LME training groups. Neural signals from central and peripheral nervous systems were not measured during pre- and post-training strength measurement sessions. The lack of nervous system signals accompanying the strength measurements hampers our ability to understand mechanisms behind the observations made by the study. Future studies could employ high density EEG or MEG to map dynamic sources of cortical signals arising during both the effort training and strength evaluation. Functional imaging such as fMRI would provide additional information regarding location and activation levels while participants perform HME vs. LME tasks, and plasticity of the events in the CNS as a result of the training programs. Both neural plasticity and muscular adaptations associated with longer training programs (as muscle structural changes such as hypertrophy take longer time to occur) should be quantified to distinguish central and peripheral contributions to the strength improvement. Finally the training regime of high effort combined with low level physical exercise needs to be tested in clinical populations with severe weakness that limits them from undergoing conventional strength training to determine whether such training is an effective muscle strengthening therapy.
5. Conclusions
This study demonstrates clear results that young and healthy individuals having undergone training with high mental effort for elbow flexion contractions combined with a low (30% maximal) level of physical elbow flexion exercise can significantly increase elbow flexion strength but those trained with a low level of effort combined with the same low level of physical elbow flexion exercise cannot. The level of mental effort involved in muscle strengthening plays a critical role in determining the amount of strength gain. The finding has potential application to medical rehabilitation in helping frail patients, older adults and injured athletes/persons gain or maintain muscle strength.
Acknowledgments
Source of Funding: This study was supported in part by National Institutes of Health grants R01NS035130 and R01HD036725 to G. H. Yue, and by State General Administration for Sports Scientific Research (2015B040) and Open Research Fund of the State Key Laboratory of Cognitive Neuroscience and Learning to C. H. Jiang.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflict of Interests: The authors declare that there is no conflict of interests regarding the publication of this paper.
References
- 1.Atha J. Strengthening muscle. Exerc Sport Sci Rev. 1981;9:1–74. [PubMed] [Google Scholar]
- 2.Berger RA. Comparison of the effect of various weight training loads on strength. Res Q. 1965;36:141–146. [PubMed] [Google Scholar]
- 3.Cotton D. Relationship of the duration of sustained voluntary isometric contraction to changes in endurance and strength. Res Q. 1967;38:366–374. [PubMed] [Google Scholar]
- 4.Dons B, Bollerup K, Bonde-Petersen F, Hancke S. The effect of weight-lifting exercise related to muscle fiber composition and muscle cross-sectional area in humans. Eur J Appl Physiol Occup Physiol. 1979;40:95–106. doi: 10.1007/BF00421155. [DOI] [PubMed] [Google Scholar]
- 5.Ikai M, Yabe K. Training effect of muscular endurance by means of voluntary and electrical stimulation. Eur J Appl Physiol Occup Physiol. 1969;28:55–60. doi: 10.1007/BF00696039. [DOI] [PubMed] [Google Scholar]
- 6.Petersen FB. Muscle training by static, concentric and eccentric contractions. Acta Physiol Scand. 1960;48:406–416. doi: 10.1111/j.1748-1716.1960.tb01874.x. [DOI] [PubMed] [Google Scholar]
- 7.Berger R. Effect of varied weight training programs on strength. Res Q. 1962;33:168–181. [Google Scholar]
- 8.Moritani T, deVries HA. Neural factors versus hypertrophy in the time course of muscle strength gain. Am J Phys Med. 1979;58:115–130. [PubMed] [Google Scholar]
- 9.Jackson PL, Lafleur MF, Malouin F, Richards C, Doyon J. Potential role of mental practice using motor imagery in neurologic rehabilitation. Arch Phys Med Rehabil. 2001;82:1133–1141. doi: 10.1053/apmr.2001.24286. [DOI] [PubMed] [Google Scholar]
- 10.Sale DG, Macdougall JD, Upton AR, Mccomas AJ. Effect of strength training upon motoneuron excitability in man. Med Sci Sports Exerc. 1983;15:57–62. [PubMed] [Google Scholar]
- 11.Malouin F, Belleville S, Richards CL, Desrosiers J, Doyon J. Working memory and mental practice outcomes after stroke. Arch Phys Med Rehabil. 2004;85:177–183. doi: 10.1016/s0003-9993(03)00771-8. [DOI] [PubMed] [Google Scholar]
- 12.Ranganathan VK, Siemionow V, Liu JZ, Sahgal V, Yue GH. From mental power to muscle power-gaining strength by using the mind. Neuropsychologia. 2004;42:944–956. doi: 10.1016/j.neuropsychologia.2003.11.018. [DOI] [PubMed] [Google Scholar]
- 13.Reiser M, Büsch D, Munzert J. Strength gains by motor imagery with different ratios of physical to mental practice. Front Psychol. 2010;2:334–342. doi: 10.3389/fpsyg.2011.00194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Shackell EM, Standing LG. Mind over matter: Mental training increases physical strength. N Am J Psychol. 2007;9:189–200. [Google Scholar]
- 15.Sidaway B, Trzaska AR. Can mental practice increase ankle dorsiflexor torque? Phys Ther. 2005;85:1053–1060. [PubMed] [Google Scholar]
- 16.Smith D, Collins D, Holmes P. Impact and mechanism of mental practice effects on strength. Int J Sport Exerc Psychol. 2011;1:293–306. [Google Scholar]
- 17.Yao WX, Ranganathan VK, Didier A, Vlodek S, Yue GH. Kinesthetic imagery training of forceful muscle contractions increases brain signal and muscle strength. Front Hum Neurosci. 2013;7:99–105. doi: 10.3389/fnhum.2013.00561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Yue GH, Cole KJ. Strength increases from the motor program: comparison of training with maximal voluntary and imagined muscle contractions. J Neurophysiol. 1992;67:1114–1123. doi: 10.1152/jn.1992.67.5.1114. [DOI] [PubMed] [Google Scholar]
- 19.Zijdewind I, Toering ST, Bessem B, van der Laan O, Diercks RL. Effects of imagery motor training on torque production of ankle plantar flexor muscles. Muscle Nerve. 2003;28:168–173. doi: 10.1002/mus.10406. [DOI] [PubMed] [Google Scholar]
- 20.Siemionow V, Yue GH, Ranganathan VK, Liu JZ, Sahgal V. Relationship between motor activity-related cortical potential and voluntary muscle activation. Exp Brain Res. 2000;133:303–311. doi: 10.1007/s002210000382. [DOI] [PubMed] [Google Scholar]
- 21.Jiang CH, Ranganathan VK, Zhang J, Siemionow V, Yue GH. Motor effort training with low exercise intensity improves muscle strength and descending command in aging. Medicine. 2016;95:e3291. doi: 10.1097/MD.0000000000003291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Giampaoli S, Ferrucci L, Cecchi F, Noce CL, Poce A, Dima F, Santaquilani A, Vescio MF, Menotti A. Hand-grip strength predicts incident disability in non-disabled older men. Age Ageing. 1999;28:283–288. doi: 10.1093/ageing/28.3.283. [DOI] [PubMed] [Google Scholar]
- 23.Rantanen T, Avlund K, Suominen H, Schroll M, Frändin K, Pertti E. Muscle strength as a predictor of onset of ADL dependence in people aged 75 years. Aging Clin Exp Res. 2002;14:10–15. [PubMed] [Google Scholar]
- 24.Patten C, Lexell J, Brown HE. Weakness and strength training in persons with poststroke hemiplegia: Rationale, method, and efficacy. J Rehabil Res Dev. 2004;41:293–312. doi: 10.1682/jrrd.2004.03.0293. [DOI] [PubMed] [Google Scholar]
- 25.Plowman EK, Watts SA, Tabor L, Robison R, Gaziano J, Domer AS, Richter J, Vu T, Gooch C. Impact of expiratory strength training in amyotrophic lateral sclerosis. Muscle Nerve. 2016;54:48–53. doi: 10.1002/mus.24990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Yue GH, Wilson SL, Cole KJ, Darling WG, Yuh WTC. Imagined muscle contraction training increases voluntary neural drive to muscle. J Psychophysiol. 1996;10:198–208. [Google Scholar]
- 27.Roland PE, Larsen B, Lassen NA, Skinhøj E. Supplementary motor area and other cortical areas in organization of voluntary movements in man. J Neurophysiol. 1980;43:118–136. doi: 10.1152/jn.1980.43.1.118. [DOI] [PubMed] [Google Scholar]
- 28.Vingerhoets G, de Lange FP, Vandemaele P, Deblaere K, Achten E. Motor imagery in mental rotation: an fMRI study. Neuroimage. 2002;17:1623–1633. doi: 10.1006/nimg.2002.1290. [DOI] [PubMed] [Google Scholar]
- 29.Grosprêtre S, Ruffino C, Lebon F. Motor imagery and cortico-spinal excitability: A review. Eur J Sport Sci. 2016;16:317–324. doi: 10.1080/17461391.2015.1024756. [DOI] [PubMed] [Google Scholar]