

ABSTRACT
Objectives: Newcomers experience unique challenges with respect to vaccination. These challenges are compounded by the need to navigate complex vaccination catch-up schedules upon arrival in their new home countries. Our group has pioneered the development of CANImmunize, a free, bilingual, pan-Canadian digital application designed to empower individuals to manage their vaccination records. To inform how a vaccine tracking app such as CANImmunize might be tailored to meet the unique needs of newcomers, this study sought to determine commonly spoken languages, technology use, and current methods of vaccine tracking among recent newcomers to Canada.
Methods: Government-assisted refugees attending a health clinic in Ottawa, Canada were invited to complete a 17-question needs assessment survey. The survey captured data on household demographics, spoken languages, country of origin, technology use and methods used to track vaccination history.
Results: 50 newcomers completed the needs assessment survey. Arabic was the predominant language spoken by surveyed individuals. Although 92% of participants owned a smartphone, the majority did not actively use digital health applications. 18 (36%) participants reported being vaccinated before arriving in Canada. 27 (54%) participants were parents, 23 of whom reported that their children were vaccinated prior to arrival in Canada. 38 (76%) participants indicated that they would use a vaccine tracking app such as CANImmunize if it were translated into their primary language of communication.
Conclusions: The results of our study indicate that mobile technology may be a useful tool to help newcomer families stay on track with provincial and territorial immunization schedules.
KEYWORDS: vaccines, immunization, refugee health, newcomers, public health, mobile technology
Introduction
The World Health Organization estimates there are nearly 250 million international migrants and 763 million internally displaced individuals across the globe.1 Newcomers, including immigrants, refugees and other migrants, are less likely to have completed vaccine dose series than the general population. This may be due in part to limited access to primary healthcare in their countries of origin where internal conflicts have arisen, or as a result of complex migration patterns.2-4 Refugee newcomers in particular often arrive with illegible, incomplete or no proof of vaccination from their home countries.3 Without complete and comprehensive knowledge of vaccination coverage among this population, public health units in host countries face economic and care challenges related to over- or under-vaccination.
Between January 2015 and November 2017, 91,630 refugees and were resettled across Canada,5 4,525 (4.9%) of whom settled in the nation's capital city, Ottawa.6 As part of the Interim Federal Health program, physicians working overseas administer routine vaccinations to immigrants, refugees and refugee claimants prior to their arrival in Canada. Physicians in this program have recently begun providing print immunization records following vaccination to individuals preparing to emigrate.7 On arrival in Canada, these print records may then be used by Canadian healthcare providers to determine the most suitable course of vaccination for the newcomer based on provincially and territorially recommended catch-up schedules to reduce the likelihood of repeat or over-vaccination and to promote cost-savings. Paper records may be easily misplaced, however, particularly in the course of migration and resettlement.8 Additionally, without reminders or instructions from healthcare providers, vaccination series doses may be missed and never fully completed.
Mobile technology has the potential to empower individuals to manage their own health information. As refugees make frequent use of mobile devices to stay connected with friends and family and to help navigate their host countries,9 there exists the opportunity to additionally leverage mobile devices as tools to support public navigation of complex health systems and promote bi-directional communication between the public and health providers. In 2014, CANImmunize was launched as a pan-Canadian mobile vaccination tool (Fig. 1). CANImmunize is a free, bilingual application (app) that allows individuals to manage their own and their families’ vaccination records. The app contains all twenty-six Canadian provincial and territorial adult and pediatric vaccination schedules with easy-to-understand information on vaccination in each jurisdiction and provides reminders of upcoming or overdue vaccinations. To date, over 211 000 users have downloaded CANImmunize. To inform how CANImmunize might best be tailored to the needs of newcomers, we sought to determine commonly spoken languages, technology use and self-reported vaccination histories of recent newcomers to Canada.
Figure 1.
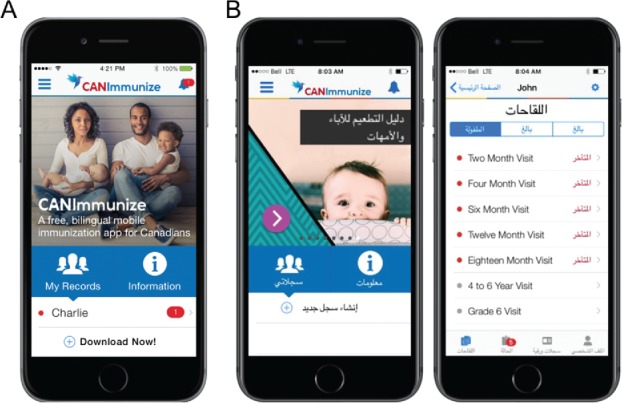
CANImmunize. (A) The CANImmunize app homepage interface; and (B) proposed Arabic version of CANImmunize homepage and record interfaces.
Results and discussion
Demographics
52 individuals were approached to participate in the study, and 50 completed the survey. A summary of participant demographics is provided in Table 1. 23 (46%) respondents were female and 27 (54%) were male. The largest proportion of participants (42%) were between 25-34 years of age. 27 (54%) of the participants were parents, of whom 23 reported having two or more children. The most common region of origin of participants was Sub-Saharan Africa (Eritrea, Ethiopia, Zimbabwe, Burundi, Burkina Faso, Democratic Republic of Congo; 35%), followed by the Middle East (Lebanon, Syria, Iraq; 32%). The most common language spoken was Arabic. 13 (26%) participants reported being multilingual and were familiar with some English or French. Almost half of participants, 24 (48%) required assistance from an interpreter to review the consent form and complete the survey.
Table 1.
Participant demographics.
| Number of respondents, n (%) | |
|---|---|
| Sex | |
| Female | 23 (46%) |
| Male | 27 (54%) |
| Age | |
| Under 20 | 7 (14%) |
| 21–24 | 4 (8%) |
| 25–34 | 21 (42%) |
| 35–44 | 11 (22%) |
| 45–54 | 6 (12%) |
| 55–64 | 1 (2%) |
| Region of origina | |
| North Africa | 8 (16%) |
| Sub-Saharan Africa | 17 (35%) |
| Middle East | 16 (24%) |
| South Asia | 8 (16%) |
| South America | 1 (2%) |
| Period of Arrival to Canada | |
| Prior to January 2016 | 2(4%) |
| January-April 2016 | 4 (8%) |
| May- August 2016 | 9 (18%) |
| September- December 2016 | 17 (35%) |
| January-April 2017 | 16 (32%) |
| May 2017-August 2017 | 1(2%) |
| Missing | 1(2%) |
| Number of Children | |
| None | 22 (44%) |
| 1 | 3 (6%) |
| 2 | 11 (22%) |
| 3 | 5 (10%) |
| >3 | 7 (14%) |
| Missing | 2 (4%) |
| Languages spoken b | |
| Arabic | 21 (42%) |
| English | 2 (4%) |
| French | 3 (6%) |
| Nepali | 3 (6%) |
| Swahili | 3 (6%) |
| Other | 5 (10%) |
| Multilingual | 13 (26%) |
| Highest level of schooling achieved | |
| Grade School | 7 (14%) |
| High School | 22 (44%) |
| College/ University attended but not completed | 7 (14%) |
| College/ University completed | 9 (18%) |
| Missing | 5 (10%) |
North Africa: Libya, Egypt, Sudan; Sub-Saharan Africa: Eritrea, Ethiopia, Zimbabwe, Burundi, Burkina Faso, Democratic Republic of Congo; Middle-East: Lebanon, Syria, Iraq; South Asia: Nepal, Tibet, India, Burma, Bhutan; South America: Colombia.
Participants had the option to select more than one answer to this question; Other: Tibetan, Afar, Spanish, Kirundi.
Immunization history and record keeping
18 (36%) participants self-reported having been vaccinated prior to arrival in Canada. 23 of 27 parents in the study (85%) reported that their children had been vaccinated before coming to Canada (Table 2). 31 (62%) participants indicated that they had previously tracked their vaccinations on paper cards in their home countries, whereas 18 (36%) reported not tracking their vaccinations at all (Table 2).
Table 2.
Immunization history and record keeping.
| Survey Question | Number of respondents, n(%) |
|---|---|
| Were you vaccinated before coming to Canada? | |
| Yes | 18 (36%) |
| No | 23 (46%) |
| I don't know | 4 (8%) |
| Missing | 5 (10%) |
| Were your children vaccinated before coming to Canada? | |
| Yes | 23 (46%) |
| No | 0 (0%) |
| I don't know | 0 (0%) |
| Missing | 2 (4%) |
| 1 Yes/ 1 No | 2 (4%) |
| N/Aa | 23 (46%) |
| How did you track your vaccinations in your home country? | |
| Vaccination Card | 31 (62%) |
| I did not track | 18 (36%) |
| Missing | 1 (2%) |
N/A, not applicable. Individuals without children did not complete this question.
Smartphone and app use
46 (92%) participants owned smartphones, the majority of which were Android devices (66%). Participants reported using a variety of social media platforms, although 86% did not have any health apps installed on their personal devices (Table 3). When asked whether participants would use an app to learn about vaccinations in Canada, 33 (66%) said ‘Yes’. An additional 10% indicated they would use such an app if it were available in their first language (Table 3).
Table 3.
Smartphone use and app acceptability.
| Survey Question | Number of respondents, n(%) |
|---|---|
| Do you have a smartphone? | |
| Yes | 46 (92%) |
| No | 4 (8%) |
| If Yes, what kind? | |
| iPhone | 13 (26%) |
| Android | 33 (66%) |
| Blackberry | 0 (0%) |
| N/Aa | 4 (8%) |
| Do you have health apps on your phone? | |
| Yes | 7 (14%) |
| No | 43 (86%) |
| What social media do you use?b | |
| 41 (82%) | |
| WhatsApp/Viber | 36 (72%) |
| 13 (36%) | |
| YouTube | 25 (50%) |
| Would you use an app to learn about vaccinations in Canada? | |
| Yes | 33 (66%) |
| No | 16 (32%) |
| I don't know | 1 (2%) |
| How will you track your vaccinations in Canada? | |
| CANImmunize | 18 (36%) |
| Vaccination Card | 13 (26%) |
| CANImmunize, Vaccination Card | 13 (26%) |
| I don't know | 5 (10%) |
| Vaccination Card, other vaccination app | 1 (2%) |
| Would you use the app if it were available in your first language? | |
| Yes | 38 (76%) |
| No | 6 (12%) |
| I don't know | 5 (10%) |
| Missing | 1 (2%) |
N/A, not applicable. Participants who did not own a smartphone did not complete this question. bParticipants had the option to select more than one answer to this question.
Discussion
This pilot study provides insight into how a Canadian vaccination tracking app might be tailored to best suit the unique needs of refugee newcomers. Although a high percentage (92%) of the study participants owned smartphones, few were active users of health apps. When asked if they would use an app to learn about vaccinations in Canada, participants indicated their interest in using such a tool, particularly if it were translated into their primary language of communication.
As refugee newcomers undertake often complex travel patterns between states, sub-optimal vaccination rates and outbreaks of vaccine preventable diseases put them at higher risk of acquiring and transmitting infectious diseases. Accurate vaccination records are critical to mitigating these risks, and a compact vaccination tracking app may be of particular use to this population. In one 2015 study of 405 children and young adults seeking asylum in Germany, the authors found that 73% of asylum seekers were up to date with their vaccinations in their home country. However, for 46.4% of individuals, their vaccination records had been lost during migration.10 Up-to-date and completion of vaccination series is critical to mitigating risk of vaccine preventable diseases. Series vaccinations can be easily interrupted due to migration patterns and barriers to accessing healthcare and immunization services. Commonly cited challenges faced by refugees include language barriers, and difficulties navigating the health system in their new host country.11 For these individuals, managing immunization catch-up schedules for their children may only further add to their anxiety. In Canada, differences in catch-up schedules across provinces and territories for children and adults may create additional challenges for newcomers.
The CANImmunize app was designed to empower Canadians to manage their own immunization information. The app permits multi-record vaccination tracking that allows parents or guardians to manage a digital record for dependents along with their own records and includes a recall-reminder system that notifies the account holder of upcoming and overdue vaccinations. Users can easily access expertly-sourced vaccine information, alerts for nearby infectious disease outbreaks, and educational tools for children. Importantly, CANImmunize includes all provincial and territorial adult and pediatric vaccine schedules. Studies have previously shown the positive effect of recall-reminders, such as SMS, on adherence to medical recommendations, including immunization series dose completion.12,13
Our findings suggest that newcomers have the technology and interest in using smartphone tools to help manage their vaccine information. If tailored to the diverse language needs of newcomers, CANImmunize may improve the ease with which newcomers can track their vaccinations after arrival in Canada. A mock-up of an Arabic version of the app is provided in Fig. 1. Notable strengths of this study include the high response rate, with 50 out of 52 participants completing the survey, and our use of a health clinic specifically providing immunization services to Government Assisted Refugees, privately sponsored refugees, and refugee claimants in a city with a large immigrant population. Half of all new immigrants to Canada make their home in Ontario,14 and in Ottawa-Gatineau 235,300 immigrants and refugees represent 19.4% of the city's population.15 Over 4,500 government assisted refugees and privately sponsored refugees were resettled in Ottawa between December 2015 and January 2017.6 In 2016, Citizenship and Immigration Canada granted permanent residency to 296,346 immigrants from nearly 200 countries. Claimants from the Philippines (14%), India (13%), Syria (12%), the People's Republic of China (9%), and Pakistan (4%) were the most common countries of origin.16 The large number of Syrian immigrants to Canada in 2016, and in our study (16%), likely reflects the government's commitment to welcoming Syrian refugees into the country in late 2015.17
The limitations of this study include small sample size and its single centre study design, both of which may limit the generalizability of our findings. The individuals surveyed for this pilot study may not be representative of the demographic make-up of newcomers to the Ottawa, Canada, or elsewhere. Similarly, only refugees were surveyed for this study. Refugees may have different vaccination experiences, as well differences in use of, preferences for, and access to digital technologies compared to other newcomers. Despite these limitations, our needs assessment survey captured data on a diverse array of participants speaking a range of languages, with varied household demographics and countries of origin. Lastly, having a CANImmunize team member administer the survey may have created the potential for response bias on the acceptability of mobile apps.
Future work should seek to determine what vaccine information newcomers require and how this information and the format in which it is presented might differ from the general population. Such information would support the customization of CANImmunize to help bridge knowledge gaps and empower newcomers with control over the management of their health, and that of their children. We specifically plan to examine the value of a translated version of the CANImmunize app as a tool to encourage vaccine tracking, promote awareness about vaccines in Canada and improve on-time vaccination rates. We also intend to evaluate the effectiveness of public health messaging toward this population and adverse event reporting. Further evaluations should examine the impact of the app on healthcare providers and explore eventual integration of the app into public health vaccination databases.
Materials and methods
Study objective
The objective of the study was to inform how an existing mobile vaccination tracking app, CANImmunize, could be tailored to meet the unique needs of newcomers to Canada. This study did not seek to determine the extent of vaccine coverage in newcomers to Canada.
Study setting and design
All government assisted refugees, privately sponsored refugees or refugee claimants attending The Ottawa Newcomer Clinic (ONC) in Ottawa, Canada who were 16 years of age or older were eligible to participate in this study. The ONC provides short-term medical services to government assisted refugees, privately sponsored refugees, and refugee claimants while they resettle and seek permanent family doctors or health-care teams. Bi-weekly vaccination clinics are held at ONC, during which nurse practitioners are available to administer routine vaccinations according to the publicly-funded Ontario childhood and adult vaccination catch-up schedules. In 2015, 1 297 newcomers attended ONC vaccination clinics.
Study recruitment occurred over the course of 10 sessions at ONC between November 2016 and July 2017. Eligible individuals attending the ONC biweekly vaccination clinics were identified to research staff by a nurse practitioner. Research staff discussed the details of the study with eligible participants during the 15-minute waiting period required of individuals after vaccination at the clinic. Eligible individuals were informed of the study requirements and were also provided an overview of the CANImmunize app. Participants were then asked to complete a needs-assessment survey. Consent to data collection was implied upon voluntary completion of the study survey. Interpreters were available to assist participants with reviewing the consent form and interpretation of survey questions.
Needs assessment survey
A 17-question paper-based needs assessment survey was provided to participants. Surveys were available in English, French, Arabic, Nepali, Somali and Swahili. The survey questions covered a range of topics including primary spoken languages, household demographics, self-reported vaccination history prior to arrival in Canada, general smartphone use and openness to using mobile apps for vaccine tracking. Research staff did not have access to participants’ personal health records.
Participants completed and submitted the survey on the same day. The study was approved by the Ottawa Health Sciences Network Research Ethics Board (#20160621–01H).
Disclosure of potential conflicts of interest
The CANImmunize project is funded by the Public Health Agency of Canada. There are no other conflicts of interests to declare. The Canadian Public Health Association was responsible for the development of ImmunizeCA, the predecessor of CANImmunize.
References
- 1.Refugee and Migrant Health: World Health Organization 2017. Available from: http://who.int/migrants/en/.
- 2.Mipatrini D, Stefanelli P, Severoni S, Rezza G. Vaccinations in migrants and refugees: a challenge for European health systems. A systematic review of current scientific evidence. Pathog Glob Health. 2017;111(2):59–68. doi: 10.1080/20477724.2017.1281374. PMID:28165878. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Pottie K, Greenaway C, Feightner J, Welch V, Swinkels H, Rashid M, Narasiah L, Kirmayer LJ, Ueffing E, MacDonald NE, et al.. Evidence-based clinical guidelines for immigrants and refugees. CMAJ. 2011;183(12):E824–925. doi: 10.1503/cmaj.090313. PMID:20530168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Protecting Australia – closing the gap in immunisation for migrants and refugees Proceedings from a stakeholder workshop: NHMRC Centre of Research Excellence in Population Health Research; 2013. [Google Scholar]
- 5.Annual Report to Parliament on Immigration 2016. Government of Canada; 2016. [Google Scholar]
- 6.Canada – Admissions of resettled refugees by province/territory and census metropolitan area (CMA) of intended destination and immigration category, Janary 2015 – November 2017. Immigration, Refugees and Citizenship Canada; 2017. [Google Scholar]
- 7.Get medical services before you leave for Canada: Government of Canada 2017. Available from: http://www.cic.gc.ca/english/refugees/outside/pdms.asp.
- 8.Wilson K, Atkinson KM, Westeinde J. Apps for immunization: Leveraging mobile devices to place the individual at the center of care. Hum Vaccin Immunother. 2015;11(10):2395–9. doi: 10.1080/21645515.2015.1057362. PMID:26110351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Worley W. (2016, May 12) “Syrian woman explains why refugees need smartphones”. Independent. 2016. Available from: http://www.independent.co.uk/news/world/europe/why-do-refugees-have-smartphones-syrian-woman-explains-perfectly-refugee-crisis-a7025356.html. [Google Scholar]
- 10.Rath B, Myles P, Haase K, Jung C, Lusgens M, Nebel T, et al.. Health Needs Assessment of Children and Young Adults Seeking Asylum in Berlin, Germany. Open Forum Infect Dis. 2016;3(Suppl 1):626. [Google Scholar]
- 11.McKeary M, Newbold B. Barriers to care: The challenges for Canadian refugees and their health care providers. J Refug Stud. 2010;23:523–45. doi: 10.1093/jrs/feq038. [DOI] [Google Scholar]
- 12.Atkinson KM, Ducharme R, Westeinde J, Wilson SE, Deeks SL, Pascali D, Wilson K. Vaccination attitudes and mobile readiness: A survey of expectant and new mothers. Hum Vaccin Immunother. 2015;11(4):1039–45. doi: 10.1080/21645515.2015.1009807. PMID:25714388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Liu Q, Abba K, Alejandria MM, Sinclair D, Balanag VM, Lansang MA. Reminder systems to improve patient adherence to tuberculosis clinic appointments for diagnosis and treatment. Cochrane Database Syst Rev. 2014(11):1–59. PMID:25403701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Guiding Newcomers to Ontario: Ontario Canada 2018. Available from: http://www.ontarioimmigration.ca/en/.
- 15.Immigration and Ethnocultural Diversity in Canada National Household Survey. Statistics Canada; 2011. [Google Scholar]
- 16.2017 Annual report to parliament on immigration. Government of Canada; 2017. [Google Scholar]
- 17.Liberals commit to leadership on Syrian refugee crisis: The Liberal Party of Canada 2015. Available from: https://www.liberal.ca/liberals-commit-to-leadership-on-syrian-refugee-crisis/.