

Summary
Introduction
Clostridium difficile (CD) is the most common cause of health-care-associated infectious diarrhea with increasing incidence and severity in recent years. The main cause of hospital’s acquired cross infections can be attributed to incorrect hand hygiene. We described the epidemiology of CD infection (CDI) in a teaching hospital in Southern Italy during a two years surveillance period and evaluated the health-care workers compliance to hand hygiene.
Methods
CDI Incidence rates were calculated as the number of patients with positive C. difficile toxin assay per 10,000 patient-days. Compliance with hand hygiene was the ratio of the number of performed actions to the number of opportunities observed. Approximately 400 Hand Hygiene (HH) opportunities/year /ward were observed. We finally checked out if any correlation could be found.
Results
From January 2015 to December 2016 a total number of 854 CD determinations were performed in patients with clinical symptoms of diarrhea. The search for toxins A and B was positive in 175 cases (21,2%), confirming the diagnosis of CDI. Compliance to hand hygiene was significantly inversely associated with the number of CDIs: the lower the compliance of health-care workers with hand hygiene the higher was the number of cases of CDIs (p = 0.003).
Conclusions
According to our results proper handwashing of health-care workers appears to be a key intervention in interrupting CD cross infections regardless of age and type of department in which the patient is admitted.
Keywords: Clostridium difficile infection, Prevention HAI, HA-CDI, Pediatric HAI, Hands hygiene
Introduction
Clostridium difficile (CD) is the most common cause of health-care associated infectious diarrhea.
It has been estimated that CD infection (CDI) is responsible for over 500,000 enteric infections per year in the United States, the majority of which are hospital acquired [1-3]. Both the incidence and severity of CDI have increased in recent years [4]. At least 7-17% of adult hospitalized patients are colonized by CD, with higher rates observed in elderly long-term patients [5]. Recurrence occurs in 25-33% of patients with primary CDI treated with metronidazole or oral vancomycin. CDI includes a spectrum of clinical features ranging from asymptomatic individuals to CD-associated diarrhea (CDAD) and pseudomembranous colitis, which can lead to fulminant, relapsing, and/or fatal colitis [6, 7]. Risk factors for CDI are 65+ years of age, female gender, previous or concomitant antibiotic exposure, prolonged stay in a health-care facility, immunodeficiency, renal impairment, previous antibiotic exposure and chemotherapy [8-12].
Hand hygiene has also shown to be the most important risk factor in hospital’s acquired infections [13].
As reported by another study, natural history of cases may explain differences in epidemiology of CDIs among hospitals and should be considered to identify the most effective measures to reduce their incidence [14]. Therefore, our study had the following objectives: describe the epidemiology of CDI in a teaching hospital in Southern Italy during two-year-surveillance period and evaluate the percentage of adherence to official hand washing procedures, by hospital care personnel, to determine whether any correlation does exist.
Methods
This study was conducted between January 1, 2015, and December 31, 2016, in Catania University Hospital “G. Rodolico”, a reference teaching and research hospital in Sicily, Italy.
STUDY ENDPOINTS
The primary endpoint was the overall incidence of CDI/10,000 patients days over two years period. Secondary endpoint were: (i) incidence of CDI/10,000 patient days stratified per specialty area, (ii) proportion of children’s cases, (iii) percentage of adherence to hand-washing procedure.
CD INFECTION
For the definition of CDI we have used the following criteria proposed by the European Centre for Disease Prevention and Control (ECDC): diarrheal stool or toxic megacolon and positive laboratory assay for CD toxin A and/or toxin B in stools [15]. We only considered diagnoses of CDI confirmed by laboratory tests performed in the Central Laboratory. We did not consider clinical criteria and pseudomembranous colitis revealed by endoscopy or on a specimen obtained during endoscopy. We have separated the CDI diagnoses observed in outpatient settings.
A case of hospital-acquired CDI (HA-CDI) was defined according to the criteria of the Clostridium difficile Study Group of the European Society of Clinical Microbiology and Infectious Diseases as follows: any patient who developed symptoms of diarrhea at least 48 hours after admission to the hospital (HA-CDI case with hospital onset); any patient who was admitted with symptoms of diarrhea at the hospital with an onset of symptoms in the community within 4 weeks following discharge from the hospital (HA-CDI case with community onset) and patients who had stool samples positive for CD toxin A or B or positive for toxin-producing CD [16].
All stools samples were tested with a two-step algorithm for detecting toxigenic CD: an enzyme immunoassay for glutamate dehydrogenase (GDH) antigen and subsequent enzyme immunoassay for CD toxins A and B. The assay principle combines a two-step enzyme immunoassay sandwich method with final fluorescent detection (ELFA). Laboratory data were collected from the Central Information System.
Epidemiological characteristics of patients (age and gender) and clinical history were collected from the hospital’s digital archives of the patients and then verified in clinical charts. Clinical history was defined as diagnosis according to International Classification Disease (ICD) 9th version, comorbidities, previous hospitalization and length of hospital stay.
Positive cases per GDH were stratified by year and by ward, namely (i) general medicine, (ii) surgery (iii), paediatrics and (iv) intensive care. The incidence of CDI was expressed as the number of CDI cases /10,000 patient days for both overall incidence and stratified per specialty area. Admissions and length of hospital days were extrapolated from the hospital’s admission archives.
HAND WASHING PROCEDURE
We assessed compliance to the hand washing procedures described in World Health Organization (WHO) guidelines [17], while delivering routine care. The WHO guidelines indicate 5 moments of hand’s hygiene in health-care: before touching a patient or before having contact with an object belonging to the healthcare area; before a clean/aseptic procedure; after body fluid exposure; after touching a patient and after touching patient surroundings.
We used WHO Observation Form to directly assess adherence to the protocol in any of the above mentioned five moments by direct visual observation of health-care workers attitude on at least 200 opportunities every six months. Where several indications coincided in a single opportunity, as WHO required, each indication was recorded and the action was then multiplied by the number of indications. The observation data were collected anonymously by the hospital infection control group every six months, in different wards.
According to the WHO manual, we considered appropriate hand washing with water and soap or hand hygiene with alcoholic gel with the exception of dirty or contaminated hands with patients affected by CDI.
Data were imputed in a local database purposely developed.
Compliance was calculated by adding the results of each session and dividing the total number of positive actions by the total number of opportunities.
Results of compliance with hand hygiene through two years period of observation (2015 and 2016) are reported.
STATISTICAL METHODS
To identify the risk (probability) of infection in the patients, we used incidence rate. Incidence rates were calculated as the number of patients with positive CD toxin assay per 10,000 patient-days and were stratified per specialty and per age.
We calculated the compliance rate as the adherence to the procedure in the wards over the total number of opportunities observed in each ward.
We also calculated the overall compliance rate of the different four medical areas. We compared the incidence rate of CDI cases per area with its compliance rate to hand washing procedure.
We performed a covariance analysis in order to see if any difference in mean compliance could explain relative differences in incidence rates.
The degree of linear correlation between the incidence of CDI cases observed and the compliance rates was measured by means Pearson’s statistic.
The significance level was set to p < 0.05.
Results
CDI RATES
From January 2015 to December 2016, a total of 854 CD determinations were performed in patients with clinical symptoms of diarrhea, who were either hospitalized or outpatients (Fig. 1). In 215 samples, glutamate dehydrogenase antigen (GDH) was positive. In these patients, the test for toxin A and B was positive in 175 cases (21.2%), confirming the diagnosis of CDI.
Fig. 1.
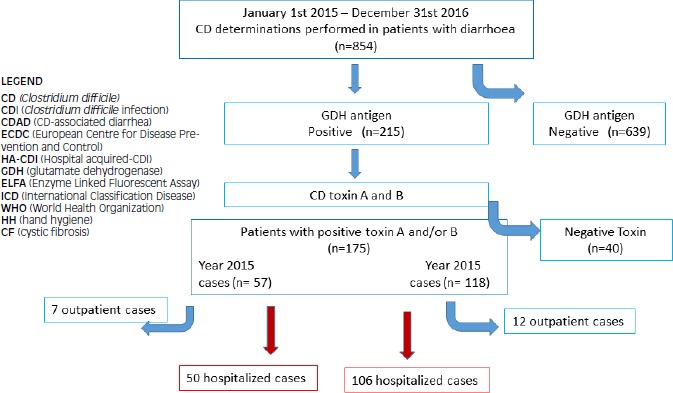
Study flow chart. Description of the path from the stool cultures to the definition of the number of Clostridium difficile infection cases in the different years.
In Table I the number of stool sampled, the percentage of positive exams, the number of inpatient and outpatient cases observed, the incidence of CDI (cases/10,000 patients days) are described. In 2015, 57 positive exams were detected for CD. Fifty cases came from patients hospitalized in 10 wards and seven from outpatients.
Tab. I.
Stool samples tested (numbers and incidence rates) and Clostridium difficile infection (CDI) cases (numbers and incidence rates) per 10000 patients-days per year.
| YEARS | ADMISSIONS | STOOL SAMPLES | CDI Cases | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Inpatients (n) | Outpatients (n) | Overall admissions (n) | Tested (n) | CD positive | % of positive sample | Inpatients (n) | n/10,000 Patients-days | Outpatients (n) | n/10,000 Patients-days | |
| 2015 | 13056 | 6383 | 19439 | 770 | 57 | 7.4 | 50 | 0.1 | 7 | 0.03 |
| 2016 | 12640 | 5688 | 18328 | 825 | 118 | 14.3 | 106 | 0.23 | 12 | 0.05 |
During 2016, we had 118 positive CD tests 106 of which were diagnosed in 11 wards and twelve from outpatients. As can be seen in Table I, the number of CDI cases increased in 2016 despite fewer total admissions. In 2016, there was a 14% increase in the number of tests performed relative to the previous year. The overall incidence was 0.1/10000 patient-days in 2015, and this figure increased to 0.23/10000 patient-days in 2016.
The number of cases in different departments is given in Table II. CDI cases were most frequently diagnosed in general medicine wards. The number of hospital admissions refers only to units in which cases were detected.
Tab. II.
Hospital admissions and incidence of Clostridium difficile infections (CDI) in the different wards per areas during the study period (2015-2016).
| 2015 | 2016 | |||||||
|---|---|---|---|---|---|---|---|---|
| Hospital admissions | No. Of CDI episodes | (% of positive cases) | Incidence/10.000 patient-days | Hospital admissions | No. Of CDI episodes | (% of positive cases) | Incidence/10.000 patient-days | |
| General medicine area | 843 | 36 | 4.27 | 1.16 | 918 | 55 | 5.99 | 1.64 |
| Surgical area | 1705 | 4 | 0.23 | 0.06 | 1443 | 10 | 0.69 | 0.189 |
| Paediatric area | 1141 | 7 | 0.61 | 0.16 | 1866 | 38 | 0.53 | 0.55 |
| Intensive care | 207 | 3 | 1.44 | 0.39 | 219 | 3 | 1.36 | 0.37 |
In Table III we report the number of cases of total CDI divided by age groups. Approximately 28% of all cases involved children aged 0-17 years. Most of these patients exhibited surgical abnormalities of the gastrointestinal tract (25.6%). Only one paediatric patient was affected by cystic fibrosis. Approximately 35% of cases were confirmed in patients over 65 years of age. The other cases were distributed in the middle age group.
Tab. III.
Clostridium difficile Infections (CDI) stratified by area and by age groups.
| CDI n | 0-17 years | 18-65 years | > 65 years | ||
|---|---|---|---|---|---|
| OVERALL | 156 | ||||
| General medicine area | 2015 | 35 | 18 | 17 | |
| 2016 | 55 | 26 | 29 | ||
| Surgical area | 2015 | 4 | 3 | 1 | |
| 2016 | 10 | 3 | 7 | ||
| Paediatric area | 2015 | 8 | 7 | 1 | |
| 2016 | 38 | 34 | 4 | ||
| Intensive care unit | 2015 | 3 | 2 | 1 | |
| 2016 | 3 | 1 | 2 | ||
| 44 (28%) | 58 (37%) | 54 (35%) |
Age, sex, length of stays and outcome of cases are described in Table IV. Since we sampled approximately the same number of males and female we didn’t find any difference between sex as others described [18]. It is particularly relevant the larger length of stay (LOS) in 2016, with an extreme case of 234 days, to which can be probably attributed a greater chance of CDI cases. The mean hospital length of stay of CDI was 27 days in 2015 and 27.6 days in 2016. Two patients relapsed in 2015 and four relapsed in 2016. The patients primarily treated with a cycle of metronidazole were subsequently treated with oral vancomycin. No fidaxomicin treatment was necessary.
Tab. IV.
Age, sex, length of stays and outcomes of Clostridium difficile infections (CDI).
| 2015 | 2016 | |
|---|---|---|
| Sex: - Male | 29 (50.5%) | 55 (47.4%) |
| - Female | 28 (49.5%) | 61 (52.6) |
| Age (years) - Mean | 48.9 | 41.6 |
| - Median | 56 | 48 |
| - Range | 0-91 | 0-96 |
| Length of stays (days) - Mean | 27 | 27.6 |
| - Median | 22 | 16 |
| - Range | 3-144 | 2-234 |
| Recurrence/relapse | 2 (3.6%) | 4 (3.4%) |
| Death | 7 | 2 |
| - Age 0-17 | 0 | 1 |
| - Age 18-65 | 1 | 0 |
| - Age > 65 | 6 | 1 |
| - Ward | 1 ICU | 1 ICU |
| 6 General Medicine area | 1 Paediatric Area |
The C. difficile International Classification of Diseases, ninth version, clinical modification (ICD-9-CM) code 008.45 was assigned as the principal discharge diagnosis only in 9 cases.
The most prevalent comorbidities in older patients were cardiovascular (32.4%) and gastrointestinal (20.6%) diseases.
HAND HYGIENE
Standardized documented activities requiring hand hygiene (HH), according to the WHO protocol, were verified. Approximately 400 HH opportunities/year/ward were observed. In total 5940 circumstances requiring hand hygiene were observed over two years. We calculated the mean compliance rate in each area; we directly observed two wards in the general medicine, surgical and paediatric areas and in the intensive care unit, twice per year. In Table V, we report the results of the percentage of adherence to the application of WHO guidelines on hand hygiene as observed during 2015 and 2016. The survey analysis showed high variability among the wards, ranging from the highest value reached in paediatric units in 2015 (78%) to the lowest value observed in general medicine wards in 2016 (44%).
Tab. V.
Number of CDI, Incidence rates and mean Hand Hygiene Compliance rates stratified by area and by period.
| Areas | CDI cases | Incidence/10000 patient-days | Number of opportunities | Hand hygiene compliance (%) | |
|---|---|---|---|---|---|
| 2015 | General Medicine area 2015 | 35 | 1.13 | 848 | 47 |
| Surgical area 2015 | 4 | 0.06 | 840 | 72 | |
| Paediatric area 2015 | 8 | 0.19 | 828 | 78 | |
| Intensive care unit 2015 | 3 | 0.39 | 492 | 58 | |
| 2016 | General Medicine area 2016 | 55 | 1.64 | 823 | 44 |
| Surgical area 2016 | 10 | 0.189 | 840 | 65 | |
| Paediatric area 2016 | 38 | 0.55 | 830 | 65 | |
| Intensive care unit 2016 | 3 | 0.37 | 457 | 60 |
Results from covariance analysis performed on data showed no significant difference in mean incidence rate between 2015 and 2016 (p = 0,15) while common significant linear correlation was conversely found between adherence to hand washing procedure and incidence rates within medical areas. Negative linear correlation coefficient was -0.8911 (p = 0.003) showing that the poorer adherence to the procedure the greater the incidence rate (Fig. 2).
Fig. 2.
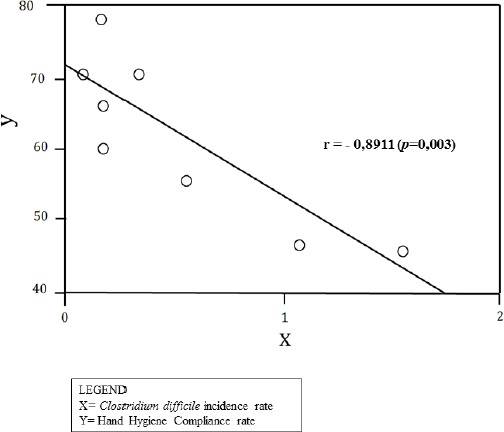
Linear correlation between Clostridium difficile incidence rates and Hand Hygiene compliance rates.
Discussion
CD is the most important cause of healthcare-associated diarrhea in both normal and immunocompromised hosts and is increasingly important as a community pathogen [19]. It has been found to be the major aetiologic agent of antibiotic-associated pseudomembranous colitis, a clinically defined syndrome associated with a recent history of antibiotic use in which pseudomembranous nodules or plaques can be found in the distal and sigmoid colon and rectum. If unrecognized or untreated, this disease can be fatal.
Our increase in CDI cases is consistent with that recently reported in the literature [20, 21]. We argue that since tests were performed only in patients with gastrointestinal symptoms of diarrhea, the greater number of tests performed in 2016 relates to an increased amount of positive cases founded.
As shown in Table III, patients hospitalized in internal medicine wards were at higher risk for CDI and CDI incidence increased with age over 65, similarly reported in other studies [14, 20, 21]. Older patients have more comorbidities and are hospitalized more frequently than younger patients [22]. In our study, the most prevalent comorbidities were cardiovascular (32.4%) and gastrointestinal (20.6%) conditions.
Interestingly we found a high incidence of positive cases (28%) in patients under 18 years old. Our 44 diagnoses referred to children that had diarrhea and diseases involving malformations of the digestive system. CD colonization of health individuals is associated with changes in distal gut microbial composition [23]. This phenomenon is much more frequent in paediatric patients, especially in infants. CDI is a relatively uncommon but costly complication after paediatric operative procedures [24]. Infants and paediatric patients with cystic fibrosis (CF) have shown to be asymptomatic carriers of toxigenic CD with reported CD colonization rates as high as 50% in infants and from 22 to 46% in the others [25-27]. However, despite this high rate of colonization, the occurrence of CDI in CF remains rare.
The large number of cases in paediatric subjects in our study is probably due to the high concentration of children with severe connatural surgical pathologies treated in our paediatric surgery or to children treated in our regional centers for diagnosis of cystic fibrosis and for the treatment of oncology disease in paediatric age.
The mean LOS is roughly the same in the two years with a large variability from one case to another. Hospital LOS has a double relationship with CDI because its increase is a well-known risk factor for cross-CDI and patients with CDI tend to stay in the hospital longer [28]. The permanence of a patient colonized by CD is a risk factor for nosocomial infection, which can be easily transmitted by the improperly washed hands of the assisting staff or relatives who are unidentified disseminators of the germ itself.
As can be seen in Table I the number of positive tests in 2016 were more than twice those positive in 2015, while incidence rates increased accordingly in inpatients, more than those occurred in outpatients. This confirm the role of proper hand-washing in CD cross-infections, as far as most health care-associated infections are preventable with good hand hygiene. It means cleaning hands at the right time and in the right way. Hand hygiene is a key intervention in interrupting transmission between patients, health care personnel and visitors [29, 30].
In our hospital, we have regular monitoring and evaluation quality protocol to control hand-washing hospital procedure. We perform hand washing following the five times for hand hygiene set by the WHO, as previously cited.
Our results gave us knowledge of how health-care workers perform hand hygiene. The data confirm the low compliance to hand hygiene practices of healthcare workers: no department reached 80% compliance, which is the limit recommended by the WHO. Not surprisingly we found a reverse correlation between the number of CDI cases recorded and the percentage of adherence to hand washing: the lower the compliance with HH, the higher the number of CDI.
Since this practice remains well below WHO recommendations, continual efforts are required to reach the optima targeted goal to prevent HA- CDI. A better knowledge of the importance of hand hygiene remains an effective health care-associated infection control intervention. Nevertheless, other measures for infection control must be reminded such as isolation of infected patients, use of gloves, gowns and chemical agents for environmental disinfection. Hydrogen peroxide vapours for terminal decontamination has been proven to be effective against CD, as has been recently reported [31-33].
Finally, our analysis suffers from some limitations. Firstly, we considered only diagnoses of CD infection carried out by laboratory tests. For diagnosis, we used EIAs that are easy and fast to perform but with a sensitivity ranging from 63% to 99%; thus, false-negative results could occur. Moreover, we did not consider pseudomembranous colitis revealed by endoscopy or on a specimen obtained during endoscopy. This decision may have resulted in missed cases.
Secondly, our study was a single centre study in a teaching hospital and results may not be reproducible in different contexts. HH observations were carried out by trained staff twice a year, a greater number of observations or video recordings of the actions might lead to different results.
Conclusions
CD is a well-known cause of hospital-acquired infectious diarrhea with prolonged hospitalizations, increasing patient morbidity and healthcare costs [34, 35]. Clinicians should consider a diagnosis of CDI in patients with severe diarrhea. Early recognition of CD colonization may help to prevent the spread of HA-CDI and the risk of transmission to non-infected patients or healthcare workers.
To reduce the incidence of CDI, it is imperative to be aware of at-risk population, which might be different in general or specialized hospitals. The large number of cases in paediatric subjects in our study is probably due to the high concentration of children with severe connatural surgical pathologies treated in our paediatric surgery centre and children who were treated in our regional reference centres for cystic fibrosis or oncology pathology.
Given the results of our survey, we propose that screening is performed in all patients admitted to the Intensive Care Unit, in all immunosuppressed patients over 65 years of age with the described comorbidities and in paediatric patients with gastrointestinal abnormalities or tumours. Screening should be performed by detecting GDH in stool in order to select colonized patients and prevent outbreaks.
Because of the difficulties associated with the isolation of infected patients in a single room with personal bathrooms, proper hand-washing remains a key intervention in interrupting transmission between patients, health care personnel and visitors.
Continuous surveillance is required to determine trends and verify whether more toxigenic strains have an increasing impact in the community and in a hospital setting [36].
Further studies are required to verify whether the proposed measures might restrict the spread of infections due to secondary outbreaks.
Acknowledgments
All authors report no conflicts of a financial, personal or any other nature that could affect or bias this article.
Footnotes
All authors report no potential conflicts of interest relevant to this article.
Financial support: None reported.
Funding source: None
Author’s contribution
RR conceived, designed the research, wrote the manuscript, GG performed the tables and data quality control, LL provided statistical data and the final correction of the manuscript, SA performed microbiological analysis,RS collected data, LVM collected data, MS performed the literature review, MM coordinated the research.
All Authors revised the manuscript and gave their contribution to improve the paper.
All Authors read and approved the final manuscript.
References
- [1].Lessa FC, Mu Y, Bamberg WM, Beldavs ZG, Dumyati GK, Dunn JR, Farley MM, Holzbauer SM, Meek JI, Phipps EC, Wilson LE, Winston LG, Cohen JA, Limbago BM, Fridkin SK, Gerding DN, McDonald LC. Burden of Clostridium difficile infection in the United States N Engl J Med 2015;372:825-34. doi: 10.1056/NEJMoa1408913. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Heinlen L, Ballard JD. Clostridium difficile Infection. Am J Med Sci 2010;340:247-52. doi:10.1097/MAJ.0b013e3181e939d8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Zhao S, Ghose-Paul C, Zhang K, Tzipori S, Sun X. Immune-based treatment and prevention of Clostridium difficile infection. Hum Vaccin Immunother 2014;10:3522-30. doi: 10.4161/21645515.2014.980193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Cohen SH, Gerding DN, Johnson S, Kelly CP, Loo VG, McDonald LC, Pepin J, Wilcox MH; Society for Healthcare Epidemiology of America; Infectious Diseases Society of America. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the society for healthcare epidemiology of America (SHEA) and the infectious diseases society of America (IDSA). Infect Control Hosp Epidemiol 2010;31: 431-55. doi: 10.1086/651706. [DOI] [PubMed] [Google Scholar]
- [5].Depestel DD, Aronoff DM. Epidemiology of Clostridium difficile infection. J Pharm Pract 2013;26:464-75. doi: 10.1177/0897190013499521 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Poutanen SM, Simor AE. Clostridium difficile-associated diarrhea in adults. CMAJ 2004;171:51-8. doi:10.1503/cmaj.1031189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Vaishnavi C. Clinical spectrum & pathogenesis of Clostridium difficile associated diseases. Indian J Med Res 2010;131:487-99. [PubMed] [Google Scholar]
- [8].Patel UC, Wieczorkiewicz JT, Tuazon J. Evaluation of advanced age as a risk factor for severe Clostridium difficile infection. Journal of Clinical Gerontology and Geriatrics 2016;7:12-6. doi.org/10.1016/j.jcgg.2015.06.003 [Google Scholar]
- [9].McFarland LV. Renewed interest in a difficult disease: Clostridium difficile infections - epidemiology and current treatment strategies. Curr Opin Gastroenterol 2009;25:24-35. doi: 10.1097/MOG.0b013e32831da7c4 [DOI] [PubMed] [Google Scholar]
- [10].Hu MY, Katchar K, Kyne L, Maroo S, Tummala S, Dreisbach V, Kelly CP. Prospective derivation and validation of a clinical prediction rule for recurrent Clostridium difficile infection. Gastroenterology 2009;136:1206-14. doi: 10.1053/j.gastro.2008.12.038 [DOI] [PubMed] [Google Scholar]
- [11].Na X, Martin A J, Sethi S, Kyne L, Garey KW, Flores SW, Hu M, Shah DN, Shields K, Leffler DA, Kelly C P. A Multi-center prospective derivation and validation of a clinical prediction tool for severe Clostridium difficile Infection. PLoS ONE 2015;10:e0123405 doi.org/10.1371/journal.pone.0123405 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Eze P, Balsells E, Kyaw MH, Nair H. Risk factors for Clostridium difficile infections - an overview of the evidence base and challenges in data synthesis. J Glob Health 2017;7:010417 doi:10.7189/jogh.07.010417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Squeri R, Genovese C, Palamara MA, Trimarchi G, La Fauci V. “Clean care is safer care”: correct handwashing in the prevention of healthcare associated infections. Ann Ig 2016;28:409-415. doi: 10.7416/ai.2016.2123. [DOI] [PubMed] [Google Scholar]
- [14].Alicino C, Giacobbe DR, Durando P, Bellina D, DI Bella AM, Paganino C, Del Bono V, Viscoli C, Icardi G, Orsi A. Increasing incidence of Clostridium difficile infections: results from a 5-year retrospective study in a large teaching hospital in the Italian region with the oldest population. Epidemiol Infect 2016; 144:2517-26. doi: 10.1017/S0950268816000935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].European Centre for Disease Prevention and Control. European surveillance of Clostridium difficle infections. Surveillance protocol version 2.3. Stockholm: ECDC, 2017. Available at: https://ecdc.europa.eu/en/publications-data/european-surveillance-clostridium-difficile-infections-surveillance-protocol-1 [Google Scholar]
- [16].Bauer MP, Kuijper EJ, Van Dissel JTEuropean Society of Clinical, M., & Infectious, D. European Society of Clinical Microbiology and Infectious Diseases (ESCMID): treatment guidance document for Clostridium difficile infection (CDI). Clin Microbiol Infect 2009;15:1067-79. doi: 10.1111/j.1469-0691.2009.03099. [DOI] [PubMed] [Google Scholar]
- [17].World Health Organization. Hand Hygiene Technical Reference Manual. Geneva: WHO; 2009. Available at: http://apps.who.int/iris/bitstream/handle/10665/44196/9789241598606_eng.pdf?sequence=1 [Google Scholar]
- [18].Chen Y, Glass K, Liu B, Korda RJ, Riley TV, Kirk MD. Burden of Clostridium difficile infection: Associated hospitalization in a cohort of middle-aged and older adults. Am J Infect Control 2017; doi: 10.1016/j.ajic.2016.12.006. [DOI] [PubMed] [Google Scholar]
- [19].Bauer MP, Notermans DW, Van Benthem BH, Brazier JS, Wilcox MH, Rupnik M, Monnet DL, Van Dissel JT, Kuijper EJ. ECDIS Study Group. Clostridium difficile infection in Europe: a hospital-based survey. Lancet 2011;377:63-73. doi: 10.1016/S0140-6736(10)61266-4. [DOI] [PubMed] [Google Scholar]
- [20].Cioni G, Viale P, Frasson S, Cipollini F, Menichetti F, Petrosillo N, Brunati S, Spigaglia P, Vismara C, Bielli A, Barbanti F, Landini G, Panigada G, Gussoni G, Bonizzoni E, Gesu GP; Epidemiology and outcome of Clostridium difficile infections in patients hospitalized in Internal Medicine: findings from the nationwide FADOI-PRACTICE study. BMC Infect Dis 2016; 16:656 doi.org/10.1186/s12879-016-1961-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Visconti V, Brunetti G, Cuomo MR, Giordano A, Raponi G. Nosocomial-acquired and community-onset Clostridium difficile infection at an academic hospital in Italy: Epidemiology, recurrences and toxin genes distribution. J Infect Chemother 2017; 23:763-768. doi: 10.1016/j.jiac.2017.08.002. [DOI] [PubMed] [Google Scholar]
- [22].Mamic P, Heidenreich PA, Hedlin H, Tennakoon L, Staudenmayer KL. Hospitalized patients with heart failure and common bacterial infections: a nationwide analysis of concomitant Clostridium difficile infection rates and in-hospital mortality. J Card Fail 2016;22:891-900. doi: 10.1016/j.cardfail.2016.06.005. [DOI] [PubMed] [Google Scholar]
- [23].Rea MC, O’Sullivan O, Shanahan F, O’Toole PW, Stanton C, Ross RP, Hill C. Clostridium difficile carriage in elderly subjects and associated changes in the intestinal microbiota. J Clin Microbiol 2012;50:867-75. doi: 10.1128/JCM.05176-11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Kulaylat AN, Rocourt DV, Podany AB, Engbrecht BW, Twilley M, Santos MC, Cilley RE, Hollenbeak CS, Dillon PW. Costs of Clostridium difficile infection in pediatric operations: a propensity score-matching analysis. Surgery 2017;161:1376-1386. doi: 10.1016/j.surg.2016.10.020. [DOI] [PubMed] [Google Scholar]
- [25].Tamma PD, Sandora TJ. Clostridium difficile infection in children: current state and unanswered questions. J Pediatric Infect Dis Soc 2012;1:230-243. doi:10.1093/jpids/pis071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Piccolo F, Tai AS, Ee H, Mulrennan S, Bell S, Ryan G. Clostridium difficile infection in cystic fibrosis: an uncommon but life-threatening complication. Respirol Case Rep 2017; 5(1):e00204 doi:10.1002/rcr2.204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Com G, Cetin N, O’Brien C.E. Complicated Clostridium difficile colitis in children with cystic fibrosis: Association with gastric acid suppression? J Cyst Fibros 2014;13: 37-42. doi.org/10.1016/j.jcf.2013.08.005 [DOI] [PubMed] [Google Scholar]
- [28].Roncarati G, Dallolio L, Leoni E, Panico M, Zanni A, Farruggia P. Surveillance of Clostridium difficile infections: results from a six-year retrospective study in nine hospitals of a North Italian Local Health Authority. Int J Environ Res Public Health 2017;14(1). pii: E61. doi: 10.3390/ijerph14010061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Pittet D, Hugonnet S, Harbarth S, Mourouga P, Sauvan V, Touveneau S, Perneger TV. Effectiveness of a hospital-wide programme to improve compliance with hand hygiene. Infection Control Programme. Lancet 2000;356:1307-12. PMID: 11073019. doi.org/10.1016/S0140-6736(00)02814-2. [DOI] [PubMed] [Google Scholar]
- [30].Sickbert-Bennett EE, DiBiase LM, Willis TM, Wolak ES, Weber DJ, Rutala WA. Reduction of healthcare-associated infections by exceeding high compliance with hand hygiene practices. Emerg Infect Dis 2016;22:1628-30. doi: 10.3201/eid2209.151440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Horn K, Otter JA. Hydrogen peroxide vapor room disinfection and hand hygiene improvements reduce Clostridium difficile infection, methicillin-resistant Staphylococcus aureus, vancomycin-resistant enterococci, and extended-spectrum beta-lactamase. Am J Infect Control 2015;43:1354-6. doi: 10.1016/j.ajic.2015.06.029. [DOI] [PubMed] [Google Scholar]
- [32].Ragusa R, Lombardo A, Bruno A, Sciacca A, Lupo L. Environmental biodecontamination: when a procedure performed by the nursing staff has an economic impact in ICU rooms. J Nurs Care 2016;5:355 doi: 10.4172/2167-1168.1000355. [Google Scholar]
- [33].Castaldi S, Ragusa R. HTA applicato all’Igiene ospedaliera. In book: Health Technology Assessment and Public Health Chapter: 13 Publisher: J Prev Med Hyg 2017;58,3 (Suppl. 1): E71-E78 EID: 2-s2.0-85033578796. [Google Scholar]
- [34].Wiegand PN, Nathwani D, Wilcox MH, Stephens J, Shelbaya A, Haider S. Clinical and economic burden of Clostridium difficile infection in Europe: a systematic review of healthcare-facility-acquired infection. J Hosp Infect 2012;81:1-14. doi: 10.1016/j.jhin.2012.02.004. [DOI] [PubMed] [Google Scholar]
- [35].Desai K, Gupta SB, Dubberke ER, Prabhu VS, Browne C, Mast TC. Epidemiological and economic burden of Clostridium difficile in the United States: estimates from a modeling approach. BMC Infect Dis 2016;16:303 doi: 10.1186/s12879-016-1610-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Jones AM, Kuijper EJ, Wilcox MH. Clostridium difficile: a European perspective. J Infect 2013;66(2):115-128. doi: 10.1016/j.jinf.2012.10.019. [DOI] [PubMed] [Google Scholar]