

Abstract
Background:
Glioblastoma (GBM) is a terminal illness and associated with poor prognosis. Brain cancer creates significant traumatic effects including death and dying fears not only on patients but also in Asia's tightly knitted families. Very few studies made attempt to elicit the death and dying issues among brain cancer patients. Therefore, the study aimed to explore the patient's perspectives on death and dying among GBM patients during hospitalization.
Methodology:
The study used qualitative approach. Purposive sampling was used to enroll 31 consented patients for in depth interviews. The in-depth interviews were guided by pre-designed open ended guidelines and took 45 min to 1 h. All interviews were conducted in the private room in the hospital. Interviews were manually documented soon after the interview. Thematic analysis was used to generate themes. R (QOL) software was used for data analysis.
Results:
Four themes were emerged from the analysis; (i). Understanding about illness (ii). Personal views and feelings on death and dying (iii). Coping with fear of death and dying (iv). Need for early preparation to face death and dying fears.
Conclusion:
Psychosocial interventions on early death preparation programs are recommended for GBM patients in the in-patient care. Yet, it should be handled carefully and sensitively, otherwise, it creates more psychological and emotional harm than the illness per se.
Keywords: Death and dying, glioblastoma, perspectives
INTRODUCTION
Glioblastoma (GBM) is a terminal illness and is associated with poor prognosis.[1,2,3] Brain cancer creates significant traumatic effects not only on patients but also in Asia's tightly knitted families.[3,4] The psychosocial needs of the terminally ill people are now matter of concern, especially among GBM patients.[4] Psychosocial manifestations such as altered decision-making, anxiety about unfinished business, withdrawal, decreased socialization, fear of loneliness, pain, meaninglessness in one's life, helplessness, and fear of death increase the severity and psychiatric comorbidity such as depression, anxiety, stress, loss of independence, loss of self, and loss of relationships.[5,6,7] Studies also show that mental, spiritual, and social needs of patients and their family members mainly death and dying issue are not explored in detail.[7] Further, coping with psychosocial, spiritual and existential, and end-of-life issues are difficult for cancer patients.[8] End-of-life care (EOL) is the term used currently for issues related to death and dying as well as services provided to address physical and psychosocial needs of terminally ill people and their family members. EOL goal is to provide comfort and supportive care during the dying process, improve the possible better quality of life, and ensure a dignified death in the last phase of life.[7]
Talking about death with a terminally ill person or trying to know about death experiences of family members has been seen as taboo; challenging and ethical dilemmas restricted professionals to elicit the issues around death and dying.[9,10,12,13] Each person's attitude is unique on death and dying. It depends on multiple factors such as age, gender, culture, and disease.[8] GBM illness creates fear of death among brain cancer patients. On the other hand, researchers had given less opportunities to discuss about GBM patients’ personal experiences, perceptions, and attitudes on death.[11,12] Therefore, the current study aimed to explore the death- and dying-related concerns among GBM patients during in-patient care.
METHODOLOGY
The study adopted the qualitative approach. A total of 31 respondents were recruited from the inpatient care in the Department of Neurosurgery, National Institute of Mental Health and Neuro Sciences, Bengaluru. Patients suffering from GBM were invited to take part in the in-depth interviews after confirming the diagnosis by neuropathologist. Adult participants who expressed willingness to share their views on death and dying voluntarily, aged between >18 and < 60 years, with no history of cognitive deficits, and who were able to communicate in Telugu, Kannada, and English were recruited in the study. Nine respondents were not interested to share their views on death and dying and did not give consent, thus excluded from the study.
The data were collected in one-to-one interviews in a separate room by the primary author. These interviews were guided by open-ended questions on death and dying. The interview guide asked general questions on understanding about illness and specific questions such as personal views on death and dying. For example, could you tell me what do you understand about your illness? What are your personal views on death and dying in general? How did you feel whenever you hear the word “Death?” What steps do you take to overcome death- and dying-related fears and thoughts whenever you get in mind? What information do you need to face the fear of death and dying in day-to-day life? The above guidelines were used to ensure the data consistency across all participants. Each interview lasted from 45 min to 1 h.
Before the interview, primary author spent enough time to establish rapport with participant and checked whether participant was comfortable to share their views on death and dying. Then, interested participants were invited to take part in the in-depth interviews. Interviews were conducted in day-to-day conversational style and documented in the narrative form soon after the interview. Interviews conducted in Telugu and Kannada languages were translated into English. Observation, filed notes, empathy, and prolonged engagement techniques were used to bring the context and ensure the data accuracy. For qualitative data analysis R software (QOL, 2012) 3.0.2 was used. The thematic analysis was used for qualitative data analysis. The methodological details were already reported in earlier study[13] Though participants shared their views on death and dying voluntarily, a 20-min debriefing also carried out to prevent the further death anxiety and fears among participants. The oral and written informed consent was obtained from study participants before the study. The ethical approval was sought from Institute ethics committee (No. NIMH/DO/SUB-COMMITTEE/2012; on 15-11-2012).
RESULTS
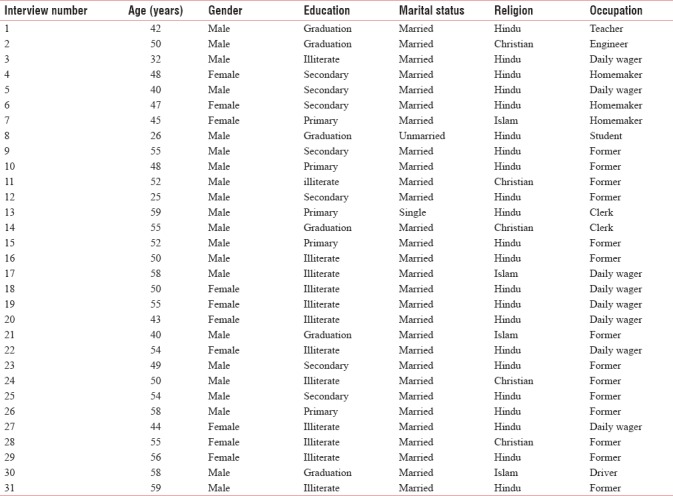
Thirty-one GBM patients (male n = 21, female n = 10) participated in the study. They all admitted for surgical interventions at neurosurgery department. Table 1 shows the demographic characteristics of GBM patients.
Table 1.
Demographic characteristics of glioblastoma patients
The emergent theme were
Understanding about illness
Personal views and feelings on death and dying
Coping with fear of death and dying
Need for early preparation to face death and dying fears.
Understanding about illness
The results reported that GBM patients had poor understanding about their illness in terms of causes, consequences, prognosis, nature of illness, treatment regimen required, and its side effects. Besides that, they expressed their desire to know complete information on GBM. This theme was evident from the following illustrations:
“I know, I am admitted for brain tumour treatment as informed by treating doctor. Apart from that, I do not know in detail; what is brain tumour? Why does it come to me?. I do not have any bad habits like smoking and drinking. I want to know about my illness. Even my relatives divert on the same whenever I ask them” (Male 1, Male 29, Male 22).
“What I am aware of is, I have been suffering with brain cancer. I had already undergone surgery, radiation, and chemotherapy once but till today, I do not know, why I should take these many treatments for my illness” (Male 15, Male 31, Female 27).
Personal views and feelings on death and dying
Talking about death and dying and even sharing views on the same was not easy for many participants. Their first reaction was fear, silence, and sadness. Few of the participants had experienced worry, nervous, anxious, and uncertain about their future. Many participants felt that death was not inevitable in life. Very few participants reported that terminal illness creates financial crisis and creates burden on family members. Hence, they viewed that death was inevitable; however, they want to die in their home.
“I feel sad… sometimes, I get fear whenever I think about my death and even future of my family members” (Male 2, Female 4, Male 11, Female 27).
“I may die soon, I am not worried for myself. I am thinking of my children and wife. Who will look after them if I die…. I am worried more for them….(Cried…….)… (After long breath)…. It's better to die than creating burden to wife and children” (Female 22, Male 30, Female 29).
“I feel worried, not only me everyone will feel fear…worried…if they know, they are dying….(…pause…. silence……for….4 min…. tears…. observed in the eyes….). I would like to die at home, if I die with my illness” (Female 27, Male 31, Female 19, Male 3).
Coping with fears of death and dying
Another theme derived from analysis was coping with fears of death and dying. Participants felt that whenever they think about their illness, death and dying thoughts also will enter into their mind. They use spirituality in terms of prayer, chanting mantras, presence and availability of family members, friends, significant others, and fulfilling their day-to-day wishes help them coping with death and dying thoughts. They also felt that they have to be respected rather than treating them as sick persons. Participants reported in their own words:
“I get death-related thoughts whenever I am alone. That time, I pray to the God and chant Mantras. Sometimes, I talk to my wife to get rid of those thoughts” (Male 1, Female 4, Male 11, Male 14).
“I know I may die soon with my brain cancer. My family is good support for me. They always be with me and help me in day–to-day activities. I call and talk to them and divert my death-related thoughts” (Male 10, Male 15, Female 19, Male 21).
“My family members have to consider me as I am before my illness. They should not treat me as ill person. I ask them only one cigarette in a day, I like cigarettes…(smiled….)…nothing more I need from them during my last days.”
Need for early preparation death and dying fears
Participants had expressed need for early preparation on recurrence of illness and early symptoms of death and dying. They felt that the early preparation on illness recurrence, deterioration, and death would help participants to complete the unfinished jobs such as children's marriage, settling, and distribution of property.
“I have been suffering with brain cancer for more than 3 years. I know, I am not going to live for more years. This, I came to know after reading about GBM in the internet. I feel sad because my children are not yet married… (cried)…. I have not finished father duties and responsibilities. I feel someone should talk to us during hospitalisation” (Male 21, Male 23).
“It would be good if doctors provide information on recurrence of brain tumour and early symptoms of approaching death. Not only for me even for others, and they are many people like me in the hospital. They do not know anything about their illness” (Male 1, Female 4, Male 9, Male 31).
DISCUSSION
Conscious and careful effort was made to find out the personal views of GBM patients on death and dying during hospitalization. Very few studies had given attention to elicit and discuss the death- and dying-related issues of GBM patients in the Indian context. In this connection, the current study holds the significance. There is a rapid decline in survival rates after diagnosis of GBM. GBM patients reach end-of-life phase soon when compared to other cancer patients.[2] Our study findings revealed that understanding about illness among GBM patients is poor. Psychosocial needs such as informational, educational, emotional, practical, and unmet needs are more in high-grade gliomas. One of the needs was fears related to recurrence of illness and death.[13,14]
The study results further depicted that talking about sensitive issues such as death and dying was inevitable among GBM patients. Death is no longer a taboo – God is. Their first reaction of participants after hearing the word GBM caused death was fear, silence, sadness, worry, nervous, anxious, and uncertainty. Hearing cancer diagnosis is a life-changing if not a life-threatening event. Initial reaction is fear of death creases the anxiety, stress, sadness, grief, mourn and fears accelerate in patients suffering with malignant brain cancer. Studies also highlighted that death is associated with psychological threat.[1,15,16] Meaning ascribed to the death, personal experiences, individual characteristics, contextual and cultural factors, social interactions, constant fear of death, and process of dying has severe interfere with quality of life in people who approaches death or in EOL.[17]
The study also revealed that GBM patients made attempts to cope with death and dying thoughts by being spiritual; persistent interaction, receiving respect from family members, and fulfilling day-to-day desires were main sources of coping. However, coping with terminal and malignant illness was challenging. Earlier studies reported that prior abilities no longer exist to cope after brain cancer diagnosis.[6] Yet, availability of support, family resources, personal resilience, and emotional support can help GBM patients to cope well with disease.[18]
The study highlighted the need for early preparation on death and dying for GBM patients during hospitalization. Preparing the early signs of recurrence and death, relief from pain and suffering, and how to have happy death is equally important. This finding goes in line with previous study reports that discussing with death-related issues with patients and caregivers are helpful which minimizes the fears related to death, reduces death anxiety, and maintains the self-regulation of life. Hence, death and dying preparation programs are need of the hour for GBM patients in inpatient care; yet, opportunities for discussion on the same are fewer for brain cancer patients.[11,12] In spite of great fears within oneself, cancer patients have expressed greater inner strength and maintained hope irrespective of devastating experience caused by malignant brain tumors.[19]
Limitation of the study
The study had few limitations. The sample was selected purposively, and interviews were not audio recorded. People from various socioeconomic and religious backgrounds participated in the study. Intensive and structured psychosocial interventions were not provided for highly distressed people. Therefore, interpretation of study findings was cautioned to other settings.
CLINICAL IMPLICATIONS AND CONCLUSION
The study observed that discussing issues related to death and dying was challenging in the initial phase. It manifested tears and stress among GBM patients. Many patients were willing to share their views on death and dying. However, it should be handled carefully and sensitively; otherwise, it creates more psychological and emotional harm than the illness per se Therefore, psychosocial interventions on early preparation on recurrence, death and dying, fears and anxiety associated with death and dying, and coping with death and dying thoughts are recommended for brain tumor patients, in particular GBM patients in the inpatient setting.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We wish to express deep gratitude to all GBM patients for actively participating in the study.
REFERENCES
- 1.Huilgol NG. Travails of the terminally ill and dying with cancer. J Cancer Res Ther. 2015;11:255–6. doi: 10.4103/0973-1482.159980. [DOI] [PubMed] [Google Scholar]
- 2.Davis FG, McCarthy BJ, Freels S, Kupelian V, Bondy ML. The conditional probability of survival of patients with primary malignant brain tumors: Surveillance, epidemiology, and end results (SEER) data. Cancer. 1999;85:485–91. [PubMed] [Google Scholar]
- 3.Armstrong TS. Head's up on the treatment of malignant glioma patients. Oncol Nurs Forum. 2009;36:E232–40. doi: 10.1188/09.ONF.E232-E240. [DOI] [PubMed] [Google Scholar]
- 4.Mezue WC, Draper P, Watson R, Mathew BG. Caring for patients with brain tumor: The patient and care giver perspectives. Niger J Clin Pract. 2011;14:368–72. doi: 10.4103/1119-3077.86786. [DOI] [PubMed] [Google Scholar]
- 5.Barre VP, Padmaja G, Saxena RK, Rana S. Impact of medical intervention on stress and quality of life in patients with cancer. Indian J Palliat Care. 2015;21:203–8. doi: 10.4103/0973-1075.156503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lucas MR. Psychosocial implications for the patient with a high-grade glioma. J Neurosci Nurs. 2010;42:104–8. doi: 10.1097/jnn.0b013e3181ce5a34. [DOI] [PubMed] [Google Scholar]
- 7.Zamanzadeh V, Jasemi M, Valizadeh L, Keogh B, Taleghani F. Effective factors in providing holistic care: A qualitative study. Indian J Palliat Care. 2015;21:214–24. doi: 10.4103/0973-1075.156506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Aydogan U, Doganer YC, Komurcu S, Ozturk B, Ozet A, Saglam K, et al. Coping attitudes of cancer patients and their caregivers and quality of life of caregivers. Indian J Palliat Care. 2016;22:150–6. doi: 10.4103/0973-1075.179598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Shrivastava SR, Shrivastava PS, Ramasamy J. Palliative care: An integral component of human right to health. Int J Prev Med. 2016;7:15. doi: 10.4103/2008-7802.173916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Biswas M. Living well till death. J Cancer Res Ther. 2015;11:257–8. doi: 10.4103/0973-1482.159982. [DOI] [PubMed] [Google Scholar]
- 11.Lipsman N, Skanda A, Kimmelman J, Bernstein M. The attitudes of brain cancer patients and their caregivers towards death and dying: A qualitative study. BMC Palliat Care. 2007;6:7. doi: 10.1186/1472-684X-6-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Jeon HW, Kim MH, Yoon JA. Death perception, death preparation and need for death educational program of the elderly. [Last accessed on 2017 Jan 10];Indian J Sci Technol. 2015 8:6–7. Available from: http://www.52.172.159.94/index.php/indjst/article/view/80275 . [Google Scholar]
- 13.Birudu R, Pandey P, Arivazhagan A, Krishna Reddy N, Santosh V. Qualitative Study on Psychosocial Needs of Persons with Glioblastoma in India. 2014;1:72–80. www.rsisinternational.org/IJRSI.html . [Google Scholar]
- 14.Halkett GK, Lobb EA, Rogers MM, Shaw T, Long AP, Wheeler HR, et al. Predictors of distress and poorer quality of life in high grade glioma patients. Patient Educ Couns. 2015;98:525–32. doi: 10.1016/j.pec.2015.01.002. [DOI] [PubMed] [Google Scholar]
- 15.Airaksinen E, Larsson M, Lundberg I, Forsell Y. Cognitive functions in depressive disorders: Evidence from a population-based study. Psychol Med. 2004;34:83–91. doi: 10.1017/s0033291703008559. [DOI] [PubMed] [Google Scholar]
- 16.Fritzsche K, Liptai C, Henke M. Psychosocial distress and need for psychotherapeutic treatment in cancer patients undergoing radiotherapy. Radiother Oncol. 2004;72:183–9. doi: 10.1016/j.radonc.2004.03.015. [DOI] [PubMed] [Google Scholar]
- 17.Sharif Nia H, Ebadi A, Lehto RH, Peyrovi H. The experience of death anxiety in Iranian war veterans: A phenomenology study. Death Stud. 2015;39:281–7. doi: 10.1080/07481187.2014.991956. [DOI] [PubMed] [Google Scholar]
- 18.Cavers D, Hacking B, Erridge SE, Kendall M, Morris PG, Murray SA, et al. Social, psychological and existential well-being in patients with glioma and their caregivers: A qualitative study. CMAJ. 2012;184:E373–82. doi: 10.1503/cmaj.111622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sterckx W, Coolbrandt A, Clement P, Borgenon S, Decruyenaere M, De Vleeschouwer S, et al. Living with a high-grade glioma: A qualitative study of patients’ experiences and care needs. Eur J Oncol Nurs. 2015;19:383–90. doi: 10.1016/j.ejon.2015.01.003. [DOI] [PubMed] [Google Scholar]