

Abstract
Introduction and Objective:
Providing and enhancing the level of health are one of the essential needs of all people, and implementation of health promotion lifestyle is the most important and effective factor in maintaining and improving the health of the elderly. The present study aimed at defining the effect of aging on health-promoting lifestyle.
Methodology:
This randomized clinical trial was conducted on 72 individuals from the retirees clubs of Education department, Social Security, and Health centers in Ramsar, in 2017. Sampling was done randomly with blocking and random allocation in two groups: Experimental and control. Data were collected in two steps by Demographic profile questionnaire, AMT, ADL, OHI and HPlP II which validity and reliability of them were confirmed. Participants attended eight training sessions (twice each week). Data analysis was performed with the use of SPSS 18 and descriptive (Frequency) and analytic tests (Chi-square, Fisher's exact test, Independent Sample t test and Paired Sample t test) with a significance level of 0.05.
Results:
The results showed that the mean age of the elderly was 64.4 ± 4.1 years. The mean score of lifestyle enhancement was 148.59 and 173.25 before and after training in the experimental group, respectively. Based on the results of paired t-test (P < 0. 323), there was no significant difference between the mean life expectancy of elderly health promotion in control group before and after educational intervention; however, there was a significant difference between the two groups before and after training (P = 0.001).
Conclusion:
Educational programs play an important role in integrating health-promoting lifestyle to encourage the elderly to accept more accountability regarding health, sustained physical fitness, proper nutrition, healthy interpersonal relationships, expected spiritual growth, and the proper management of stress and anxiety in life.
Keywords: Education, elderly, health-promoting behaviors, lifestyle
Introduction
The elderly forms a significant number of population in all human societies, and along with increase in the number of elderly people, their health problems get more and more important.[1,2] Maintaining and improving the health of the elderly not only prevent chronic diseases but also greatly contribute to their independence and participation in family and social activities.[3]
Every person's lifestyle has an impact on his/her health, and health-promoting activities and healthy lifestyle are the main strategies for the facilitation and protection of health and are essential for maintaining and improving health, correcting and improving lifestyles.[4] Health promotion lifestyle includes six dimensions of health responsibility, physical activity, nutrition, spiritual growth, interpersonal relationships, and stress management.[5]
Feeling responsible and accountable toward one's health means understanding the activities that can be done to improve health so that people and society take responsibility for choosing a healthy lifestyle and have the ability to take responsibility for their health.[6]
Nowadays, many scholars have focused their attention on the relationship between physical activity and physical and mental health;[7] they have come to believe that although the ability of the body decreases with age, it can be improved.[8] Individuals with regular physical activity maintain their physical and mental function and live their daily lives independently and self-sufficiently; in addition, physical activity can also improve mental health.[9]
Nutrition is essential for health and disease prevention, and it should focus more on health promotion.[10] Nutrition is one of the important determinants of health in the elderly and plays a recognized role in common diseases of the elderly such as cancer, cardiovascular disease, and dementia.[11] Spirituality is also part of the philosophy of life and includes personal and private experiences that can be learned through good or bad situations and life.[11] Having meaning in life, hope with God's help in difficult situations, and feeling of belonging to a supreme source are all methods that help individuals tolerate less pressure in dealing with harmful incidents.[1]
The next dimension of health promotion lifestyle is interpersonal relationships. People are in constant communication with others to share their thoughts, feelings, and desires.[12] Communication is a transactional, target-oriented, multidimensional, irreversible, and possibly inevitable process, and the abundance of problems with which the elderly is struggling influences the communication skills of the community.[13]
The last aspect of health promotion lifestyle is stress management, one of the several factors the incorrect implementation of which can affect the performance of individuals, endanger their health, and lead to physical and psychological disorders, impairment in performance and adjustment capacity, and ultimately loss of quality of life.[11] The most effective and useful way to deal with stress is to strengthen mental and psychological powers, to apply adaptive methods, and to manage stress.[9]
Therefore, provision and promotion of health are one of the essential needs of all people.[15] Moreover, implementation of health promotion behaviors is the most important and effective factor in maintaining and improving the health of the elderly.[16] It is recommended to implement health promotion lifestyle programs to reach the goal of promoting the health of the elderly and to reduce chronic diseases and multiple complications due to the lack of a healthy lifestyle in a wide range.[17]
Based on limited research in this field in Iran, the researcher decided to design and implement a research aimed at determining the effect of education on the health-promoting lifestyle in the elderly to investigate the effect of education on health-promoting lifestyle among the elderly.
Methodology
This randomized clinical trial was conducted on 72 individuals from the retirees clubs of Education department, Social Security, and Health centers in Ramsar, in 2017. Sampling was done randomly with blocking and random allocation in two groups: experimental and control. After obtaining informed consent from the participants, the questionnaires were completed by both the test and control groups, with full explanation and follow-up by the researcher. Being aged above 60 years, willing completion of written form consent, having reading and writing skills, obtaining a minimum score of 8 in the cognitive test, acquisition of an independent score from the daily activities of life questionnaire, absence of known acute and chronic diseases, and non-compliance with a specific diet were the main inclusion criteria of the present study; the discontinuation of cooperation, failure to complete more than 50% of the health promotion lifestyle questionnaire, and lack of participation in more than one session of health education lifestyle education sessions were the main exclusion criteria. Samples were randomly divided into two groups, with 36 subjects in each group.
Four questionnaires were used to collect required data. A demographic questionnaire includes age, sex, marital status, educational level, residence, home ownership status, chronic disease history, health insurance coverage, household status, financial status, employment status, the level of family income and the amount of monthly income; with 10 items, the second questionnaire was the scale of Abbreviated Mental Test, the validity and reliability of which were verified in Bakhtiyari et al.'s study, with Cronbach's alpha coefficient of 0.76 for internal reliability and 0.89 for external reliability.[18] Health-promoting lifestyle questionnaire II (HPLP II) includes 52 items categorized in six dimensions; each of the four options is always, most often, sometimes, and never scored from 1 to 4, and the total score of overall health promotion behaviors is between 52 and 208.[4,19,20] According to Walker et al.'s research, the total Cronbach's alpha turned out to be 0.94 and the subscales turned out to be 0.49–0.97;[19] the validity of this questionnaire was assessed and approved with total Cronbach's alpha of 0.82 and subscales of 0.46–0.91 by Mohammedi Zeidi et al.[4] Activities of daily living questionnaire (ADL) includes eight items. Each item has three options of dependent (zero point), need help (1 point), and standalone (2 points). The overall score of the ADL index is from 0 to 16, and each subject will need help (8–11 points) and standalone (12–16 points) depending on the grade he/she earns in one of the three dependent classes (0–7 points).[21] In Iran, the content validity index was 0.82 and Cronbach's alpha was 0.80 for this questionnaire.[21]
The intervention was conducted in the form of eight sessions of 45–60 min face-to-face training, held weekly in two sessions over a period of 4 weeks, by lecture, group discussion, presentation of PowerPoint, and the provision of booklets, pamphlets, and compact discs based on scientific resources.[11,22,23] After the end of the sessions, to remind and control the activities, follow-up and counseling were continued by telephone and SMS for 1 month. At this stage, no intervention was performed for the control group. Three months after the end of the training sessions (according to similar studies),[24,25] the HPLP II questionnaire was completed by both groups in the presence of the researcher. After the completion of the data collection, educational materials were also provided for the control group. Collected data were analyzed using Statistical Package for the Social Sciences software version 18 and descriptive statistics included frequency distribution, mean, and standard deviation, whereas analytical statistics included Chi-square, independent t-test, and paired t-test; significance level was considered <0.5.
Results
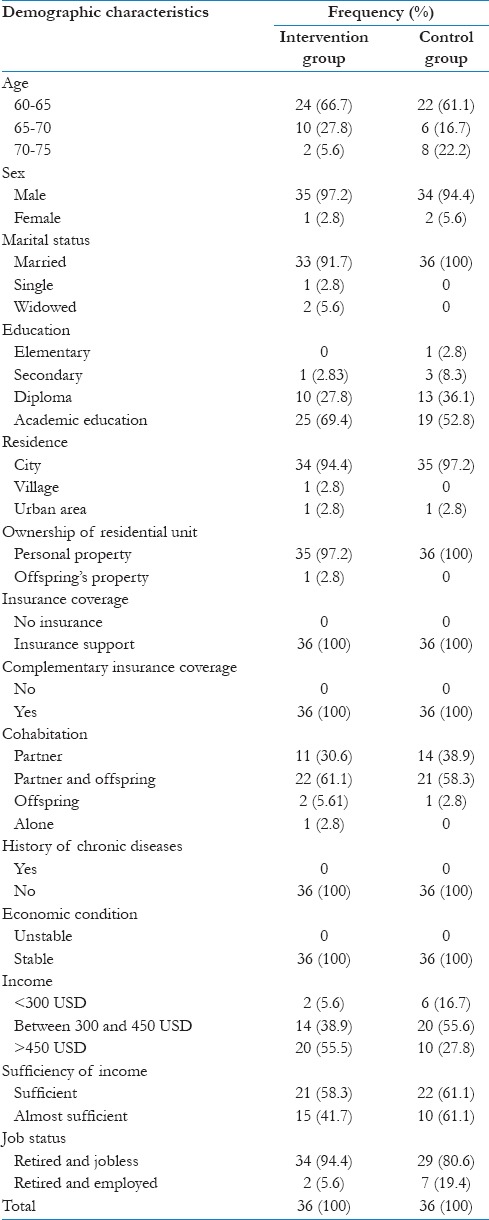
The results of the present study showed that the mean age of the elderly participating in the present study was 64.4 ± 4.1 years; the majority of them lived in the city and had private residential unit. 95.8% (69 people) of participants were male and married. 61.1% (44 people) of respondents had academic education and 59.7% (43 people) lived with their spouses and children. The amount of monthly income of 47.2% (43 people) was between 350 and 500 USD, and 59.7% (43 people) considered their income to be insufficient. 86.1% (62 persons) of respondents did not work after retirement, and all participants were covered by health insurance and supplementary care [Table 1].
Table 1.
Frequency distribution of demographic variables in two groups of control and intervention
Discussion
The analysis of the results of the posttest, which was conducted 3 months after training classes, showed that the mean score of total lifestyle improvement of elderly health was 148.59 and 173.25 before and after educational intervention, respectively [Table 2]; this difference was statistically significant (P = 0.001) [Table 3]. According to Khavoshi et al.'s study (2015), the mean of lifestyle score increased 3 months after intervention and reached 143.93, a difference of which was statistically significant (P = 0.02).[26] The results of Taghdisi et al.'s study showed that the difference in mean score of knowledge about the aging was statistically significant before and after education (P < 0.0001).[24]
Table 2.
The mean distribution of total score and dimensions of health promotion lifestyle before and after the intervention in two groups of intervention and control
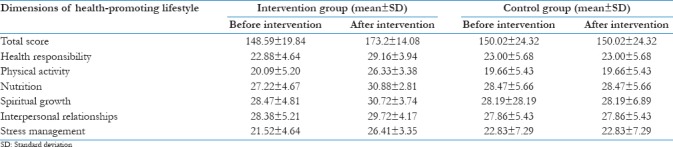
Table 3.
Comparison of mean total score and dimensions of health promotion lifestyle in the experimental group

The results of Heidari et al.'s study (2013) showed that there is a significant difference between the mean scores of life-promoting health in the experimental group before and after the intervention (P < 0.05).[27] The results of Rahimi Foroushani et al. showed that the difference between the mean scores of healthy lifestyle and its dimensions in the control and test groups was statistically significant (P < 0.0001).[25] Mehdipour et al. (2015) concluded, in their study, that the effect of the educational program on the increase in mean scores of physical activity, mental health, and interpersonal communication in the experimental group was positive and significant (P < 0.001); however, this difference was not meaningful in regard with nutrition (P = 0.113).[28]
Feeling responsible toward one's health is of paramount importance in old age.[24] The mean score of health responsibility increased from 22.88 to 29.16 in the intervention group of the present study [Table 2], a difference of which turned out to be statistically significant (P = 0.001) [Table 3].
Exercise and physical activity are quite important in guaranteeing a long, healthy life. The average score of physical activity increased from 20.09 to 26.33 in the intervention group; a difference which was, again, statistically significant (P = 0.001) [Table 3]. The mean score of this factor experienced considerable increase 3 months after intervention, a difference of which turned out to be statistically significant (P = 0.004).[26] According to the results of this study and similar studies, it is clear that sports activities are major sources of guaranteeing a high quality of life, and older people should be encouraged to increase their physical activity or keep minimum required physical activities and sports recommendations.[29]
Nutrition status is one of the most important aspects of promoting the lifestyle of elderly people.[24] The mean postnutrition score increased from 27.22 to 30.88 in the intervention group [Table 3], a difference which was, again, statistically significant (P = 0.001) [Table 3]; this was consistent with the results of Khavoshi et al.'s study because the average score of nutrition increased within 3 months after the intervention in the test group, which was statistically significant (P = 0.26).
A deep understanding of the interpersonal relationships of individuals in their social context provides an effective approach to health promotion.[30] The mean score of interpersonal relationships increased from 28.38 to 29.72 after intervention in the test group [Table 2], a difference which was, again, statistically significant (P = 0.001) [Table 3]. Although, in Khavoshi et al.'s study, the average score of the interpersonal relationships increased 3 months after the intervention in the test group, this difference did not turn out to be statistically significant (P = 0.26).[26] Based on the results of Taghdisi et al.'s study, it was observed that the implementation of the educational program did not show a significant increase in the mean of interpersonal relationships in the test group and no difference was witnessed in the intervention group.[24] With regard to the importance of interpersonal communication in promoting health, interventions such as communication skills training such as active hearing, dialog, and empathy are effective.[30]
Spiritual growth, and need, is one of the most important needs in the elderly that needs to be planned for.[11] Elderly is the period in which a person considers events throughout his/her life.[9] The mean score of spiritual growth increased from 28.38 to 29.72 after intervention in the test group [Table 2], a difference which was, again, statistically significant (P = 0.001) [Table 3]. This was, also, consistent with the results of Taghdisi et al.'s study, who showed that although the average score of the spiritual growth increased 3 months after the intervention in the test group, this difference did not turn out to be statistically significant.[24] Consequently, the belief that there is a God controlling the situation and observing his/her servants and belief that it is possible to control the uncontrollable situations in a way by relying on God and resorting to God reduce the anxiety greatly.[23]
Stress is one of the factors, affecting the performance of individuals that can endanger the health of individuals and lead to physical and mental illness, impairment of performance and adjustment power, and ultimately loss of quality of life.[11,14] Stress management training helps reduce the level of anxiety by increasing the level of people's understanding of the situation and using relaxation techniques; these programs, which are provided step by step for the individual, enable the person to have a clear understanding of the environment and its stressors, and by doing this, control his/her sense of stress and anxiety.[31] According to the findings of the present study, the mean score of stress management increased from 21.52 to 26.41 after intervention in the test group [Table 2], a difference which was, again, statistically significant (P = 0.001) [Table 3]. Although, in Khavoshi et al.'s study, the average score of stress management increased 3 months after the intervention in the test group, this difference did not turn out to be statistically significant (P = 0.99).[26] Although the same increase was observed in the intervention group studied in Taghdisi et al.'s research, no change was witnessed in the control group of this study.[24] Including training in relaxation methods in healthy lifestyle programs ensures physical and mental health and reduces the psychological stress and physical symptoms associated with it.[24]
Conclusion
Given the important role of education and training, health-promoting lifestyle programs can be implemented to enhance the level of mental and physical health in society.
Financial support and sponsorship
Deputy of Babol University of Medical Sciences.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The present study is a part of the approved Master's degree thesis, associated with Babol University of Medical Sciences, with Ethical registration code of (MUBABOL.HRI.REC.1395.87). Hereby, the researcher feels deeply obligated to thank the Research Deputy of Babol University of Medical Sciences for their financial support, Ramsar Education Organization Retirement Center and Social Security and Health Centers in Ramsar for their honest cooperation, and finally, the beloved elderly for participating in this study.
References
- 1.Hatami H, Razavi SM, Eftekhar Ardebili H, Majlesi F, Seyednozadi M, Parizadeh MJ. Text Book Public Health. Tehran: Arjmand; 2004. [Google Scholar]
- 2.Molashahri M, Nooripour Layavali R, Hosseinian S, Alikhani M, Rasooli A, Tabatabaei H. Comprehensive study of elderly's happiness in Zahedan city. J Aging Psychol. 2015;1:23–34. [Google Scholar]
- 3.Eliopoulos CH. In: Gerontological Nursing. Ghasemi S, Godrati V, Fallah Mehrabadi E, Rezaei F, editors. Tehran: Jameenagar; 2014. [Google Scholar]
- 4.Mohammadi Zeidi I, Pakpour Hajiagha A, Mohammadi Zeidi B. Reliability and validity of Persian version of the health-promoting lifestyle profile. J Mazandaran Univ Med Sci. 2012;22:103–13. [Google Scholar]
- 5.Wittayapun Y, Tanasirirug V, Butsripoom B, Ekpanyaskul C. Factors affecting health-promoting behaviors in nursing students of the faculty of nursing, Srinakharinwirot University, Thailand. J Public Health. 2010;40:215–25. [Google Scholar]
- 6.Parker JE, Parke K. Textbook of Preventive and Social Medicine: General Health Services (Part II) In: Shojaei Tehrani H, Malek Afzali H., editors. Tehran: Samatat; 2011. [Google Scholar]
- 7.Soheylipoor S, Hemayat Talab R, Heydar Abad ME, Hojjati A, Mahmood Abad EZ. Comparing of mental health between active olders and inactive olders in Tehran. J Psychol Sci. 2014;50:1–7. [Google Scholar]
- 8.Lobo A, Santos P, Carvalho J, Mota J. Relationship between intensity of physical activity and health-related quality of life in Portuguese institutionalized elderly. Geriatr Gerontol Int. 2008;8:284–90. doi: 10.1111/j.1447-0594.2008.00478.x. [DOI] [PubMed] [Google Scholar]
- 9.Shahbazi M. Tehran: Allameh Tabatabaei University; 2015. Effectiveness of Healthy Lifestyle Education Based on Global Health Model on Death Anxiety and Life Satisfaction in Elderly in Ilam. [Google Scholar]
- 10.Robinson JM. Nutrition and Nutrition Therapy. Translated by Ghorbani A. Tehran: SharAb and Future Builders; 2004. [Google Scholar]
- 11.Abdollahi A. Health Aging. Tehran: Jameenagar; 2013. [Google Scholar]
- 12.Vaghee S, Koushan M. Mental Health for Operating Room Students. Tehran: Andshe- e- Rafie; 2011. [Google Scholar]
- 13.Moin A, Anbari Akmal K. The patient-physician communication. Med Daneshvar J. 2010;17:71–80. [Google Scholar]
- 14.Philip Rice F. In: Human Development a Lifespan Approach. 4th ed. Foroughan M, editor. Tehran: Arjmand; 2016. [Google Scholar]
- 15.Ochieng BM. Factors affecting choice of a healthy lifestyle: Implications for nurses. Br J Community Nurs. 2006;11:78–81. doi: 10.12968/bjcn.2006.11.2.20445. [DOI] [PubMed] [Google Scholar]
- 16.Heshmati H, Behnampour N, Asna Ashari R, Ayatollahi A. Nutritional status and its related factors in elderly in Kashmar. Zahedan J Res Med Sci. 2014;16:43. [Google Scholar]
- 17.Rashidi S, Bahrami M. Factors associated with health-promoting lifestyle in elderly patients in selected hospitals of Isfahan University of Medical Sciences. J Urmia Nurs Midwifery Fac. 2015;13:90–8. [Google Scholar]
- 18.Bakhtiyari F, Foroughan M, Fakhrzadeh H, Nazari N, Najafi B, Alizadeh M, et al. Validation of the Persian version of Abbreviated Mental Test (AMT) in elderly residents of Kahrizak charity foundation. Iran J Diabetes Metab. 2014;13:487–94. [Google Scholar]
- 19.Walker S, Hill-Polerecky D. Psychometric Evaluation of the Health. Promoting Lifestyle Profile II. Unpublished Manuscript. University of Nebraska Medical Center. 1996:120–6. [Google Scholar]
- 20.Aghamolaei T, Ghanbarnejad A. Validity and reliability of the Persian health-promoting lifestyle profile II questionnaire. J Res Health. 2015;5:358–65. [Google Scholar]
- 21.Tanjani PT, Azadbakht M. Psychometric properties of the Persian version of the activities of daily living scale and instrumental activities of daily living scale in elderly. J Mazandaran Univ Med Sci. 2015;25:103–12. [Google Scholar]
- 22.Yektamaram S. Guideline Health of Older (over 50 years) Tehran: Department of Rehabilitation Welfare Organization; 2009. [Google Scholar]
- 23.Rafiee-Far SH. From Health Education to Health. Tehran: Ministry of Health and Medical Education: Office of Communications and Health Education; 2004. [Google Scholar]
- 24.Taghdisi M, Estebsari F, Rahimi Foroushani A, Eftekhar Ardebili H, Shojaeizadeh D, Dastoorpoor M, et al. An educational program based on the successful aging approach on health-promoting behaviors in the elderly: A clinical trial study. J Med Sci. 2014;21:25–36. doi: 10.5812/ircmj.16314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Rahimi Foroushani A, Estebsari F, Mostafaei D, Eftekhar Ardebili H, Shojaeizadeh D, Dastoorpour M, et al. The effect of health promoting intervention on healthy lifestyle and social support in elders: A clinical trial study. Iran Red Crescent Med J. 2014;16:e18399. doi: 10.5812/ircmj.18399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Khavoshi N, Tol A, Shojaeizade D, Shamshiri A. An effect of educational intervention on the lifestyle of elderly people referred to clinical centers of Eslamshahr, Iran: Application of health belief model. J Nurs Educ. 2015;3:19–28. [Google Scholar]
- 27.Heidari F, Khan Kermanshahi SM, Vanaki Z. The effect of a supportive health promotion program on the lifestyle of premenopause teachers. J Feyz. 2013;17:14–24. [Google Scholar]
- 28.Mahdipour N, Shahnazi H, Hassanzadeh A, Sharifirad G. The effect of educational intervention on health promoting lifestyle: Focusing on middle-aged women. J Educ Health Promot. 2015;4:51. doi: 10.4103/2277-9531.162334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.de Souto Barreto P. Direct and indirect relationships between physical activity and happiness levels among older adults: A cross-sectional study. Aging Ment Health. 2014;18:861–8. doi: 10.1080/13607863.2014.896863. [DOI] [PubMed] [Google Scholar]
- 30.Tol A, Tavassoli E, Shariferad GR, Shojaeezadeh D. Health-promoting lifestyle and quality of life among undergraduate students at school of health, Isfahan University of Medical Sciences. J Educ Health Promot. 2013;2:11. doi: 10.4103/2277-9531.108006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Servat F, Morovatisharifabad M, Sadeghipoor M, Rezaeipandari H, Fallahian FM, Mehrabbeik A, et al. Study of the effect of stress management skills on anxiety status among teachers in Meybod district high schools on 2012. Bimonthly J Sunrise Yazd. 2015;14:89–100. [Google Scholar]