

Abstract
Introduction:
Nowadays, pulmonary diseases have become one of the most important causes of mortality in the world. In this regard, the present study was aimed at examining the effect of implementing an educational package on quality of life (QoL) among patients with chronic obstructive pulmonary disease (COPD) referring to teaching hospitals affiliated with Ilam University of Medical Sciences.
Materials and Methods:
The present study was an interventional clinical trial in which the participants were randomly assigned into an intervention group and a control group. The statistical population included all COPD patients who had referred to the teaching hospitals affiliated with Ilam University of Medical Sciences. Sixty patients were selected by a convenience sampling method out of the whole patients who had referred to Shahid Mostafa Khomeini Hospital in Ilam. Afterward, they were randomly assigned into an intervention group and a control group (each including 30 patients). The collected data were analyzed using descriptive statistics; Chi-square test, independent and paired samples t-test, and correlational tests at a significance level of 0.05.
Results:
The results of the present study showed that as a result of the educational package, the intervention patients had a significantly higher QoL than the control patients (P = 0.001). The results also showed that implementing the educational package had a significant effect on QoL among the intervention patients in dimensions of physical function, mental health, social status, playing physical role, playing emotional role, physical pains, general health, and energy and vitality (P = 0.001).
Conclusion:
Based on the results of the present study, it can be concluded that collaborative education is a significant issue in health and treatment, and different dimensions of QoL can be enhanced by an appropriate educational program.
Keywords: Chronic obstructive pulmonary, quality of life, treatment
Introduction
Chronic obstructive pulmonary disease (COPD) is a disease in which progressive respiratory tract obstruction is irreversible. Airway obstruction and diffuse stenosis exist in all airways which increase resistance to air passage.[1]
COPD is one of the main causes of mortality in developing and developed countries. Its prevalence is increasing on a daily basis. Moreover, COPD is the fourth cause of mortality in the USA, and it is estimated that by 2020, it will rise from the sixth to the third cause of death in the world.[2] According to the newest statistics of the USA in 2008, the prevalence of this disease is 13.5 million people or one case per 20 people.[3] In Iran, the number of patients with COPD in 2001 was estimated to be 105 people per 100,000 in the age group of 15–49 years in 18 provinces and 1,057 per 100,000 in the age group of over 50.[4] The most important risk factor for COPD is tobacco use. Approximately 15 to 20% of cigarette smokers and more than 50% of smokers over 75 years old will develop COPD.[5]
Progress of obstruction of airways as a result of the disease restricts the patient to carry out his/her daily activities and exerts a heavy mental and physical burden on the patient, and it is also associated with high degrees of disability. All of these issues lead to a decrease in the quality of life (QoL) among such patients. Therefore, treatment of this disease is mainly aimed at decreasing the symptoms, increasing the functions, and improving QoL.[6]
Health-related QoL (HRQoL) is defined as the effect of disease and its treatment on the individual's function and refers to the individual's subjective experience and understanding of the effect of disease in QoL and the feeling of health.[7] QoL is a multidimensional concept, and its main dimensions are physical, emotional, mental, economic, familial, and social well-being. In addition to these, factors, such as disease, are important in QoL because disruption in physical dimension and its symptoms have a direct effect on all aspect of QoL.[8]
One of the methods of modifying and improving QoL, especially in chronic diseases, such as COPD is to provide such patients with necessary education. Teaching patients are a combination of planned educational activities that are aimed at helping individuals experiencing a disease so that they can change their behavior in a way that their health is preserved and enhanced.[9] Teaching patients brings about numerous advantages to patients, families, physicians, and nurses. Moreover, it also has a great influence on an increase in the level of compliance with treatment regimen and acceptance of the medical personnel's advice and appropriate communication between the nurses and the patients.[10] On the other hand, it enhances the patient's satisfaction and quality of care, increases the patient's participation in self-care, and improves the patient's QoL.[11] Designing and implementing educational programs with an emphasis on enhancing all QoL dimensions including spiritual-mental dimension and self-esteem among the patients with chronic diseases is highly significant and can improve the patients’ feeling of lack of independence, qualification, strength, and spirit in dealing with the problems caused by the disease. On the other hand, the patient's physical aspects of life can be affected and his/her QoL and in turn self-esteem can be improved by teaching about sports and diet. The effectiveness of such educational programs to a large extent depends on using educational methods.[12] Choosing an appropriate educational method depends on numerous factors including the intensity of the disease, the type of patients, the available facilities, etc. As they differ with regard to the method of administration, educational methods bring about various results regarding learning, and each method follows certain goals and may neglect some others. If a proper combination of different methods is used for chronic diseases such as respiratory diseases, better results can be obtained.[13] Since COPD engages different aspects of QoL using an educational package that transfers the information through five main types of media (i.e., text, video, sound, graphic, and animation) and covers all dimensions of QoL can be effective; therefore, it is not sufficient to utilize one type of educational method for such patients. Up to now, no studies focusing on measuring the effects of a complete educational package retrieved from several educational methods on QoL among such patients have ever been conducted; as a result and due to a lack of conducted studies in this field; the present study was carried out to evaluate the effect of an educational package on QoL among patients with COPD who had referred to the teaching hospital affiliated with Ilam University of Medical Sciences in 2016.
Materials and Methods
The present study was an interventional clinical trial. The study sample consisted of 60 patients with COPD who were selected by a convenience sampling method and randomly assigned into an intervention group and a control one. The control group had odd numbers and the intervention group had even numbers. Before administration of the intervention, informed consent was received from all of the participants, and they were provided with necessary explanations. Afterward, both questionnaires were completed by both groups in the form of interview. The intervention group received some interventions based on the educational package in two phases including three sessions of educational intervention and two sessions of follow-up intervention.
The first phase
The educational materials were carried out in three sessions in the form of groups of 4–5 over average periods of 60–90 min. It should be noted that this phase was conducted in a total of three visits over 6 weeks.
The second phase
It included two sessions of follow-up intervention. The content of these visits somewhat included final evaluation of the program and providing the patients with feedbacks and information on the level of their participation.
This phase took a total of two visits and 5 weeks.
Sessions of educational participation (3 sessions)
The aims of the first visit
The patients can be given attitude by familiarizing them with care problems, current conditions, disease threats and complications, and COPD signs and symptoms. In the first visit, the patients were empowered such that they could define COPD and its causes and complications.
The content of the first session
In included a review of chest anatomy, the causes of COPD, aggravating factors, mitigating factors, and complications. It was conducted through group discussion, lectures, and video projector.
The aims of the second visit
This visit was aimed at conducting the second phase, i.e., preparing the patients to participate in the care and treatment procedure with an interval of 2 weeks.
The patients should be able to explain the importance of appropriate lifestyle for other patients with COPD. They should be able to explain the appropriate lifestyle (including physical activities, staying away from dust, etc.) with examples.
The content of the second session
In this session, a definition of healthy lifestyle and the relationship between lifestyle and disease attacks and the number of hospitalization and quality of education were provided. These were presented through PowerPoint, video projector, group discussion, and animation.
The aims of the third visit
In this visit, the patients were expected to reach an acceptable level of awareness, attitude, and function to participate in care and treatment procedures.
The educational materials were presented in three sessions by a nurse in the form of groups of 4–5, each session took 60–90 min on average. It should be noted that this phase was carried out with three visits and over 6 weeks.
Follow-up visit (second phase)
This visit was aimed at continuing the care program and engaging the patients. The content of these visits somewhat included final evaluation of the program and providing feedback to the patients regarding the level of their participation. The visits took place at intervals of 2 weeks and in two sessions for each group of the patients. In fact, the final phase of education, i.e., evaluation was carried out during those visits. Evaluation was carried out in the form of stages in the beginning and end of each session, and for final evaluation, 3 months after the study the effect of education on QoL was tested by completing the QoL questionnaire again. In the end, after the 3rd month, final evaluation was conducted in the 6th session, and QoL among the patients before and after the intervention was checked by filling out the QoL questionnaire.
Study inclusion criteria
Having complete consent to enter the study
Not being in the acute phase of the disease
Having no other underlying diseases
Having stable physical status and being homodynamic
Having no sensorimotor and mental problems.
Study exclusion criteria
Exacerbation of the disease
Lack of satisfaction to continue the study.
Data analysis method
The data obtained from the questionnaires were analyzed through descriptive statistics and Chi-square test, Independent and paired samples t-tests, and one-way ANOVA at a significant level of 0.05 using Statistical Package for the Social Sciences (IBM SPSS Statistics for Windows, Version 22.0. IBM Corp., Armonk, NY). To test the homogeneity or heterogeneity of the intervention and control groups, Chi-square test was employed, and normality of the variables was checked using Kolmogorov–Smirnov test.
Moral considerations
Conduction of the present study not only required precision and skill but is also based on honesty and confidentiality. Conduction of moral studies begins with determining the participants and continues until the publication of the study.[14]
Results
According to the results of the present study, most of the patients in the experimental group (80%) and in the control group (73.33%) were men. The results of Fisher's exact test indicated that there was no significant difference between the two groups regarding the patients’ gender; therefore, the two groups were homogeneous with regard their gender.
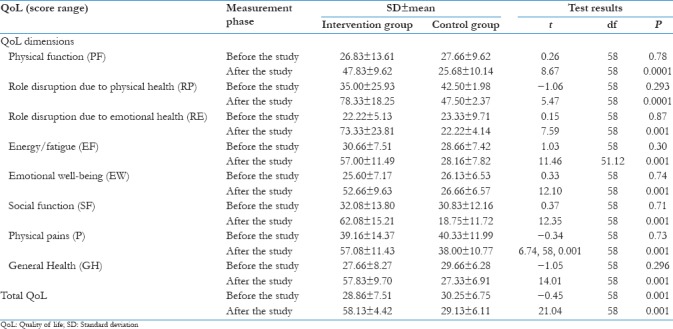
The results presented in Table 1 showed that the administration of the educational package had a significant effect on QoL among the intervention group in dimensions of physical function, social status, mental health, playing physical role, playing emotional role, physical pains, energy, and vitality (P = 0.001).
Table 1.
Comparing the mean of quality of life dimensions and total quality of life before and after the study in the intervention and control groups
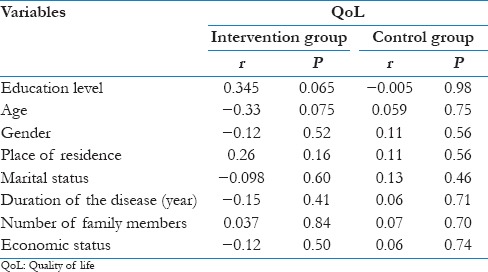
The results presented in Table 2 showed that the effect of administration of the educational package was significant on QoL among the intervention patients regarding gender, education level, age, place of residence, marital status, duration of the disease, number of the family members, and economic status.
Table 2.
The relationship between the demographic variables and quality of life in the intervention and control groups
Discussion
The results of the study showed that the administration of the educational package affected different dimensions of QoL in the intervention group compared to the control group. They also indicated that the dimensions of physical function, role disruption due to physical health, role disruption due to mental health, energy and fatigue, emotional well-being, social function, physical pains, and general health had significant improvement (P < 0.05). In addition, the results showed that the total QoL in the intervention group improved (P < 0.05). However, it is noteworthy that social function and general health in the control group were statistically worse after evaluations and interval (P < 0.05).
Since QoL among patient with scores under 34 was considered as low QoL, scores between 34 and 67 as average QoL, and scores between 67 and 100 as high QoL. In the present study, the score of total QoL in the intervention group rose from low QoL[15] before the intervention to average QoL[16] after the intervention. In the control group, however, the score of QoL changed from a low level[17] to a worse level.[18] The results of the present study showed that the application of the educational package of special behavior modification of patients with COPD had a significant effect on enhancing the QoL among the patients and led to remarkable changes in dimensions of QoL 3 months after the administration. Providing patients with attitude by familiarizing them with care problems, current conditions, disease threats and complications, and COPD signs and symptoms can be highly helpful. Moreover, a review of chest anatomy, the causes of COPD, aggravating factors, mitigating factors, complications, staying away from risk factors, proper diet and consumption of liquids, maintaining weight and energy, correct consumption of medicines, vaccination and individual sanitation, respiratory exercises through group discussions, lectures, and video projector can help the patient to understand the importance of appropriate lifestyle in COPD and appropriate lifestyle.
The review studies carried out by Devine,[19] Bourbeau et al.,[20] and Effing et al.[21] reported different results. It should be noted that educational programs in different studies were completely different. For example, Monninkhof et al.[22] studied the effectiveness of self-management plan along with sport training, but they observed no effect. Bourbeau et al.[20] however, reported remarkable results by utilizing a short, simple multidimensional intervention program. It is likely that making such interventions complex leads to a decrease in appropriate opportunity to learn and apply the skills provided by the interventional programs in the real conditions of life. Since in the present study, QoL and its dimensions had a significant improvement in the intervention group as a result of the educational package, it can be stated that a large portion of the capital of each country is nowadays spent on health services, which leads to the progress of national goals and decrease in poverty, and if such services are not sufficient, public dissatisfaction will rise, which has enhanced the level of attention to health in all countries. Since QoL is a mental self-assessment, individuals judge the quality of their lives by themselves and because QoL is a dynamic concept, external, and internal changes have an influence on it in different times. In this regard, educating individuals are one of the key components in empowering them, which has been paid close attention by health trainers and is used to improve QoL. Educating patients are a process through which QoL and the physical and mental levels of health are promoted, and the individuals’ self-confidence is improved.[23] The present study is in line with the one carried out by in terms of examining QoL dimensions. In their study, in examining the mean scores of QoL, the subdimensions of psychological outcome before and after the intervention, including mental health and restriction of mental role and social function, paired samples t-test, indicated a significant difference and examining the total score of QoL before and after the study showed that the amount of this variable increased.
Moreover, the present study is in agreement with the study entitled “the effect of short educational-psychological intervention (self-management and behavior modification method) on enhancing the QoL among patients with COPD” conducted by who focused on four dimensions of QoL including physical dimension, psychological dimension, social dimension, and environmental dimension which showed a significant difference. In the present study since psychological[24] and physical dimension[21] obtained the highest scores in the intervention group, there was no significant difference between the two groups in psychological dimension.
The main question regarding the effect of chronic physical disease on QoL is whether physical restrictions caused by such diseases alone can reduce QoL or not or whether the diseases lead to changes in QoL by influencing psychological, social, and individual dimensions. Although responding to these questions seems to be somewhat difficult, it can be stated that human is a creature with three dimensions of physiological, psychological, and social; therefore, components related to social life of human including QoL is affected by the three dimensions of human existence. The present study also proved the existence of such status.
The results showed that the administration of the educational package did not have a significant effect on the intervention patients’ QoL regarding their demographic characteristics (gender, age, education, place of residence, marital status, duration of disease, number of family members, and economic status), and there was no significant relationship between these characteristics and QoL (P < 0.05).
There are also some studies that reported that no significant difference between men and women with COPD regarding their QoL scores.[25] In the study conducted by Han et al.[26] the men obtained better scores than the women although the total score and score of other fields showed no difference between the men and women. In their epidemiological study, Carrasco Garrido et al.[27] showed that women with COPD had a lower QoL than men in mental and physical fields.
The effect of age on QoL among patients with COPD is controversial. Some studies have indicated that there is no relationship between the two factors of age and QoL[28] while some other studies referred to age as an essential and effective factor in QoL.[29] In the present study, however, there was no significant relationship between QoL and age after the intervention. Since there was not a lot of elderly in the present study, it can be stated that if there were more elderly patients, a significant relationship would be expected.
Conclusion
Since the results of the present study showed that different dimensions of QoL can be improved through an appropriate educational program, it can be concluded that collaborative education is a regular process of establishing effective mutual and dynamic relationship and health and care services (i.e., the participant) to understand the needs and problems more so as to control the disease and motivate and engage the patients to accept responsibility and help to improve and maintain their health. It also causes them to have more motivation and get prepared for dealing with and engage in the disease. In general, the results of the present study put emphasis on supplementing regular medical treatments with a short, simple multidimensional education program. Any educational program is inevitably associated with some limitations which necessitate interpreting the results with regard those limitations. Due to time limitation, the criterion of selecting the individuals, and the lack of sufficient facilities, the size of the study sample was also restricted. Therefore, much care should be taken into account while generalizing the results.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Hassanpour N, Attar bashi Moghadam B, Musavi S, Sami R, Entezari E. The relationship between demographic variables, disease severity and quality of life in chronic obstructive pulmonary disease patients. mrj. 2015;9:19–26. [Google Scholar]
- 2.Hosseini S, Yadollah K. Investigating the Impact of Participatory Care Model on the Quality of Life on Chemical Patients with Chronic Obstructive Pulmonary Disease. Fourth Congress of Applied Science of Military Medicine and Crisis Management (Scientific Research) 2008 [Google Scholar]
- 3.Roohafza HR, Akochakian S, Sadeghi M, Fardmoosavi A, Khairabadi GR, Ghasemi H. Investigating the Relation between Lifestyle and Chronic Obstructive Pulmonary Disease. Journal of Guilan University of Medical Sciences. 2006;15:32–7. [Google Scholar]
- 4.Kheirabadi GR, Ekochakian S, Amanat S, Nemati M. Comparison of the quality of life in patients with chronic obstructive pulmonary disease and control group. Hormozgan Medical Journal. 2009;12(4):255–60. [Google Scholar]
- 5.Bagherian Sararoodi R, Attaran N, Keypoor M, Khierabadi G, Maracy M. Beneficial Effects of Brief Psychoeducational Intervention (Self-Management and Behavioral Modification) on Quality of the Life for Patients with Chronic Obstructive Pulmonary Disease. Avicenna Journal of Clinical Medicine. 2008;15(3):52–9. [Google Scholar]
- 6.Montazeri A, Gashtasbi A, Vahdaninia MA. Translation, Determination of Reliability and Validity of the Persian version of the SF-36 Questionnaire. Paesh. 2005;5:49–56. [Google Scholar]
- 7.Aghakhani N, Alizadeh M, Feizi A, Rahbar N, Aliinejad B. The effect of dietary education on quality of life in hemodialysis patients referring to Taleghani hospital in Urmia. Nutrition Congress for Infants and Children. 2012 [Google Scholar]
- 8.Saeid Pour J, Jafari M, Ghazi Asgar M, Dayani Dardashti H, Teymoorzadeh E. Effect of educational program on quality of life in diabetic patients. JHA. 2013;16:26–36. [Google Scholar]
- 9.Tawafiyan SS, Jamshidi SM. Study of the effect of educational program on quality of life in women with low back pain: An interventional study. Q J Health Educ Promot Health. 2014;2:49–56. [Google Scholar]
- 10.Rabe KF, Hurd S, Anzueto A, Barnes PJ, Buist SA, Calverley P, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176:532–55. doi: 10.1164/rccm.200703-456SO. [DOI] [PubMed] [Google Scholar]
- 11.Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: Systematic analysis of population health data. Lancet. 2006;367:1747–57. doi: 10.1016/S0140-6736(06)68770-9. [DOI] [PubMed] [Google Scholar]
- 12.Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global burden of disease study. Lancet. 1997;349:1436–42. doi: 10.1016/S0140-6736(96)07495-8. [DOI] [PubMed] [Google Scholar]
- 13.Hoeymans N, Gommer AM, Poos MJ. Wat is de ziektelast in Nederland? 2010. [Last accessed on 2010 Aug 16]. Available from: http://www.nationaalkompasnl .
- 14.Khani Majid Industries, Zohreh M, Majid A. Reviewing Students’ Viewpoints on the Teaching and Evaluation of Clinical Units in Mashhad Dental School. 36 November. 2009 [Google Scholar]
- 15.Salvi SS, Barnes PJ. Chronic obstructive pulmonary disease in non-smokers. Lancet. 2009;374:733–43. doi: 10.1016/S0140-6736(09)61303-9. [DOI] [PubMed] [Google Scholar]
- 16.Hogg JC, Chu F, Utokaparch S, Woods R, Elliott WM, Buzatu L, et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. N Engl J Med. 2004;350:2645–53. doi: 10.1056/NEJMoa032158. [DOI] [PubMed] [Google Scholar]
- 17.Wedzicha JA, Seemungal TA. COPD exacerbations: Defining their cause and prevention. Lancet. 2007;370:786–96. doi: 10.1016/S0140-6736(07)61382-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bastable SB. Nurse as educator: Principles of teaching and learning. AJN Am J Nurs. 1998;98:16L. [Google Scholar]
- 19.Devine EC. Meta-analysis of the effects of psychoeducational care in adults with asthma. Res Nurs Health. 1996;19:367–76. doi: 10.1002/(SICI)1098-240X(199610)19:5<367::AID-NUR1>3.0.CO;2-O. [DOI] [PubMed] [Google Scholar]
- 20.Bourbeau J, Julien M, Maltais F, Rouleau M, Beaupre A, Begin R, et al. Reduction of hospital utilization in patients with chronic obstructive pulmonary disease: A disease-specific self-management intervention. J Cardiopulm Rehabil Prev. 2004;24:282. doi: 10.1001/archinte.163.5.585. [DOI] [PubMed] [Google Scholar]
- 21.Bourbeau J, Julien M, Maltais F, Rouleau M, Beaupré A, Bégin R, et al. Reduction of hospital utilization in patients with chronic obstructive pulmonary disease: A disease-specific self-management intervention. Arch Intern Med. 2003;163:585–91. doi: 10.1001/archinte.163.5.585. [DOI] [PubMed] [Google Scholar]
- 22.Monninkhof E, van der Valk P, van der Palen J, van Herwaarden C, Zielhuis G. Effects of a comprehensive self-management programme in patients with chronic obstructive pulmonary disease. Eur Respir J. 2003;22:815–20. doi: 10.1183/09031936.03.00047003. [DOI] [PubMed] [Google Scholar]
- 23.Garrison DR, Vaughan ND. San Francisco, CA: USA. Jossey-Bass Pub., A Wiley Imprint; 2008. Preface. Blended Learning in Higher Education: Framework, Principles, and Guidelines. [Google Scholar]
- 24.Monninkhof EM, van der Valk PDLPM, van der Palen J, van Herwaarden CLA, Partidge MR, Walters EH, Zielhuis GA. Self-management education for chronic obstructive pulmonary disease. Cochrane Database of Systematic Reviews. 2002;(issue 4) doi: 10.1002/14651858.CD002990. Art. No.: CD002990. DOI: 10.1002/14651858.CD002990. [DOI] [PubMed] [Google Scholar]
- 25.Ståhl E, Lindberg A, Jansson SA, Rönmark E, Svensson K, Andersson F, et al. Health-related quality of life is related to COPD disease severity. Health Qual Life Outcomes. 2005;3:56. doi: 10.1186/1477-7525-3-56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Han MK, Swigris J, Liu L, Bartholmai B, Murray S, Giardino N, et al. Gender influences health-related quality of life in IPF. Respir Med. 2010;104:724–30. doi: 10.1016/j.rmed.2009.11.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Carrasco Garrido P, de Miguel Díez J, Rejas Gutiérrez J, Centeno AM, Gobartt Vázquez E, Gil de Miguel A, et al. Negative impact of chronic obstructive pulmonary disease on the health-related quality of life of patients. Results of the EPIDEPOC study. Health Qual Life Outcomes. 2006;4:31. doi: 10.1186/1477-7525-4-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ketelaars CA, Schlösser MA, Mostert R, Huyer Abu-Saad H, Halfens RJ, Wouters EF, et al. Determinants of health-related quality of life in patients with chronic obstructive pulmonary disease. Thorax. 1996;51:39–43. doi: 10.1136/thx.51.1.39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ferrer M, Alonso J, Morera J, Marrades RM, Khalaf A, Aguar MC, et al. Chronic obstructive pulmonary disease stage and health-related quality of life. The quality of life of chronic obstructive pulmonary disease study group. Ann Intern Med. 1997;127:1072–9. doi: 10.7326/0003-4819-127-12-199712150-00003. [DOI] [PubMed] [Google Scholar]