

Abstract
Aims and Objectives:
The introduction of ceramic brackets was a much-heralded development in the field of orthodontics. However, the increased frictional resistance with these brackets led to the development of ceramic brackets with metal slots, which claimed to combine the esthetics of ceramic brackets with the low frictional resistance of metal brackets. Hence, this study was undertaken to evaluate the rate of canine retraction and the amount of anchor loss while using ceramic brackets and ceramic brackets with metal slots and with conventional preadjusted edgewise appliance (PEA) metal brackets.
Materials and Methods:
The patient sample consists of 12 patients. Six patients received ceramic brackets on one canine and conventional PEA metal brackets on the opposite canine within the same arch. The other six patients received ceramic brackets with metal slot on one canine and conventional PEA metal brackets on the opposite canine within the same arch. Unpaired t-test was used to analyze the data using SPSS version 20 (3M Unitek, Bangalore, Karnataka, India). The rate of retraction was calculated for individual canine retraction after initial leveling and aligning. Anchor loss was also calculated using the pterygoid vertical to the mesiobuccal cusp of the upper first molar on the lateral cephalograms.
Results:
The result of this study showed that the difference in the rate of retraction between ceramic brackets with metal slot and conventional PEA metal brackets and ceramic bracket while clinically significant was not statistically significant. The difference in the amount of loss of anchorage of both the groups was not statistically significant.
Conclusions:
Incorporation of the metal slot in ceramic brackets has reduced frictional resistance for more efficient and desired tooth movement. Ceramic brackets with metal slot generate lower frictional forces than ceramic brackets but higher than conventional PEA metal brackets.
Keywords: Anchor loss, canine retraction, ceramic brackets, ceramic brackets with metal slot
INTRODUCTION
The changes in the design of edgewise bracket by Andrews led to improved and more consistent result with shorter treatment time and simplification of orthodontic techniques. During the past 10 years, a wide range of metal, plastic, and now ceramic brackets, based on straight wire system, have evolved and become available.[1,2]
The introduction of ceramic bracket was a much-heralded development in the field of orthodontics. The ceramic brackets offer improved esthetics and are well suited to the oral environment.[3,4]
Ceramic brackets are especially popular among adult patients who express a desire for more esthetic appliances. However, ceramic brackets move teeth less efficiently than do the metal brackets according to Karamouzos et al.[4]
Studies have found that frictional resistance is significantly higher in ceramic brackets than in stainless steel brackets, for most wire size–alloy combinations regardless of slot size.[5,6] Therefore, ceramic brackets with a metal slot system were introduced to incorporate the esthetic properties of the ceramic brackets along with the less frictional properties of metal brackets according to Karamouzos et al.[4] However, the frictional resistance between orthodontic wires and ceramic brackets with metal slot during actual or simulated tooth movement has never been fully investigated.
Hence, this study is being undertaken to evaluate canine retraction using ceramic bracket, ceramic bracket with metal slot, and conventional preadjusted edgewise appliance (PEA) metal bracket systems. This study compares the amount of anchor loss during canine retraction using ceramic bracket, ceramic bracket with metal slot, and conventional PEA metal bracket system.
AIMS AND OBJECTIVES
To determine the efficiency of ceramic and ceramic with metal slot brackets during segmental canine retraction by the following:
By comparing canine retraction using ceramic bracket and ceramic bracket with metal slot with conventional PEA metal bracket systems
By comparing the amount of anchor loss after canine retraction, using ceramic bracket and ceramic bracket with metal slot with conventional PEA metal bracket system.
MATERIALS AND METHODS
All 12 orthodontic patients who needed first premolar extraction and canine retraction in the maxilla as a part of orthodontic treatment were selected during the period of January–March 2004 a convenient sample, method of sample size determination is mentioned below.
Sample size was determined using the following formula:
![]()
Where,
Z = 1 – α = 1.96
SD = Pooled standard deviation = 0.11 (based on pilot study)
L = Allowable error = 10%
N = Sample size
Level of significance = 10%
Power of study (1− β) = 90%
Substituting the values in the formula, sample size:
![]()
= 11.10
Thus, the sample size was 12.
The patients selected were undergoing orthodontic treatment in the Department of Orthodontics and Dentofacial Orthopedics, College of Dental Sciences, Davangere. Six patients received ceramic brackets on one canine and conventional PEA metal bracket on the opposite canine within the same arch. The other six patients received ceramic brackets with metal slot on one canine and conventional PEA metal bracket on the opposite canine of the same arch. The canine brackets which are used in the study were ceramic (Transcend, 3M), ceramic with metal slot (Clarity, 3M) and conventional PEA metal bracket (Gemini 3 M)/0.022 MBT prescription. The entire study was carried out from April 2004 to January 2006. Ethical clearance was obtained from Institutional Review Board of College of Dental Sciences with ethical approval letter no. 04_ D031_22904. Informed written consent was obtained from the patients before beginning of the study.
SELECTION CRITERIA
Inclusion criteria
Patients selected were explained regarding the procedure, and a written consent was obtained for the same
Case selection was limited to those teeth that were well aligned or cases with mild crowding
Patients who needed segmental canine retraction and first premolar extraction as a part of orthodontic treatment were included
All patients had Class I molar relationship
All teeth mesial to second molar were fully erupted before the commencement of the study
Canine retraction of at least 3 mm was required.
Exclusion criteria
Patients with certain oral manifestations of disease (e.g., cysts) or a chronic debilitating disease
Patients with loss of periodontal support >10% before treatment
Patients with excessive pain, root resorption, or devitalization of canines during treatment.
MATERIALS REQUIRED
Ceramic canine brackets (Transcend, 3M)
Ceramic with metal slot canine brackets (Clarity, 3M)
Conventional PEA metal canine brackets (Gemini, 3M)
Vernier calipers (Dentaurum)
E-chain (GAC International)
Dontrix gauge (American Orthodontics).
DETERMINATION OF RATE OF RETRACTION
The rate of retraction was calculated as the distance traveled, divided by the time required to complete space closure. This was recorded in millimeters per interval. An interval was defined as a 4-week period. Each patient was provided with two different brackets placed on opposite canine teeth within the maxillary arch. The canine brackets used in the study were ceramic brackets (Transcend, 3M), ceramic brackets with metal slot (clarity, 3M), and conventional PEA metal brackets’ MBT prescription. The remaining teeth were bonded with conventional PEA metal brackets (022 MBT prescription).
The canines were retracted with elastic chain extending from the second molar to the canine brackets. Class I mechanics were used with a force level of about 200 g. Again the force was applied by the same operator, which is to be as close to the selected valve and then rechecking the minimizing operator error. The force was measured at each appointment with a Dontrix gauge. Patients were seen at 4-week interval until retraction was completed.
A continuous, passively fitted (0.017 × 0.025) stainless steel archwire was used for canine retraction. Initial leveling and aligning was done, as required with 0.016” followed by 0.016 × 0.022 nickel–titanium archwires before the placement of 0.017 × 0.025 stainless steel wire. Measurements of retraction and anchorage loss were not made until after this leveling procedure was completed in these patients.
The canines were ligated to the archwire during retraction with elastomeric chain [Figures 1 and 2].
Figure 1.
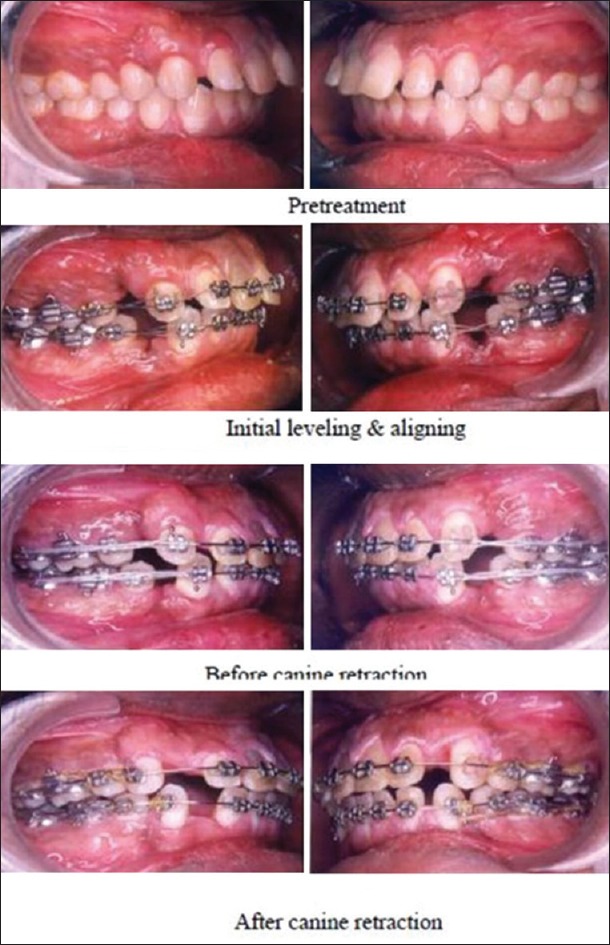
Case 1
Figure 2.
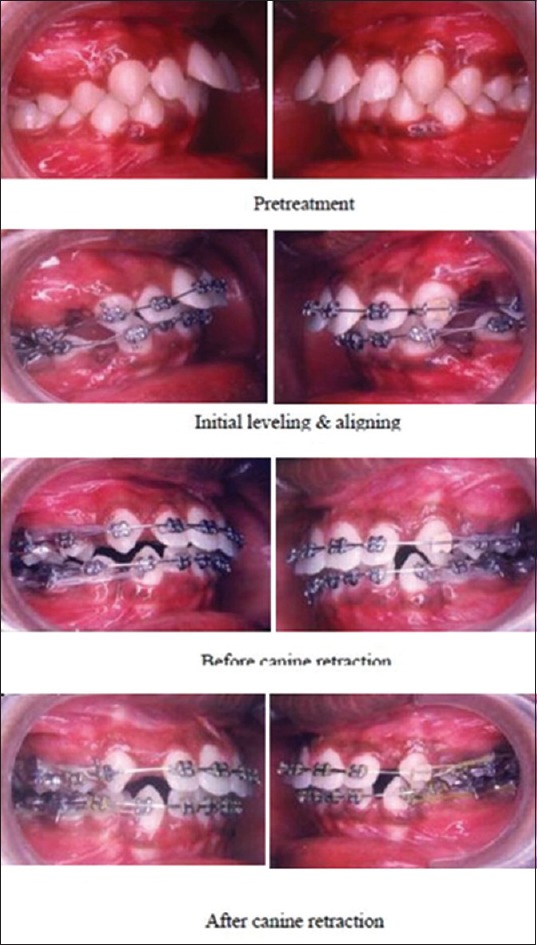
Case 2
The width of the extraction spaces was measured, and along with it, the space closure and time of the retraction were recorded.
Since it is not known exactly when canine retraction completes within an interval, the midpoint of the last interval was declared as the end point of retraction.
DETERMINING ANCHORAGE LOSS
Anchorage loss was recorded the movement in millimeters that occurred in the direction opposite to that of the applied resistance. Lateral cephalometric radiographs were taken right before the first premolar extraction and after the completion of the canine retraction.
These cephalometric radiographs were traced and pre- and postcanine retraction radiographs were superimposed. A pterygoid vertical was dropped perpendicular to FH. The distance between pterygoid vertical and the mesiobuccal cusp of the upper first molar on the lateral cephalogram was measured to determine anchor loss.
STATISTICAL ANALYSIS
Descriptive data that included mean, standard deviation, and minimum and maximum values were calculated for all the groups at each time interval. Unpaired t-test was used for comparison between two groups. P ≤ 0.05 was considered for statistical significance.
RESULTS
The patient sample consisted of 12 patients. Six patients received ceramic brackets on one canine and conventional PEA metal brackets on the opposite canine of the same arch. The other six patients received ceramic brackets with metal slot on one canine and conventional PEA metal brackets on the opposite canine of the same arch.
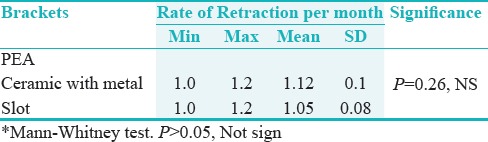
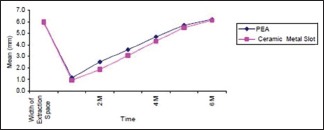
Table 1 and Graph 1 summarize the distance of retraction for ceramic bracket with metal slot and conventional PEA metal bracket systems. The maximum distance traveled by ceramic bracket with metal slot is 6.2 mm and PEA metal brackets is 6.2 mm. The minimum distance traveled was 5.5 and 5.4 mm, respectively, with a mean distance of was 5.97 and 5.93 mm, respectively. The maximum rate for the ceramic bracket with metal slot was 1.1 mm/interval, and for the PEA metal bracket, it was 1.3 mm/interval. The minimum rate observed was 0.7 mm/interval for the ceramic bracket with metal slot and 0.9 mm/interval for the PEA metal bracket. The mean was 1.05 and 1.12 mm/interval, respectively. The average difference observed in the rates of retraction was 0.07 mm/interval, where the P value was found to be P = 0.26, which is not significant (NS, P = 0.05).
Table 1.
Rate of Canine Retraction Ceramic Brackets With Metal Slot And Conventional Pea Bracket
Graph 1.
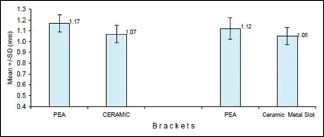
Comparison of rate of canine retraction PER month
Table 2 summarizes the anchorage loss. The ceramic bracket with metal slots’ maximum loss was 1.0 mm with a minimum of 0.2 mm and mean of 0.52 mm. The PEA metal bracket samples had a maximum anchorage loss of 0.8 mm and minimum loss of 0.2 mm and a mean loss of 0.45 mm. The mean difference in the anchorage loss was observed between ceramic bracket with metal slot samples and PEA metal bracket was 0.07 mm. The difference in amount of anchorage loss was also not statistically significant (P = 0.68, NS).
Table 2.
Anchorage loss ceramic brackets with metal slot and convetional PEA bracket

Graphs 2 and 3 graphically here are been depicted the correlation of anchorage loss and rate of retraction for ceramic bracket with metal slot and PEA metal brackets. There was no statistically significant correlation between anchorage loss and the rate of retraction for either bracket systems.
Graph 2.
Rate of canine retraction as per the mean value
Graph 3.
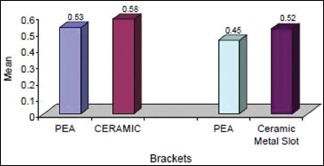
Comparison of anchor loss
Table 3 and Graph 1 summarize the distance of retraction for ceramic brackets and conventional PEA metal bracket systems. The maximum distance traveled by ceramic bracket was 6.8 mm, and for the PEA metal bracket, it was 6.6 mm. The minimum distance traveled was 5.5 and 5.4 mm, respectively, with a mean distance of 6.05 and 6.10 mm, respectively. While comparing the rate of retraction, the maximum rate for ceramic bracket was 1.2 mm/interval, and for PEA metal bracket, it was 1.3 mm/interval. The minimum rate was 0.7 mm/interval for the ceramic bracket and 0.8 mm/interval for PEA metal bracket. The mean was 1.07 and 1.17 mm/interval, respectively. The average difference in the rate of retraction was 0.10 mm/interval where the P value was found to be P = 0.07, which is NS.
Table 3.
Rate of canine retraction ceramic brackets with metal slot and conventional pea bracket
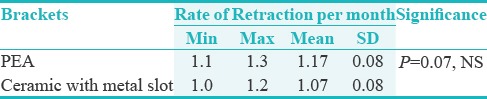
Table 4 summarizes the anchorage loss. The ceramic brackets’ maximum anchorage loss was 1.10 mm with a minimum of 0.2 mm and the mean was 0.58 mm. The PEA metal bracket had a maximum anchorage loss of 0.8 mm and minimum loss of 0.3 mm and the mean loss was 0.53 mm. The mean difference in anchorage loss between ceramic bracket and PEA metal brackets was 0.05 mm. The difference in the amount of anchorage loss was also NS (P = 1.0, NS).
Table 4.
Anchorage loss ceramic brackets & conventional pea bracket

Graphs 3 and 4 graphically depict the correlation of anchorage loss and rate of retraction for ceramic bracket and PEA metal brackets. There were no statistically significant correlation findings between anchorage loss and the rate of retraction for either bracket systems.
Graph 4.
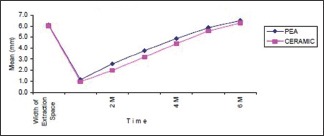
Rate of canine retraction
When compared between the groups, i.e., ceramic bracket with metal slot and ceramic bracket, the P value was found to be P = 0.72, which is NS.
DISCUSSION
The changes in the design of edgewise brackets by Andrews led to improved and more consistent result with shorter treatment time and simplification of orthodontic techniques. During the last decade, a wide range of metal, plastic, and now ceramic brackets based on the straight wire system have become available.
In clinical orthodontics, various multibracket techniques are used, to achieve desired tooth movement. In these techniques, sliding mechanics are frequently employed for mesiodistal tooth movement. Frictional resistance between wire and bracket is indicated as a shortcoming during sliding movement of a tooth.[1]
The greater friction of ceramic brackets with lighter wires is most likely related to the surface roughness of the ceramic bracket archwire slot. This surface roughness is likely the reason for friction [Figures 3 and 4].[7]
Figure 3.

Ceramic bracket (Transcend, 3M)
Figure 4.

Ceramic bracket with metal slot (Clarity, 3M)
The addition of stainless steel inserts in ceramic brackets generally did reduce the resistance to sliding. The stainless steel inserts, however, did improve the strength and rigidity of ceramic brackets [Figure 5].[8]
Figure 5.

Conventional PEA metal bracket (Gemini-3M)
The results indicated that there was variability among the subjects taken. This was noted with the time intervals, the rate of retraction, and the anchorage loss. Reitan[9] reported the importance of biologic response and the individual variation in tissue reaction. Hixon et al.[10,11] agreed with Reitan[9] in that the individual variation in its metabolic response was so great, it deluges any differences caused by the force magnitude. They concluded that since there was a large variation between patients, which precludes the formation of simple theories regarding force and anchorage, hence their results indicated that the variable, metabolic response, and not the magnitude of the force accounted for the major source of variation. It is generally considered valid that the higher forces produce more rapid movement than lighter forces, probably seen only within the individual patient.[12]
The force selected for canine retraction in our study was 200 g. The force magnitude selected was mentioned by some authors as being light. Quinn and Yoshikawa[13] estimated that a force between 100 and 200 g would be better for canine retraction. Hixon et al.[10] stated that when total forces of 300 g or less are applied, the average rate of tooth movement increases as the load per unit area of the periodontal ligament increased, no matter whether a tooth was allowed to be tipped or bodily moved.
Reitan[8] stated that the initial force application should be light because this tends to produce desirable biologic effects. The lighter forces will produce less extensive hyalinized tissue that could be readily replaced by cellular elements. He stated that an appropriate force of 150–250 g for maxillary canines and 100–200 g for mandibular canines should be used for translatory movement.
In the present study, the rate of retraction was calculated for individual canine retraction after initial leveling and aligning in which two different bracket groups (ceramic brackets with metal slot and conventional PEA metal brackets – Group 1 and ceramic brackets and conventional PEA metal brackets – Group 2) were placed on opposite canine teeth within the same arch.
The rate of retraction was calculated as the distance traveled, divided by the time required to complete space closure. The maximum rate for the ceramic brackets with metal slot was 1.1 mm/interval, and for the PEA metal brackets, it was 1.3 mm/interval. The minimum rate was 0.7 and 0.9 mm/interval, respectively [Figure 6]. The average difference in the rate of retraction was 0.7 mm/interval. There was no statistically significant difference in the rates between ceramic brackets with metal slot and PEA metal brackets.
Figure 6.
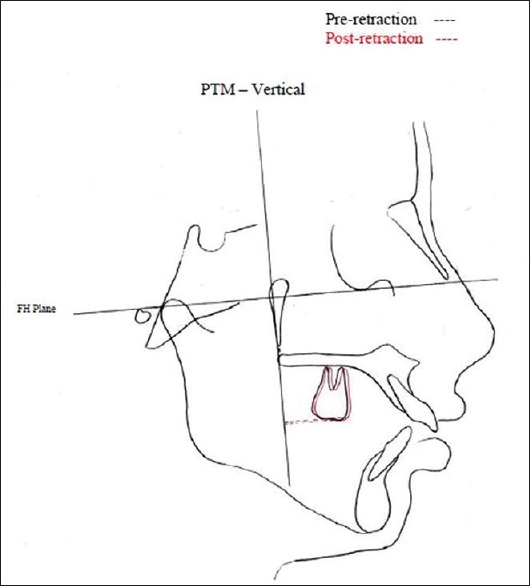
Superimposition to measure anchor loss
While comparing the other group, i.e. ceramic brackets and conventional PEA metal brackets, the maximum rate for the ceramic brackets was 1.2 mm/interval, and for the PEA metal bracket, it was 1.3 mm/interval. The minimum rate was 0.7 mm/interval for ceramic bracket and 0.8 mm/interval for PEA metal bracket, respectively. The average difference in the rate of retraction was 0.10 mm/internal. There was no statistically significant difference in the rates between ceramic brackets and PEA metal brackets.
Anchorage loss was the second query investigated in this study.
Determination of anchorage loss can be done in various methods. In the present study, the method proposed by Rickets was used, the distance between pterygoid vertical and the mesiobuccal cusp of the upper first molar on the lateral cephalogram, to measure the anchor loss.
The anchorage loss results appeared to have a clinical difference. The PEA metal bracket had a mean loss of 0.45 mm whereas the mean loss for ceramic brackets with metal slot was 0.52 mm. The difference in the amount of anchorage loss was not statistically significant.
In the other group, the PEA metal brackets had a mean loss of 0.53 mm whereas the mean loss for ceramic brackets was 0.58 mm. The difference in the amount of anchorage loss was not statistically significant.
In the present study, we have used ceramic brackets, which have no power arm.
Hence, there was difficulty in engaging the elastomeric chain for the purpose of canine retraction, whereas the ceramic brackets with metal slot have solved the above-mentioned problem. The widespread application of ceramic brackets and ceramic brackets with metal slot systems in orthodontics practice awaits further follow-up in issues concerning friction, overall treatment time, and patient comfort which needs to be investigated.
STRENGTH, LIMITATIONS, AND RECOMMENDATIONS
The strength of this study includes the following: it was an interventional study carried out for 2 years and strict protocol and procedure were followed during study to eliminate bias.
As the sample size taken is small and the duration of the study is also less, hence it is considered as the limitation of the study. To improve the validity of the study, further more studies should be implemented for more duration.
As this study was carried out among fewer subjects and results are not statistically significant, further studies should be carried out in other parts of the world with larger sample to validate the results.
CONCLUSIONS
Although the rate of canine retraction between ceramic bracket with metal slot and conventional PEA metal brackets showed a clinical difference, it was not statistically significant. The anchorage loss for the same was also NS.
The rate of canine retraction between ceramic brackets and conventional PEA metal brackets showed a clinical difference. It was not statistically significant. The anchorage loss for the same was also NS.
When compared, the rate of canine retraction between ceramic brackets with metal slot and ceramic brackets showed a clinical difference. It was also not statistically significant.
It was shown that efficiency of tooth movement was slightly reduced by the ceramic brackets when compared with ceramic brackets with metal slots and conventional PEA metal brackets. The loss of efficiency seems to be caused by frictional resistance between wire and ceramic bracket. Refinements in ceramic brackets by incorporating metal slots have reduced frictional resistance for more efficient and desired tooth movement, the ultimate goal in clinical orthodontics.
FINANCIAL SUPPORT AND SPONSORSHIP
Nil.
CONFLICTS OF INTEREST
There are no conflicts of interest.
REFERENCES
- 1.Angolkar PV, Kapila S, Duncanson MG, Jr, Nanda RS. Evaluation of friction between ceramic brackets and orthodontic wires of four alloys. Am J Orthod Dentofacial Orthop. 1990;98:499–506. doi: 10.1016/0889-5406(90)70015-5. [DOI] [PubMed] [Google Scholar]
- 2.Tariq M, Asif S. An overview of the Andrews preadjusted edgewise appliance. Indian J Orthod Dentofacial Res. 2016;2:32–3. [Google Scholar]
- 3.Camara CA. Aesthetics in orthodontics. Dental Press J Orthod. 2010;15:118–31. [Google Scholar]
- 4.Karamouzos A, Athanasiou AE, Papadopoulos MA. Clinical characteristics and properties of ceramic brackets: A comprehensive review. Am J Orthod Dentofacial Orthop. 1997;112:34–40. doi: 10.1016/s0889-5406(97)70271-3. [DOI] [PubMed] [Google Scholar]
- 5.Guerrero AP, Guariza Filho O, Tanaka O, Camargo ES, Vieira S. Evaluation of frictional forces between ceramic brackets and archwires of different alloys compared with metal brackets. Braz Oral Res. 2010;24:40–5. doi: 10.1590/s1806-83242010000100007. [DOI] [PubMed] [Google Scholar]
- 6.Ansari MY, Agarwal DK, Gupta A, Bhattacharya P, Ansar J, Bhandari R, et al. Shear bond strength of ceramic brackets with different base designs: Comparative in-vitro study. J Clin Diagn Res. 2016;10:ZC64–8. doi: 10.7860/JCDR/2016/20624.8910. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Omana HM, Moore RN, Bagby MD. Frictional properties of metal and ceramic brackets. J Clin Orthod. 1992;26:425–32. [PubMed] [Google Scholar]
- 8.Hoggan BR, Sadowsky C. The use of palatal rugae for the assessment of anteroposterior tooth movements. Am J Orthod Dentofacial Orthop. 2001;119:482–8. doi: 10.1067/mod.2001.113001. [DOI] [PubMed] [Google Scholar]
- 9.Reitan K. Some factors determining the evaluation of force in orthodontics. Am J Orthod Dentofacial Orthop. 1957;43:32–45. [Google Scholar]
- 10.Hixon EH, Aasen TO, Arango J, Clark RA, Kolosterman R, Miller SS, et al. On force and tooth movement. Am J Orthod Dentofacial Orthop. 1970;57:476–89. doi: 10.1016/0002-9416(70)90166-1. [DOI] [PubMed] [Google Scholar]
- 11.Hixon EH, Atikian H, Callow GE, McDonald HW, Tacy RJ. Optimal force, differential force, and anchorage. Am J Orthod. 1969;55:437–57. doi: 10.1016/0002-9416(69)90083-9. [DOI] [PubMed] [Google Scholar]
- 12.Roth RH. The straight wire appliance: 17 years laster. Am J Orthod Dentofacial Orthop. 1987;21:632–42. [PubMed] [Google Scholar]
- 13.Quinn RS, Yoshikawa DK. A reassessment of force magnitude in orthodontics. Am J Orthod. 1985;88:252–60. doi: 10.1016/s0002-9416(85)90220-9. [DOI] [PubMed] [Google Scholar]